Abstract
Urinary bladder catheter encrustations are known complications of long-term urinary catheterisation, which is commonly seen in clinical practice. These encrustations can impede deflation of the balloon and therefore cause problems in the removal of the catheter. The options in managing an encrusted and incarcerated urinary bladder catheter include extracorporeal shock wave lithotripsy and lithoclast. We describe here another technique of dealing with a stuck and encrustated catheter, via direct crushing of the encrustations with a rigid cystoscope inserted through a suprapubic cystostomy tract.
Introduction
Complications associated with the use of urinary catheters include infection, bladder spasms, catheter encrustations, and retained catheters. This is more so with long-term catheter usage. Even with sophisticated and improved nursing care, these issues still cause much debility and inconvenience to the patient. Catheter encrustations are frequently encountered and can be challenging to the attending urologist managing them. These can be classified as either intraluminal or extraluminal. The encrustations on the outside surface of the catheter can break away into the bladder, forming a focus for bladder calculi and infections on catheter removal. Prompt removal of the catheter and the encrustations are paramount in preventing further complications to the patient. Encrustation can impair deflation of the balloon and, therefore, making it impossible to remove the catheter.
Case report
A 58-year-old man who has had lower urinary tract symptoms for a year, developed acute urinary retention, and was subsequently catheterised. On examination, his prostate was enlarged. Trial of void was attempted with alpha-blocker medication (alfuzosin) but failed. He was then planned for transurethral resection of the prostate (TURP) but it was postponed a few times due to active urinary tract infection. While waiting for his surgery, he had a 2-weekly change of his catheter.
During the last change of catheter, it was found to be stuck and the balloon of the catheter could not be deflated. An ultrasound was done but the balloon was not seen and the tip of the catheter was seen to be calcified. There was also surrounding haematoma and clots. An attempt to puncture the balloon with a spinal needle under ultrasound guidance was attempted but failed. The tip of the catheter with the balloon was stuck at the base of the bladder neck. Attempts to push the balloon and the tip further into the bladder failed. A suprapubic puncture was made under ultrasound guidance and a size 16 French (F) urinary bladder catheter was inserted. The track was allowed to mature for 2 weeks.
After 2 weeks, a guide wire was inserted through the suprapubic catheter into the bladder. The tract was then dilated with dilators from the percutaneous lithotomy set, till it reached size 24 F. A size 22 F rigid cystoscope was then introduced into the bladder with the guide wire in place (). A stone crushing forceps was introduced and the encrustations were successfully removed (). The balloon was deflated and the catheter was removed via the urethra (). The patient made an uneventful recovery and was discharged the following day with a date given for TURP.
Fig. 1. A guide wire is inserted through the suprapubic catheter tract into the bladder followed by a 22 F rigid cystoscope.
Fig. 2. The encrustation seen from the rigid cystoscope (arrow).
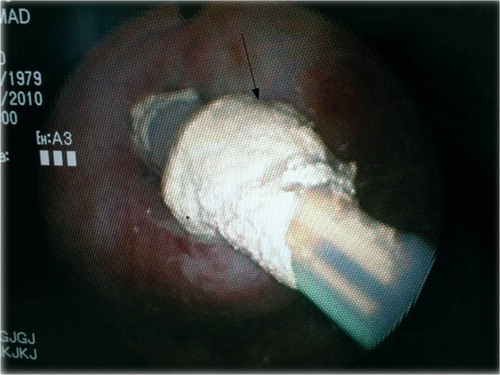
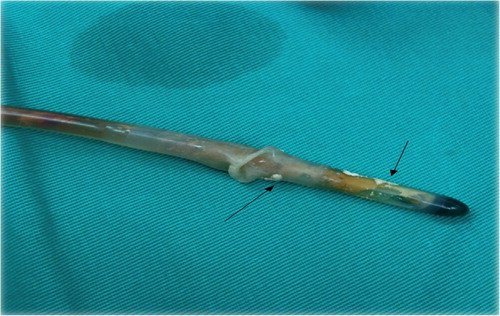
Fig. 3. The catheter tip after removal. The residual encrustations can still be seen at the balloon (arrow).
Discussion
Approximately 10 to 15% of patients admitted to the hospital receive a urinary catheter. Complications associated with the use of urinary catheters include infection, bladder spasms, catheter encrustations, and retained catheters Citation1.
Encrustations can occur either in the lumen of the catheter or extraluminally. This can possibly result in blockage or retention of the catheter. The main cause of catheter encrustation is infection by urease-producing organisms, particularly Proteus mirabilis Citation2Citation3. These organisms colonise the catheter, forming a bio film Citation4Citation5. The bacterial urease generates ammonia from the urea, and the urine becomes alkaline. Under these conditions, crystals of calcium and magnesium phosphate are formed and a crystalline bio film develops, which eventually blocks the flow of urine from the bladder Citation6Citation7Citation8. The main route of infection of the catheterised urinary tract is through the urethra along the outer surface of the catheter. Infections, however, can occur from contaminants in the urine drainage bag ascending through the catheter lumen into the bladder Citation9.
Patients with a retained encrusted Foley catheter suffer from pain in the genitalia, bladder irritability causing spasms and urinary leakage, besides the great discomfort caused by urinary retention. The removal of an encrusted catheter is not only painful, but can cause trauma to the urethra. Encrustation can lead to significant damage to the delicate urethral wall while the catheter is being removed resulting in bleeding, scarring, urethral strictures, and infection Citation10.
The management of a retained Foley catheter with encrustation and stone formation around the bulb of the catheter is a complicated problem due to the resistance offered by the overlying calculus encrustation. In such circumstances, the catheter can be removed via suprapubic cystotomy.
Since any technique used to remove the catheter must not disturb the patient or create any additional morbidity, minimally invasive techniques have been preferred over these procedures. Canby-Hagino et al. Citation11 described using intraluminal pneumatic lithotripsy (Swiss lithoclast) for the removal of encrusted urinary catheters. In each case a pneumatic lithotripsy probe was inserted into the lumen of the catheter and advanced in a jackhammer-like fashion. This technique resulted in disruption of the intraluminal encrustations and straightening of the tubes so that they were removed in an atraumatic manner. Even though they recommended its use as a first-line treatment of removing encrusted urinary catheters, its efficacy is not known in cases of extraluminal encrusted urethral catheters.
Extracorporeal shock wave lithotripsy (ESWL) has been utilised in the treatment of the bladder stones. Borrowing this principle, Kunzman et al. Citation12 has even used ESWL to fragment the stone-like encrustation over the retained Foley catheter balloon. After removal of the encrustation, the balloon can be deflated manually or, if it is stuck, a spinal needle can be used to puncture the balloon with ultrasound guidance.
In this patient, we did not attempt ESWL because the catheter could not be pushed into the bladder further. The balloon and the encrustation were stuck at the bladder neck. Therefore, it was shielded by the pelvic bones and the shockwaves would not be able to break-up the encrustation. The lithoclast, on the other hand, could not be introduced via the urethra because it was difficult to negotiate the lithoclast through the urethral lumen with the urinary catheter in place, surrounding the haematoma and enlarged prostate.
Since we could not use the ESWL or lithoclast, we resorted to first inserting a suprapubic catheter. After the suprapubic track had matured (about 2 weeks), we introduced a cystoscope after dilatation of the track, done under spinal anaesthesia. A stone-crushing forceps was then used to fragment the encrustations. After removing the encrustations, the catheter was free to be pushed into the bladder, exposing the balloon. The balloon was easily punctured with a spinal needle under ultrasound guidance. With this, the catheter could be easily removed. To date, this method has not been described in the literature.
Conclusion
The options for removal of an encrusted and stuck urinary catheter include using the ESWL or introducing the lithoclast via the urethra to fragment the encrustations. This would, however, need a catheter that is not stuck at the bladder neck. The technique we described is another option to overcome this problem. It has been shown to be applicable and safe.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Related Research Data
References
- Shapiro AJ, Soderdahl DW, Stack RS, North JHJ. Managing the nondeflating urethral catheter. J Am Board Fam Pract. 2000; 13: 116–9.
- Kunin CM. Blockage of urinary catheters: role of microorganisms and constituents of the urine on formation of encrustations. J Clin Epidemiol. 1989; 42: 835–42.
- Mobley HLT, Warren JW. Urease-positive bacteriuria and obstruction of long-term catheters. J Clin Microbiol. 1987; 25: 2216–7.
- Stickler DJ, Ganderton L, King J, Nettleton J, Winters C. Proteus mirabilis biofilms and the encrustation of urethral catheters. Urol Res. 1993; 21: 407–11.
- Stickler DJ, Morris NS, Moreno MC, Sabubba N. Studies on the formation of crystalline bacterial biofilms on urethral catheters. Eur J Clin Microbiol Infect Dis. 1998; 17: 649–52.
- Choong SKS, Hallson P, Whitfield HN, Fry CH. The physicochemical basis of urinary catheter encrustation. BJU Int. 1999; 83: 770–5.
- Cox AJ, Hukins DW, Sutton TM. Infection of catheterised patients: bacterial colonization of encrusted Foley catheters shown by scanning electron microscopy. Urol Res. 1989; 17: 349–52.
- Morris NS, Stickler DJ, McLean RJ. The development of bacterial biofilms on indwelling catheters. World J Urol. 1999; 17: 345–50.
- Stamm WE. Catheter-associated urinary tract infections: epidemiology, pathogenesis and prevention. Am J Med. 1991; 91: 65S–71S.
- Getliffe KA, Hughes SC, Le Claire M. The dissolution of urinary catheter encrustation. Br J Urol Int. 2000; 85: 60–4.
- Canby-Hagino ED, Caballero RD, Harmon WJ. Intraluminal pneumatic lithotripsy for the removal of encrusted urinary catheters. J Urol. 1999; 161: 2058–60.
- Kunzman SA, Srinadh ES, Lala SM, Albusaidi Q. Management of retained encrusted urethral catheter with extracorporeal shockwave lithotripsy. Indian J Urol. 2002; 19: 83–4.