
Abstract
Introduction
Most of the literature related to the effects of Ramadan fasting on physical performance has focused on adults, and only three studies have examined its impact on children's physical performance.
Aims
To examine the effects of Ramadan fasting on first-time fasting boys’ performance in short-term explosive exercises [vertical and horizontal jump tests (VJT and HJT), 20-m and 30-m sprints and medicine-ball throw (MBT)], as well as in sub-maximal endurance [6-min walking distance (6MWD) measured during the 6-min walk test (6MWT)].
Methods
Eighteen Tunisian boys [mean±standard deviation (SD) of age and body mass (BM): 11.9±0.8 y and 55.4±18.2 kg, respectively] were included. The experimental design comprised four testing phases: 2-weeks before Ramadan (BR), the end of the second week (R2) and the fourth week (R4) of Ramadan, and 10–12 days after the end of Ramadan (AR). At each phase, boys performed two test sessions in the afternoon (15:00–17:00 h) interrupted by 48 h of recovery (first test session: BM, VJT, HJT, and 20-m and 30-m sprint tests; second session: MBT and 6MWT). The study was conducted during the summer of 2012 from July 5 to August 29.
Results
6MWDs (m) were significantly shorter during R2 (652±101) and R4 (595±123) compared to BR (697±86) and came back to baseline values AR. BM (kg) mean±SD did not significantly change during R2 (52±15) and during R4 (53±15) compared to BR (55±17), and short-term explosive performances were unchanged throughout the study.
Conclusion
In non-athletic children, first-ever Ramadan fasting impairs sub-maximal aerobic capacity but has no effect on BM or short-term explosive performance.
To access the supplementary material for this article please see Supplementary files under Article Tools online
Ramadan fasting (RF) is the fourth pillar of Islam and requires adult Muslims to refrain from all types of liquid and food intake from dawn to sunset (Citation1). Ramadan advances 11 days each year over a western calendar. Hence, the fast duration depends on the geographical location and the season of the year, and can be as long as 18 h a day in the summer of high-latitude regions (Citation2). According to Islamic rules, this practice concerns every healthy Muslim from the time of puberty (Citation1). Nevertheless, although RF is not compulsory for young pre-pubescent children, many practice it from early adolescence.
Children engage mostly in multiple-sprint sports (e.g. soccer, basketball, tennis), or intermittent playing activities (Citation3), that rely on the capacity to recover and reproduce performance in subsequent sprints or short efforts (Citation4). As training and competitions continue to be held during Ramadan, the number of studies that have examined the effects of RF on sport performance is increasing. Unfortunately, most published studies were performed on adult subjects (Citation4, Citation5), and data regarding the effects of RF on children and/or adolescents are scarce (Citation6–Citation8). Some authors have also pointed out that the RF history of the participants (the number of years the subjects used to fast and exercise at the same time) could impact their adaptation and response to physical testing (Citation9). In this context, to the best of the authors’ knowledge, only three studies (Citation6–Citation8) have examined the impact of RF on children's sporting performance, without mentioning whether the participants had any experience with respect to their fasting and exercising at the same time.
In 2008, Meckel et al. (Citation6) published data about the performance of 19 young soccer players aged 14–16 years performing different tests carried out before Ramadan (BR) and at the end of the fourth week of Ramadan (R4). They concluded that participation in RF reduced children's physical work capacity but had no significant effect on sprint performance or agility. In Ramadan 2010, Girard and Farooq (Citation7) investigated the impact of RF on the ability of 18 non-athlete boys aged 12.6±1.5 years to perform repeated sprints between 13:00 and 14:00 h. They concluded that repeated sprinting performance was compromised towards R4, and that this effect persisted for 2 weeks after the end of Ramadan (AR2), while fatigue resistance was not affected. More recently, our group (Citation8) investigated the effect of RF on the performance of 12 male soccer players aged 13.3±0.4 years. We concluded that RF led to impairment in boy soccer players’ performance in the afternoon and affected their diurnal pattern observed BR. Although some studies (Citation6–Citation8) gave a general idea about the RF effect on children's physical performance, they present some methodological limitations [e.g. lack of information about the season and/or the geographical location (Citation6–Citation8) or about previous experience with RF (Citation8) or about the training status of the participants (Citation6, Citation8) or lack of acute AR control measurements (Citation6)].
The effects of RF on some aspects of short-term explosive capacities, such as horizontal jump and medicine-ball throw (MBT) distances, have not been evaluated. In addition, data about the effect of RF on cardiorespiratory responses to maximal and/or sub-maximal exercise in sedentary adults are controversial: small reduction (Citation10, Citation11) or no influence on maximal exercise capacity and walking efficiency (Citation11, Citation12) has been reported. To the best of the authors’ knowledge, no previous study has examined the effect of RF on children's sub-maximal functional capacity. This could be evaluated, for example, by measuring the greatest distance that a child could walk in 6 min (6MWD) during the 6-min walk test (6MWT) (Citation13, Citation14). The 6MWT is a simple test that has been increasingly used in children because it is easy to administer, better tolerated and more reflective of daily living activities than other exercise tests (Citation13–Citation16).
There is no consensus about the effects of RF on body mass (BM) (Citation17), with weight reduction (Citation18, Citation19) or gain (Citation20, Citation21) or no significant changes (Citation11, Citation22) being reported. Unfortunately, most of these studies focused primarily on adult Muslims (Citation17). In children, Meckel et al. (Citation6) found no significant change in BM when comparing the BR measures to the last 2 days of Ramadan ones. However, Girard and Farooq (Citation7) found that BM was elevated at R4 and AR2 when compared to BR baseline values. Changes in BM could influence physical performance, for instance, through alteration of lean mass.
In view of the above considerations, the aim of the present study was to examine, in untrained boys fasting for the first time in their lives, the effects of RF on BM, sub-maximal aerobic performance (determined through the 6MWD) and short-term explosive physical capacities [determined through MBT, vertical jump test (VJT), horizontal jump test (HJT), and 20-m and 30-m sprint tests].
Population and methods
Participants
Eighteen Tunisian healthy untrained boys who were going to fast the entire month of Ramadan for the first time ever took part in this study. The fact that they were going to fast for the entire month of Ramadan during summer 2012 was checked well before the experiment began. This was done by individual interview with the participants and with their parents at the moment of signing the informed consent for participation in the study. In that regard, it is common that children fast half-days and go progressively to isolated fasting days during Ramadan for the 2–3 years preceding the first entire month attempt.
The participants were recruited from two primary schools located in Kalaa-Kebira, Sousse (altitude<100 m) in Tunisia. None of them participated in any sporting activity other than at school, where they usually practice for a maximum of 2 h a week. The study measures were carried out in the Laboratory of Physiology of Sousse, Faculty of Medicine.
For the present study, the elapsed time from dawn to sunset was ~16 h at the beginning (20th of July) and ~15 h at the end (18th of August) of Ramadan 2012. The laboratory room temperature was ~25°C and humidity was ~40%.
Study approval was obtained from the local Hospital Ethics Committee, as complying with the Helsinki ethics guidelines, and written informed consent was obtained from all boys and their parents before the commencement of the study. Participants knew they could withdraw from the study at any time without any penalty.
Sample size
The sample size was calculated according to the following equation (Citation23): N=(Zα)2 s2/d2, where ‘s’ is the standard deviation (SD) obtained from a previous study (Citation8), and ‘d’ is the accuracy of estimated or how close to the true mean, ‘Zα’ is normal deviate for one-tailed alternative hypothesis at a level of significance (equal to 1.28 for 10% level of significance). According to Aloui et al. (Citation8), the mean±SD of counter movement jump (CMJ, cm) measured BR and during R4 was 44.50±5.63 vs. 42.81±4.98, respectively (so ‘s’ is equal to 5.31 and ‘d’ is equal to 1.69). The estimated sample size gives a sample of 16 boys. An allowance of 10% was assumed for absence, loss to follow-up, and withdrawal, and then the corrected sample was of 16/(1.0–0.10)=16/0.9=18.
Study design
Prior to actual measurements, boys were familiarised with all the study tests to optimise their performance while minimising the learning effect (Citation24–Citation27). Furthermore, they did not perform any strenuous physical activity (sport session at school, nor any other intense effort), 24 h before each testing period.
The experimental design consisted in four testing phases: 2 weeks BR, the end of the second week of Ramadan (R2), the R4 and 10–12 days AR. During each phase, participants performed two test sessions interrupted by 48 h of recovery. During the first session, participants’ BM was measured, then they completed the VJT, HJT, and 20-m and 30-m sprint tests, with 5–10 min of recovery in between. During the second session, they carried out the MBT and the 6MWT.
Test sessions were conducted at the same time of day between 15:00 and 17:00 h, which was about 2.5–4.5 h before sunset, time at which fasters are allowed to break their fast (mean hour =19:22 h).
The decimal age was calculated to the nearest 0.01 years from the date of measurements and the date of birth (Citation28). BM (±1 kg) was measured upon arrival at the laboratory (fasting state) on each first day of testing of each period, using an electronic balance (Tanita TBF300WA, Tokyo, Japan). AR, BR and BM was measured 4 h after lunch. Height (±1 cm) was measured once at the start of the study with a height gauge (standing stadiometer type DETECTO®).
Evaluation of short-term exercise capacities
Vertical jump test
VJT height was measured by a maximum vertical jump using a free-arms CMJ technique (Citation6, Citation29). Boys began in an erect standing position and rapidly moved into a semi-squat position and sprang into an immediate jump. The participants used a vigorous double-arm swing as they jumped vertically (Citation9, Citation29). Three trials were completed (with a ~2-min rest period in between). The highest CMJ height achieved was recorded. All jumps were performed on a 60×40-cm force platform (Optojump, Microgate, Bolzano, Italy) connected to a digital timer that recorded the flight time of all jumps.
Horizontal jump test
Boys began by standing on their preferred leg with the toes on the starting line and their hands on their hips (Citation30). They were instructed to sink (approximately 120° knee angle) as quickly as possible and then jump as far forward as possible and land on two adjacent feet (Citation30). The distance jumped was measured with a tape to the nearest one cm between the starting line and the back edge of the heel closest to that line at landing. As for CMJ, 2 min interrupted the three trials and the longest distance was selected for analysis.
Sprints
Separated sprint times of 20 m and 30 m were recorded using a photocell system (Microgate, Bolzano, Italy). For each sprint, two runs were completed and the boys rested for 3–4 min between runs. The shorter time of the two runs was recorded.
Medicine ball throw
The participant started with the feet shoulder-width apart, the back edge of the heels on the zero measurement line and the medicine ball (weight=1.5 kg) held with arms straight out front at shoulder height (Citation31). Then, he flexed his knees and lowered the ball to approximately the height of the knees. From there, he extended his legs, extended his back, elevated his shoulders and finally flexed his shoulders to throw the medicine ball backwards over his head, attempting to achieve maximum horizontal distance (Citation32). Each participant performed three trials separated by approximately 3 min of recovery (Citation33) and the longest ball throw distance was used for further analysis.
Sub-maximal aerobic capacity evaluation
The 6MWT was performed according to a standardised protocol (Citation13). No warm-up was allowed before the test. Participants remained seated for at least 10 min before the beginning of the walk. They were then instructed to walk up and down a 40-m corridor, with markers every one-meter, and cover as much distance as possible over a 6-min period. The test was self-paced and boys were allowed to rest if they desired, although the clock continued to run. However, none of them needed to rest because they knew how to pace based on pre-experiment trials. Boys were verbally encouraged during all the tests. The words of encouragement were consistent and standardised (‘keep going’, ‘you are doing fine’, ‘everything is going well’) and were given by the same person (MAF) at set times during the test. At the end of the 6MWT, the 6MWD in meters (m) was noted and expressed as a percentage of the predicted local reference values (Citation14): 6MWD (m)=4.63×height (cm) − 3.53×BM (kg)+10.42×age (years)+56.32. All tests have been shown to be valid and reproducible (Citation24–Citation27).
Statistical analysis
The Kolmogorov-Smirnov test for normality revealed that the data were normally distributed. Data were presented as means±SD, 95% confidence interval (95% CI) and range (minimum–maximum).
To compare the mean values of BM and performance data in the four testing phases, repeated measures analysis of variance (ANOVA) was used. When appropriate, significant differences between means were tested using the Wilcoxon test or ANOVA Chi2.
Analyses were carried out using Statistica software (Statistica Kernel version 6; StatSoft, Paris, France). Significance was set at the 0.05 level.
Results
Twenty-five boys and their parents first agreed to contribute to the study, but five dropped out because of transportation difficulties and two due to illness, leaving 18 for analysis. The anthropometric data of the 18 boys are displayed in .
Table 1 Baseline anthropometric data of the 18 non-athlete boys fasting for the first time
Effects of RF on BM
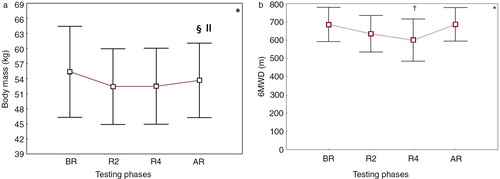
BM values measured during the four testing phases are presented in a. There was a significant phase effect between the four testing periods [ANOVA (n=18, df=3)=10.53; p<0.014]. However, BM (kg) mean±SD did not change significantly during R2 (52±15) (range 45–60) and during R4 (53±15) (range 45–60] compared to BR (55±17) (range 46–63).
Fig. 1 Effects of Ramadan fasting on body mass (a) and 6-min walking distance (b) of 18 non-athlete boys fasting for the first time.
Mean values are shown. Error bars represent 95% confidence intervals. BR: before Ramadan, R2: end of the second week of Ramadan, R4: end of the fourth week of Ramadan, AR: 10–12 days after the end of Ramadan. *p<0.05: ANOVA. (A, B) † p<0.05 (Wilcoxon test): BR vs. other periods; ‡ p<0.05 (Wilcoxon test): R2 vs. R4; ll p<0.05 (Wilcoxon test): R4 vs. AR. (A) ‡ p<0.05 (Wilcoxon test): R2 vs. R4. (B) ll p< 0.05 (Wilcoxon test): R4 vs. AR.
Effects of RF on short-term explosive performance
VJT height, HJT distance, 20-m and 30-m sprint times and MBT distance measured during the four testing phases are presented in . There was no statistically significant difference between the four testing periods for any of the variables.
Effects of RF on sub-maximal aerobic capacity
The measured 6MWD (m) during the four testing phases are presented in b. There was a significant phase effect [ANOVA (n=18, df=3)=22.0391; p<0.00006]. The 6MWD mean±SD [95% CI] was lower during R2 (635±105) [583–687] and R4 (601±122) [540–661] compared to BR (686±98) [637–735] (p=0.001) but returned to baseline values AR [687±97] [639–735].
Discussion
The main findings of the present study showed that untrained boys aged about 12 years and fasting for the first time in their lives during Ramadan underwent a significant reduction in sub-maximal aerobic capacity while BM and short-term explosive physical capacities were unchanged. Sub-maximal aerobic capacity significantly increased AR to return towards BR baseline values.
Table 2 Effect of Ramadan fasting on short-term exercise capacities in 18 non-athlete boys fasting for the first time
To the best of our knowledge, only three studies (6–8; summarised in Supplementary Table 1) have examined the effect of RF on children's physical performance. Meckel et al. (Citation6) concluded that participation in RF reduced endurance (increase in the 3,000-m running time and in the sum of 6×40 m run time) and vertical jump performance but had no significant effect on 40-m sprint performance and 4×10-m shuttle run time. Girard and Farooq (Citation7) concluded that repeated sprinting performance (6×15-m interspersed with 15 s of passive recovery) was compromised towards R4 and that this effect persisted after Ramadan (AR2), while fatigue resistance was not affected. Aloui et al. (Citation8) concluded that RF led to impairment in soccer players’ performances in the afternoon and affected the participants’ diurnal pattern observed BR. Although the latter studies (Citation6–Citation8) gave a general idea about the RF effect on children's physical performance, they present some methodological limitations:
Information about the season and/or the geographical location was lacking (Citation6–Citation8). Indeed, Ramadan occuring in summer time at high latitudes presents very different issues compared to Ramadan in winter times or even at lower latitudes (Citation34).
Information about previous experience with RF was mentioned in only one study (Citation8). In the study of Girard and Farooq (Citation7), no information is provided about the RF experience of the children. Direct contact with the authors allowed determining that participants in their study had all fasted at least for one Ramadan month before the study was conducted. In that regard, RF for the first time may present a challenge for children/young adolescents (Citation8).
In two studies (Citation6, Citation8), the children's physical activity status was described as ‘athletes’ [soccer players with regular training program during Ramadan (Citation6) or with a minimum of 3 years of previous practice (Citation8)]. The training status of the participants should be acknowledged, as it may interfere with the independent effects of RF on physical capacity (Citation6).
Lack of acute AR control measurements (Citation6). In this case (Citation6), it is still unknown whether the diurnal nutrition and sleep cycle alterations imposed by Ramadan could lead to transient performance adaptations and/or persisting effects (Citation5).
Discussion of results
Effects of RF on BM
RF did not influence BM (). This is opposite to that observed by Girard and Farooq (Citation7) [showing that BM (kg) was elevated at R4 (46±3) and AR2 (47±3) vs. BR (45±3)] but similar to the findings of Meckel et al. (Citation6) [no significant change in BM (kg) in the last 2 days of Ramadan (63±7) when compared to BR (63±7)]. Differences in daily habits, occupation and social and geographical environment can influence the energy balance and may contribute to the inconsistency in findings among studies (summarised in Supplementary Table 1) (Citation6). The participants in our study, fasting for the first time, might have followed an adequate dietary pattern during Ramadan, resulting in a stable BM.
Effects of RF on sub-maximal aerobic capacity
6MWD, a parameter reflecting sub-maximal aerobic capacity (Citation13–Citation16), was 85 m shorter during R4 compared to BR (b). This difference of 85 m is higher than the 90% level minimal detectable change in 6MWD that can be used to determine whether the change in the children's 6MWD following intervention is statistically significant (MDC90 = 48.34 m) (Citation35). To the authors’ knowledge, no previous study has examined the effect of RF on children's performance during sub-maximal endurance testing. When interpreting the 6MWD performed by a child undergoing RF and in order to avoid data misinterpretation, one recommendation is to take the 6MWD decrease during this holy month into consideration. It is interesting to note that impairment in children's performance during Ramadan was also observed in endurance exercises with higher intensities (Citation6). Indeed, Meckel et al. (Citation6) showed a significant reduction in maximal aerobic endurance (increased 3,000 m running time) during Ramadan. According to Meckel et al. (Citation6), the significant reduction in maximal aerobic endurance may indicate a physiological adaptation in individuals fasting during Ramadan. Indeed, this suggests that during Ramadan, the body's metabolism slows down during the day, reflecting a drive to conserve energy stores (especially glycogen, switching to more lipolysis energy use for sub-maximal efforts) (Citation6). Fasting has also been associated with catecholamine inhibition and reduced venous return, causing a decrease in the sympathetic tone, which leads to a decrease in heart rate, cardiac output and blood pressure (Citation36, Citation37). These physiological changes may also influence physical work capacity and cause further deterioration in athletic ability (Citation6). It has been demonstrated that the worse the chronotropic response was, the lower the children's 6MWD was (Citation14). Gutierrez et al. (Citation38) found a significant and progressive decrease in the aerobic capacity (physical work capacity at 170 bpm) of adult athletes who fasted for 72 h. Another possible explanation of the decrease in sub-maximal performance could come from the fasting history. The present study's participants observed the RF for the first time, while in the study of Chaouachi et al. (Citation39), which showed no effect of RF on endurance performance, participants used to train and fast for ~7 years. A speculated negative effect of RF on lung function parameters (expiratory flow and/or lung volumes) could also be advanced. In fact, in children, the worse the spirometric data were, the lower was the 6MWD (Citation14). To the authors’ knowledge, no previous study has examined the effect of RF on healthy children's lung function. In healthy adults, reports about the effect of RF on lung function are controversial, describing either no significant effect on expiratory flow rates (Citation21) or an increase in lung volume (Citation40). Another explanation, not evaluated in the present study, could be the degree of children's motivation that could have been negatively affected by RF (Citation13, Citation41).
Effects of RF on short-term explosive physical capacity
One main finding of the present study was that participation in RF did not reduce short-term physical capacity of non-athlete young boys fasting for the first time (). On the one hand, the results are consistent with those of other studies that found hand-grip strength and reaction time to be unchanged during Ramadan (Citation38, Citation42). The ability of the subjects to perform these activities reflects mainly their anaerobic power and muscle strength. On the other hand, the results are partly opposite to those found by some other authors (Citation6–Citation8) (Supplementary Table 1). According to Meckel et al. (Citation6) RF led to a significant decrease in short-term physical capacities: reduction in speed endurance (increased sum of 6×40-m run time and performance decrement) and CMJ performance. However, these authors showed that RF did not have a significant effect on the 40-m sprint time or agility performance. The possible explanation of the decrease in speed endurance may be a decreased glycolytic capacity as well as a slower replenishment of muscle creatine phosphate stores during the short recovery period between sprints (Citation6). According to Girard and Farooq (Citation7), repeated sprinting performance was compromised towards the end of Ramadan, and this effect persisted for 2 weeks, while fatigue resistance was not affected (significant main effect of sprint number and time period on sprint times without interaction effect, cumulated sprint times differed across time periods: compared to BR, cumulated sprint times lengthened during Ramadan (R1; R4) and remained elevated AR (AR2 and AR4)). Initial/peak sprint performance and sprint decrement score did not change; however, the precise underlying mechanisms of the repeated sprint ability impairment cannot be identified in their sample of non-athlete youth Muslims observing Ramadan. Nevertheless, Girard and Farooq (Citation7) assume that the negative effects of dehydration, the daily refraining from food consumption and the modification of the sleep–wake cycle account for impairment in physical performance during Ramadan (Citation5). It also remains possible that the lower levels of readiness and capacity to concentrate, which usually accompany physical performance impairments during Ramadan, may also have contributed to the alterated repeated sprint ability (Citation7). According to Aloui et al. (Citation8), RF leads to impairment in adolescent soccer players’ performance in the afternoon (the afternoon squat jump and CMJ performances and predicted maximal oxygen uptake were lower during R4 than BR, and the afternoon perceived exertion scores were higher during R4 compared to BR). The observed decrease in performance during Ramadan is likely not linked to changes in caloric intake (Citation8). Indeed, they found that the estimated energy intake and percentages of carbohydrates, fats and proteins in the diets were not modified during Ramadan compared to BR (Citation8). However, the performance decline could be attributed to a change in sleep patterns (Citation8): soccer players noticed that their sleep duration was reduced because they were consuming food later at night. In that regard, one limitation of the present study is that both energy intake and sleep patterns were not monitored. However, the fact that the subjects were able to keep their BMs constant (compared to BR values) shows that overall they did not cope badly with their first RF month. Consequently, by keeping their BMs unchanged, it is likely that their fat-free mass was maintained (even though this was not specifically measured). Most of the studies showing maintenance of short-term powerful physical capacities throughout RF were related to unchanged fat-free masses, while a decrease in the latter was usually accompanied by reduced powerful performances (Citation2, Citation4).
Mechanisms responsible for performance decrement during Ramadan
The effect of RF on sport performance is a controversial issue (Citation4). Indeed, performance during single brief or very short-duration exercises is generally maintained, while repetitive short-term maximal or long-duration efforts are reported by some authors to be reduced during Ramadan. This is mainly true when test sessions are conducted in the late afternoon just before Iftar (Citation4). However, the point at which the components of performance are affected is not well established (Citation4). Till now, the exact underlying mechanisms of performance decrement observed during Ramadan (when it occurs) are not well identified (Citation4). Although speculative, overall the outcome of the experiments on the topic suggest that disturbances of the sleep–wake cycle and circadian rhythms, hypo-hydration, possible alterations in body composition, environmental conditions, training load/regimen changes, lung or heart function alterations and mental fatigue could explain the negative effect of RF on sport performance.
Discussion of methodology
Although RF is not compulsory for young pre-pubescent children, many practice it from early adolescence. Indeed, even though it might be questionable that pre-pubescent children fast while religion requires such a practice only after puberty, it is a relatively common practice that very young children try their first attempt to fast the entire month while they are still pre-pubescent. This is generally achieved through a progressive approach with half-days of fast when they are around 6–9 years of age, to isolated complete fasting days at later ages, until they perform their first trial, usually at the age of 11–15 years.
Differences in subjects characteristics (age, training status), nature of the tests (e.g. sprint number/duration, recovery time) or timing of tests (Ramadan period, time of day) are known to affect physical performance (Supplementary Table 1), i.e. task-dependency of the Ramadan effects. This leads to anecdotal comparisons of physical responses between studies (Citation7).
Participants
The baseline 6MWD data of the participants of the present study are very close to what have already been published by our group on another sample of healthy Tunisian young boys (Citation14). Indeed, the BR 6MWD mean±SD (95% CI) expressed as a percentage of predicted values was 99±11% (93–105%). This further strengthens the BR values presented here. Furthermore, the statistical analysis used is appropriate and shows a clear significant effect of RF on a sub-selection of the measured variables. Consequently, it is most probable that the observed effect is due to RF. However, one major limitation of the present study is the absence of a control group (e.g. healthy non-athlete boys not fasting during Ramadan). But it should be stressed that obtaining non-fasting groups in countries with a Muslim majority is not easy due to ethical reasons. Therefore, most of the studies on RF conducted in Muslim majority countries used pre-Ramadan (BR) values as control/baseline. A Medline research (performed on the 9th of August 2014) using as keywords ‘RF’ and ‘control group’ found only 12 studies (Citation43–Citation54), all performed on adults, and only five studies (Citation44–Citation47, Citation53) were exercise physiology. In the future, studies aiming to evaluate the effect of RF on children's physical activity should try to systematically include a non-fasting control group. The inclusion of a control group should reduce the possibility of learning effects skewing the results and avoid the threat to the internal validity of the findings.
RF duration and season
Ramadan lasts 29 or 30 days, based on detection of the new moon. In addition, this month moves ahead about 11 days each year compared to the Gregorian calendar and can occur during any season (Citation4). Consequently, the effects of daytime fasting are strongly influenced by climatic conditions. Ramadan occurring in summer at high altitudes presents very different features compared to Ramadan in winter at lower altitudes (Citation4). The fasting duration depends on the geographical location and the season of the year, and can be as long as 18 h a day in the summer of temperate regions (Citation4). In other countries in the far north, the fasting duration is even longer, representing a real challenge for fasters (Citation4). The present study was carried out in Tunisia during the summer of 2012, when the time from dawn to sunset was about 16 h at the beginning and 15 h at the end of Ramadan. The median testing temperature was about 25°C and humidity ranged from 38 to 42%. These conditions could be considered as relatively challenging as temperature was quite warm and the subjects had fasted 11–15 h before the tests, depending on whether they had Suhour (last allowed meal before dawn) or had their last meal just before going to bed. This is a long time for such young people fasting for the first time in their lives. In that regard, information about the season and/or the geographical location was lacking in some previous studies (Supplementary Table 1).
Test timing
One wonders whether the test timing could have a negative influence on physical performance. Participants of the present study performed tests only about 2 h before breaking the fast. Aloui et al. (Citation8) recently evaluated the effects of Ramadan on the diurnal variations of physical performance of adolescents. Twelve young male soccer players completed VJT and the multistage 20-m shuttle run test 1 week BR and during R4 in the morning and in the afternoon. Authors showed that Ramadan leads to impairment in adolescent soccer players’ performances in the afternoon and therefore affects their diurnal pattern observed BR (Citation8).
Sample size
Though sample size dropped from 25 to 18, we consider it satisfactory. It is larger than that of Aloui et al. (Citation8) (n=12) and similar to those of Meckel et al. (Citation6) (n=19) and Girard and Farooq (Citation7) (n=18) (Supplementary Table 1).
Justification of short-term exercises choice
Children perform many short activities daily (Citation14). In addition, in Muslim countries, during Ramadan children do not interrupt their study or school physical activities. Jump, sprints and ball throw are among the most recommended tests for the assessment of anaerobic capacity in children (Citation55).
Justification of the 6MWT choice to evaluate sub-maximal aerobic capacity
The 6MWT has been found to be a valid measure of sub-maximal exercise capacity in healthy children aged 12–16 years [excellent test–retest reliability and significant correlation between 6MWD and peak aerobic capacity (Citation27)].
Conclusion
The present study showed no significant effect on BM or short-term explosive physical capacity in young untrained boys aged about 12 years undergoing RF for the first time ever during the summer of 2012. However, sub-maximal endurance performance, evaluated by the 6MWT, was reduced.
Conflict of interest and funding
The authors declare they have no conflicts of interest concerning this article.
Supplementary Table
Download PDF (204.4 KB)Acknowledgements
The authors wish to thank Professor Bechir SAADAOUI for his invaluable contribution to the improvement of the quality of the writing of the present paper. They also wish to express their sincere gratitude to all participants and their parents for their maximal effort and cooperation.
Notes
To access the supplementary material for this article please see Supplementary files under Article Tools online
References
- Rashed AH. The fast of Ramadan. BMJ. 1992; 304: 521–2.
- Chaouachi A, Leiper JB, Chtourou H, Aziz AR, Chamari K. The effects of Ramadan intermittent fasting on athletic performance: recommendations for the maintenance of physical fitness. J Sports Sci. 2012; 30(Suppl 1): S53–73. [PubMed Abstract].
- Jebali T, Moalla W, Elloumi M, Padulo J, Baquet G, Chamari K. The relevant use of the traditional Tunisian game “raqassa” for cardiovascular stimulation in schoolchildren. Biol Sport. 2013; 30: 219–25. [PubMed Abstract] [PubMed CentralFull Text].
- Aloui A, Chtourou H, Souissi N, Chamari K, Chtourou H. Ramadan fasting and sport performance. Effects of Ramadan fasting on health and athletic performance. 2013; OMICS Group eBooks. 2–8. [downloaded 2014 August 24]. Available from: http://www.esciencecentral.org/ebooks/effects-of-ramadan-fasting/ramadan-fasting-sport-performance.php [cited 25 July 2013]..
- Maughan RJ, Fallah J, Coyle EF. The effects of fasting on metabolism and performance. Br J Sports Med. 2010; 44: 490–4. [PubMed Abstract].
- Meckel Y, Ismaeel A, Eliakim A. The effect of the Ramadan fast on physical performance and dietary habits in adolescent soccer players. Eur J Appl Physiol. 2008; 102: 651–7. [PubMed Abstract].
- Girard O, Farooq A. Effects of Ramadan fasting on repeated sprint ability in young children. Sci Sports. 2012; 27: 237–40.
- Aloui A, Chtourou H, Hammouda O, Souissi H, Chaouachi A, Chamari K, etal. Effects of Ramadan on the diurnal variations of physical performance and perceived exertion in adolescent soccer players. Biol Rhythm Res. 2013; 44: 869–75.
- Chtourou H, Hammouda O, Chaouachi A, Chamari K, Souissi N. The effect of time-of-day and Ramadan fasting on anaerobic performances. Int J Sports Med. 2012; 33: 142–7. [PubMed Abstract].
- Ramadan JM, Barac-Nieto M. Cardio-respiratory responses to moderately heavy aerobic exercise during the Ramadan fasts. Saudi Med J. 2000; 21: 238–44. [PubMed Abstract].
- Ramadan J. Does fasting during Ramadan alter body composition, blood constituents and physical performance?. Med Princ Pract. 2002; 11(Suppl 2): 41–6. [PubMed Abstract].
- Sweileh N, Schnitzler A, Hunter GR, Davis B. Body composition and energy metabolism in resting and exercising Muslims during Ramadan fast. J Sports Med Phys Fitness. 1992; 32: 156–63. [PubMed Abstract].
- Laboratories ATSCoPSfCPF. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002; 166: 111–17.
- Ben Saad H, Prefaut C, Missaoui R, Mohamed IH, Tabka Z, Hayot M. Reference equation for 6-min walk distance in healthy North African children 6–16 years old. Pediatr Pulmonol. 2009; 44: 316–24. [PubMed Abstract].
- Goemans N, Klingels K, van den Hauwe M, Boons S, Verstraete L, Peeters C, etal. Six-minute walk test: reference values and prediction equation in healthy boys aged 5 to 12 years. PloS One. 2013; 8: e84120. [PubMed Abstract] [PubMed CentralFull Text].
- Pane M, Mazzone ES, Sormani MP, Messina S, Vita GL, Fanelli L, etal. 6 minute walk test in Duchenne MD patients with different mutations: 12 month changes. PloS One. 2014; 9: e83400. [PubMed Abstract] [PubMed CentralFull Text].
- Trabelsi K, Stannard S, Shephard R, Jamoussi K, Hakim A, Chtourou H. Body composition, hematological and biochemical modifications during Ramadan fasting. Effects of Ramadan fasting on health and athletic performance. 2013; OMICS Group eBooks. 3–8. [downloaded 2014 August 24]. Available from: http://www.esciencecentral.org/ebooks/effects-of-ramadan-fasting/body-composition.php [cited 25 July 2013]..
- Hallak MH, Nomani MZ. Body weight loss and changes in blood lipid levels in normal men on hypocaloric diets during Ramadan fasting. Am J Clin Nutr. 1988; 48: 1197–210. [PubMed Abstract].
- Ramadan J, Telahoun G, Al-Zaid NS, Barac-Nieto M. Responses to exercise, fluid, and energy balances during Ramadan in sedentary and active males. Nutrition. 1999; 15: 735–9. [PubMed Abstract].
- Frost G, Pirani S. Meal frequency and nutritional intake during Ramadan: a pilot study. Hum Nutr Appl Nutr. 1987; 41: 47–50. [PubMed Abstract].
- Siddiqui QA, Sabir S, Subhan MM. The effect of Ramadan fasting on spirometry in healthy subjects. Respirology. 2005; 10: 525–8. [PubMed Abstract].
- el Ati J, Beji C, Danguir J. Increased fat oxidation during Ramadan fasting in healthy women: an adaptative mechanism for body-weight maintenance. Am J Clin Nutr. 1995; 62: 302–7. [PubMed Abstract].
- Suresh K, Chandrashekara S. Sample size estimation and power analysis for clinical research studies. J Hum Reprod Sci. 2012; 5: 7–13. [PubMed Abstract] [PubMed CentralFull Text].
- Acero RM, Fernandez-del Olmo M, Sanchez JA, Otero XL, Aguado X, Rodriguez FA. Reliability of squat and countermovement jump tests in children 6 to 8 years of age. Pediatr Exerc Sci. 2011; 23: 151–60. [PubMed Abstract].
- Davis KL, Kang M, Boswell BB, DuBose KD, Altman SR, Binkley HM. Validity and reliability of the medicine ball throw for kindergarten children. J Strength Cond Res. 2008; 22: 1958–63. [PubMed Abstract].
- Ingle L, Tolfrey K. The variability of high intensity exercise tests in -pre-pubertal boys. Int J Sports Med. 2013; 34: 1063–9. [PubMed Abstract].
- Li AM, Yin J, Yu CC, Tsang T, So HK, Wong E, etal. The six-minute walk test in healthy children: reliability and validity. Eur Respir J. 2005; 25: 1057–60. [PubMed Abstract].
- Quanjer PH, Hall GL, Stanojevic S, Cole TJ, Stocks J. Age- and height-based prediction bias in spirometry reference equations. Eur Respir J. 2012; 40: 190–7. [PubMed Abstract].
- Racinais S, Hue O, Blonc S. Time-of-day effects on anaerobic muscular power in a moderately warm environment. Chronobiol Int. 2004; 21: 485–95. [PubMed Abstract].
- Maulder P, Cronin J. Horizontal and vertical jump assessment: reliability, symmetry, discriminative and predictive ability. Phys Ther Sport. 2005; 6: 74–82.
- Stockbrugger BA, Haennel RG. Validity and reliability of a medicine ball explosive power test. J Strength Cond Res. 2001; 15: 431–8. [PubMed Abstract].
- Mayhew JL, Bird M, Cole ML, Koch AJ, Jacques JA, Ware JS, etal. Comparison of the backward overhead medicine ball throw to power production in college football players. J Strength Cond Res. 2005; 19: 514–18. [PubMed Abstract].
- Matuszak ME, Fry AC, Weiss LW, Ireland TR, McKnight MM. Effect of rest interval length on repeated 1 repetition maximum back squats. J Strength Cond Res. 2003; 17: 634–7. [PubMed Abstract].
- Burke LM, King C. Ramadan fasting and the goals of sports nutrition around exercise. J Sports Sci. 2012; 30(Suppl 1): S21–31. [PubMed Abstract].
- Klepper SE, Muir N. Reference values on the 6-minute walk test for children living in the United States. Pediatr Phys Ther. 2011; 23: 32–40. [PubMed Abstract].
- Al Suwaidi J, Bener A, Gehani AA, Behair S, Al Mohanadi D, Salam A, etal. Does the circadian pattern for acute cardiac events presentation vary with fasting?. J Postgrad Med. 2006; 52: 30–3. [PubMed Abstract].
- Stokholm KH, Breum L, Astrup A. Cardiac contractility, central haemodynamics and blood pressure regulation during semistarvation. Clin Physiol. 1991; 11: 513–23. [PubMed Abstract].
- Gutierrez A, Gonzalez-Gross M, Delgado M, Castillo MJ. Three days fast in sportsmen decreases physical work capacity but not strength or perception–reaction time. Int J Sport Nutr Exerc Metab. 2001; 11: 420–9. [PubMed Abstract].
- Chaouachi A, Coutts AJ, Chamari K, Wong del P, Chaouachi M, Chtara M, etal. Effect of Ramadan intermittent fasting on aerobic and anaerobic performance and perception of fatigue in male elite judo athletes. J Strength Cond Res. 2009; 23: 2702–9. [PubMed Abstract].
- Moosavi SA, Kabir A, Moghimi A, Chehrei A, Rad MB. Evaluation of the effect of Islamic fasting on lung volumes and capacities in the healthy persons. Saudi Med J. 2007; 28: 1666–70. [PubMed Abstract].
- Chtourou H, Aloui A, Hammouda O, Haddad M, Souissi N, Chamari K, Chtourou H. Ramadan fasting and diurnal variation in sport performance. Effects of Ramadan fasting on health and athletic performance. 2013; OMICS Group eBooks. 3–11. [downloaded 2014 August 25]. Available from: http://www.esciencecentral.org/ebooks/effects-of-ramadan-fasting/ramadan-fasting-and-diurnal-variation.php [cited 25 July 2013]..
- Roky R, Iraki L, HajKhlifa R, Lakhdar Ghazal N, Hakkou F. Daytime alertness, mood, psychomotor performances, and oral temperature during Ramadan intermittent fasting. Ann Nutr Metab. 2000; 44: 101–7. [PubMed Abstract].
- Altuntas YE, Gezen FC, Sahoniz T, Kement M, Aydin H, Sahin F, etal. Ramadan fasting in patients with a stoma: a prospective study of quality of life and nutritional status. Ostomy Wound Manage. 2013; 59: 26–32. [PubMed Abstract].
- Aziz AR, Chia MY, Low CY, Slater GJ, Png W, Teh KC. Conducting an acute intense interval exercise session during the Ramadan fasting month: what is the optimal time of the day?. Chronobiol Int. 2012; 29: 1139–50. [PubMed Abstract].
- Aziz AR, Wahid MF, Png W, Jesuvadian CV. Effects of Ramadan fasting on 60 min of endurance running performance in moderately trained men. Br J Sports Med. 2010; 44: 516–21. [PubMed Abstract].
- Bouhlel H, Shephard RJ, Gmada N, Aouichaoui C, Peres G, Tabka Z, etal. Effect of Ramadan observance on maximal muscular performance of trained men. Clin J Sport Med. 2013; 23: 222–7. [PubMed Abstract].
- Brisswalter J, Bouhlel E, Falola JM, Abbiss CR, Vallier JM, Hausswirth C. Effects of Ramadan intermittent fasting on middle-distance running performance in well-trained runners. Clin J Sport Med. 2011; 21: 422–7. [PubMed Abstract].
- Chamari K, Haddad M, Wong del P, Dellal A, Chaouachi A. Injury rates in professional soccer players during Ramadan. J Sports Sci. 2012; 30(Suppl 1): S93–102. [PubMed Abstract].
- Karatoprak C, Yolbas S, Cakirca M, Cinar A, Zorlu M, Kiskac M, etal. The effects of long term fasting in Ramadan on glucose regulation in type 2 diabetes mellitus. Eur Rev Med Pharmacol Sci. 2013; 17: 2512–16. [PubMed Abstract].
- Trabelsi K, El Abed K, Stannard SR, Jammoussi K, Zeghal KM, etal. Effects of fed- versus fasted-state aerobic training during Ramadan on body composition and some metabolic parameters in physically active men. Int J Sport Nutr Exerc Metab. 2012; 22: 11–18. [PubMed Abstract].
- Trabelsi K, El Abed K, Trepanowski JF, Stannard SR, Ghlissi Z, Ghozzi H, etal. Effects of Ramadan fasting on biochemical and anthropometric parameters in physically active men. Asian J Sports Med. 2011; 2: 134–44. [PubMed Abstract] [PubMed CentralFull Text].
- Trabelsi K, Stannard SR, Ghlissi Z, Maughan RJ, Kallel C, Jamoussi K, etal. Effect of fed- versus fasted state resistance training during Ramadan on body composition and selected metabolic parameters in bodybuilders. J Int Soc Sports Nutr. 2013; 10: 23. [PubMed Abstract] [PubMed CentralFull Text].
- Trabelsi K, Stannard SR, Maughan RJ, Jammoussi K, Zeghal K, Hakim A. Effect of resistance training during Ramadan on body composition and markers of renal function, metabolism, inflammation, and immunity in recreational bodybuilders. Int J Sport Nutr Exerc Metab. 2012; 22: 267–75. [PubMed Abstract].
- Ziaee V, Kihanidoost Z, Younesian M, Akhavirad MB, Bateni F, Kazemianfar Z, etal. The effect of Ramadan fasting on outcome of pregnancy. Iran J Pediatr. 2010; 20: 181–6. [PubMed Abstract] [PubMed CentralFull Text].
- Van Praagh E. Anaerobic fitness tests: what are we measuring?. Med Sport Sci. 2007; 50: 26–45. [PubMed Abstract].