
Abstract
Libya is a vast country situated in North Africa, having a relatively better functioning economy with a scanty population. This article is the first known attempt to review the current state of oral health care in Libya and to explore the present trends and future challenges. Libyan health system, oral health care, and human resources with the present status of dental education are reviewed comprehensively. A bibliographic study of oral health research and publications has been carried out. The results point toward a common indicator that oral health–related research is low. Strategies have to be developed to educate the medical and dental professionals, to update the current curriculum and enable the system to be competent in all aspects of oral health care management.
The Arab Spring had brought about tremendous and unexpected political changes in Libya and elsewhere in the Middle East and North Africa (MENA) region. Libya is an oil-rich economy and had been a significant oil exporter over decades. The total estimated population in 2012 was 5.922 million (Citation1). It spends 4% of its GDP on health (Citation2). Its major cities are Alzawia, Benghazi, Derna, Musrata, Sabha, Sirte, and Tripoli. The majority of the Libyan population lives in cities located on its Mediterranean coastline. The country has considerably vast investments in the health sector. Libya had a human development index of 0.76 in 2010; it stands 53rd among the listed nations and was classified as a high human development country in the MENA region. However, it also has a poverty rate of 21.6% due to considerable economic inequality (Citation3).
WHO has defined health as a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity (Citation4). Complete health and wellness is merely impossible without oral health. The oral health care system in Libya consists of the public and private sectors, which include the majority of dentists. Public dental clinics deliver simple oral examinations, scaling, tooth extractions, and dental fillings. No reports have qualitatively or quantitatively evaluated the functioning of the present Libyan oral health care system on a national level.
This paper is the first attempt known to the authors to review the Libyan health system in relation to oral health in Libya, its present status, future directions, and challenges.
Libyan health system, oral health care, and human resources
Libya has 25 specialized hospitals, 18 central hospitals, 21 general hospitals, 32 rural hospitals, with a total of 96 public hospitals and 1,424 primary health care facilities. Many of the general, rural hospitals and primary health care facilities have dental clinics attached to them (Citation5). Hospitals in Libya are autonomous bodies by law. The designing and development of oral health services in Libya has been carried out with little evidence of the dental needs of the population, as data are sparse. The Health Ministry provides dental health services to people of all ages through the public dental clinics with dental health services generally spread throughout the cities. The main treatments are minor oral surgery, tooth scaling, and restorations with very little development of preventive services. For a long time, populations decided to seek treatment only when they noticed symptoms, contrary to preventing disease before its occurrence. Unfortunately, government expenditure in respect to oral health follows this outdated model and it targets on diagnosis of and treatment for oral and dental diseases rather than on oral health prevention programs (Citation6). Every procedure involving basic oral treatment such as dental extractions, dental restorations of both amalgam and anterior tooth coloring are offered free in the public oral health sector. Public schools employ dentists for providing primary dental treatments and dental education. Impressively, population access to local health services for both rural as well as urban populations during 1999–2012 has remained 100%. Furthermore, six dentists per 10,000 persons by 2012 were present in Libya (Citation7).
Dental caries and periodontal diseases are the most common oral ailments and the major causes of tooth loss. Libya is one of the most arid countries in the world, yet potable water is available across the country. Water fluoridation is a primary prevention mechanism employed against dental caries across the globe. There is a steady rise in the use of bottled water in Libya. A clear agenda or scheme that could oversee water fluoridation is lacking. With urbanization on the rise, increasingly westernized food intake (Citation6) and a lack of primary preventive measures in place, Libya could see a rise in dental caries and related ailments. This could burden its already ailing health care system.
Periodontal diseases are widely prevalent in the human population worldwide. They, along with dental caries, encompass the common dental ailments of any given human population. Dental plaque is the primary cause of both dental caries and general periodontal diseases. Oral hygiene is the most advised primary prevention for removal of dental plaque. Insufficient data exists with regard to dental caries and periodontal disease prevalence in the Libyan population. Available data also suggest that a significant percentage of the population does not practice basic oral hygiene (Citation8).
MENA has also seen a sharp rise in HIV cases (Citation9). This increase is compounded by a lack of security and an increase in the availability of injectable drugs, which could put the dental health care workers – a high-risk profession – at an even greater risk. A strategy to evaluate the knowledge, know the attitudes of dentists and other oral health care workers toward such patients and to impart and inculcate among them necessary working knowledge and attitudes about this unexpected and sudden rise is a matter of grave urgency which has not been addressed in Libya at governmental level.
Education
Education is the cornerstone of development and the hallmark of intellectual renaissance, and Libya recognizes this. There are 12 government-run universities in addition to two private ones (Citation10). A good portion of the budget is directed toward education. The education provided by the public universities is free. A considerable number of students are given scholarships for postgraduate and doctorate studies in universities of their choice and this process has been in place for over a decade. The public universities’ dental faculties at Benghazi, Gariyan-Zintan, Misurata, Sebha, Sirte, Tripoli, Zawia-Surman, Zliten, as well as the private universities of LIMU in Benghazi and At-Tahadi University in Tripoli, offer bachelor degree programs. A bachelor degree in dental surgery is offered to the students on completion of the course. Surprisingly, the number of colleges which offer courses as dental auxiliaries is small. In the past few years, to satisfy the population, politicians have exponentially hiked the intake of both medical and dental colleges. The Tripoli dental faculty admits up to 1,000 new students per year, while other colleges also admit relatively large numbers of students. These numbers overburden the education system and, in due course, may have a negative impact on the labor market of private dental practice. Libya is a large country geopolitically; hence, it may require a considerable number of dental faculties. The dental faculties act as centers for learning and professional interaction. They also cater for the quality treatment needs of the local and regional populations. However, lack of teaching staff, excessive admission of students beyond the capacity and means of the faculty, shortcut approaches to education and a decade of abandoning English language education at the school level has made the Libyan medical and dental health education decay. The students enrolling for the dental schools in the country should be strictly on merit basis, should be given a thorough knowledge of their medium of instruction-English and the huge gap between the student–teacher ratio should be reduced drastically to overhaul and make the oral and dental health education healthy. The number of new admissions in dental faculties across the country should be based on the needs and requirements of the population. An open policy, a culture of dialogue in matters of health education among the MENA region countries, a single and unified, innovatively and meticulously tailor-made syllabus for the whole MENA region will be of great benefit. The level and proficiency of clinical skills taught to the oral health students may vary at least to some degree among different dental schools and among various students of the same school. However, it is a necessity that future dentists, dental specialists, dental health care auxiliaries and the dental health care workers should be able to communicate with other team members in relation to treatment planning and patient-related problem solving and should be of innovative worth (Citation11). They should also be able to carry out oral health research in Libya and handle an exponentially rising scientific knowledge pertaining to oral health (Citation12). The universities across the country should be made to have a single agreed upon curriculum and a uniform system of examination. The curriculum designed should make a consolidated effort to highlight the importance of understanding research, its design, the types of research papers, their structure and basic statistical terminologies. The graduate student should be trained to cope with the rising knowledge and be equipped with necessary skills to incorporate the new research findings into the clinical care of his/her patients (Citation13).
Oral health research and publications – the recent present
Research is the backbone of development and progress. It is worth noting that the scientific production of the MENA is low in general, and that of Libya is extremely low (Citation14–Citation16). Several nations conduct regular cross-sectional studies on representative samples of their population to assess the health needs of their respective populations. The knowledge of the prevalence and severity of disease is vital in developing and planning of public health policies and their implementation. Nevertheless, in the case of oral health status of the Libyan population, there is a general paucity in literature.
To study and investigate all of the research that emanated from Libya, both indexed and non-indexed, was beyond the scope of this review. Multiple descriptors were searched in PubMed, such as Libya, Oral health in Libya, and so on. The searches were limited to the past decade from November 2003 to November 2013, oral health–related research work carried out in Libya and work done relating to oral health in Libya was included. We limited our search within PubMed for the sake of convenience. We also limited ourselves to original research and review articles, as the number of case reports was too small to add value. The searched material was refined and handpicked with an eye on oral research that was relevant to Libya.
Discussion
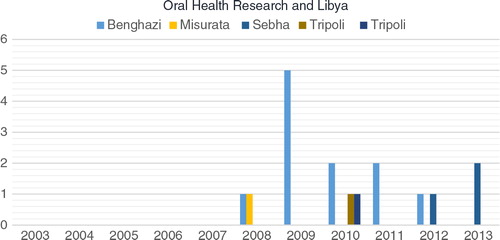
Our study of the research on oral health over the past decade from public and private universities of Libya showed low research productivity. Benghazi University – formerly known as the Garyonus University and Arab Medical University – had a lead in research productivity, followed by Sebha University. When comparing the dental faculty staff numbers and the oral health–related published research, Sebha University is far ahead of Benghazi University. Our search results are in complete agreement with Benamer et al. (Citation15, Citation39) who observed that Libya was lagging behind its peers in biomedical research publications and that the published scholarship of Libyan medical schools and, in our case, the Libyan dental schools, is extremely low and that only a few academic staff have a handful of publications listed in PubMed.
A segregation of authors, based on their nationality was not carried out, since a thorough bibliometric study was not within the scope of this review. Our search results also noted a pattern of no longitudinal studies, no multi-center trails, just a review, almost no clinical studies, and very few case reports over a 10-year period. The ministry of higher education, the policy makers and the dental university faculties are all responsible in their capacities for this poor state of Libyan University research output (Graph I). Nevertheless, in our view, the most important thing is that Libya needs an urgent policy review. It needs a mechanism to support, encourage and appreciate its honest and hardworking scientific elite to develop a culture of progress. Having said that, at present Libya has low research productivity, but we acknowledge that this country has a huge untapped potential.
Graph I. Libyan dental faculties and oral health–related research.
Conclusion and recommendations
Libya has a relatively well-functioning economy, a good literacy rate and a large segment of its population is young. Hence, it has a remarkable potential for growth and development. The authorities should holistically look forward with courage, and develop and establish sensible, stable and tailor-made policies for furthering the health of their general population. Achieving this by proper evaluation of the existing public health system and health education system, and improving its efficiency with proper utilization of available resources is the only way forward. The government should encourage and involve the oral health care researchers and efficient professionals to develop proposals and plans of relevance, to evaluate the oral and dental status and needs of the general population and reduce the prevalence of dental caries and periodontal disease. This will bring a positive trend and have a significant beneficial impact on the overall oral health of the population. The dental faculties should introspectively look at their poor research performance, and develop mechanisms to increase their productivity. The brands that market their oral health care products also have a reasonable responsibility to invest in oral health research in Libya.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
References
- World Health Organization (2013). Demographic, social and health indicators for countries of the eastern Mediterranean [monograph on the Internet]. WHO. [downloaded 2013 November 28]. Available from: http://applications.emro.who.int/dsaf/EMROPUB_2013_EN_1537.pdf.
- World Health Organization. Libya. WHO. 2013. Available from: http://www.emro.who.int/countries/lby/index.html [cited 28 November 2013]..
- World Health Organization. About Libya. United Nations Development Programme. 2013. Available from: http://www.undp.org/content/libya/en/home/countryinfo/ [cited 28 November 2013]..
- World Health Organization. International health conference, New York, 19–22 June, 1946; signed on 22 July 1946 by the representatives of 61 states (official records of the World Health Organization, no 2, p. 100) and entered into force on 7th April 1948..
- Libyan National Centre for Infectious Diseases Control. 2008. Annual report. Tripoli, Libya: Government of Libya.
- Huew R, Waterhouse P, Moynihan P, Kometa S, Maguire A. Dental caries and its association with diet and dental erosion in Libyan schoolchildren. Int J Paediatr Dent. 2012; 22: 68–76.
- World Health Organization. Dentists, regional health observatory. WHO. 2012. Available from: http://rho.emro.who.int/rhodata/?vid=2625 [cited 28 November 2013]..
- Peeran SW, Singh AJ, Alagamuthu G, Abdalla KA, Naveen Kumar PG. Descriptive analysis of toothbrushing used as an aid for primary prevention: a population-based study in Sebha, Libya. Soc Work Public Health. 2013; 28: 575–82.
- HIV on the rise in Mena. Gulf News. 2013. Available from: http://gulfnews.com/news/gulf/oman/hiv-on-the-rise-in-mena-1.1248978 [cited 28 November 2013]..
- Libyan Public Universities. Ministry of higher education and research, Libya. 2011. Available from: http://highereducation.gov.ly/%D8%A7%D9%84%D8%AA%D8%B9%D9%84%D9%8A%D9%85-%D8%A7%D9%84%D8%B9%D8%A7%D9%84%DB%8C/%D8%A7%D9%84%D8%AC%D8%A7%D9%85%D8%B9%D8%A7%D8%AA/ [cited 28 November 2013]..
- Plasschaert AJM, Holbrook WP, Delap E, Martinez C, Walmsley AD. Profile and competences for the European dentist. Eur J Dent Educ. 2005; 9: 98–107.
- Mattheos N, Schoonheim-Klein M, Walmsley AD, Chapple IL. Innovative educational methods and technologies applicable to continuing professional development in periodontology. Eur J Dent Educ. 2010; 14: 43–52.
- Botelhol MG, Lo EC, McGrath MS, Yiu CKY. Journal-based learning, a new learning experience building on PBL at HKU. Eur J Dent Educ. 2013; 17: 120–5.
- Hodhodinezhad N, Zahedi R, Ashrafi-rizzi H, Shams A. A scientometric study of general internal medicine domain among Muslim countries of middle East (1991–2011). Acta Inform Med. 2013; 21: 55–9.
- Benamer HT, Bredan A, Bakoush O. Scientific publication productivity of Libyan medical schools: a bibliometric study of papers listed in PubMed, 1988–2007. Educ Health (Abingdon). 2009; 22: 310.
- Bakoush O, Al-Tubuly A, Ashammakhi N, Elkhammas E. PubMed medical publications from Libya. Libyan J Med. 2007; 2: 125–8.
- Jaber MA. Intraoral minor salivary gland tumors: a review of 75 cases in a Libyan population. Int J Oral Maxillofac Surg. 2006; 35: 150–4.
- Fteita D, Ali A, Alaluusua S. Molar–incisor hypomineralization (MIH) in a group of school-aged children in Benghazi, Libya. Eur Arch Paediatr Dent. 2006; 7: 92–5.
- El Gehani R, Krishnan B, Orafi H. The prevalence of inflammatory and developmental odontogenic cysts in a Libyan population. Libyan J Med. 2008; 3: 75–7.
- Krishnan B, El Sheikh MH. Dental forceps reduction of depressed zygomatic arch fractures. J Craniofac Surg. 2008; 19: 782–4.
- Fanas SH, Omer SM, Jaber M, Thomas S. The periodontal treatment needs of Libyan schoolchildren in Kufra and Tobruk. J Int Acad Periodontol. 2008; 10: 45–9.
- Elarbi M, El-Gehani R, Subhashraj K, Orafi M. Orofacial tumors in Libyan children and adolescents. A descriptive study of 213 cases. Int J Pediatr Otorhinolaryngol. 2009; 73: 237–42.
- El-Fegh I, Galhood M, Sid-Ahmed M, Ahmadi M. Automated 2-D cephalometric analysis of X-ray by image registration approach based on least square approximator. Conf Proc IEEE Eng Med Biol Soc. 2008; 2008: 3949–52.
- El-Gehani R, Orafi M, Elarbi M, Subhashraj K. Benign tumours of orofacial region at Benghazi, Libya: a study of 405 cases. J Craniomaxillofac Surg. 2009; 37: 370–5.
- Elgehani RA, Orafi MI. Incidence of mandibular fractures in Eastern part of Libya. Med Oral Patol Oral Cir Bucal. 2009; 14: 529–32.
- Krishnan B, Sheikh MH, Rafa el- G, Orafi H. Indications for removal of impacted mandibular third molars: a single institutional experience in Libya. J Maxillofac Oral Surg. 2009; 8: 246–8.
- Subhashraj K, Orafi M, Nair KV, El-Gehani R, Elarbi M. Primary malignant tumors of orofacial region at Benghazi, Libya: a 17 years review. Cancer Epidemiol. 2009; 33: 332–6.
- Gujjar KR, Indushekar KR. Comparison of the retentive strength of 3 different posts in restoring badly broken primary maxillary incisors. J Dent Child (Chic). 2010; 77: 17–24.
- Elhadiry SS, Yunus N, Ariffin YT. Effect of cavity preparation on the flexural strengths of acrylic resin repairs. J Appl Oral Sci. 2010; 18: 546–50.
- Byahatti SM, Ingafou MS. Reasons for extraction in a group of Libyan patients. Int Dent J. 2011; 61: 199–203.
- Huew R, Waterhouse PJ, Moynihan PJ, Maguire A. Prevalence and severity of dental caries in Libyan schoolchildren. Int Dent J. 2011; 61: 217–23.
- Huew R, Waterhouse PJ, Moynihan PJ, Kometa S, Maguire A. Dental erosion and its association with diet in Libyan schoolchildren. Eur Arch Paediatr Dent. 2011; 12: 234–40.
- Gujjar KR, Khadija H, Suleiman MO, Amith HV. Gingival health status of 2- to 15-year-old Benghazi children with type-I diabetes mellitus. J Dent Child (Chic). 2011; 78: 96–101.
- Byahatti S, Ingafou MS. Prevalence of eruption status of third molars in Libyan students. Dent Res J (Isfahan). 2012; 9: 152–7.
- Peeran SW, Singh AJ, Alagamuthu G, Peeran SA, Naveen Kumar PG. Periodontal status and risk factors among adults of Sebha City (Libya). Int J Dent. 2012; 2012: 787502.
- Huew R, Waterhouse PJ, Moynihan PJ, Maguire A. Dental erosion among 12 year-old Libyan schoolchildren. Community Dent Health. 2012; 29: 279–83.
- Huew R, Maguire A, Waterhouse P, Moynihan P. Nutrient intake and dietary patterns of relevance to dental health of 12-year-old Libyan children. Public Health Nutr. 2013; 3: 1–7.
- Peeran SW, Singh AJ, Alagamuthu G, Naveen Kumar PG. Periodontal status and its risk factors among young adults of the Sebha city (Libya). Dent Res J (Isfahan). 2013; 10: 533–8.
- Benamer HT, Bredan A, Bakoush O. A negative trend of biomedical research in Libya: a bibliometric study. Health Info Libr J. 2009; 26: 240–5.