Abstract
Amebic colitis is common in tropics, usually presenting with variable and non-specific symptoms. Amebomas occur rarely, usually in cecum and ascending colon, when they can masquerade as colon carcinoma. This report describes the case of a 27-year-old male who presented with right abdominal mass. Radiological examination prompted us to the differential diagnosis of ameboma and he was treated with metronidazole and broad-spectrum antibiotics for two weeks. Amebic colitis should be considered as a possible diagnosis when dealing with right-sided abdominal mass.
1 Case representation
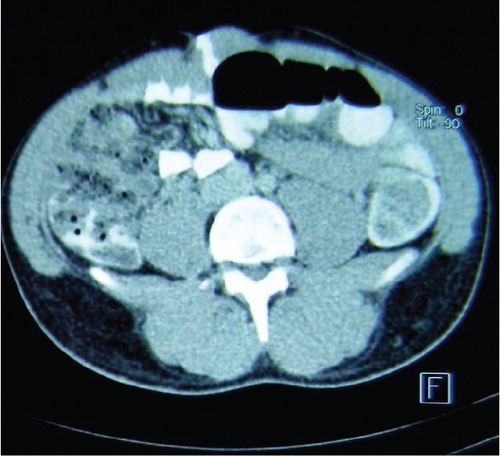
A 27-year-old man was admitted to the surgical department with right abdominal mass of 10 days’ duration associated with abdominal distension, fever, and constipation. There was no preceding diarrhea or bleeding per rectum. His medical history was unremarkable. Physical examination revealed a mildly tender right abdominal mass. Digital rectal examination was normal. A working diagnosis of colon cancer was made. Abdominal X-ray revealed dilated small bowel loops (), while blood tests showed marked leucocytosis (white cell count 15×103/dL). Liver function test and tumor markers (alpha-feto protein and chorioembryonic antigen) were normal. Ultrasound showed a complex bowel mass in relation to cecum and ascending colon with typical ‘whorl’ appearance (). Computed tomographic (CT) scanning of the abdomen confirmed an ascending colon mass with inflammatory changes (). No focal liver lesion was detected. Radiological findings prompted the surgeons to investigate for amebic etiology and ameboma was considered a more probable diagnosis. Stool microscopic examination revealed ova of Entameba histolytica thereby confirming the diagnosis of ameboma and the patient was put on broad spectrum antibiotic (Augmentin 1 gm) and metronidazole. His general condition improved dramatically over 72 hours, when he became afebrile and the abdominal mass showed signs of regression. A follow-up CT scan after two weeks of treatment showed almost complete resolution ().
Figure 1. Abdominal radiograph shows multiple air-fluid levels in small intestine.
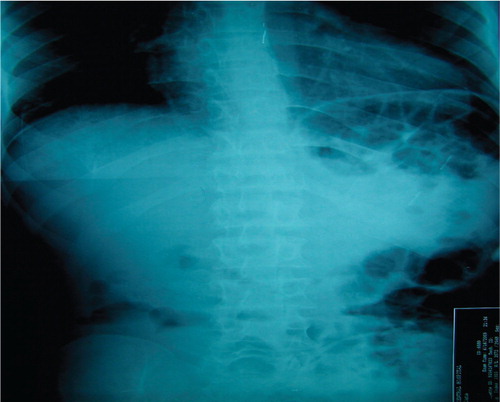
Figure 2. Ultrasound showed the typical ‘target’ sign.
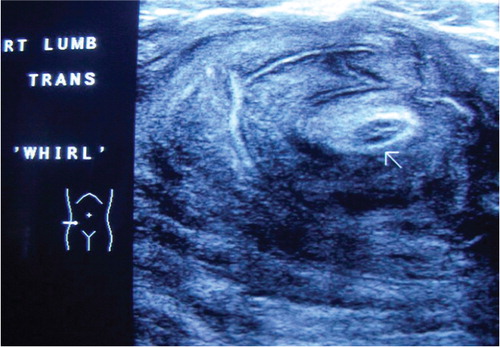
Figure 3. a and b: Axial (a) and reformatted coronal; (b) CT scan images show the concentric irregular colonic wall thickening with multiple mesenteric nodes.

Figure 4. Two weeks post-treatment CT scan shows dramatic resolution of the right-sided colonic mass.
2 Diagnosis
Colonic ameboma.
3 Discussion
Amebiasis is an important global problem especially in the tropical and subtropical regions. Trophozoites of E. histolytica are responsible for the invasive disease. Intestinal invasion results in ‘flask-shaped’ ulcers. Rarely, patients with long standing or partially treated infections develop tumors, exophytic, cicatricial, and inflammatory masses known as ‘amebomas.’ Amebomas occur in only 1.5% of patients’ with amebiasis Citation1. The differential diagnosis includes Crohn's disease and appendicular abscess in younger individuals, and colon cancer and diverticulitis in the elderly Citation2. Because ameboma is an uncommon condition, it is often usually discovered only at laparotomy Citation3. Only a few cases of colonic amebomas have been reported where the diagnosis was made on colonoscopic biopsy and successfully treated with pharmacotherapy Citation3. Although plain radiograph of abdomen and ultrasound cannot differentiate between colon cancer and ameboma, CT scan plays a crucial role in clinching the diagnosis. CT scan not only provides information about the lumen and colonic wall, it also provides valuable information about the pericolic space which is critical for differentiation between malignancy and ameboma. In our center, we always perform the CT scan with rectal contrast or air insufflation which aids in the demarcation of colon wall and lumen from pericolic space. In this patient, although the clinical presentation was non-specific, the radiological findings prompted us to do a stool microscopic examination which revealed ova of E. histolytica thereby confirming the diagnosis of ameboma. This spared the patient unnecessary surgery. Metronidazole still remains the mainstay of treatment for amebiasis Citation4. Surgery is rarely required and is indicated only in cases of diagnostic uncertainty or any arising complications such as toxic megacolon. Pai had reviewed 11 patients with suspected tuberculosis or inflammatory bowel disease where amebiasis was suggested in the differential diagnosis in only three cases Citation5. Histopathologic diagnosis of amebic colitis was made in all 11 patients. He concluded that amebic colitis must be included in the differential diagnosis of all patients with suspected inflammatory bowel disease and tuberculosis.
In conclusion, amebiasis should always be considered in the differential diagnosis in patients presenting with colonic mass.
3.1 Consent
Written informed consent was obtained from the patient for publication of the features and accompanying images.
4 Conflict of interest and funding
The authors have not received any funding or benefits from industry to conduct this study.
References
- Misra SP, Misra V, Dwivedi M. Ileocaecal masses in patients with amobic liver abscess: etiology and management. World J Gastroenterol. 2006; 12: 1933–6.
- Majeed SK, Ghazanfar A, Ashraf J. Caecal ameboma simulating malignant neoplasia, ileocecal tuberculosis and Crohn's disease. J Coll Physicians Surg Pak. 2003; 13: 116–7.
- Sharma D, Patel LK, Vaidya VV. Ameboma of ascending colon with multiple liver abscesses. J Assoc Physicians India. 2001; 49: 579–80.
- Powell SJ, MacLeod I, Wilmot AL, Elsdon-Dew R. Metronidazole in amoebic dysentery and amoebic liver abscess. Lancet. 1966; 2: 1329–31.
- Pai SA. Amebic colitis can mimic tuberculosis and inflammatory bowel disease on endoscopy and biopsy. Int J Surg Pathol. 2009; 17: 116–21.