Background
Over the last decade, facial vascularized composite allotransplantation (VCA) has earned its place at the top of the reconstructive ladder. However, as in free tissue transfer, post-operative revisions are necessary to achieve optimal functional and aesthetic results. Although revising a facial VCA may potentially risk the integrity of the graft, we believe that the advantages of appropriately chosen revisions may provide great benefit.
Methods
Following the most extensive face transplant performed to date, revisions were performed in 2 surgical procedures. The first included a Le Fort 3 osteotomy for malocclusion correction, midface tissue resuspension and coronal eyebrow lift to correct soft tissue ptosis, and submental lipectomy. Bilateral blepharoplasty to minimize tissue excess and scar revision were done at a subsequent operation. Cephalometric analysis and angiography were performed and blink data collected.
Results
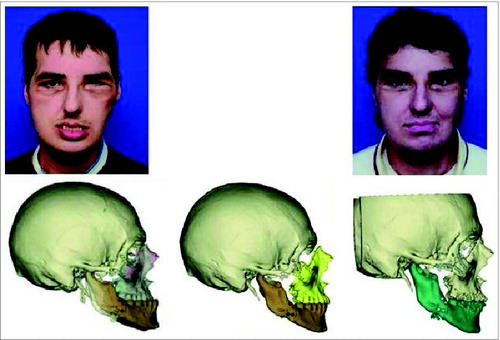
Pre-transplant, the patient was in class 3 malocclusion (Fig. 1). Post-transplant, class 1 occlusion was obtained, however, the patient subsequently returned to class 3 occlusion. After skeletal revision, class 1 occlusion was obtained, however, a corneal blink deficit was noted. Eight months after skeletal revision, blink had spontaneously improved. Angiography revealed collateralization providing retrograde flow from the flap to the recipient.
Conclusion
Although the necessity for revisions is clear, determining which revisions to safely perform and their timing and execution have not been explored. We address 4 distinct categories of revisions including: soft tissue revision, hard tissue mismatch, and craniofacial skeleton and dental occlusion. We illustrate the success of these revisions and assess their advantages, disadvantages, and relative risk.
Figure 1. (top left) The patient relapsed into class 3 malocclusion after transplant. (bottom left) Overlay of relapsed occlusion over the original digital 3D image of the post-transplant skeleton. (bottom middle) Digital plan to correct the malocclusion via midface advancement. (top/bottom right) 11-months following initial revisions (and 8-months following second revision) with a digital 3D skeletal image.