
Abstract
Background
Health research knowledge translation (KT) is important to improve population health outcomes. Considering social, geographical and cultural contexts, KT in Inuit communities often requires different methods than those commonly used in non-Inuit populations.
Objectives
To examine the extent, range and nature of literature about health-related KT in Inuit communities.
Design
A scoping review was conducted. A search string was used to search 2 English aggregator databases, ProQuest and EBSCOhost, on 12 March 2015. Study selection was conducted by 2 independent reviewers using inclusion and exclusion criteria. To be included, studies had to explicitly state that KT approaches were used to share human health research results in Inuit communities in the Circumpolar North. Articles that evaluated or assessed KT approaches were thematically analysed to identify and characterize elements that contributed to KT success or challenges.
Results
From 680 unique records identified in the initial search, 39 met the inclusion criteria and were retained for analysis. Of these 39 articles, 17 evaluated the KT approach used; thematic analysis identified 3 themes within these 17 articles: the value of community stakeholders as active members in the research process; the importance of local context in tailoring KT strategies and messaging; and the challenges with varying and contradictory health messaging in KT. A crosscutting gap in the literature, however, included a lack of critical assessment of community involvement in research. The review also identified a gap in assessments of KT in the literature. Research primarily focused on whether KT methods reflected the local culture and needs of the community. Assessments rarely focused on whether KT had successfully elicited its intended action.
Conclusions
This review synthesized a small but burgeoning area of research. Community engagement was important for successful KT; however, more discussion and discourse on the tensions, challenges and opportunities for improvement are necessary.
The purpose of applied health research is to contribute to the development of actions that will improve the health of populations (Citation1). The creation of new knowledge from research is, on its own, often unlikely to lead to implementation or improvement of population health; therefore, a process to translate knowledge into practical action is necessary (Citation2). Many health research funding agencies have recognized the importance and necessity of the transmission, translation and exchange of new and existing health knowledge between researchers and stakeholders (e.g. other researchers, practitioners, policy-makers and community members) (Citation3–Citation5). Knowledge translation (KT) is a widely used term that describes the attempt to move research results into practical action. There are, however, many other terms used in health research to describe knowledge sharing with similar functions, such as “knowledge transfer,” “knowledge exchange,” “dissemination,” “results sharing,” among others (Table ) (Citation6, Citation7). The concept of KT is broad and commonly involves “end of grant KT,” whereby researchers share the research results with stakeholders at the end of the project (Citation2). More recently, there has been movement towards “integrated KT,” whereby stakeholders are involved throughout the research process (Citation8–Citation10), working together to build the research question, develop the methods and data collection tools, as well as actively engage in data collection, results interpretation and results dissemination (Citation2). For the purpose of this paper, the term KT will serve as an all-encompassing term for those knowledge-sharing activities that involve moving research results to practical action in some capacity, ranging from KT approaches that are integrated throughout the research process (i.e. integrated KT) to research results dissemination (i.e. end of grant KT).
Table I. Example definitions of knowledge translation–related terms
While the KT literature is diverse and growing (Citation6, Citation11), there has been comparatively less published about KT in Indigenous contexts (Citation14). The articles that have been published about Indigenous health KT suggest that differential social and cultural mechanisms of communication, along with historical, political and economic contexts within Indigenous populations necessitate unique approaches to KT (Citation9, Citation15–Citation19). Moreover, many argue that the disparities in health outcomes between Indigenous and non-Indigenous populations are, in part, due to challenges in effective KT (Citation12, Citation20–Citation22). Thus, the unique KT approaches required for Indigenous communities, disparities in Indigenous health outcomes and failures in past Indigenous health KT underpin the need for further research in this area (Citation14, Citation21,Citation22).
Within the existing, albeit limited, Indigenous health KT literature, there is a clear deficit in Inuit (i.e. individuals self-identifying as Inupiat, Yupik, Inuit, Inuvialuit, Kalaallit and Yupik (Citation23)) health KT–published literature. Indeed, while health KT literature for Inuit is sparse, there are several publications focusing on KT frameworks, approaches, ethical imperatives and best practices for several other Indigenous groups, including First Nations people in Canada (Citation23–Citation25) and the USA (Citation26), Canadian Metis (Citation27), Indigenous communities in Southern Canada (Citation20), Australian Aborigines (Citation28, Citation29) and Māori in New Zealand (Citation30). Similar to other Indigenous contexts, local uptake of Inuit health research results is particularly important because Inuit continue to experience health inequities compared to non-Inuit (e.g. lower life expectancies, higher infant mortality rates, higher infectious and chronic disease rates, and more mental health and wellness challenges) (Citation31–Citation33). As such, health research KT in Inuit communities is particularly important to move research results into practical action (Citation24, Citation34–Citation39).
It is important to understand how KT approaches in Inuit health research reflect differential cultural, political, economic and social norms to increase local uptake of research results. As such, the purpose of this scoping review was to better understand health research KT conducted within Inuit communities in the Circumpolar North. Specifically, the scoping review characterized the extent, range and nature of existing health-related KT literature in the Circumpolar North.
Methods
There were 5 key stages in this scoping review: (a) research question identification and search query development; (b) relevant study identification; (b) study selection; (d) data charting; and (e) results collation, summarization, thematic analysis and reporting (Citation40, Citation41).
Research question development, data sources and search strategy
The research question identified was “What does the literature tell us about knowledge translation in Inuit communities in the Circumpolar North?” To develop a search query to investigate this question, a preliminary search of general KT articles was conducted to identify KT terminology used in published papers and to create a broad list of potentially relevant terms. A library scientist assisted in developing various combinations of terms o develop a search string that included concepts (e.g. KT terms), populations (e.g. Inuit in Circumpolar locations) and outcomes (e.g. health and well-being). The final search string (Table ) was used to search EBSCOHost and ProQuest® aggregator databases with select electronic databases (Appendix 1), including peer-reviewed and grey literature. Searches were conducted on 12 March 2015 and limited to English language publications. The searches were not limited by year (except for restrictions on database capacity). Hand-searching key journals for relevant articles is commonly recommended for scoping reviews (Citation40, Citation41); as such, 3 key journals (International Journal of Circumpolar Health, Arctic and Inuit Studies) were hand-searched for relevant articles published in the past decade (March 2005 to March 2015). All returned citations from database searches were exported into RefWorks© online research management tool and then exported into the systematic review software DistillerSR, where all duplicates were removed.
Table II. Search string used in EBSCOHost and ProQuest® aggregator databases including terms for population, knowledge translation, health and location
Eligibility criteria
Articles that reported using KT approaches to share human health research results in Inuit communities in the Circumpolar North were included in this scoping review. The World Health Organization's definition of health was used to define human health, which involves a holistic understanding of health (i.e. physical, mental and social well-being) and not simply the absence of disease (Citation42). Therefore, the health research topic had to include an investigation of the physical, mental or social well-being of humans. Research results being shared about the environmental impact on human health were considered but those focused solely on the health of the environment were excluded. Studies had to focus on peoples originating from Thule culture, using the Inuit Circumpolar Council definition, including Inupiat, Yupik (Alaska), Inuit, Inuvialuit (Canada), Kalaallit (Greenland) and Yupik (Russia) (Citation23). Furthermore, the articles had to engage Inuit in the KT activity itself (i.e. Inuit were transferring, exchanging or receiving knowledge). Strategies for KT with solely non-Inuit target audience (e.g. academic poster presentations targeting southern scientists) and studies that used pan-Indigenous (e.g. combining First Nation, Métis and Inuit populations together) instead of Inuit-specific approaches were excluded. Geographically, studies conducted in countries in the Circumpolar North were considered, which included parts of Canada, Alaska (United States), Greenland and Chukotka (Russia) (Citation23).
Relevance screening
A two-stage screening process was conducted by 2 independent reviewers to identify relevant articles. First, the title and abstracts of all returned citations were screened based on the eligibility criteria using a form developed prior to the review. The relevant citations proceeded to the second stage, where the full text of the article was reviewed based on the eligibility criteria using a form developed prior to the review. Conflicts were discussed between reviewers; if a consensus could not be reached, a third reviewer decided if the study would be included. The degree of agreement between reviewers was assessed (i.e. inter-rater agreement via Cohen's Kappa (κ)) for both stages of screening (i.e. title/abstract and full text). The hand-search of the 3 key journals used the same inclusion/exclusion criteria as database searches. When the same study was published twice (e.g. a thesis dissertation and journal article of the same study), the article with the most information about KT was retained for analysis, and the duplicate article was discarded.
Data extraction & synthesis
Data were extracted from the included studies using a charting form to capture both count data, as well as descriptions of study results (Citation41). Information extracted included author(s), year of publication, year of study, location of study within the Circumpolar North, types of documents (journal article, thesis), specific health subfield and health outcome studied (Table ). The methodology for KT was also charted, including the KT method used, method of KT assessment and outcome measures of KT success. To identify and characterize elements that contributed to KT success and/or challenges, qualitative analysis was conducted for those studies that evaluated the KT approaches used to share human health research results in Inuit communities in the Circumpolar North. Specifically, to be included in the qualitative analysis, the KT activities had to be assessed (e.g. quantitative and/or qualitative evaluations, and/or reflections) in the study. For instance, several studies described the KT process but did not evaluate the process, and these studies were excluded from the qualitative analysis. Thematic analysis was conducted, which involved familiarization with the article content; generating initial codes; and developing, refining and defining themes (Citation43).
Table III. Summary of information collected in data charting form during the data extraction step of this scoping review included knowledge translation (KT) methodology, article information and overall recommendations given by the studies
Results
General characteristics of the articles
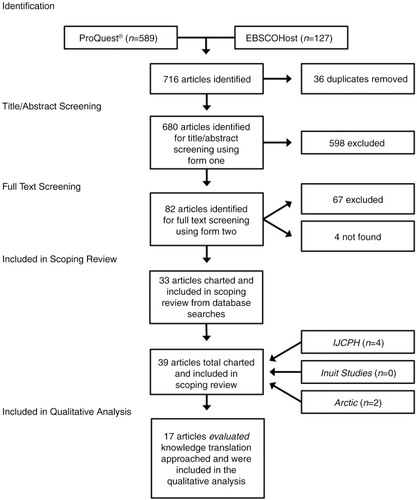
From 680 unique records identified in the initial search, 39 articles met the inclusion criteria and were retained for quantitative analysis (). There was strong agreement between reviewers at the title/abstract level (inter-rater reliability was high at κ = 0.82) and full-article screening level (inter-rater reliability was high at κ = 0.84). Herein, we outline the general characteristics of the 39 included articles.
Fig. 1. Search result numbers in the form of a flow diagram including identification, title/abstract screening, full article screening, as well as included articles in the scoping review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for reporting standards in systematic reviews (Citation44).
Most studies were published in the past decade and were primarily from Canada
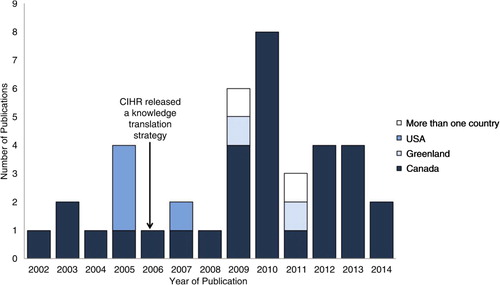
Thirty-one (80%) of the articles included were conducted in Northern Canada (Citation45–Citation74), 4 (10%) in Alaska, United States (Citation75–Citation78), 2 (5%) in Greenland (Citation31, Citation79) and 2 (5%) were international in focus (Citation33, Citation80). All studies were published between 2002 and 2014 (). A wide variety of health outcomes were discussed in the studies, including, but not limited to, environmental health (Citation38, Citation40,Citation81), diet and nutrition (Citation24, Citation30,Citation60), drinking water (Citation31, Citation43), zoonotic parasites (Citation48), substance misuse (i.e. drugs and alcohol) and foetal alcohol spectrum disorder (FASD) (Citation51), unintentional injury (Citation40, Citation54,Citation63), lifestyle behaviours (Citation34, Citation35,Citation60), contaminants (Citation52–Citation54), sexual health (Citation31) and heart and vascular disease (Citation75), as well as genetics (Citation76, Citation77).
Fig. 2. Location and year of the study, with an arrow indicating the year that Canadian Institutes of Health Research (CIHR) released its Knowledge Translation Strategy (Citation82).
Of the 39 included articles, 17 articles (44%) performed some form of evaluation or assessment of the KT approaches mentioned in this paper (Table ). These 17 articles were further examined in order to identify and characterize the elements that contributed to KT success and/or challenges. Herein, we describe the general characteristics of the evaluations conducted in these 17 articles, as well as the findings from the qualitative thematic analysis.
Table IV. Select findings from charting of articles that evaluated knowledge translation (KT) including author(s), title, document type, year study was published, year study was conducted, field of health research, location, type of KT assessment and funding source(s)
Methods used to assess KT were often informal
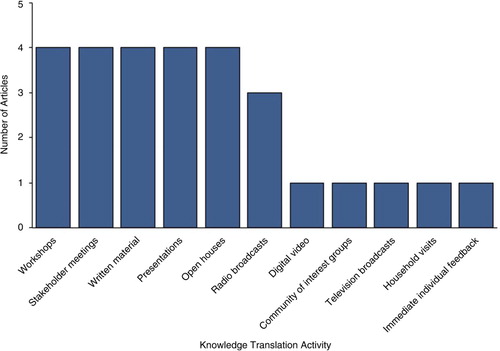
There were a wide variety of KT techniques outlined. Fourteen studies (82.4%) used oral KT methods (e.g. radio, presentation, open house and meeting) in conjunction with, or instead of, written KT methods (e.g. poster and report) (Table , ) (Citation45, Citation46,Citation48, Citation50–Citation57, Citation75–Citation77).
Fig. 3. Bar graph indicating the knowledge translation (KT) methods that were assessed in the literature including workshops (Citation53, Citation54,Citation73, Citation77), stakeholder meetings (Citation50, Citation51,Citation53, Citation75), written material (Citation50, Citation53,Citation54, Citation75), presentations (Citation50, Citation57,Citation75, Citation76), open houses (Citation52, Citation54,Citation55, Citation57), radio broadcasts (Citation50, Citation53,Citation57), digital video (Citation46), community of interest groups (Citation47), television broadcasts (Citation53), household visits (Citation75) and immediate individual feedback (categories are not mutually exclusive) (Citation76).
Appendix 1. Databases included in EBSCOHost and ProQuest® searches on March 12, 2015.
Of the articles that performed some form of evaluation or assessment of KT, the assessment activities ranged from reflections on the KT process (e.g. author of the article commented on what did or did not work in the KT strategy used in their study without any formal assessment), to quantitative evaluations (e.g. Likert scale questions, independent and paired t-tests) (a). Reflection on the KT strategy was used as the sole assessment tool in 10 studies (58.8%) (Citation50–Citation53, Citation55–Citation57, Citation75–Citation77). Qualitative evaluation were used in 4 (23.5%) studies (Citation45, Citation47–Citation49), and mixed quantitative and qualitative evaluations were used in 3 (17.6%) (Citation46, Citation54,Citation76) studies.
Fig. 4. Graphs displaying (a) the type of knowledge translation (KT) assessment (reflection (Citation50–Citation53, Citation55–Citation57, Citation75–Citation77), qualitative evaluation alone (Citation45, Citation47–Citation49) and both quantitative and qualitative methods (Citation46, Citation54,Citation76)), and (b) the elements that the author attributed to KT success (necessity of community involvement (Citation46, Citation50,Citation51, Citation56,Citation76), context (Citation45, Citation47,Citation49, Citation53,Citation54) or both (Citation31, Citation48,Citation51, Citation52,Citation57, Citation75,Citation77)).

Most studies assessed the social, political and cultural relevance of the KT method
Thirteen (76.5%) studies assessed whether KT methods fit with social, political and cultural needs or preferences of communities (Citation31, Citation45–Citation49, Citation51,Citation52, Citation55–Citation57, Citation76,Citation77). For example, one study found that stakeholder interviewees preferred KT methods that were interactive, oral–visual and presented in both English and Inuktitut (Citation48). Seven (41.2%) studies assessed whether their health research results had effectively moved to action through their assessment of the extent of local uptake and implementation of policy outcomes (Citation31, Citation45,Citation46, Citation54,Citation57). For example, local uptake of information was assessed in one study, which formally evaluated whether Elder stories on DVD were successful in transferring traditional knowledge about nutrition to youth using a comparison of pre- and post-DVD questionnaires distributed to youth (e.g. independent and paired t-test, content analysis and Likert scale interpretation) (Citation46).
Thematic analysis results
The thematic analysis of the 17 articles that evaluated KT methods resulted in 3 themes (detailed below): (a) community stakeholders as active members in the research process improved KT; (b) context was important in tailoring KT strategies and messaging; (c) varying and contradictory messaging reduces KT success.
Theme 1: Community stakeholders as active members in the research improved KT
All studies indicated the necessity of community involvement (29.4%) (Citation46, Citation50,Citation55, Citation56,Citation76), importance of context (29.4%) (Citation45, Citation47,Citation49, Citation53,Citation54), or both (41.2%) (Citation31, Citation48,Citation51, Citation52,Citation57, Citation75,Citation77) for successful KT in Inuit communities in the Circumpolar North (b). Involvement of community stakeholders in the original research was described as a contributing factor to the success of integrated KT throughout the research process in 12 (70.6%) studies (Citation31, Citation46,Citation48,Citation50–Citation52, Citation56,Citation57, Citation75–Citation77). One study informally reflected that the development of Inuit ownership of the research project seemed to increase KT success (Citation56). Another study reflected that the overall success of integrated KT was attributed to developing trusting partnerships with stakeholders, which appeared to allow researchers to anticipate and avoid potential problems and misunderstandings (Citation76). Indeed, other studies echoed similar findings, reflecting that their partnership with community-based researchers was central to the success of KT efforts, increasing the validity and relevance of research results and improving the potential for local uptake of research (Citation48, Citation52,Citation55, Citation57). For instance, one study reflected that consultation with community stakeholders helped improve appropriateness of both the content and delivery of KT (Citation52). Studies reported that approaches to KT were strengthened when local stakeholders directed the KT process (Citation45, Citation46,Citation48). For example, one study indicated that the involvement of youth in the communication of research results was perceived to increase local information uptake (Citation48). While many studies discussed the importance of community involvement in KT (Citation31, Citation46,Citation48,Citation50–Citation52, Citation55–Citation57,Citation75–Citation77), they did not evaluate the impact, if any, that this approach had on local uptake of research results. Furthermore, minimal analysis of the tensions and challenges (if any), or opportunities for improvement were included in the KT assessments. None discussed a decision-making process to decide when, and how much community involvement should occur, or to decide which community stakeholders should be involved. None assessed the appropriateness of varying involvement of community stakeholders and the effect on successful KT. Yet, there were obvious variances in the type and level of community involvement between studies based on the nature of the project and purpose of the KT.
Theme 2: Context was important in tailoring KT strategies and messaging
Attention to local cultural, social and geographical context, and target audiences were identified as an important consideration for successful KT in 12 studies (70.6%) (Citation31, Citation45,Citation47–Citation49, Citation51–Citation54, Citation57,Citation75, Citation77). For example, young females were interviewed about past and future food contaminant messaging, and identified that “if the material was deemed irrelevant to their setting and the food choice options they have, it may be disregarded no matter how clear or otherwise balanced the message is” (29, p. 105). The study explained that KT efforts may be ineffective if local challenges are not understood (e.g. public health messaging that instructs young women to not eat a particular food when other options are limited; or, instructing women to not eat a particular food that has important cultural implications) (Citation45). The young female interviewees also suggested that attention to social context (influential KT brokers, sharing networks, pathways of communication used in a particular subgroup) plays a role in successful KT strategies; in particular, many informal pathways (family, friends) were preferred for transmission of nutritional issues (Citation45). Indeed, another study found that youth were influential KT brokers as focus groups and key informant interviewees preferred dissemination strategies where “children were identified as key elements of KT efforts because their involvement in the delivery of research results would increase impact of the message due to their influential role in the community, especially their parents” (31, p. 107–108).
Geographical location was described in one study as an aspect of local context that must be considered in some KT processes (Citation47). Community stakeholder interviewees identified that the remoteness of target communities was a barrier to effective KT, especially for KT-involving training programmes (Citation47). Interviewees identified distance, weather and lack of roads in the community as major obstacles in holding training courses and suggested adaptations to in-person KT approaches, such as training videos or call centres, which may help to overcome these barriers (Citation47).
Theme 3: Varying and contradictory messaging reduces KT success
A challenge discussed in 3 (17.6%) of the studies was the lack of consolidated of KT efforts between research groups and organizations, leading to varying and sometimes contradictory messaging causing confusion among target audiences (Citation45, Citation50,Citation54). For instance, one study conducted a survey to evaluate the degree to which community stakeholders had been exposed to and comprehended messages about contaminants in country food (Citation54). The study found that the information had not been broadly received due, in part, to changing and conflicting messages from KT efforts over a period of several years (e.g. “contaminants are bad for them; but country food is the best food; they are being ‘poisoned’ by southern pollution, but are blessed by a strong, nutritious, culturally valued, country food tradition” (36, p. 57)). Furthermore, another study concluded that outreach messaging was more successful, clearer and easier to understand when organizations presented joint messages that reinforced one another, instead of contradicting one another (Citation45).
Discussion
Internationally, there is an increasing number of peer-reviewed publications that evaluate health-related KT (Citation7). However, we identified a small number of Inuit health publications reporting KT approaches and even fewer Inuit health KT evaluations. In health research, conducting and publishing KT evaluations are critical to learn from past successes or failures in KT. Researcher reflections on their own experience with KT methods can be useful for developing KT strategies; however, critical assessment of tensions and challenges (if any), or opportunities for improvement in various stages throughout KT is necessary. The results of this scoping review speak for the need of more studies that evaluate the efficacy of KT in the Circumpolar North.
The literature identified in this scoping review primarily focused on the importance of considering the local context in KT approaches; however, few evaluations of KT in this review measured or critically evaluated local uptake of research, or the efficacy of moving research results to practical action in some way. As such, future evaluations should focus on formally evaluating whether KT successfully elicited its intended action. For instance, evaluations could investigate whether KT efforts impacted policy, health behaviour, medical practice or public health practice. There is still much to learn about moving research results into practical action, especially in Inuit communities where little is known about local uptake of research results within Inuit knowledge sharing systems and ways of knowing (Citation14, Citation21,Citation52).
The timing and large proportion of studies conducted in Canada could be due partially to endorsement of KT from major Canadian government agencies such as Canadian Institutes of Health Research (CIHR) (Citation31,Citation45–Citation48,Citation50, Citation57,Citation83) and Health Canada (Citation51, Citation52). Indeed, the increase of published KT literature in Canada began 1 year after the CIHR released a Knowledge Translation Strategy in 2004 with specific objectives to fund grants that support KT research (Citation82). Furthermore, another study stated that “CIHR is recognized within Canada and internationally for leading and funding the advancement of KT science and practice” (54, p. 1), which may, in part, explain the predominance of Canadian papers identified in this review. While fewer studies were captured from the United States (Citation75–Citation77) and Greenland (Citation31), KT is still recognized as important by the U.S. National Institutes of Health (Citation75–Citation77) and Greenlandic Medical Research Council (Citation31). Few studies from Russia, USA and Greenland do not necessarily indicate a dearth of KT assessments in these regions; this result may have been due to our English-only search strategy, and/or a lack of peer-reviewed publications of such assessments from these countries.
Our results indicated that KT is more effective when community stakeholders are active members in the research process. Indeed, research in Indigenous communities that is conducted by non-Indigenous researchers can sometimes be met with scepticism and resentment by community members (Citation24, Citation84–Citation88). This potential resentment can be understood by reflecting on decades of research on Indigenous peoples, where some non-Indigenous researchers historically “parachuted” into communities to collect data (often without consent) with limited attempts to involve community stakeholders before, during or following the research process, in the form of KT (Citation24, Citation84–Citation88). Attempts have been made to improve research methods by focusing on community participation, capacity development and social equity (Citation84, Citation87); however, there continue to be embedded power dynamics such as conflicting goals between universities and communities, hierarchy of scientific knowledge over Indigenous knowledge and the production of knowledge by researchers that has limited direct value to the community (Citation24, Citation84–Citation88). In comparison to written or less interactive KT, we found that the interactive oral KT was most commonly used in Inuit communities and was supported by the extended literature as a preferred means of engagement by Inuit and other Indigenous groups (Citation89, Citation90). Future health research projects in Inuit communities should consider the incorporation of oral methods when building KT strategies as Inuit have a strong oral history and culture. While oral methods are appropriate for cultural and historical reasons, they may not be sufficient in moving research results into practical action due, in part, to embedded power dynamics between researchers and research participants (Citation91, Citation92).
There are a number of different approaches available to reduce power differentials in research (Citation93, Citation94). For instance, narrative or story-based approaches to data collection can reduce power imbalances and could be expanded to approaches in KT (Citation87), providing a method for giving voice to Indigenous communities through sharing stories (Citation85, Citation87,Citation95). However, influence from non-Inuit researchers on the stories shared through narrative or story-based approaches (e.g. selection and interpretation of stories shared) can perpetuate these power dynamics despite attempts to avoid this; as such, they should be used with caution (Citation87). One way researchers have attempted to diminish power dynamics in data collection is through methods such as digital storytelling, where Inuit are able to create and control their own research framework, in their own voices (Citation87). If methods such as digital storytelling can decrease power imbalances in primary data collection, then perhaps such methods could also reduce power imbalances in KT, whereby knowledge is generated by the community and disseminated through methods primarily locally led. It may be necessary to rebuild the KT methodological framework for Inuit communities, such that it is grounded in Inuit oral histories and cultural practices, and based on actively attempting to deconstruct power dynamics in the KT process between researchers and research participants and between Inuit and non-Inuit (Citation87).
Community participation as a driver for successful KT was a theme echoed by the findings of van der Velde et al., in their assessment of participatory action research (PAR) in the context of multiethnic mental health research and KT (Citation96). The researchers examined the degree of success relative to the 4 main tenets of PAR – empowerment, social change, participation and learning (or KT) – and found that success in each of the tenets was dependent on the level of community stakeholder participation in the research process (Citation96). Participation was viewed as the “gateway” for engaging in PAR, while successful KT, opportunities for learning and empowerment supported continued engagement in the research process (Citation96). The inclusion of community stakeholders in the study process allowed integrated, and often informal, KT between external and internal community researchers, which can aid in the integration of community values, knowledge and technical assessments in KT processes (Citation97). This engagement with community researchers can lead to a more informed and culturally relevant KT strategy, which promotes successful dissemination and utilization of research (Citation90). In a study that examined factors that influence environmental health KT processes in Canadian Indigenous communities (i.e. Inuit, First Nations and Metis), decision-making actors identified participatory processes as fundamental to successful dissemination and utilization of research (Citation90). Recently, literature has questioned whether or not engagement of community stakeholders in the entire research project is appropriate in all projects at all times (Citation98–Citation100). There is a need to move beyond uncritically advocating for community engagement and move towards discussion and discourse on the tensions, challenges and opportunities for improvement in community engagement (Citation100). Similarly, assessments of KT should include a critical discussion of the role of community engagement and its effect on whether the KT outcome was achieved. Guidelines regarding when, how and which community members should be involved in KT research should be developed to create strategies for appropriate community engagement.
There are strong arguments for Indigenous health research that is self-determined (owned, controlled, accessed, possessed) by Indigenous communities (Citation101); however, this review only captured one study that explicitly indicated that the community had taken ownership over the entire research process, including KT. One method of facilitating community ownership of KT processes throughout the research project is through the use of negotiated Indigenous research agreements as a natural extension of participatory research (Citation9, Citation102). For instance, the Canadian Tri-Council (Citation102), as well as the Australian Institute of Aboriginal and Torres Strait Islander Studies (Citation9), created a set of guidelines for conducting research with Indigenous partners, whereby complete ownership of the data by Indigenous partners is considered a major principle. These agreements can be advantageous to KT in some communities; however, for other communities these types of formal research negotiations may hold negative connotations stemming from periods during colonization when unethical signing of contracts took place (Citation103). In communities where formal signed research negotiations hold negative connotations, oral negotiations may be more appropriate (Citation103). It is important to ensure clarity of KT expectations (before, during and after the study) of all concerned (funders, researchers, community). It is essential that research bodies in the Circumpolar North continue to commit to equitable research including KT with Indigenous communities, by thinking critically about equitable ownership of research production and dissemination.
Our study found that a comprehensive understanding of the context of target subgroup(s) increased the likelihood of finding appropriate KT methods. The aim of both health promotion and KT is to use health knowledge to elicit an action from community stakeholders. Examination of the literature on health promotion may help to enhance KT strategies to improve moving research results into practical action. The need to tailor KT strategies for individual Inuit communities and subgroups within Inuit communities can be understood through health behaviour models. Many health behaviour models explain that local health promotion can be greatly affected by community and personal context, and that health behaviours are determined by personal perceptions about a disease and the strategies available to decrease its occurrence (Citation104). We can apply many concepts from health behaviour and public health promotion to KT. For instance, subgroup and individual uptake of research results through KT may be explained by the perceived seriousness of disease, susceptibility to disease, and benefits and barriers to behavioural change (Citation104). Perceptions about a disease and the strategies available to decrease its occurrence can be very different between subgroups and can be modified by cues to action (e.g. events, people or things that motivate behavioural change), motivating factors (e.g. culture, education level and past experiences) and self-efficacy (i.e. belief in one's own ability to do something) (Citation104). Strategies for KT may be more effective if they are grounded in a health behaviour model and incorporate understandings of local or target subgroup cues to action, motivating factors and self-efficacy. If KT messages are able to capture the particular Inuit community or subgroup's context, and elicit social modelling, KT may be more successful in influencing health behaviour within particular subgroups. Indeed, tailoring the research process to specific subgroups can help promote the development of more nuanced and relevant research for the participants and community, and is enhanced by involving members of the subgroup in KT strategies (Citation105, Citation106).
Conflicting messaging was identified as a challenge in health-related KT in the Circumpolar North and is also a common challenge in public health promotion globally (Citation107, Citation108). Contradictory messaging can cause confusion about what behavioural changes or actions are appropriate (Citation45). Health researchers working with Inuit communities must find ways to increase the cohesiveness and consistency of messages within and between studies. Active involvement of community stakeholders as liaisons between research projects can encourage discussion across research groups helping researchers increase their own awareness of previous results that were communicated and may be outdated (Citation107, Citation108). This increased coordination among research groups can improve cohesiveness of messages in the future (Citation107, Citation108). Active communication among all affected parties can help facilitate integrated KT (Citation90), improving the comprehension and cohesion of messages in results dissemination KT between researchers, communities, policy-makers and practitioners (Citation97). Lack of time, resources and personnel in the region may be barriers for community stakeholder involvement as research liaisons (Citation45). This may be a place where boundary organizations (e.g. Nunavut Research Institute, Inuit Research Advisors in each settled land claim region of Canada, Arctic Research Consortium of the United States and Greenland Center for Health Research) may be able to play a role in results dissemination of high impact and controversial issues (Citation45).
This study used a systematic, transparent, repeatable approach to identify, evaluate and synthesize literature. Furthermore, 2 independent reviewers screened the literature for relevance (with a high level of agreement) and 2 aggregator databases were searched. While these approaches increase the rigour and robustness of literature reviews, there were several study limitations that should be noted. The small number of health studies that assess KT in Inuit communities in the Circumpolar North that were identified in this review could be a result of an underreporting of KT assessments, a lack of quantity of KT assessments, and/or our search strategy. This review did not seek to capture assessments of KT from key organization websites or other grey literature publications; information from these sources may add to the discussion surrounding KT in Inuit communities.
Conclusion
The small but growing number of peer-reviewed health-related KT evaluations suggests there is still much to be learned about KT in the Circumpolar North. To learn from past successes or failures in KT, it is strongly suggested that assessment of the KT process takes place, and researchers disseminate the KT assessment results in a format that is accessible and available to future projects and researchers (e.g. peer-reviewed journal article). It may be necessary to rebuild the KT methodological framework for Inuit communities, such that it is grounded in Inuit oral histories and cultural practices, and based in actively attempting to deconstruct power dynamics in the KT process between researchers and research participants. Although community engagement was considered key to successful KT in the majority of the studies included in the review, discussion and discourse on the tensions, challenges and opportunities for improvement in community engagement are necessary. Similarly, assessments of KT should include a critical discussion on the role of community engagement and its effect on successful KT. It is important to develop guidelines for the decision-making process around when, how much and which community member involvement should occur; these guidelines would provide useful direction around community engagement within KT methodological frameworks. Overall, this scoping review was intended to inform future KT methods within Inuit communities and improve future critical reflection and assessments of the KT process.
Conflict of interest and funding
Additional thanks to our funding from ArcticNet, the CIHR/NSERC/SSHRC Tri-council and IDRC International Research Initiative on Adaptation to Climate Change (IRIACC) grant (IHACC), as well as the Public Health Agency of Canada (PHAC).
Acknowledgements
We would like to extend our sincere thanks to J. Brett, User Services Librarian at the University of Guelph, for his expertise in search string development and overall search strategy.
Related Research Data
References
- Canadian Institutes of Health Research.2015; Institute of Population and Public Health. [cited 2016 Feb 4]. Available from: http://www.cihr-irsc.gc.ca/e/13777.html.
- Canadian Institutes of Health Research. More about knowledge translation at CIHR knowledge translation – Definition. 2014. [cited 2016 Feb 4]. Available from: http://www.cihr-irsc.gc.ca/e/39033.html.
- Tetroe J. Knowledge translation at the Canadian Institutes of Health Research: a primer. Focus Technical Brief. 2007; 18: 1–8.
- National Institutes of Research. National Center for Advancing Translational Sciences (NCATS). 2016. [cited 2016 Feb 4]. Available from: https://ncats.nih.gov.
- Ladefoged K, Bjerregaard P. Greenland Institute of Health Research inaugurated in October. Int J Circumpolar Health. 2008; 67: 485.
- Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, etal. Lost in knowledge translation: time for a map?. J Contin Educ Health Prof. 2006; 26: 13–24.
- Tetroe JM, Graham ID, Foy R, Robinson N, Eccles MP, Wensing M, etal. Health research funding agencies support and promotion of knowledge translation: an international study. Milbank Q. 2008; 86: 125–55.
- Bjørk IT, Lomborg K, Nielsen CM, Brynildsen G, Frederiksen AMS, Larsen K, etal. From theoretical model to practical use: an example of knowledge translation. J Adv Nurs. 2013; 69: 2336–47.
- Kendall E, Sunderland N, Barnett L, Nalder G, Matthews C. Beyond the Rhetoric of participatory research in indigenous communities: advances in Australia over the last decade. Qual Health Res. 2011; 21: 1719–28.
- Pearce TD, Ford JD, Laidler GJ, Smit B, Duerden F, Allarut M, etal. Community collaboration and climate change research in the Canadian Arctic. Polar Res. 2009; 28: 10–27.
- Shaxson L, Bielak A, Biela A, Ahmed I, Brien D, Conant B, etal. Expanding our understanding of K* (Kt, KE, Ktt, KMb, KB, KM, Etc.): a concept paper emerging from the K*. Ontario, Canada: Conference Held in Hamilton. April 2012, UNUINWEH, Hamilton; 2012.
- Rabin B, Brownson R, Haire-Joshu D, Kreuter MW, Weaver NL. A glossary for dissemination and implementation research in health. J Public Health Manag Pract. 2008; 14: 117–23.
- Schwartz DG. Encyclopedia of knowledge management. 2006; London, UK: Idea Group Inc..
- Estey E, Kmetic A, Reading J. Knowledge translation in the context of aboriginal health. Can J Nurs Res. 2008; 40(2): 24–39. [PubMed Abstract].
- Estey E, Smylie J, Macaulay A. Aboriginal knowledge translation: understanding and respecting the distinct needs of aboriginal communities in research. 2009; Ottawa, Canada: Institute of Aboriginal Peoples’ Health, Canadian Institutes of Health Research. 1–5.
- American Indian Law Center. Model Tribal Research Code. 1994; Albuquerque, NM: American Indian Law Center. 3rd ed.
- CIHR. Guidelines for health research involving aboriginal people. 2007; Ottawa, Canada: Canadian Institutes for Health Research.
- Fediuk A, Kuhnlein HV. Indigenous peoples & participatory health research. 2003; Geneva, Switzerland: World Health Organization.
- Inuit Tapiriit Kanatami. Negotiating research relationships: a guide for communities. Pimatisiwin. 2003; 1: 17–25.
- Smylie J, Kaplan-Myrth N, McShane K. Indigenous knowledge translation: baseline findings in a qualitative study of the pathways of health knowledge in three indigenous communities in Canada. Health Promot Pract. 2009; 10: 436–46.
- Smylie J, Martin CM, Kaplan-Myrth N, Steele L, Tait C, Hogg W. Knowledge translation and indigenous knowledge. Int J Circumpolar Health. 2003; 63(Suppl 2): 139–43.
- Hanson PG, Smylie J. Knowledge translation for indigenous communities: policy making toolkit. 2006; Indigenous KT Summit Steering Committee.
- Inuit Circumpolar Council. Charter Article 1 – definitions; 2015 [cited 2016 Feb 4]. Available from: http://www.inuitcircumpolar.com/charter--bylaws.html.
- Castleden H, Morgan VS, Lamb C. ‘I Spent The First Year Drinking Tea’: exploring Canadian University Researchers perspectives on community-based participatory research involving indigenous peoples. Can Geogr. 2012; 56: 160–79.
- Fletcher CM. Community-based participatory research relationships with aboriginal communities in Canada: an overview of context and process. Pimatziwin. 2003; 1: 27–62.
- OCAP: Ownership, Control, Access and Possession. Sanctioned by the First Nations Information Governance Committee, Assembly of First Nations. First Nations Centre. 2007; Ottawa, Canada: National Aboriginal Health Organization. 23.
- Chino M, DeBruyn L. Building true capacity: indigenous models for indigenous communities. Am J Public Health. 2006; 96: 596–9.
- Metis Centre, National Aboriginal Health Organization. Principles of ethical Métis research. 2010; Ottawa, Canada: Métis Centre of NAHO. 5.
- National Health and Medical Research Council. Values and ethics: guidelines for ethical conduct in aboriginal and Torres Strait Islander Health Research. 2003; Canberra, Australia: Commonwealth of Australia. 1–27.
- HRC. Guidelines for researchers on health research involving Māori. 2010; Auckland, New Zealand: Health Research Council of New Zealand. 1–52.
- Gesink D, Rink E, Montgomery-Andersen R, Mulvad G, Koch A. Developing a culturally competent and socially relevant sexual health survey with an urban Arctic Community. Int J Circumpolar Health. 2010; 69: 25–37.
- Wilkins R, Uppal S, Finès P, Senécal S, Guimond É, Dion R. Life expectancy in the Inuit-inhabited areas of Canada, 1989 to 2003. Health Rep. 2008; 19: 1–13.
- King M, Smith A, Gracey M. Indigenous Health Part 2: the underlying causes of the health Gap. Lancet. 2009; 374: 76–85.
- Ellison C. Indigenous knowledge and knowledge synthesis, translation and exchange (KSTE). 2014; Prince George, BC: National Collaborating Centre for Aboriginal Health. 1–28.
- National Collaborating Center for Aboriginal Health. Landscapes of First Nations, Inuit, and Métis Health: an environmental scan of organizations. 3rd ed. 2014; Prince George, BC: National Collaborating Centre for Aboriginal Health. 1–91.
- Health Council of Canada. The health status of Canada's First Nations, Métis and Inuit peoples. 2005; Toronto, ON: Health Council of Canada.
- Adelson N. The embodiment of inequity. Can J Public Health. 2005; 96: 45–61.
- Statistics Canada. Aboriginal peoples in Canada: First Nations people, Métis and Inuit. National Household Survey, 2011. 2013; Ottawa, Canada: Statistics Canada. 1–23.
- Jardine C, Furgal C, Garvin T, McGee T. Factors affecting the communication and understanding of health risks in northern aboriginal communities in Canada. Int J Psychol. 2004; 39(5–6): 518.
- Arksey H, O'Malley L. Scoping studies: toward a methodological framework. Int J Soc Res Methodol. 2005; 8: 19–32.
- Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010; 5: 69.
- Awofeso N. Re-defining health: comment on ‘Calling a Spade a Spade: meaningful definitions of health conditions’. Bull World Health Organ. 2005; 83: 802.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006; 3: 77–101.
- Moher D, Liberati A, Tetzlaff J, Altman DG, The Prisma Group. Preferred reporting items for systematic reviews and meta-analysis: the PRISMA statement. PLoS Med. 2013; 6: 1–4.
- Dean LS. Environment and health risk communication pathways in aboriginal communities: Learning from the case of foodweb contaminants and nutrition issues with young Inuit women in Nunatsiavut. [thesis dissertation]. 2009; Peterborough, Ontario: Trent University.
- Yohannes S. Traditional food consumption, anthropometry, nutrient intake and the emerging relationship between Inuit youth and traditional knowledge in a Baffin Island Community. [thesis dissertation]. 2009; Montreal, Quebec: McGill University.
- Kot M. Challenges and opportunities for small community drinking water systems – A knowledge translation perspective. [thesis dissertation]. 2009; Halifax, Nova Scotia: Dalhousie University.
- Pufall EL, Jones AQ, McEwen SA, Lyall C, Peregrine AS, Edge VL. Community-derived research dissemination strategies in an Inuit Community. Int J Circumpolar Health. 2012; 70: 532–41.
- Hamel C. Determinants of participation in an Online Community of Practice (OCoP). [thesis dissertation]. 2009; Ottawa, Ontario: University of Ottawa.
- Counil É, Gauthier MJ, Blouin V, Grey M, Angiyou E, Kauki T, etal. Translational research to reduce trans-fat intakes in Northern Québec (Nunavik) Inuit Communities: a success story?. Int J Circumpolar Health. 2012; 71: 1–7.
- Poole N, Chansonneuve D, Hache A. Improving substance use treatment for First Nations, Métis and Inuit women: recommendations arising from a virtual inquiry project. First Peoples Child Fam Rev. 2013; 8: 1–23.
- Jardine C, Furgal C. Knowledge translation with northern aboriginal communities: a case study. Can J Nurs Res. 2010; 42: 119–27. [PubMed Abstract].
- Tyrrell M. Making sense of contaminants: a case study of Arviat, Nunavut. Arctic. 2006; 59: 370–80.
- Myers H, Furgal C. Long-range transport of information: are Arctic residents getting the message about contaminants?. Arctic. 2006; 59: 47–60.
- Thomas D. Development of a coastal community climate change action plan for Arviat, Nunavut. [thesis dissertation]. 2008; Winnipeg, Manitoba: University of Manitoba.
- Bradshaw C. Sailivik: a place of tranquility. [thesis dissertation]. 2009; Winnipeg, Manitoba: University of Manitoba.
- Durkalec A. Understanding the role of environment for indigenous health: A case study of sea ice as a place of health and risk in the Inuit Community of Nain, Nunatsiavut. [thesis dissertation]. 2013; Peterborough, Ontario: Trent University.
- Martin BD. Palliative care and the Kivalliq region of Nunavut: determinants of programme development and implementation. [thesis dissertation]. 2003; Winnipeg, Manitoba: University of Manitoba.
- Blakney SL. Connections to the land: The politics of health and wellbeing in Arviat, Nunavut. [thesis dissertation]. 2009; Winnipeg, Manitoba: University of Manitoba.
- Harper SL. Weather, water, and infectious gastrointestinal illness in the context of climate change in Nunatsiavut, Canada. [thesis dissertation]. 2009; Guelph, Ontario: University of Guelph.
- Rasmussen D, Guillou J. Developing an Inuit-specific framework for culturally relevant health indicators incorporating gender-based analysis. J Aborig Health. 2012; 8: 24–35.
- Reading J. A global model and national research excellence. Can J Public Health. 2003; 94: 185–9. [PubMed Abstract].
- Brant Castellano M. Ethics of aboriginal research. J Aborig Health. 2004; 1: 98–114.
- Castellano MB, Reading J. Policy writing as dialogue: drafting an aboriginal chapter for Canada's Tri-council policy statement: ethical conduct for research involving humans. Int Indig Policy J. 2010; 1: 1–18.
- Sullivan C. Integrating culturally relevant learning in Nunavut high schools: student and educator perspectives from Pangnirtung, Nunavut, and Ottawa, Ontario. [thesis dissertation]. 2013; Ottawa, Ontario: Carleton University.
- Reeves A, Bull J, Heaslip A, Iskwew GRMI. Indigenizing academia: student reflections on aboriginal health research in Canada. Can J Native Stud. 2014; 34: 185–96.
- Jacob S, Desautels G. Evaluation of aboriginal programs: what place is given to participation and cultural sensitivity?. Int Indig Policy J. 2013; 4: 31.
- Kay-Raining Bird E. A resource kit: to assist speech-language pathologists and audiologists in providing informed services to First Nations, Inuit, and Métis people. Can J Speech-Language Pathol Audiol. 2014; 38: 238–50.
- Mead E, Gittelsohn J, De Roose E, Sharma S. Important psychosocial factors to target in nutrition interventions to improve diet in Inuvialuit communities in the Canadian Arctic. J Hum Nutr Diet. 2010; 23(Suppl 1): 92–9.
- Laidler GJ, Hirose T, Kapfer M, Ikummaq T, Joamie E, Elee P. Evaluating the Floe Edge Service: how well can SAR imagery address Inuit Community concerns around sea ice change and travel safety?. Can Geogr. 2011; 55: 91–107.
- Government of Canada. Harper Government helps tackle tuberculosis in Nunavut; 2012. [cited 2016 Apr 19]. Available from: http://www.cihr-irsc.gc.ca/e/45086.html.
- Reading J, Nowgesic E. Improving the health of future generations: the Canadian Institutes of health research Institute of Aboriginal Peoples’ Health. Am J Public Health. 2002; 92: 1396–400.
- Kovesi T, Giles BL, Pasterkamp H. Long-term management of asthma in First Nations and Inuit children: a knowledge translation tool based on Canadian paediatric asthma guidelines, intended for use by front-line health care professionals working in isolated communities. Paediatr Child Health. 2012; 17: 46–64.
- Ford J, Pearce T, Smit B, Wandel J, Allurut M, Shappa K, etal. Reducing vulnerability to climate change in the Arctic: the case of Nunavut, Canada. Arctic. 2007; 60: 150–66.
- Ebbesson SOE, Laston S, Wenger CR, Dyke B, Romenesko T, Swenson M, etal. Recruitment and community interactions in the GOCADAN study. Int J Circumpolar Health. 2006; 65: 55–64.
- Boyer BB, Mohatt GV, Lardon C, Plaetke R, Luick BR, Hutchison SH, etal. Building a community-based participatory research center to investigate obesity and diabetes in Alaska Natives. Int J Circumpolar Health. 2005; 64: 281–90.
- Boyer BB, Mohatt GV, Pasker RL, Drew EM, McGlone KK. Sharing results from complex disease genetic studies: a community based participatory research approach. Int J Circumpolar Health. 2007; 66: 19–30.
- Caldwell JY, Davis JD, DuBoise B, Echo-Hawk H, Erickson JS, Goins RT. Culturally competent research with American Indians and Alaska Natives: findings and recommendations of the first symposium of the work group on American Indian research and program evaluation methodology. Am Indian Alsk Native Ment Health Res. 2005; 12: 1–20.
- Derry KW. New Risks, New strategies: Greenlandic Inuit responses to climate change. [thesis dissertation]. 2011; Fort Collins, Colorado: Colorado State University.
- Carry CL, Clarida K, Rideout D, Kinnon D, Johnson RM. Qanuqtuurniq-finding the balance: an IPY television series using community engagement. Polar Res. 2011; 30: 1–10.
- Mikhailovich K, Morrison P, Arabena K. Evaluating Australian indigenous community health promotion initiatives: a selective review. Rural Remote Health. 2007; 7: 81–7.
- Canadian Institutes of Health Research. Innovation in action: knowledge translation strategy 2004–2009. 2004; Ottawa, Canada: Canadian Institutes of Health Research. 14.
- Lomas J. Using ‘Linkage and Exchange’ to move research into policy at a Canadian Foundation. Health Aff. 2000; 19: 236–40.
- Zavala M. What do we mean by decolonizing research strategies? Lessons from decolonizing, indigenous research projects in New Zealand and Latin America. Decolonization Indigeneity Educ Soc. 2013; 2: 55–71.
- Castleden H, Garvin T. Huu-ay-aht First Nation. Modifying photovoice for community-based participatory indigenous research. Soc Sci Med. 2008; 66: 1393–405.
- Humphery K. Dirty questions: indigenous health and ‘Western Research. Aust N Z J Public Health. 2001; 25: 197–202.
- Cunsolo Willox A, Harper SL, Edge VL. ‘My Word’ digital media and storytelling lab, Rigolet Inuit community government. Storytelling in a digital age: digital storytelling as an emerging narrative method for preserving and promoting indigenous oral wisdom. Qual Res. 2012; 13: 127–47.
- Wilson S. Progressing toward an indigenous research paradigm in Canada and Australia. Can J Native Educ. 2003; 27: 161.
- McShane KE, Smylie JK, Hastings PD, Prince C. Evaluation of the acceptability of a CD-ROM as a health promotion tool for Inuit in Ottawa. Int J Circumpolar Health. 2013; 72: 1–9.
- Jack SM, Brooks S, Furgal CM, Dobbins M. Knowledge transfer and exchange processes for environmental health issues in Canadian aboriginal communities. Int J Environ Res Public Health. 2010; 7: 651–74.
- Sullivan M, Kone A. Researcher and researched – community perspectives: toward bridging the Gap. Health Educ Behav. 2001; 28: 130–49.
- Koster R, Baccar K, Lemelin R. Moving from research on, to research with and for indigenous communities: a critical reflection on community-based participatory research. Can Geogr. 2012; 56: 195–210.
- Smith L. Decolonizing methodologies: research and indigenous peoples. 1999; New York: Zed Books.
- Denzin N, Lincoln Y, Smith L. Handbook of critical and indigenous methodologies. 2008; Thousand Oaks, CA: Sage. 624.
- Hendry PM. The future of narrative. Qual Inq. 2007; 13: 487–98.
- van der Velde J, Williamson DL, Ogilvie LD. Participatory action research: practical strategies for actively engaging and maintaining participation in immigrant and refugee communities. Qual Health Res. 2009; 19: 1293–302.
- Jardine C, Hrudey S, Shortreed J, Craig L, Krewski D, Furgal C, etal. Risk management frameworks for human health and environmental risks. J Toxicol Environ Health. 2003; 6: 569–641.
- Dodman D, Mitlin D. Challenges for community-based adaptation: discovering the potential for transformation. J Int Dev. 2010; 96: 10–4.
- Sherman MH, Ford J. Stakeholder engagement in adaptation interventions: an evaluation of projects in developing nations. Clim Policy. 2014; 14: 417–41.
- Ford J, Stephenson E, Cunsolo Willox A, Edge VL, Farahbakhsh K, Furgal C, etal. Community-based adaptation research in the Canadian Arctic. WIREs Clim Change. 2016; 7: 175–191. doi: http://dx.doi.org/10.1002/wcc.376.
- Schnarch B. Ownership, Control, Access, and Possession (OCAP) or self-determination applied to research: a critical analysis of contemporary First Nations research and some options for First Nations communities. J Aborig Health. 2004; 1: 80–95.
- Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, Social Sciences and Humanities Research Council. Chapter 9: Research involving the First Nations, Inuit and Métis peoples of Canada. In: Tri-Council policy statement: ethical conduct for research involving humans. 2014; Ottawa, Canada: Government of Canada. 109–38.
- Kelley A, Belcourt-Dittloff A, Belcourt C, Belcourt G. Research ethics and indigenous communities. Am J Public Health. 2013; 103: 2146–52.
- Champion VL, Skinner CS. Glanz K, Rimer BK, Viswanath K. Health belief model. Health behavior and health education: theory, research and practice. 4th ed. 2008; San Francisco, CA: Wiley. 45–66.
- Ford T, Rasmus S, Allen J. Being useful: achieving indigenous youth involvement in a community-based participatory research project in Alaska. Int J Circumpolar Health. 2012; 71: 1–7.
- Ulturgasheva O, Wexler L, Kral M, Allen J, Mohatt GV, Nystad K, etal. Pathways to adulthood project. J Community Engagem Scholarsh. 2011; 4: 50–9. [PubMed Abstract] [PubMed CentralFull Text].
- Wu L, Ahn H. Making sense of conflicting health information: an exploratory study. Proc Am Soc Inform Sci Technol. 2010; 47: 1–9.
- Wray RJ, Becker SM, Henderson N, Glik D, Jupka K, Middleton S, etal. Communicating with the public about emerging health threats: lessons from the pre-event message development project. Am J Public Health. 2008; 98: 2214–22.