Figures & data
Figure 1. Key events in the development of BCR::ABL1 TKIs. A timeline highlighting significant research breakthroughs that led to the development of TKIs for CML treatment.
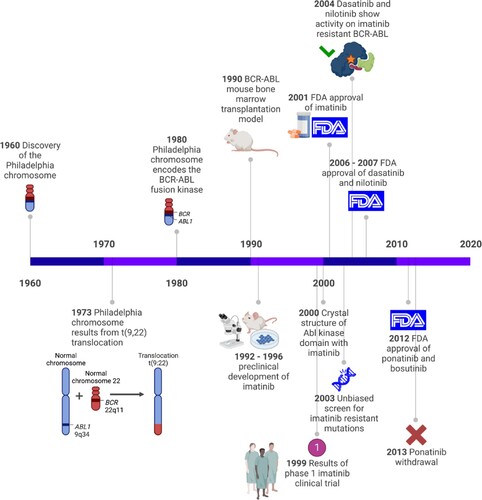
Figure 2. Mechanism of action of BCR::ABL1 tyrosine kinase and TKI in CML. BCR::ABL1 tyrosine kinase in CML (left). TKI in treatment of CML (right). P indicates phosphate. Figure was created with BioRender.com.
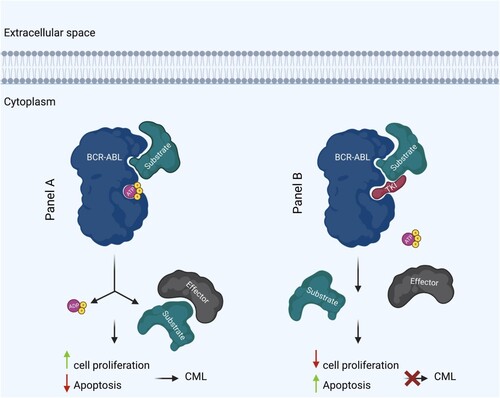
Figure 3. Mechanisms of TKI resistance in CML. BCR::ABL1 dependent mechanisms include (1) mutations that affect TKI binding. (2) overexpression or amplification of BCR::ABL1 leading to elevated kinase activity. BCR::ABL1 independent mechanisms include (3) increased expression of drug efflux pumps, including P-glycoprotein (Pgp), and reduced expression of drug influx pumps, including the organic cation transporter hOCT1. Other mechanisms that play a role BCR::ABL1 independent TKI resistance include (4) epigenetic alterations and (5) activation of alternative signaling pathways downstream of BCR::ABL1. Figure was created with BioRender.com.
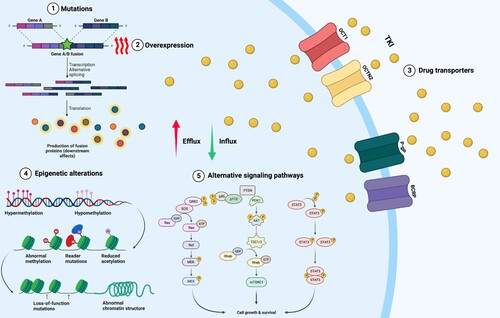
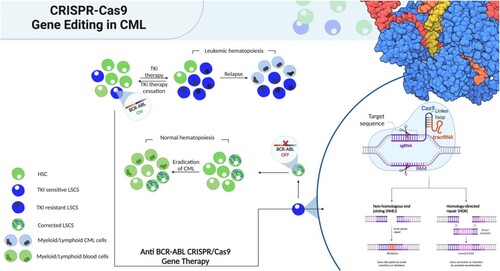
Figure 4. Gene therapy vs conventional therapy for CML. Conventional therapy based on tyrosine kinase inhibitors (TKI) effectively silences BCR::ABL1 in leukemic stem cells (LSCs). Because there are still cells that are BCR::ABL1 positive after treatment has ended, recurrence is possible. Recurrence of the disease may result from the emergence of TKI-resistant LSCs during therapy. However, the oncogene would be eradicated at the genome level via anti- BCR::ABL1 gene therapy. Corrected LSCs could replenish the bone marrow niche, enabling regular hematopoiesis. Figure was created with BioRender.com.