Figures & data
Figure 1. Equvalent dose in 2 Gy fractions (EQD2) for the lung (α/β = 4 Gy) versus isodose level for 30- and 15-fraction schedules and a prescription dose of 60 Gy with standard fractionation. The physical dose is adjusted to iso-effect in the hypofractionated case by ensuring that the equivalent dose to the target remains constant assuming α/β = 10 Gy. The overall effect of the decrease in physical dose and the increase in fraction size is a rise in EQD2 for isodose levels above 40%. In contrast, lung exposed to less than 40% of the prescription dose will experience a minor decrease in EQD2 with hypofractionation.
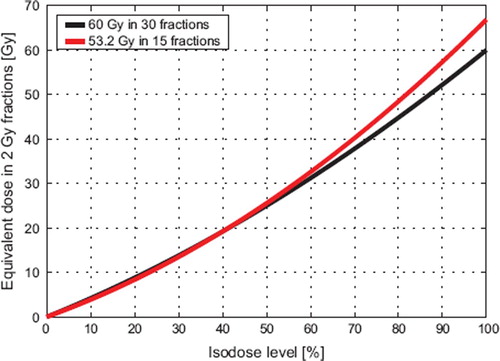
Figure 2. An illustrative case with a tomotherapy and a 3D-CRT plan and the corresponding dose volume histograms corrected for fractionation by using α/β = 4 Gy for the residual lung and α/β = 10 Gy for the tumor.
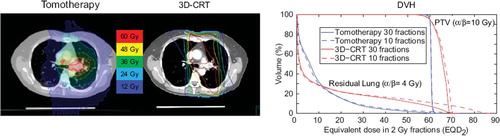
Figure 3. Mean risk of RP with the 3D-CRT and the tomotherapy plans for the 18 patients for different fractionation schedules. The solid lines represent the mean estimated risk of RP, while the dotted lines are the 68% confidence interval of the mean as estimated by bootstrap resampling. A more pronounced fractionation sensitivity is seen for 3D-CRT plans than for the tomotherapy plans.
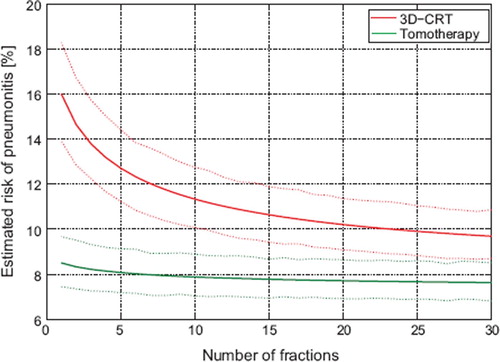
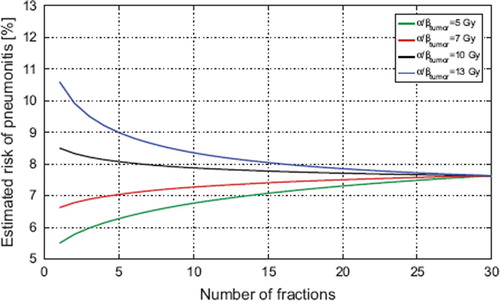
Figure 4. A sensitivity analysis of the dependence on the tumor fractionation sensitivity for the tomotherapy plans. The risk of RP increases as the tumor fractionation sensitivity decreases because the physical dose required for iso-effect increases with tumor α/β. As long as only moderate hypofractionation is applied, however, the change in RP is much less than the interpatient variation and the uncertainty in the model. For a 20-fraction schedule the difference in estimated risk of RP between α/β = 7 Gy and α/β = 13 Gy is less than 0.4%.