Abstract
During the last decade an increasing use of differentiated support measures for pupils with special educational needs, indicative of a discrepancy between educational policies and practices, has been witnessed in Sweden. Another trend has been the increased use of medical diagnoses in school. The aim of this study was to explore the main concern of support given to pupils with special educational needs and how pupils and parents experience and handle this. Interviews were conducted with eight pupils in Grades 7–9—and their parents—at two compulsory schools in a city in northern Sweden. A grounded theory approach was used for analyzing the interview data. A conceptual model was generated illuminating the main concern of special support measures for pupils and parents. The core category of the model, struggling for recognition and inclusion, was related to two categories, which further described how this process was experienced and handled by the participants. These categories were labeled negotiating expertise knowledge within a fragmented support structure and coping with stigma, ambivalence, and special support measures. The developed conceptual model provides a deeper understanding of an ongoing process of struggle for recognition and inclusion in school as described by the pupils and parents.
Introduction
Inclusive education has, in Sweden as in many other countries, been a prominent issue on the political agenda for a number of years. The main objective for Swedish education policy has been to create “a school for all,” with the aim of including all pupils—irrespective of disabilities—within mainstream education and, for those pupils with special educational needs, to provide support first and foremost within the ordinary class or group (SFS, Citation1994). In the 1970s, a new relational definition of disability that conceptualized disability in terms of an interplay between individual impairments and the design of the environment began to emerge. This re-orientation contested the medical, pathological perspective on pupils’ difficulties in school, i.e., that problems did not solely relate to the child, but also to the schools’ organization and practices of education. Haug (Citation1998Citation1999) points out that the earlier tradition of school work compensated for a lack of social justice by providing special education in segregated settings outside the classroom. Since 1970s onwards, educational policy in Sweden favored a democratic participatory interpretation of social justice, which laid the foundation for the “inclusive school” (Haug, Citation1999). Nevertheless, working in a small group or alone with a special educationalist/special teacher is still commonplace in many schools today. In addition, there has, during the last decade, been a trend to organize special classes for children with neuropsychiatric disabilities, e.g., autism, attention deficit/hyperactivity disorder (ADHD), Asperger and Tourette's syndrome. Such segregated support for pupils with neuropsychiatric disorders have been favored by experts and also relied upon by particular groups of parents to children with such disabilities (Börjesson, Citation1999a). This somewhat paradoxical development in school have been criticized since such practices are similar to the so-called “observation classes” or “educational clinics” that were commonplace during the 1960s (Börjesson, Citation1997; Börjesson & Palmblad, Citation2003). The rationale underpinning such practices implied that differentiation between groups of pupils was a device for the pupils’ own good. Hence, the traditional segregated character of special education has been difficult to change, even if the ideals and basic values articulated in official documents support more inclusive practices.
Furthermore, another trait of special support measures for pupils with special educational needs has been the intensified use of medical diagnoses in Swedish schools since the 1990s and onwards. Such diagnoses appear to have become more crucial in school for pupils with special educational needs in order to motivate and secure special support measures, even if pupils have to accept a segregated environment (cf. Heimdahl Mattson & Roll-Pettersson, Citation2007). At the beginning of the 21st century, scientific debates has taken place in Sweden between neuropsychiatric scholars and social scientists concerning the diagnosis of deficits in attention, motor control, and perception (DAMP) (cf. Börjesson, Citation1999b; Kärfve, Citation2000) and about the impact and power of similar diagnoses (Brante, Citation2006aCitationbCitation2007; Modigh, Citation2006Citation2007). These debates elucidate the lack of consensus on the validity and usage of such diagnoses. A similar debate regarding dyslexia/reading and writing difficulties has taken place focusing in a similar way an individually oriented diagnostic tradition and a more socially oriented anti-diagnostic tradition (Solvang, Citation1998).
Some scholars point to a “medicalization process” of pupils’ difficulties in school, implying that social problems are interpreted and explained in medical terms (Malacrida, Citation2004; Palmblad, Citation2000; Solvang, Citation1998Citation1999). Such a medicalization of a problem have both “bright” and “dark” sides, i.e., positive and negative social outcomes for the individual (Conrad, Citation1992; Conrad & Schneider, Citation1992). Within the school context, the positive outcomes of a medical label, e.g., dyslexia, are related to de-stigmatizing effects of lack of motivation, laziness, a low capacity to learn, and lack of support from parents. A medical label is also related to increased resource allocation to special education and social control with a humanitarian face, i.e., that the medical prestige makes the difficulties easier to handle (Solvang, Citation2007). In contrast, negative outcomes are supposed to mask social factors such as the impact of the organization of school work and the social situation of the family. Moreover, a medical label might also eradicate difference, i.e., eliminate or “treat” dyslexia and promote perfection and “normality,” instead of celebrating diversity (Solvang, Citation2007). The main criticism toward the medicalization of school problems thesis is that it tends to decontextualize and individualize what might otherwise be interpreted as collective social problems (Conrad, Citation1992). However, Solvang (Citation2007) points out that, although the positive outcomes of a medical label certainly may have an empowering potential on the individual level, the positive sides may also be problematic when seen from a structural perspective. They tend to expand medical interpretations to an increasing number of arenas and thereby obscure the impact of organizational and societal conditions on special education and special needs practices.
A relatively small proportion of research on special education has specifically focused on pupils’ and parents’ experiences of the support measures in school. Previous research has shown that pupils’ experiences of being taught in small groups are rather diverse (Westling Allodi, Citation2002) but leaving the regular class seems to create ambivalent feelings of the pupils (Heimdahl Mattsson & Roll-Pettersson, Citation2007). Furthermore, such support might also affect pupils’ peer relations in a negative way (Westling Allodi, Citation2000), and pupils’ self-images and self-esteem (Groth, Citation2007). The differentiated character of support measures such as small groups or remedial classes/special teachings groups has also shown to make pupils feel excluded and isolated from the other pupils (Groth, Citation2007; Ljusberg, Citation2009) and make them develop low agency and weak voices about themselves (Karlsson, Citation2007). There is also a risk that such organizational solutions are being experienced by the pupils as temporary solutions that limits these pupils’ participation in activities where other pupils are involved (Persson, Citation2008). Furthermore, studies on pupils with disabilities in school has shown that they experience it as essential that the teacher has knowledge about their impairments and special educational requirements necessary to meet such needs (Persson, Citation2008).
Another interesting aspect of special support is what the pupils themselves prefer. For example, a study in Greece reported that half of their informants preferred to receive support within the class, even though pupils were not familiar with such support (Vlachou, Didaskalou, & Argyrakouli, Citation2006). Such perceptions highlight that pupils have divergent views on appropriate support measures in school. In terms of attaining academic qualifications, class placement could affect achievement among students with special educational needs (Myklebust, Citation2006) and their occupational success on the labor market (Myklebust & Båtevik, Citation2009). Finally, from a parental perspective, parents to children with diagnostic difficulties has also been described as having to actively “struggle” for their children in order to receive appropriate support in school, as well as obtaining a diagnosis (Roll-Pettersson & Heimdahl Mattsson, Citation2007).
The increasing use of special classes/small groups and medical diagnoses in school give rise to questions about what both pupils and parents experience to be the main concern of special support measures in school, and how they deal with difficulties that relate to such support.
2 Aims of the study
The overall aim of this study was to examine how pupils with special educational needs and their parents experience the special support measures they receive from school. The research questions were as follows:
What is the main concern of special support given to pupils with special educational needs?
How do pupils and parents experience and handle this?
3 Method
3.1 The informants/participants
This study is based on interviews with pupils with special educational needs and with their parents.Footnote1 The study, which comprised a sample of pupils in Grades 7–9, was conducted in two compulsory schools in a city in northern Sweden. The pupils participating in the study had various difficulties in school, such as socio-emotional difficulties, learning, reading and writing difficulties, dyslexia, etc. The main reason for focusing on these kinds of difficulties was that they had proved to be quite common in an earlier study of individual educational plans conducted by the authors (Isaksson, Lindqvist, & Bergström, Citation2007).
As an initial attempt to recruit pupils, a letter containing information about the purpose of the study was published on both schools’ websites. Along with this letter, the parents and pupils were asked to fill in a web-based interest form and send it to one of the authors (JI) by e-mail. Due to limited number of responses, a second recruitment round was carried out. Pupils were selected from a list prepared in cooperation with special educationalists in both schools. An invitation to participate in the study was sent to the parents, which yielded an additional five participants. All in all, interviews with eight pupils with various special educational needs and their parents (six from one school and two from the other) were conducted. Of these eight pupils, seven had received a medical diagnosis; five having dyslexia and two ADHD (see ). The parents and pupils accepted to participate in the study. However, since almost all pupils were below, or had just reached, the age of 15 years, informed consent was given by both the parents and the pupils.
Table I. Participants in the study.
An interview guide was constructed thematically and the interviews were recorded and transcribed verbatim. Themes such as experiences of special support measures, the diagnosis, the pupil's history of school difficulties and parental collaboration with the school were topics covered in the interviews. The interviews were carried out in the informants’ own homes and each pupil and her/his parent/parents were interviewed together simultaneously. Initial questions were directed mainly to the pupil whilst subsequent questions focused more on the parent/parents’ experiences. Our impression was that the voices of the pupils were given adequate scope and that the parents did not dominate the interview situation at the expense of the child. Each interview lasted for between 45 and 90 mins and the pupils generally participated during the whole of the interview. However, when interviewing the two pupils’ with ADHD, it was agreed in advance that the child could leave after the initial questions if he/she wanted to.
We assured all the participants that the content of the interviews be treated confidentially so that none of the informants hardly could be identified. Neither the names of the participants, the schools, and the city or the municipality were to be mentioned when reporting the study, which is in line with the demands of confidentiality in ethical guidelines for research. Furthermore, all citations used were considered to be of non-sensitive character and the translation from Swedish to English language makes it even more difficult to identify specific participants.
Both of the schools in our study had similar processes of identifying pupils with special educational needs. Usually, the schools received documentation and were informed by staff from the previous school, e.g., about potential difficulties and previous support measures. Various tests related to the formulated knowledge goals were also used to assess the pupil's educational development. If no previous documentation was available, the pupil's special educational needs were usually identified by the regular class teacher who then made a referral to the relevant work team. Pupils’ difficulties were also assessed and judged on the basis of various (objective) test results related to knowledge goals, but also according to normative aspects assessed by means of observations of the child's behavior within class (cf. Isaksson, Lindqvist, & Bergström, Citation2009) for a more detailed description of the identification process in both schools).
3.2 A grounded theory approach
We chose to use the research method of grounded theory for this study. Grounded theory was originally developed by Glaser and Strauss (Citation1967) and provides a way to transform collected data systematically into more abstract forms of information in order to generate concepts and theories that fit empirical situations. Although the method originally had its roots within a positivist and, later, a post-positivist position (cf. Strauss & Corbin, Citation1990), a constructivist grounded theory aimed toward the interpretative understanding of the subject's meanings was later developed by Charmaz (Citation2003). Consequently, this position differs ontologically from the other positions since it assumes that social reality does not exist independently of human action. Furthermore, Charmaz argues that such a position “fosters the development of qualitative traditions through the study of experience from the standpoint of those who live it” (2003, p. 270). However, even if there are different ontological positions related to grounded theory, Charmaz states that grounded theory offers a set of flexible strategies, not rigid prescriptions. In this article, we adhere mainly to the constructivist version of grounded theory, since the focus is on pupils’ and parents’ experiences and an interpretation of how the subjects construct their realities, i.e., how they handle and ascribe meaning to the special support measures received in school.
3.3 Analysis
In accordance with the analytical process of grounded theory, we constructed a series of concepts as open codes, with the aim of organizing the data into meaningful categories or concepts that characterized important information in the interview material. This procedure of open coding also allowed us to make text comparisons within and between documents. During the process of coding, we followed the recommendations of Strauss (Citation1987, p. 30) and posed a specific and consistent set of questions to the data, e.g., what is the meaning of respondents’ views and in what way are statements relevant to the aims of our study? The initial open coding resulted in some background ideas or “sensitizing concepts” (cf. Charmaz, Citation2006; Starrin, Dahlgren, Larsson, & Styrborn, Citation1997) that were used as new points of departure from which to analyze our empirical data.
The initial coding procedure was followed by a clustering of the codes with similar content which were brought together in summarized categories. Thereafter, a more selectively focused coding of our empirical material took place in order to explore the relationship between categories and their properties. The selective coding also involved a recoding of previously assessed data, as well as posing theoretically refined questions regarding our data, in order to refine our categories. We also adhered to the constant comparison method of comparing data with data, and data with categories and core categories (cf. Charmaz, Citation2003; Hallberg, Citation2006). Finally, the categories and the conceptual model were compared with our data material in order to “saturate” the categories and groups (cf. Charmaz, Citation2006). A core category was identified, describing parents’ and pupils’ main concern of special support measures in school. This core category was central to the data and was related to two additional categories and their properties (subcategories) grounded in the data.
4 Results
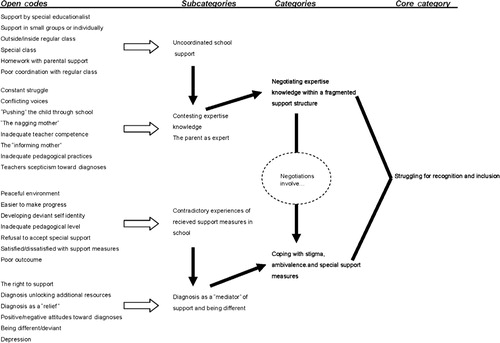
A conceptual model was generated illuminating that pupils and parents were struggling for recognition and inclusion by challenging expertise knowledge within a fragmented support structure using different strategies to deal with stigma, ambivalence, and special support measures (see ). Hence, the model intended to show how pupils and parents actively negotiated and coped with problems that occurred related to the support measures they were offered. The developed conceptual model provides a deeper understanding of an ongoing process of struggle for recognition and inclusion in school as described by the pupils and parents.
Figure 1. Audit trail describing the struggle for recognition and inclusion as a process.
4.1 Struggling for recognition and inclusion
The parents and pupils described their main concern of special support measures in school as a struggle for recognition and inclusion. This was identified as the core category of the study. The pupils and parents struggled to gain greater recognition of the child's difficulties related to a medical diagnosis by the school personnel, but also greater recognition of their suggestions/information about what they perceived as adequate support measures and specific teaching methods. Many parents had acquired substantial knowledge about their child's difficulties, the consequences of and conditions for, giving a diagnosis and proper teaching methods. However, the success of such suggestions from the parents varied among the participants. Due to uncoordinated support measures and dissatisfaction with the arrangements and the outcome of the support, pupils and parents claimed more inclusive support measures in school. Such inclusive practices did not necessarily imply support given within the pupil's ordinary class, but rather that the character of the support measures avoided singling out pupils as different/deviant and that the support was better coordinated with the ordinary class. Special support measures must not make pupils feel excluded in terms of participation with their classmates. In order to deal with the experienced main concern of the support measures the pupils and parents used various strategies, conceptualized as negotiating expertise knowledge within a fragmented support structure and coping with stigma, ambivalence, and special support measures. The categories, with their properties (subcategories), are described in the following section illustrated by means of quotations from the interviews.
4.2 Negotiating expertise knowledge within a fragmented support structure
Characteristics of this category are pupils’ and parents’ experiences of the structural arrangements of the special support and the collaboration with teachers on teaching methods and the design of the support measures. The participants experienced the support as uncoordinated and fragmentary. Such experiences created a scope for parents to contest the school personnel's expert knowledge and to engage in negotiations on the design and adequacy of the support measures.
4.2.1 Uncoordinated school support
A majority of the support received took place outside the regular classroom, either alone or in a small group with a special educationalist/special teacher (). Various special skills training outside the classroom with a special educationalist or a placement in a special class were used in all cases. Only some of the pupils had received in-class support, i.e., support by a special educationalist within the regular class. The support that was provided for outside the regular class was described by both pupils and parents as uncoordinated with teaching in the regular class. For example, pupils could miss out on important information given by the teacher in the regular class:
Well it was not that fun because you missed a lot of other lessons, you missed … what was it? … twenty minutes of some lessons. You missed when the teacher was going through problems/tasks, and this is very important.
4.2.2 Contesting expertise knowledge
The fact that all the pupils (except one) had a diagnosis brought to the fore conflicting voices concerning teaching methods, behavioral implications of specific diagnoses, and the design of support measures. The diagnosis was seen by the parents (and pupils) as implicit promises of adequate support for their children in school. Many of the parents explained that they had been informed by medical experts, or received information from other sources, on how their child's particular difficulties should be supported in school. However, their experience of encounters with staff at the schools told that they had to struggle to convince them on such issues since they often had differing opinions about the type of support that could be carried out. Although a medical diagnosis of school problems like ADHD and dyslexia often carries with it suggestions for adequate support measures, it is the responsibility of the staff at the school to “translate” the diagnosis into concrete educational support. On this matter, parents challenged the supposed expertise knowledge that teachers would have. The diagnosis and its implications for support measures were contested and became an issue for negotiation between the parents and the teachers in terms of the scope and adequacy of support measures.
Furthermore, some of the participants had also experienced skepticism from teachers toward both the diagnoses of ADHD and dyslexia. Some teachers expressed that the pupil was more or less lazy and disinterested in school, and that, with a little hard and systematic work problems in school could be overcome. Evidently, some teachers were not convinced that a diagnosis captured the pupil's real problems, i.e., they had not fully accepted the medical definitions of the various difficulties in school. This skepticism further complicated the collaboration between parents and teachers concerning the consequences of the diagnosis and the adequacy of provided support measures. Although some parents and pupils reported that the support increased after getting a diagnosis, such examples was the result of both pupils’ and parents’ struggles to obtain what they considered to be adequate support measures.
4.2.3 The parent as expert
Some of the parents expressed criticism over the perceived lack of adequate pedagogical measures to support pupils with difficulties such as dyslexia and ADHD. While the school claimed that they indeed possessed the knowledge about how to handle these difficulties and how to give these pupils adequate support, some parents questioned teachers’ competence and felt that they had to suggest appropriate measures to be taken. One of the parents described this like: “… It feels so frustrating for me to always be the one who have to come up with the solutions.” Another parent felt that her opinion on proper educational methods was ignored by the school and she said that teachers did not know what pedagogical working modes were the most suitable: “They made the ADHD-symptoms even worse due to their lack of knowledge and their reluctance to understand these children.” Evidently, the parents experienced that the description of the pupil's difficulties—crystallized in the language of diagnoses—was rarely translated into adequate support provision. The pedagogical practice of placing children with similar diagnosis in the same class was also criticized by one parent to a child with ADHD and portrayed as a temporary solution:
They sort of used their small group, and considered that they couldn't do anything else. They only had this small group where they could put them … since they couldn't stay in the regular class; they had to be alone by themselves.
Well I think that if they were open … i.e. they see pupils as being obstinate, troublesome and something that you … well you have for your own sins. But if they instead turned it around and saw the opportunities … because if they had started early with someone like him and saw that there were difficulties in reading, that they actually had thought about other ways for him to do this?
4.3 Coping with stigma, ambivalence, and special support measures
Characteristics of this category are the pupil's and parents’ experiences of the received special support measures and of having a medical diagnosis in school and the coping strategies that they developed on the basis of such experiences. Their experiences of the received support measures were contradictory and created ambivalent feelings that the pupils had to handle. The pupils also had to cope with stigmatizing effects of a medical diagnosis in school, but the diagnosis was also used as a coping strategy to reduce blame for both pupils and parents and to obtain support and specific rights within the school context.
4.3.1 Contradictory experiences of received support measures in school
Most of the pupils and parents thought that the support had been helpful, but to varying degrees. Although generally support was given outside the regular classroom, either alone or in small groups, many of the pupils were positive toward this way of working since it offered peace and quiet, something that they rarely obtained within the ordinary classroom. One of the pupils said: “Well it's better than just working in the classroom.” The pupils told that they were disturbed by other pupils in the ordinary classroom and the other way around, that they were told that they disturbed their classmates during lessons, and thus, for both of these reasons, a small group was considered to be more suitable by both pupils and teachers. However, the pupil's and parents’ also had negative experiences of the special support measures that they had to deal with. One of the pupils thought that the pedagogical level was far to low in the small group:
… Things are repeated … me and the boy from my class—he has more difficulties than me and I work on his level, and that is way too easy for me. So, I am sitting there and doing tasks that I already know.
Furthermore, although many pupils generally preferred to have support given individually or in small groups due to the more peaceful environment such arrangements provided, some of the parents described occasions when their child had refused to leave the regular class for special education support, even when the support was regarded as appropriate and appreciated. Such protests were, in part, directed toward a specific teacher's work methods but they were also related to stigmatizing experiences of having to leave the regular class. Such a strategy had the effect that the pupil could stay in the regular class for some time and/or the opportunity to receive support from another teacher. The ambivalent and somewhat contradictory feelings that the pupils expressed regarding the received special support also caused ambivalent coping strategies. This was perhaps best articulated by one of the pupils who said that:
I feel that it is good as well as bad. I miss so much … if I should stand still on the same spot, but it's also too hard within the ordinary class. I should be somewhere in between, so I don't know …
4.3.2 Diagnosis as a “mediator” of support and being different
Some of the pupils received their medical diagnosis at an early stage and did not remember how they reacted while those who had received it more recently told more about their perceptions. One pupil received his dyslexia diagnosis in the seventh grade and felt somewhat ambivalent about it: “No, I was a bit disappointed … I mean; it wasn't the funniest thing to get a diagnosis.” This pupil felt sad and a bit stupid because the diagnosis made him/her feel different from the classmates. He/she had difficulties handling this since it made him/her feel uncomfortable, depressed, and less self-confident. The two other pupils with the diagnosis ADHD reacted, according to their mothers, in the same way in terms of feelings depressed about being perceived as different. Such ambivalent experiences were difficult to cope with even though many pupils were familiar with their specific difficulties since other classmates or pupils in the school had such diagnoses. However, one of the pupils managed his/her problems in a different way and requested a test for dyslexia on his/her own initiative. In this case, the pupil felt relief when he/she received the diagnosis of dyslexia because it proved that: “it wasn't just some crazy idea I had.” Previously, this pupil had only received infrequent support measures since other pupils were prioritized for support. Therefore, the diagnosis was strategically used in order to receive additional support:
Well I have to … if I will receive support then I have to say “I really need this, I have a diagnosis so I should get it!” But if I only say that I can't handle this, that I don't understand, then they'll just say “well OK, but we will deal with that later.”
… I mean if there is something, then we want a diagnosis because we understood that it's much easier … and this was confirmed in the 7th grade by his teacher (who said) “how fortunate that he has a diagnosis because then we …” and then I thought “but what about those children who don't have one?.”
… The school thought that there were problems at home, that something was wrong at home. I heard that all the time; that he acted like he did because of that. So it was reassuring to get … and I continued to fight and told them that this was not the case since his other siblings were not like him … and then we finally received help and an ADHD-test and got it on paper (the diagnosis). And then the next battle with the school began, i.e. to receive the rights that these pupils should have.
5 Discussion and conclusions
In this study we set out to explore the main concern of special support given to pupils with special educational needs and how pupils and parents experience and handle this. The core category generated from our empirical data showed that both pupils and parents struggled for recognition and inclusion in school. This struggle indicated that they wanted to gain greater recognition of the child's special educational needs related to a medical diagnosis by the school personnel, but also greater recognition of their suggestions about what they perceived as adequate support measures and specific teaching methods. However, the success of such suggestions, which were often based on information they had obtained by themselves or from medical experts, varied among the participants. The main contribution of this article, we would argue, is that our generated conceptual model illuminates how pupils and parents struggle for recognition and inclusion in school and that this process of struggle involves both negotiations due to diverging interests of experts and strategies to deal with stigma, ambivalence, and special support measures. Hence, the model shows how pupils and parents actively negotiated and coped with problems that occurred related to the support measures and of having a medical diagnosis in school.
An interesting observation deriving from this study was that most of the support for pupils with special educational needs was individual support or support provided in the form of a small group of pupils outside their regular class. This finding is contrary to the intentions of Swedish educational policy (cf. Tideman, Rosenqvist, Lansheim, Ranagården, & Jacobsson, Citation2004), but in line with the observations that special classes or groups for pupils with special educational needs have increased in Sweden (National Agency for Education, Citation2007). The pupils’ and parents’ experiences of the special support given in this manner were both positive and negative and many of the informants had an ambivalent attitude toward the support (cf. Heimdahl Mattson & Roll-Pettersson, Citation2007). The findings from current studies were verified; receiving differentiated support measures seemed to contribute to ambivalent experiences in terms of feeling excluded and isolated from the other pupils in the regular class (Groth, Citation2007; Ljusberg, Citation2009). Although many pupils preferred to receive support measures outside the regular classroom, the ambivalent experiences were related to being singled out as different/deviant and the risk of limiting the participation with their classmates (cf. Westling Allodi, Citation2002). Furthermore, the fact that such support measures were experienced as uncoordinated with regular education and lacked pedagogical adequacy indicated that such support was perceived as temporary organizational solutions by both pupils and parents (Persson, Citation2008). Such experiences created a scope for the participants to contest the school personnel's expert knowledge of specific needs and special educational requirements to meet such needs, and engage in negotiations on the design and adequacy of the support measures.
The experiences of pupils and their parents of receiving a diagnosis related to special educational needs only in part confirm some of the bright and dark sides of medicalization that Solvang (Citation2007) has pointed out within the school context. The positive aspects of a medical label were related to a perception that a diagnosis could generate extra resources for special support in school, but it did not always have the de-stigmatizing effect one would expect in terms of leading to enhanced self-esteem and the removal of blame from the pupil and the parents. Sometimes it caused stigma, or at least ambivalence. A medical label also contributed to stigmatizing experiences in terms of depression (ADHD) and feeling stupid (dyslexia), i.e., the individual is seen as the source of her/his own problems and other social factors are afforded much less attention. Hence, medicalization need not always mean social control with a humanitarian face. Consequently, it seems that a medical label might contribute to contradictory experiences within the context of special education. However, these positive and productive outcomes of medicalization reported above are mainly grounded in the experiences of medical labeling on the individual and interactional level. Even if a medical diagnosis might contribute to the provision of extra resources within the broader welfare system, ultimately it is the responsibility of the school staff to decide how to implement such support. Therefore, in line with Solvang's arguments, we believe that it is important to broaden the perspective and also to interpret these positive aspects of a medical label from a structural perspective.
The different perspectives of medical and pedagogical professions seem to give rise to problems at the individual level that derive from the different ways of categorizing and describing the pupil's difficulties. Whilst the diagnosis may well capture the individual's difficulties, it may nevertheless be of little help to teachers in their daily work in supporting pupils with special educational needs (cf. Jakobsson, Citation2002; Zetterqvist Nelson, Citation2003). The results from this study indicate that the parents’ struggles could be related to lack of collaboration between groups of professionals, i.e., educators and medical professionals (cf. Malacrida, Citation2004). Therefore, many parents felt that they had to struggle with the school staff in order to have their child's difficulties recognized and convince the staff about adequate educational methods and solutions for their child (cf. Roll-Pettersson & Heimdahl Mattson, Citation2007). Parents and pupils negotiations of the design and content of support measures are crucial and medical diagnoses have proven to be essential vehicles in this context since they have both productive and restrictive consequences for pupils and parents. In order to cope successfully with experiences of stigma, ambivalence, and special support based on a medical diagnosis, a closer collaboration between parents/pupils, special educationalists, physicians, and psychologists is needed, especially since parents are, in a sense, the “experts” regarding their own child's particular needs. This study also points to the need to listen to the pupils’ own experiences of special educational support in school since such support seem to be more differentiated and organizationally fragmented. Even if the number of informants within this study was limited, the informant's experiences still provide valuable insights into some of the dilemmas of differentiated special support and perceptions of having a medical diagnosis in school.
6 Conflict of interest and funding
The project was financed by the Swedish Research Council (errand 721-2004-3315).
Acknowledgements
This article has been produced as part of the three-year project “Between normalcy and deviance—support for school children with special educational needs, 2005–2008.”
Notes
1. The project was approved by the Ethical Research Committee at the Medical Faculty, Umeå University (Dnr 02/401, approved 030211).
References
- Brante, T. (2006a). Den nya psykiatrin: exemplet ADHD [The new psychiatry: The example of ADHD]. In: G. Hallerstedt. Diagnosens makt: Om kunskap, pengar och lidande [The power of the diagnosis: On knowledge, money and suffering]. (pp. 73–111.). Gothenburg: Daidalos.
- Brante T. Om psykiatrikers kritiska syn på sociologi. Replik till Kjell Modigh [On psychiatrists’ critical view of sociology. Response to Kjell Modigh]. Socialvetenskaplig tidskrift. 2006b; 13(4): 376–380.
- Brante T. Psykologi och sociologi, arv och miljö. Replik till Kjell Modigh [Psychology and sociology, heredity and environment. Response to Kjell Modigh]. Socialvetenskaplig tidskrift. 2007; 14(1): 95–99.
- Börjesson M. Om skolbarns olikheter: Diskurser kring “särskilda behov” i skolan – med historiska jämförelsepunkter [On schoolchildren's differences: Discourses on “special needs” in school—with historical points of comparison]. Liber Distribution. Stockholm, 1997
- Börjesson M. Det historiska spelet om skolans förmåner [The historical gambling about the schools benefits]. Locus. 1999a; 2: 6–15.
- Börjesson M. A newspaper campaign tells. The launch of neuro-psychiatric diagnoses in the Swedish daily press 1997–1999. Scandinavian Journal of Disability Research. 1999b; 1(2): 3–25.
- Börjesson, M., & Palmblad, E. (2003). Problembarnets århundrade: normalitet, expertis och visionen om framsteg [The century of the troublesome child: Normalcy, expertise and the vision of progress]. Lund: Studentlitteratur.
- Charmaz K. Grounded theory. Objectivist and constructivist methods. Strategies of qualitative enquiry2nd ed. Denzin N. K. Lincoln Y. S. Sage. Thousand Oaks CA, 2003; 249–291.
- Charmaz K. Constructing grounded theory. A practical guide through qualitative analysis. Sage. London, 2006
- Conrad P. Medicalization and social control. Annual Review of Sociology. 1992; 18(1): 209–231.
- Conrad P. Schneider J. W. Deviance and medicalization. From badness to sickness. Temple University Press. Philadelphia PA, 1992
- Glaser B. G. Strauss A. L. The discovery of grounded theory. Strategies for qualitative research. Aldine. Chicago IL, 1967
- Groth D. Uppfattningar om specialpedagogiska insatser—aspekter ur elevers och speciallärares perspektiv [Perceptions on special educational measures—aspects from pupils’ and remedial teachers’ perspectives]. Doctoral dissertation, Luleå University of Technology. Luleå, 2007
- Hallberg L. R.-M. The “core category” of grounded theory: Making constant comparisons. International Journal of Qualitative Studies on Health and Well-being. 2006; 1(3): 141–148.
- Haug P. Pedagogiskt dilemma: Specialundervisning [Pedagogical dilemma: Special education]. National Agency for Education. Stockholm, 1998
- Haug P. Formulation and realization of social justice: The compulsory school for all in Sweden and Norway. European Journal of Special Needs Education. 1999; 14(3): 231–239.
- Heimdahl Mattson E. Roll-Pettersson L. Segregated groups or inclusive education? An interview study with students experiencing failure in reading and writing. Scandinavian Journal of Educational Research. 2007; 51(3): 239–252.
- Isaksson J. Lindqvist R. Bergström E. School problems or individual shortcomings? A study of individual educational plans in Sweden. European Journal of Special Needs Education. 2007; 22(1): 75–91.
- Isaksson, J., Lindqvist, R., & Bergström, E. (2009). ‘Pupils with special educational needs’: A study of the assessments and categorising processes regarding pupils’ school difficulties in Sweden. International Journal of Inclusive Education. , First published on: 22 September 2009 (iFirst).
- Jakobsson I. Diagnos i skolan: En studie av skolsituationer för elever med syndromdiagnos [Diagnosis at school: A study of school situations of pupils with a syndrome-diagnosis]. Doctoral dissertation, University of Gothenburg. Gothenburg, 2002
- Karlsson Y. Att inte vilja vara problem—social organisering och utvärdering av elever i en särskild undervisningsgrupp [Resisting problem talk—social organization and evaluation practices in a special teaching group]. Doctoral dissertation, Linköping University. Linköping, 2007
- Kärfve E. Hjärnspöken. Damp och hotet mot folkhälsan [Figments of brain. DAMP and the threat to public health]. Brutus Östling. Stockholm, 2000
- Ljusberg A.-L. Pupils in remedial classes. Doctoral dissertation, Stockholm University. Stockholm, 2009
- Malacrida C. Medicalisation, ambivalence and social control: Mothers’ description of educators and ADD/ADHD. Health. 2004; 8(1): 61–80.
- Modigh K. Om sociologers kritiska syn på psykiatrin [On sociologists’ critical view of psychiatry]. Socialvetenskaplig tidskrift. 2006; 13(4): 370–375.
- Modigh K. Sänk garden Thomas Brante! [Lower your guard Thomas Brante!]. Socialvetenskaplig tidskrift. 2007; 14(1): 91–94.
- Myklebust J. O. Class placement and competence attainment among students with special educational needs. British Journal of Special Education. 2006; 33(2): 76–81.
- Myklebust J. O. Båtevik F. O. Earning a living for former students with special educational needs. Does class placement matter?. European Journal of Special Needs Education. 2009; 24(2): 203–212.
- National Agency for Education. (2007). Skolverkets utbildningsinspektion: en sammanfattning av resultat och erfarenheter under tre år [National agency for educations’ inspection of education: A summary of results and experiences during three years]. Stockholm: National Agency for Education.
- Palmblad E. Diagnostics and ideology. Scandinavian Journal of Disability Research. 2000; 2(1): 58–81.
- Persson B. On other people's terms: Schools’ encounters with disabled students. European Journal of Special Needs Education. 2008; 23(4): 337–347.
- Roll-Petterson L. Heimdahl Mattson E. Perspectives of mothers of children with dyslectic difficulties concerning their encounters with school: A Swedish example. European Journal of Special Needs Education. 2007; 22(4): 409–423.
- SFS. (1994). SFS 1994:1194. Grundskoleförordning [The Swedish compulsory school ordinance]. Most recent change 2009-01-01. Stockholm: Allmänna förlaget.
- Solvang P. Velferdstatens problemlogik i lys av en debatt om dysleksi [The logic of problems in the welfare state in a debate about dyslexia]. Sociologisk forskning. 1998; 2: 5–24.
- Solvang P. Medikalisering av problem i skolan [Medicalisation of problems in school]. Locus. 1999; 2: 16–29.
- Solvang P. Developing an ambivalence perspective on medical labelling in education: Case dyslexia. International Studies in Sociology of Education. 2007; 17(1–2): 79–94.
- Starrin B. Dahlgren L. Larsson G. Styrborn S. Along the path of discovery. Qualitative methods and grounded theory. Studentlitteratur. Lund, 1997
- Strauss A. Qualitative analysis for social scientists. Cambridge University Press. New York, 1987
- Strauss A. Corbin J. Basics of qualitative research. Grounded theory procedures and techniques. Sage. Newbury Park CA, 1990
- Tideman M. Rosenqvist J. Lansheim B. Ranagården L. Jacobsson K. Den stora utmaningen. Om att se olikhet som resurs i skolan [The big challenge. Regarding difference as a resource in school]. Halmstad tryckeri AB. Halmstad, 2004
- Vlachou A. Didaskalou E. Argyrakouli E. Preferences of students with general learning difficulties for different service delivery modes. European Journal of Special Needs Education. 2006; 21(2): 201–216.
- Westling Allodi M. Self-concept in children receiving special support at school. European Journal of Special Needs Education. 2000; 15(1): 69–78.
- Westling Allodi M. Support and resistance. Ambivalence in special education. Doctoral dissertation, Stockholm Institute of Education. Stockholm, 2002
- Zetterqvist Nelson, K. (2003). Medfödd ordblindhet: Lanseringen av en diagnos för 100 år sedan—och idag [Inborn word blindness. The launching of a diagnosis 100 years ago—and today]. In M. Börjesson & E. Palmblad Problembarnets århundrade: normalitet, expertis och visionen om framsteg [The century of the troublesome child—Normalcy, expertise and the vision of progress]. (pp. 55–92.). Lund: Studentlitteratur.