
Abstract
Group A rotavirus infections cause diarrhea in infants and primarily occur in winter. These viruses are characterized by the viral structural proteins VP7 (G subtypes) and VP4 (P subtypes). Current treatments employ vaccines combined with symptomatic treatments. Through a review of published papers from 2003–2013, which included articles, theses, dissertations and academic conference proceedings in PubMed and CNKI (China National Knowledge Infrastructure), we examined the epidemiological and clinical studies conducted in the 7 regional administrative geographical divisions of the People's Republic of China. Binning of the clinical studies provided a quantitative synthesis of the published incidences of rotavirus-positive numbers, the infection rates and the distributions of different subtypes in the provinces. In an investigation of the 32 provincial administrative regions from 1994–2013, the number of positive infections in children, primarily ≤ 5 years of age, was highest in Guangdong (187,000 cases), Zhejiang (133,000 cases) and Hubei (11,000 cases) Provinces; the provinces that displayed the highest positive rates were Henan (75.20%), Jilin (64.94%) and the Ningxia Hui Autonomous Region (60.16%). Furthermore, the virus, which causes diarrhea, can also infect adults. Statistics regarding the rotavirus subtypes indicated that the top 3 G-subtypes reported were G3 (8,509 cases), G1 (6,490 cases) and G2 (1,601 cases); the top 3 P-subtypes reported were P[8] (8,483 cases), P[4] (2,017 cases) and P[6] (740 cases). The majority of clinical treatments for these infections comprised a combination of Chinese traditional and Western medicines, together with nursing and the administration of a variety of oral liquids to relieve symptoms. The top 3 positive rates were identified in provinces at higher latitude, which confirms increases in humidity and ambient temperature reduce the rotavirus infection rate and the number of rotavirus infections tends to be highest under cool, dry conditions. However, the presence of rotavirus in low-latitude provinces likely indicates living habits, living environments, and education level influencethe precautions and vaccine utilization rate. The traditional subtypes are the rotavirus G- and P-subtypes, thus allowing for the development of vaccines. In China, the treatments that are primarily used to combat the infection are integrative medicines combining a variety of nursing and adjuvant therapies.
Introduction
Rotavirus(RV) is an intestinal virus belonging to the reoviridae family.Citation1 This type of virus was first described in the 1970s. RV can cause autumn diarrhea. Seven types of RV have been described, designated A to G. Among these types, group A causes 90% of the infections observed in human infants and children. Therefore, almost every child ≤ 5 years old has been infected by a rotavirus at least once.Citation2 However, a single virus infection strengthens the immunocompetence of an individual and will lower the chance of future infections.Citation3 Therefore, adults are rarely infected withrotavirus.Citation4
The RNA-based genome of group A rotaviruses is double-stranded and linear. These genomes encode 11 genes (VP1, VP2, VP3, VP4, VP5, VP6, VP7, NSP1, NSP2, NSP3, NSP4, NSP5 and NSP6) (). The order of the genes in the genome for these viruses is VP7-VP4-VP6-VP1-VP2-VP3-NSP1-NSP2-NSP3-NSP4-NSP5/6. Additionally, the expression pattern of the rotavirus genotype is Gx-P[x]-Ix-Rx-Cx-Mx-Ax-Nx-Tx-Ex-Hx, where x is the number of copies of a certain type of gene. We traditionally abbreviate the viruses as GxP[x].Citation5
Figure 1. The rotavirus gene structure. A: The names and locations of rotavirus genes;Citation6 B: Polyacrylamide gel electrophoresis image of the rotavirus genome and the function of its genes.Citation7
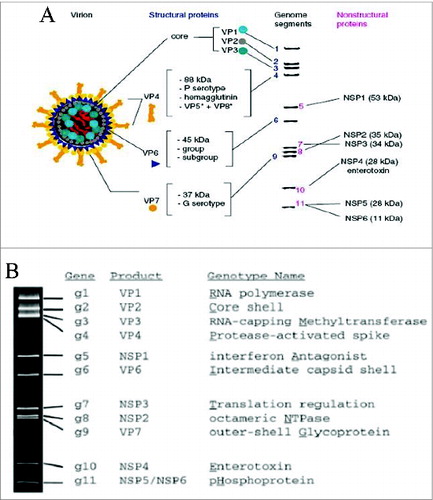
In epidemiology, immunology, microbiology, vaccine development and other related industries, the genes VP7 and VP4 are mainly used to define rotavirus types. The sequence of VP7 is defined as G-type(glycoprotein antigen), and the sequence of VP4 is defined as P-type (proteinase). The G- and P-types also display many subtypes. Coating the VP4 and VP7 proteins prevents infection.Citation8 Epidemiological studies have found that the genotypes of wild strains change from time to time. However, the G-and P-subtypes evolve at a slower rate compared with other viruses. The variations in the G- and P-subtypes are concentrated in several major subtypes. Rotaviruses are most commonly identified as the cause of severe gastroenteritis in children <5 y old. In China, published data show that rotavirus-associated hospitalizations account for 32% to 50% of all hospitalizations attributed to diarrhea among infants and children < 5 y old.Citation9-13
According to data from the National Bureau of Statistics of the People's Republic of China, China had a population of 1.35 billion people at the end of 2012,16.38 million of which were newborns. The mortality rate of infants and children less than 5 y of age was 13.2%.Citation14 A 2012 survey indicated that at the end of 2008, the annual mortality rate in infants and children under 5 as a result of rotavirus infections was 0.58%, which accounted for 3.1% of all deaths in this age bracket. On mainland China, rotavirus infections primarily occur between October and March. In Hong Kong, the epidemic typically occurs from November to May, whereas in Taiwan, rotavirus epidemics are prone to occur from December to May. The prevention and treatments of rotavirus infections on the Chinese mainland cost636 million USD (Yuan 4.70 billion) between 2001–2008; in Hong Kong, this figure was8.3 million USD (HK 64.7 million), and in Taiwan, it was8.3 million USD (NT 830 million).Citation15
There is no current cure for rotavirus infections. Therefore, clinical treatments for rotavirus infections usually adopt vaccines as a preventative measure and, after infection, employ drugs combined with auxiliary treatments to relieve symptoms. On the Chinese mainland, the Department of Viral Diarrhea, the National Institute of Viral Disease Control and Prevention and the Chinese Center for Disease Control and Prevention (CDCC)Citation16 are the leading agencies involved in policy formulation, epidemiological surveillance and the control of rotavirus infections. These departments have established numerous disease surveillance hospitals throughout the provinces to monitor rotavirus epidemiology and outbreaks.
To successfully develop rotavirus vaccines and reasonable treatments in China, a full review of intermediate- and long-term rotavirus-focused epidemiological studies is needed. Therefore, nearly 20 y of data covering the distribution of the general rotavirus, the G-subtypes and the P-subtypes are reviewed and reported here.
Results
Epidemiological survey
Fromthe2003–2013 publications, we identified421 and 9,299 published papers in PubMed and CNKI (Chinese National Knowledge Infrastructure), respectively, in the initial screening. These sources included periodical articles, theses, dissertations and academic conference proceedings. Two hundred duplicate records were removed after the initial screening. An additional 4,000 papers were removed because the studies focused only on the pathogenic mechanism and did not provide a description of the patient characteristics. Overall, 5,520 full-text articles were analyzed. Of these reports, 4,973 entries were removed because they lacked complete and explicit information. Therefore, 547 studies were ultimately included in the quantitative synthesis ().
Figure 2. Eligibility of studies for inclusion in this systematic review. The initial search identified 9,720 rotavirus-related citations from CNKI and PubMed. Five hundred 4seven studies that passed the inclusion and exclusion criteria were included in the pooled analysis.
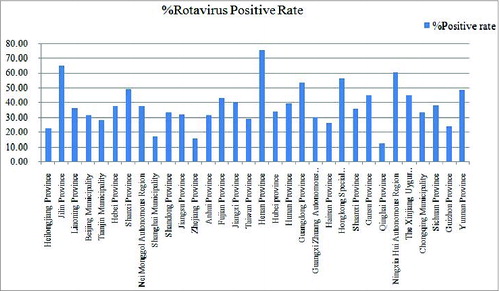
We applied epidemiological statistics (Table S1, and ) according to the data published from sentinel hospitals, other hospitals, CDCs of the provinces or cities, health care centers and universities. The positive testing methods included PAGE, EIA, ELISA, RT-PCR and the use of a colloidal gold device. The children described in these reports were ≤ 5 years old; however, adults were also reported to be infected with the group A rotavirus.Citation17 The top 3 provinces that displayed the most cases of infection were Guangdong (186,587 cases), Zhejiang (133,390 cases), and Hubei (11104 cases). In contrast, the top 3 provinces with the highest infection rates were Henan (75.20%), Jilin (64.94%) and the Ningxia Hui Autonomous Region (60.16%).
Figure 3. Epidemiological investigation of positive rotavirus cases. As shown in the figure, the top 3 provinces that displayed the most cases of infection were Guangdong, Zhejiang and Hubei Provinces.
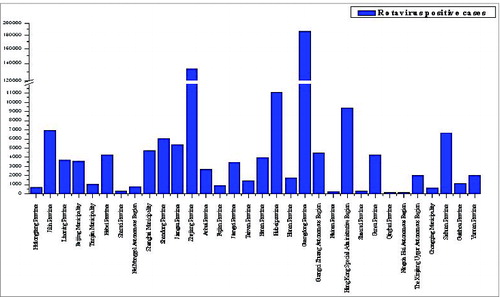
Figure 4. Epidemiological investigation of rotavirus positivity rates. As shown in the figure, the top 3 provinces that displayed the highest rates of infection were Henan Province, Jilin Province and the Ningxia Hui Autonomous Region.
Subtype statistics
The identified studiesthat used RT-PCR and sequencing techniques revealed the distributions of VP7 genotypes (G subtypes) (Table S2, , and ) and VP4 genotypes (P subtypes) in the provinces and the entire nation (Table S3, , and ). The top 3 populations ofthe G-subtypes were the G3 subtype (8,509 cases), G1 subtype (6,490 cases)and G2 subtype (1,601 cases); the top 3 populations ofthe P-subtypes were theP[8] subtype (8,483 cases), P[4] subtype (2,017 cases) and P[6] subtype (740 cases).
Figure 5. Epidemiology of VP7 subtypes in China. As shown in the figure, the top 3 subtypes were G3, G1 and G2.
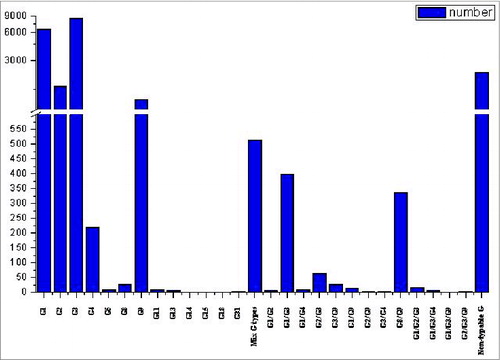
Figure 6. Distributions of group A rotavirus VP7 genotypes (G-types).
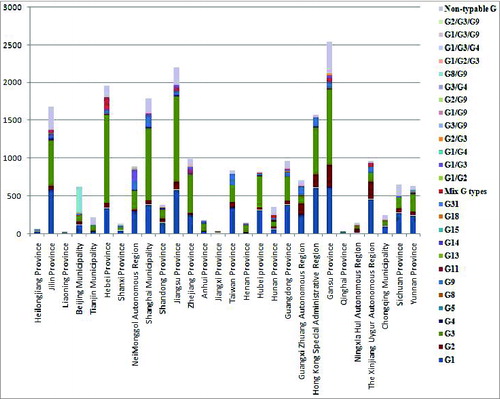
Figure 7. Epidemiology of VP4 subtypes in China. As shown in the figure, the top subtypes were P8, P4 and P6.
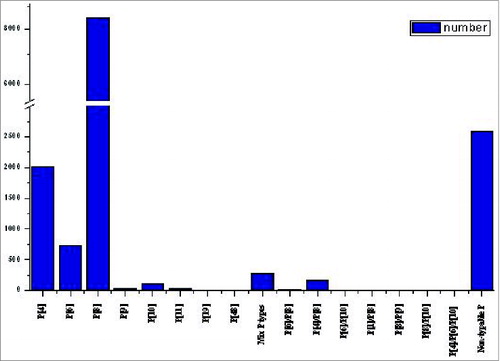
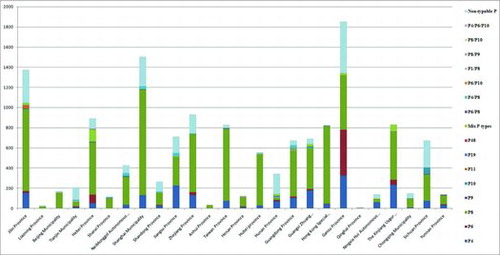
Figure 8. Distributions of group A rotavirus VP4 genotypes (P-types).
Analysis of clinical treatments
The statistics from the papers published by hospitals, CDCs, healthcare centers and universities (Table S4) focused on clinical manifestations in children and the treatment of symptoms. The clinical manifestations noted in children were gastroenteritis, parenteral multiple organ injury and other syndromes, such as liver damage, myocarditis, benign convulsion, enteritis, transaminase and changes in the myocardial enzyme spectrum, and rotavirus infection usually induced asthma and central nervous system damage. The applied clinical treatments included Chinese traditional medicine combined with Western medicine, auxiliary foods and oral liquids. The drugs that were commonly employed in the treatment of symptoms included ribavirin, cimetidine, virazole, potassium sodium dehydroandroandrographolide succinate, xiyanping and dioctahedral smectite. Furthermore, clinical nursing and adjuvant therapies were effective in relieving symptoms, typically through the administration of an oral salt solution with low permeability, such as lactose-free milk or zinc gluconate, and by providing nutrition.
Discussion
In this review, we analyzed the data from all of the available published articles. This applied method was inexpensive and was conducted on the internet in a short period of time. Most of the children mentioned in these studies, which covered a large time-span, were considerably older by the time of the analysis than in the original study. Therefore, fresh samples could not be collected from these individuals for clinical analysis. Thus, this retrospective research was useful for these cases.
These cases originated from provinces, autonomous regions, municipalities and special administrative regions in the territories of the People's Republic of China. Notably, the top 3 provinces with the highest infection rates were Henan (75.20%), Jilin (64.94%)and the Ningxia Hui Autonomous Region (60.16%), all of which are located in high latitude regions; these findings confirm reports that increases in humidity and ambient temperature reduce the rotavirus infection rate, and that the number of rotavirus infections tends to be highest under cool, dry conditions.Citation18,19 However, the top 3 provinces that displayed the most cases of infection were Guangdong (186,587 cases), Zhejiang (133,390 cases), and Hubei (11,104 cases), all of which are located in low latitude regions; these findings suggest living habits, living environments, and education level influence the precautions and vaccine utilization rate.Citation20 If a vaccine to prevent rotavirus infectionis not available, the epidemic situation may remain for a period of time in the future.
According to previous research, we determined that rotavirus infections in children primarily occurred from 6 months to 3 y of age. Therefore, we can expect infections to continue to occur in this age group if vaccinations are not provided.
Furthermore, the data that were analyzed via RT-PCR and sequencing techniques revealed the distributions of VP7 genotypes (G subtypes) andVP4 genotypes (P subtypes) in the provinces and the entire nation. The top 3 populations of the G-subtypes were the G3 subtype (8,509 cases), G1 subtype (6,490 cases) and G2 subtype (1,601 cases); the prevalence of G9, which was once rarely discovered, had an obvious tendency of growth, and it may evolve into a major epidemic strain in the future. The top 3 populations of the P-subtypes were the P[8] subtype (8,483 cases), P[4] subtype (2,017 cases) and P[6] subtype (740 cases); there were no other P subtypes with their own growth trend.
The data discussed in this report originated from sentinel hospitals, various provinces and cities, CDCs, healthcare centers and universities. The sentinel hospitals are set in densely populated metropolitan centers or health-conscious villages. However, the dataset lacked information covering prefecture-level cities and poor villages without established sentinel hospitals. Additionally, vital statistics missing from the data included an analysis of virus carriers in the floating population and the flow of the virus between different times and areas. Epidemiological studies on rotavirus are rarely published annually and often lack information regarding diarrhea cases, rotavirus positive cases, the sex ratios of patients and subtype profiles. Moreover, identical cases were included in different articles, causing repeats within the patient statistics. All of these factors influenced the observed epidemiological trends. Furthermore, several areas, such as the Macao Special Administrative Region and Tibet Autonomous Region, lacked any papers published after 2003 in PubMed and CNKI. Therefore, the epidemiological statistics cover only 32 provincial administrative regions.
To diagnose rotavirus infections and separate these infections from the more general cases of diarrhea, practitioners have employed enzyme immunoassays (EIA), polyacrylamide gel electrophoresis (PAGE), enzyme-linked immunosorbent assays (ELISA), electron microscopy (EM), RT-PCR and colloidal gold devices. The patients were primarily ≤5 years old, although adults also exhibited group A rotavirus infections.Citation17 Overall, the rotavirus infection rate was 28.4%. Therefore, infants and children with diarrhea should be tested for rotavirus infection.
The identification of rotavirus subtypes depended on a combination of RT-PCR and sequencing analyses. These methods are sensitive and accurate (displaying fewer false positive results). However, the statistics covering subtypes did not always match the total numbers. This disparity was caused by several samples displaying low quality, meaning that RNA could not be extracted. Additionally, several studies noted that the RNA extracted from several samples presented a low quality of rotavirus RNA. Therefore, sequencing (and in several cases PCR) could not be successfully performed on these low-quality RNA pools.
In China, the treatments for rotavirus infections primarily employ vaccines as a preventative measure and mitigate the symptoms after infection. Three problems in vaccine development must be addressed: the rotavirus mutation rates; the effectiveness of the vaccines; and the safety of the vaccines. Additionally, the development of vaccines concentrates on 2 questions: whether the vaccines can prevent rotavirus infection and whether the vaccines can reduce the lethality of rotavirus diarrhea and other manifestations.Citation5 Two vaccines have been developed and are currently sold globally: Rotarix21 and RotaTeq.22 In China, clinical treatments for rotavirus infections involve the use of traditional Chinese medicines combined with Western medicine, supplemented with nursing and the oral administration of a variety of liquids.
This reviewinvestigated32 provinces over 20 y However, several limits to the applied methods were noted in this study. First, the data were collected from published papers and may have repeat cases reported by the same work unit. Additionally, in numerous studies, the raw data were not published. Notably, the Macao Special Administrative Region and Tibet Autonomous Region lacked any published reports after 2003 in both PubMed and CNKI.
The data compiled in this review are intended to provide useful information for future research on epidemics, pathogenic mechanisms, clinical treatments and vaccine development and even for determining governmental policies.
Materials & Methods
Search strategy
Scientific articles published in English or Chinese were identified in the PubMed (United States) and CNKI databases. The standardized medical subject heading (MeSH) terms “rotavirus” and “China” were used to search the PubMed database, and the term “rotavirus” was used to search the CNKI database.
Definition
To be identified in our searches, the articles must have included the keywords “epidemic”, “medicine”, “nurse” and “China”. Additionally, thestudies must have examined rotavirus infectionsor treatments for diarrhea in infants and children. Seven administrative regions (Northeast, North China, East China, Central China, South China, Northwest and Southwest) divide the territory of the Republic of China; these regions are further divided into32 provincial administrative regions. Within these provinces, the epidemiological studies and clinical treatment reports published by sentinel hospitals and coherent units from 2003–2013 were identified. These studies reported the number of patients identified in the People's Republic of China, the incidence of diarrhea and the number of samples collected that were representative of the G- and P-subtypes. The results included provincial and national incidences of rotavirus positivity, the number and distribution of different subtypes and basic clinical research.
Review strategy
The papers were screened in the CNKI and PubMed websites. Each study was assigned a unique identifier to track the reviews and analysis following the initial title/abstract screening. Endnote® (version Ⅶ, Thomson Reuters, Inc.)bibliographic software was used to create an electronic library of the citations identified in the database searches. PubMed searches were performed using Endnote®, and duplicate records were deleted. To accurately identify the records, the initial text proofread from the CNKI and PubMed website was reviewed for each article.
A pilot study was conducted to refine the questionnaire for quality assessment of the inclusion/exclusion criteria. The principles of Transparent Reporting of Systematic Reviews and quantitative synthesis were implemented throughout the study.
Study inclusion and exclusion criteria
Each included publication was required to include a description regarding the epidemiological or diagnosis characters related to an epidemiological study and/or clinical research; publications that focused only on the pathogenic mechanism were not considered. Additionally, the data from studies reported over similar times for identical regions were averaged. The articles were screened to determine the distributions of the positive incidences of rotavirus infection, the G-and P-types and the clinical treatments; the important factors were calculated for the 32 provincial administrative regions.
Synthesis strategy
Microsoft office Excel® (version 2007, Microsoft, Inc.) and Originpro® (version 8E, OriginLab, Inc.)were used for the quantitative synthesis and creation of figures. The tables present the study durations, children'sages, detection assays, diarrhea cases, Rotavirus positive cases, G types and P types. The positive rates were expressed the rotavirus positive cases as the percentage of divided diarrhea cases.
Author Contributions
Xiao Nan drafted the initial paper and led the reviews, analyses and preparation of the final submitted version. Wu Jinyuan and Zhou Yan provided technical leadership and contributed to the preparation and editing of the manuscript. Sun Maosheng and Li Hongjun checked the final paper for intellectual content.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Supplementary_Tables.docx
Download MS Word (40.6 KB)Funding
This research was financially supported by the National High the National High Technology Research and Development Program (National 863 Project, 2012AA02A404); the Yunnan Research Program of Application Foundation and Advanced Technology, self-raised funds (project number:2013FZ140); and the State Project For Essential Drug Research and Development, the national “Twelfth Five-Year” plan (project number: 345 2014ZX09102041004); the PUMC Youth Fund and the Fundamental Research Funds for the Central Universities (project number: 33320140082); This research was financially supported by Science and Technology plan Project of Yunnan Province(2014BC008). The funding did not affect the study design, data collection or analysis. The authors were solely responsible for the design, data collection, and analysis.
Related Research Data
References
- Dennehy PH. (2000) Transmission of rotavirus and other enteric pathogens in the home. Pediatr. Infect. Dis. J 19(10 Suppl):S103-5; PMID:11052397; http://dx.doi.org/10.1097/00006454-200010001-00003
- Velázquez FR, Matson DO, Calva JJ, Guerrero L, Morrow AL, Carter-Campbell S, Glass RI, Estes MK, Pickering LK, Ruiz-Palacios GM. Rotavirus infections in infants as protection against subsequent infections. N. Engl. J. Med 1996; 335(14):1022-8; PMID:8793926
- Linhares AC, Gabbay YB, Mascarenhas JD, Freitas RB, Flewett TH, Beards GM. Epidemiology of rotavirus subgroups and serotypes in Belem, Brazil: a three-year study. Ann. Inst. Pasteur Virol 1988; 139(1):89-99; PMID:2849961
- Bishop RF, Davidson GP, Holmes IH, Ruck BJ. Virus particles in epithelial cells of duodenal mucosa from children with acute non-bacterial gastroenteritis. Lancet1973 2(7841):1281-3; PMID:4127639
- Matthijnssens J, Ciarlet M, Rahman M, Attoui H, Bányai K, Estes MK, Gentsch JR, Iturriza-Gómara M, Kirkwood CD, Martella V. Recommendations for the classification of group A rotaviruses using all 11 genomic RNA segments. Arch Virol 2008; 153(8):1621-9; PMID:18604469
- Nakagomi T, Nakagomi O. A critical review on a globally-licensed, live, orally-administrable, monovalent human rotavirus vaccine: Rotarix. Expert Opin Biol Ther 2009; 9(8):1073-86; PMID:19591630; http://dx.doi.org/10.1517/14712590903103787
- Patton JT. Rotavirus diversity and evolution in the post-vaccine world. Discov Med 2012; 13(68):85-97; PMID:22284787
- Pesavento JB, Crawford SE, Estes MK, Prasad BV. Rotavirus proteins: structure and assembly. Curr. Top. Microbiol. Immunol 2006; 309:189-219; PMID:16913048
- Fang ZY, Wang B, Kilgore PE, Bresee JS, Zhang LJ, Sun LW, Du ZQ, Tang JY, Hou AC, Shen H, et al. Sentinel hospital surveillance for rotavirus diarrhea in the People's Republic of China, August 2001–July 2003. J Infect Dis 2005; 192:s94-99; PMID:16088812
- Sun LW, Tong ZL, Li LH, Zhang J, Chen Q, Zheng LS, Liu J, Xie HP, Wang CX, Zhang LJ, et al. Surveillance finding on rotavirus in Changchun children's hospital during July 1998-June 2001.2003. Zhonghua Liu Xing Bing Xue Za Zhi 2003; 24(11):1010-2. [In Chinese]; PMID:14687501
- Tong ZL, Ma L, Zhang J, Hou AC, Zheng LS, Jin ZP, Xie HP, Ma L, Zhang LJ, Ivanoff B, et al. Epidemiological study of rotavirus diarrhea in Beijing, China - a hospital-based surveillance from 1998–2001. Zhonghua Liu Xing Bing Xue Za Zhi 2003; 24(12):1100-3. [In Chinese]; PMID:14761624
- Wang XY, Riewpaiboon A, von Seidlein L, Chen XB, Kilgore PE, Ma JC, Qi SX, Zhang ZY, Hao ZY, Chen JC, et al. Potential cost-effectiveness of a rotavirus immunization program in rural China. Clin Infect Dis 2009; 49(8):1202-10; PMID:19739973; http://dx.doi.org/10.1086/605632
- Orenstein EW, Fang ZY, Xu J, Liu C, Shen K, Qian Y, Jiang B, Kilgore PE, Glass RI. The epidemiology and burden of rotavirus in China: a review of the literature from 1983 to 2005. Vaccine 2007; 25(3):406-13; PMID:6668726
- National Bureau of Statistics of the People of the People's Republic of China. ( Access at http://data.stats.gov.cn/workspace/index?m=hgnd.)
- Kawai K, O'Brien MA, Goveia MG, Mast TC, El Khoury AC. Burden of rotavirus gastroenteritis and distribution of rotavirus strains in Asia: a systematic review. Vaccine 2012; 30(7):1244-54; PMID:22212128; http://dx.doi.org/10.1016/j.vaccine.2011.12.092
- Department of Viral Diarrhea, National Institute of Viral Disease Control and Prevention, China Center for Disease Control and prevention(CDCC) ( Access at http://www.ivdc.chinacdc.cn/jypx/)
- Shen Z, Wang G, Zhang W, Qian F, Li Y, Zhang M, Gu S, Wang M, Lin F, Hu Y, et al. Rotavirus infection and its genetic characterization in non-hospitalized adults with acute gastroenteritis in Shanghai, China. Arch Virol. 2013 Aug;158(8):1671-7.
- Wang H. Molecular Epidemiology of Rotavirus among Children under 5 Years old Hospitalized for Diarrhea in three Regions of China. Beijing: China Center for isease Control and prevention. 2009:21-56. (In Chinese)
- The introduction of the rotavirus vaccine Rotarix ( access to https://www.gsksource.com/gskprm/en/US/adirect/gskprm?cmd=ProductDetailPage&product_id=1244173585205&featureKey=600594)
- The introduction of the rotavirus vaccine RotaTeq ( access to http://www.fda.gov/biologicsbloodvaccines/vaccines/approvedproducts/ucm094063.htm)