
In mammals, gender is determined at conception and male births occur slightly in excess (Citation1). The male to female ratio of live births is technically incorrectly referred to as M/F as this is given as male divided by total births, and it is expected to approximate 0.515 (Citation1).
A declining M/F has been observed in many industrialised countries since 1950 as the more fragile male foetus may be spontaneously aborted at a higher rate than the more robust female foetus when exposed to hypothetical deleterious environmental factor/s (Citation2). Stress has been shown to decrease M/F (Citation3), while long-duration warfare (such as the World Wars) increases it (Citation4). Adverse environmental factors or traumatic experiences that affect entire populations have both been shown to lower M/F. For example, M/F declines after warfare (Citation5), earthquakes, and a multiplicity of environmental disasters (Citation6). It appears that such events promote stressed pregnant women to spontaneously abort male foetuses to a greater extent than female foetuses (Citation7). M/F has therefore been proposed as a potential surrogate sentinel health indicator (Citation8).
There is only one extant study which deals with M/F in countries located in the Middle East (Citation9). This studied Iran and showed that M/F declined slowly between 1976 and 1981, stabilised, and then rose up to 1999. M/F decreased significantly during periods of warfare when compared with pre-war. There was also a decrease post-war when compared with pre-war.
This study identifies secular trends in M/F in the Middle East from a World Health Organization (WHO) dataset that includes the past 60 years. This dataset has been utilised extensively in order to study M/F in South America (Citation10), Asia (Citation11), and selected parts of Europe (Citation12, Citation13).
The only reliable datasets available were those of Israel, Egypt, and Kuwait. Chi square tests (including trend testing) were applied. The results are shown in .
Fig. 1 M/F trends for Israel, Egypt, and Kuwait.
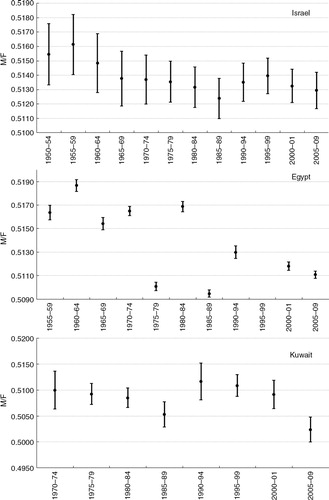
There were 34,644,020 live births available for analysis. Israel displayed a significant decline in M/F from 1950 to 1989 (x trend=10.1, p=0.0014). There was one outlier value in 1981, when M/F dipped significantly. M/F then appeared to have stabilised.
Egypt also reported an overall (albeit less smooth) decline in M/F from 1955 to 2012 (x trend=7664.108, p<0.0001). There was also a single outlier value in 1979, when M/F dipped significantly.
Kuwait exhibited a significant decline in M/F from 1972 to 1987 (x trend=7.9, p=0.005). M/F then increased sharply and significantly from 1985–87 to 1993–95 (data missing for 1988–92) and this increase is statistically significant (x=7.9, p=0.0005). M/F then declined again during 1993–2009 (x trend=15.9, p<0.0001).
M/F has been shown to be declining in Europe and in North America (Citation14), and the results obtained in this study are in accordance with this trend.
In 1978, Egypt and Israel signed the Camp David Accords, which resulted in the signing of the Israel–Egypt Peace Treaty in the following year. One wonders whether these events are somehow related to the Egyptian M/F dip in 1979.
In 1981, Israeli forces destroyed a nuclear reactor that was still under construction near Baghdad. One wonders whether the spectre of war provided sufficient stress to cause a dip in M/F in Israel.
In conclusion, this study shows that M/F in this region, for the countries available for study, is in decline, similar to the situation in Europe and North America (Citation14).
Department of Paediatrics
Mater Dei Hospital
L-Imsida, Malta
Email: [email protected]
Conflict of interest and funding
The author has not received any funding or benefits from industry or elsewhere to conduct this study.
Acknowledgements
Mie Inoue and Gauden Galea from the World Health Organization.
References
- James WH. The human sex ratio. Part 1: a review of the literature. Hum Biol. 1987; 59: 721–52. [PubMed Abstract].
- James WH. Evidence that mammalian sex ratios at birth are partially controlled by parental hormone levels around the time of conception. J Endocrinol. 2008; 198: 3–15.
- Catalano RA. Sex ratios in the two Germanies: a test of the economic stress hypothesis. Hum Reprod. 2003; 18: 1972–5.
- Houdaille J. Le rapport de masculinite. Population et Societes. 1973; 61: 1–3.
- Zorn B, Sucur V, Stare J, Meden-Vrtovec H. Decline in sex ratio at birth after 10-day war in Slovenia: brief communication. Hum Reprod. 2002; 17: 3173–7.
- Lyster WR. Altered sex ratio after the London smog of 1952 and the Brisbane flood of 1965. J Obstet Gynaecol Br Commonw. 1974; 81: 626–31.
- Byrne J, Warburton D. Male excess among anatomically normal fetuses in spontaneous abortions. Am J Med Genet. 1987; 26: 605–11.
- Davis DL, Gottlieb MB, Stampnitzky JR. Reduced ratio of male to female births in several industrial countries: a sentinel health indicator?. JAMA. 1998; 279: 1018–23.
- Ansari-Lari M, Saadat M. Changing sex ratio in Iran, 1976–2000. J Epidemiol Community Health. 2002; 56: 622–3.
- Grech V. Secular trends in sex ratios at birth in South America over the second half of the 20th century. J Pediatr (Rio J). 2013; 89: 505–9.
- Grech V. Secular trends and latitude gradients in sex ratios at birth in Asia over the past sixty years. Pediatr Int. 2013; 55: 219–22.
- Grech V. Sex ratios at birth in the British Isles over the past sixty years. Eur J Pediatr. 2013; 172: 525–8.
- Grech V. Declining male births in Germany before and after reunification. Turk J Pediatr. 2013; 55: 300–3. [PubMed Abstract].
- Grech V, Vassallo-Agius P, Savona-Ventura C. Secular trends in sex ratios at birth in North America and Europe over the second half of the 20th century. J Epidemiol Community Health. 2003; 57: 612–15.