
The copper intrauterine contraceptive device (IUCD) has been largely superseded by the intrauterine system (IUS) in recent years. However, it is still a widely used contraceptive option and is the most effective non-hormonal form of birth control. The suggested duration of effectiveness ranges from 3 to 10 years, depending on the make of IUCD; however most are removed after around 5 years. Risks of neglecting an IUCD include migration, infection, and calcification. A case of IUCD calcification, with an unusual presentation as a possible vesico-vaginal fistula is described and discussed.
A 52-year-old woman presented to accident and emergency, feeling generally unwell. Her medical background included idiopathic myelopathy, which had left her bed bound because of increased tone in her lower limbs. She also suffered from hypercalcaemia and urinary incontinence. On examination, she was found to have necrotic ulcer on her sacral area. Debridement was carried out and a vac pump dressing applied. To maintain hygiene, a catheter was inserted. After a difficult attempt, the surgical team asked the gynaecology team for a review as it was believed a vaginal prolapse might be the cause of the difficulty inserting the catheter.
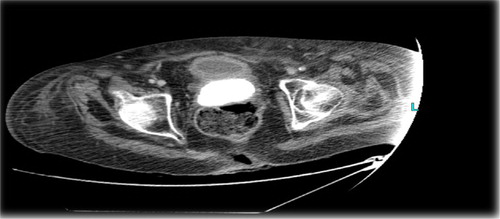
She had an IUCD inserted more than 20 years ago, and this had not been removed. A large, grey, hard, mass was visualised in the vagina measuring 8×5 cm. A CT scan showed a large vaginal stone with IUCD at superior margin, within cavity of atrophic uterus (–).
Fig. 1 CT scan showing calcified IUCD.

Fig. 2 CT scan showing calcified IUCD.

Fig. 3 CT scan showing calcified IUCD.
A cystogram was performed which confirmed that there was no fistula demonstrated between the bladder and the vagina.
Examination under anaesthesia revealed a friable stone in the vagina measuring at least 8 cm in length around the IUCD, extending into the uterine cavity. The stone was removed.
Hysteroscopy was performed, and no abnormalities were seen. A diagnosis of a calcified mass originating from the IUCD was made.
Close examination of the stone demonstrated calcification around a central core of the IUCD and its associated threads ().
Fig. 4 Calcified IUCD after removal.

Calculus analysis had a brown, hard, crystalline appearance and weighed 6,958 mg, consisting of predominantly magnesium ammonium phosphate (88%) and ammonium urate (12%).
Serious complications secondary to IUCD are rare but well recorded. Perforation of the uterine fundus is the most common problem (Citation1). Surface deposition on IUCD occurs in a linear manner with time (Citation2); deposition on copper-containing devices occurs significantly sooner than on inert devices (Citation3). Extensive encrustation as in this case has not been previously reported and is particularly unusual with the IUCD subsequently acting as a focus for calcification although no convincing evidence of vesico-vaginal fistula was ever demonstrated.
King’s College Hospital NHS Foundation Trust
London, UK
Email: [email protected]
References
- Key TC, Kreutner AK. Gastro-intestinal complications of modern intrauterine devices. Obstet Gynecol. 1980; 55: 239–44.
- Rizk M, Shaban N, Medhat I, Moby el Dien Y, Ollo MA. Electron microscopic and chemical study of the deposits formed on copper and inert IUCD. Contraception. 1990; 42: 643–53.
- Yuan W, Shen H, Lu J, Fan J. Analysis of surface deposits on intrauterine contraceptive devices. Adv Contracept. 1986; 2: 193–204.