
Figures & data
Table 1. Patient and treatment characteristics.
Figure 1. Overall survival (OS) for patients divided by histopathology before (pre-ART) and after (ART) the implementation of adaptive radiotherapy. No significant improvement of 2-year OS for adenocarcinomas (AC) from 53.9% (95% CI [44.5%:65.4%]) to 58.9% (95% CI [51.3%:67.6%]) was observed (A). Meanwhile, 2-year OS for squamous cell carcinomas (SCC) increased significantly from 31% (95% CI [22.5%:42.6%]) to 54.5% (95% CI [45.6%:65.3%]) (B).
![Figure 1. Overall survival (OS) for patients divided by histopathology before (pre-ART) and after (ART) the implementation of adaptive radiotherapy. No significant improvement of 2-year OS for adenocarcinomas (AC) from 53.9% (95% CI [44.5%:65.4%]) to 58.9% (95% CI [51.3%:67.6%]) was observed (A). Meanwhile, 2-year OS for squamous cell carcinomas (SCC) increased significantly from 31% (95% CI [22.5%:42.6%]) to 54.5% (95% CI [45.6%:65.3%]) (B).](/cms/asset/0e793934-eac5-4e18-a2b1-517fc5941144/ionc_a_2260944_f0001_c.jpg)
Table 2. Multivariate Cox proportional hazards model for overall survival for each histology.
Figure 2. Kaplan–Meier curves showing incidences of radiation pneumonitis (RP) grade 3 or higher. Incidences declined significantly after implementing an adaptive strategy (ART) for both patients with adenocarcinoma (AC) (A) and squamous cell carcinoma (SCC) (B).
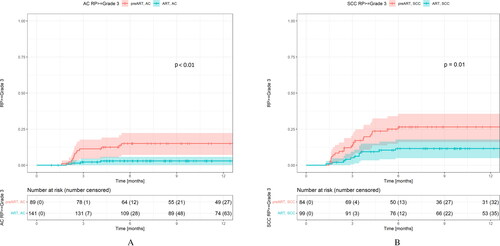
Figure 3. Loco-regional failure (LRF) for patients divided by histopathology (AC: adenocarcinoma; SCC: squamous cell carcinoma) before (pre-ART) and after (ART) the implementation of ART. Two-year freedom from LRF was 62.4% (95% CI: [51.0–76.3] for AC pre-ART and 52.9% (95% CI [43.6–64.2]) for AC after ART (A). For SCC, 2-year freedom for LRF was 32.8% (95% CI [22.6–47.7]) pre-ART and 42.3% (95% CI [33.1–54.2]) (B).
![Figure 3. Loco-regional failure (LRF) for patients divided by histopathology (AC: adenocarcinoma; SCC: squamous cell carcinoma) before (pre-ART) and after (ART) the implementation of ART. Two-year freedom from LRF was 62.4% (95% CI: [51.0–76.3] for AC pre-ART and 52.9% (95% CI [43.6–64.2]) for AC after ART (A). For SCC, 2-year freedom for LRF was 32.8% (95% CI [22.6–47.7]) pre-ART and 42.3% (95% CI [33.1–54.2]) (B).](/cms/asset/0455badf-1e31-4b71-b7ff-c177d58fd008/ionc_a_2260944_f0003_c.jpg)
Table 3. Multivariate Cox proportional hazards model for loco-regional failure for each histology.
Data availability statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.