
ABSTRACT
With the better understanding of human genome and genetic contributions to human complex diseases, more and more clinical genetic tests have been developed for the prevention, diagnosis, and treatment of human diseases. This has raised new challenges to classroom teaching of medical genetics (MG) in medical education of undergraduates, who are relatively naive about the theory and technology of MG. A clear understanding of genotype-phenotype relationships is critical in MG learning. In the current study, we incorporated a practical approach of classroom MG teaching by using alcohol tolerance, a phenotype that is widely experienced by students and closely related to genetic polymorphism. To verify this teaching approach, which we named as student experience-based teaching (SEBT), undergraduates of two classes were recruited, with one accepting SEBT and the other accepting conventional lecture-based teaching (LBT). Final examination of the MG course indicated that while the two classes showed similar results to multiple-choice questions, the SEBT class showed significantly better performance to short-answer questions about gene polymorphism and phenotype, suggesting that SEBT might improve understanding. Thus, using student experience-based phenotypic instances and explaining the phenotype by practical genetic tests could improve understanding of genotype-phenotype relationships in classroom MG teaching.
Introduction
Medical education has had long-lasting challenges for both medical educators and undergraduates, especially in the age of knowledge explosion in life sciences. While more and more new knowledges are continuously added into medical textbooks, stronger abilities to use knowledges by students in their future clinical practice are expected. Numerous studies have been performed and many education models have been raised to meet these challenges. For instance, outcome-based education (OBE) emphasizes learner and programme outcomes, while competence-based medical education (CBME) focuses on the attainment of competence, but not learning based on units of time (Harris et al. Citation2010). On the learning side, problem-based learning (PBL) is a student-focused approach applied to solve a real-world problem (Neville and Norman Citation2007; Lawal, Ramlaul, and Murphy Citation2021). Lecture-based teaching (LBT) is conductive to passive learning on behalf of learners, and conversely, experiential learning is constructing knowledge and meaning from real-life experience which is widely used in medical education especially in clinical courses to develop students’ clinical skills (Yardley, Teunissen, and Dornan Citation2012). Many aspects of classroom activities are also improved. Team-based learning (TBL) provides students with opportunities to apply conceptual knowledge in learning (Burgess et al. Citation2020). More recently, the flipped classroom has been increasingly popular, because it uses classroom time for application of knowledge and critical thinking rather than for a passive didactic lecture (Hermsen et al. Citation2019). However, for undergraduates who have not experienced clinical practice, it might still be difficult to connect basic and advanced knowledges of life sciences to diseases and medicine.
With the discovery of more and more diseases- and therapy-related genetic loci in human genomes, clinical genetic tests are frequently employed in the prevention, diagnosis, and treatment of human complex diseases (Liu et al. Citation2014). Moreover, molecular targeted drugs are continuously developed for the treatment of cancer, and effective cancer therapy using these drugs heavily depends on genetic tests to determine the existence of specific targets (Hodgson, Eng, and Maher Citation2007). The widespread existence of polymorphism in pharmacokinetic- and pharmacodynamic-related genes, which results in remarkable variations in drug metabolism and efficacy, respectively, has prompted clinical genetic tests of these genes to instruct drug administration (Daly Citation2014). Future physicians will be directly involved in the clinical practice of genomic medicine – from ordering genetic tests to using the results to monitor medical processes. Consequently, systemic and practice-oriented knowledge of medical genetics (MG) is indispensable in the curriculum for medical students.
Indeed, MG has been adopted as one of the obligatory courses for medical students in most medical colleges (Duan et al. Citation2013). The MG course is usually provided in the second or third year as a part of the fundamental medical curriculum, following earlier courses such as Anatomy, Histology, Cell Biology, and Biochemistry and Molecular Biology. In general, MG curriculum consists of three parts, including fundamentals of genetics, genetic diseases, and application of genetic techniques (). To promote students’ learning, some universities have offered elective courses to help students understand genomic and personalised medicine. For example, Stanford University School of Medicine provides personal genome testing to students (Vernez et al. Citation2013; Salari et al. Citation2013), while University of Maryland School of Medicine gives summer elective course on the same topic (Perry et al. Citation2016). However, in most medical institutions, the major teaching model for MG is still lecture-based, which is dictated by the educator and explains genetic theory in detail but lacks practice, leaving students hardly perceiving genotype-phenotype relationships via a real-world experience (Plunkett-Rondeau, Hyland, and Dasgupta Citation2015).
Table 1. Current medical genetics curriculum in FMMU.
Alcohol exposure is quite popular in adults worldwide (Knox et al. Citation2019). A large adult population including college students have experienced or witnessed alcohol exposure under certain circumstances, and can evaluate alcohol tolerance simply by flush and associated behaviour changes. Alcohol metabolism in human involves mainly two enzymes, the alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH), which serially oxidise ethanol into acetaldehyde and non-toxic acetate, respectively (Knox et al. Citation2019). There are 7 ADH genes including ADH1A, ADH1B, ADH1C, ADH4, ADH5, ADH6, ADH7, and 4 ALDH genes including ALDH1-4 in human genome. Among these, ADH1B and ALDH2 play the most important roles in alcohol metabolism. Polymorphism in these two genes is responsible for variations in alcohol tolerance in populations (Agarwal Citation2001; Edenberg Citation2007). Human populations harbour many allelic variations in the ADH1B and ALDH2 loci. It has been shown that the rs1229984 allele of ADH1B (resulting in G143A mutation) and rs671 allele of ALDH2 (resulting in G1510A mutation) encode ADH and ALDH enzymes with reduced activities, which do not function optimally and that if a person inherits two of these alleles for either of the proteins, they will be less tolerant to alcohol. However, if they just inherit one of these alleles and then an allele that encodes a better functioning protein, they will be better able to tolerate alcohol (Peng and Yin Citation2009; Crabb et al. Citation1989).
Alcohol tolerance and the polymorphism of alcohol-metabolising enzymes may serve as an excellent example to explain the relationship between phenotype-genotype in classroom MG teaching. Because alcohol tolerance is a personal phenotype, it is possible to evaluate simultaneously this phenotype and genetic polymorphism of ADH and ALDH genes in a group of students in classroom by polymerase chain reaction (PCR)-sequencing. This might stimulate a discussion on the phenotype-genotype relationship, technologies used by clinical genetics in the class, and clinical genetics-related ethical concerns and skills, leading to improved learning. To achieve this goal, we designed our study using samples from student volunteers, who recorded their experience in drinking alcohol as phenotypes. We call this teaching approach as student experience-based teaching (SEBT). SEBT aims at helping students better understand genotype-phenotype relationships, and make students familiar with procedures and interpretation of clinical genetic tests. The attainments in knowledge and practical capacities will enhance students’ competence in their future clinical studies. In this study, we assess the following questions: would SEBT improve students’ performance in classroom teaching as compared with conventional LBT, and would SEBT lead to better understanding of genotype and phenotype relationships?
Materials and methods
Experimental design
Alcohol tolerance was selected as the instance for putative SEBT in our MG teaching because of its clear and popular phenotypes, and the well-known gene polymorphism determining the phenotypes. According to the SEBT procedure (), ten volunteers were randomly recruited at the beginning of the MG course, and a survey was conducted to evaluate their phenotypes of alcohol tolerance (). Meanwhile, saliva samples were collected from each volunteer for genotyping by PCR-sequencing, which could later be carried out in a laboratory or by commercial service provided by genetic test companies. The results of the genotyping and phenotype survey will then be presented in the pharmacogenetics unit of the MG course ().
Figure 1. Diagram of Student Experience-Based Teaching (SEBT). (A) A framework of MG curriculum, which includes 3 teaching parts. SEBT was initiated at Part I and a classroom discussion using SEBT data was carried out at pharmacogenetics unit of Part III. (B, C) Contents of SEBT. The classroom part (B) includes the announcement of SEBT, ethics education, recruitment of volunteers and their phenotype survey, as well as classroom discussion of phenotype and genotype data and related ethics questions. The laboratory part (C) includes sampling, DNA extraction, and PCR-seq experiments of SEBT, which were performed by teaching staff members. The LBT class followed the whole process of this curriculum shown in (A). The SEBT class also accepted the curriculum but were involved in SEBT shown in (B and C). In the pharmacogenetic unit, the SEBT class was given lectures on genetic polymorphism of ADH/ALDH and alcohol tolerance, and discussed genotype and phenotype data from their own samples.
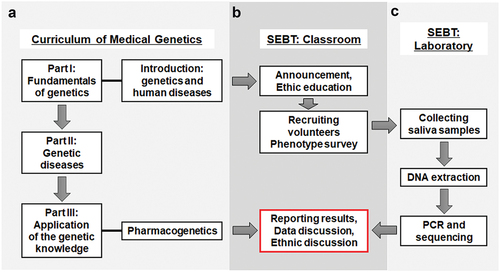
Table 2. Questionnaire about alcohol tolerance.
Subjects
There are altogether 379 students in the MG course, and they are randomly assigned by the university administrator in the second academic year into two classes. Two classes were recruited in this study: SEBT class (N = 175) and LBT class (N = 204). The curriculum of MG is shown in . Lectures of MG were given to students in classrooms twice a week, with two class-hours as one unit. In students’ previous courses of Biochemistry and Molecular Biology, the average scores in SEBT class and LBT class were 80.18 and 79.27, respectively. A T-test showed that there was no significant difference (t = 0.813, p = 0.208), suggesting no significant difference in learning performance between the two classes.
An announcement was made to all students in SEBT class about the number of volunteers recruited, the purpose of the gene testing of ADH1B and ALDH2 genes, related methods of sampling and testing, and how the results would be used. Ten volunteers out of 98 applicants from SEBT class were then randomly recruited, and informed consent forms were signed. All students were educated that genetic information is a kind of personal privacy, and the results of the test would be anonymous. The use of human samples was approved by the Medical Ethics Committee of the Fourth Military Medical University.
Survey on alcohol tolerance phenotypes in volunteers
To evaluate the phenotype of alcohol tolerance in volunteers, a single-choice survey was designed, focusing on the alcohol exposure of the individual such as the frequency of drinking liquor, appearance, and behaviour changes after drinking liquor (). To facilitate discussion, alcohol experience of volunteers was artificially classified as strong tolerance (late flush and short duration), weak tolerance (early flush and long duration), and intermediate tolerance (between strong and weak).
Gene polymorphism analysis by PCR-sequencing
Genomic DNA was prepared from saliva (about 0.5 mL) using the Mag-Bind Blood & Tissue DNA HDQ 96 Kit (Omega Bio-tek, Inc., 400 Pinnacle Way, GA) according to the supplier’s protocol. In brief, saliva samples (250 µL) were digested in a proteinase K solution at room temperature for 10 min with shaking. HDQ Binding Buffer (400 μL) and Mag-Bind® Particles HDQ (20 μL) were then added to each sample, and mixed by vortex for 10 min. DNA was then recovered by magnetic separation, and subjected to PCR to amplify the ADH1B and ALDH2 gene fragments encompassing the polymorphisms regions (sequences of ADH1B and ALDH2 refer to Genbank with accession numbers NM_000668.6 and NM_000690.4, respectively). The amplified fragments were sequenced to determine the genotypes of each locus. PCR primers are as below (underlined are primers for sequencing): ADH1B, 5′-TGTAAAACGACGGCCAGTAGGGCTTTAGACTGAATAACCTTGGGG, and 5′-CAGGAAACAGCTATGACCCCCCTTCTCCAACACTCTCCACGAT; ALDH2, 5′-TGTAAAACGACGGCCAGTATGTGTTTGGAGCCCAGTCACCCTT, and 5′-CAGGAAACAGCTATGACCCGCCCAGCAGACCCTAAATCCCT.
Final examination
Two questions were designed to evaluate effects of the SEBT in the final examination (). One was a multiple-choice question asking students to choose the key metabolic enzyme during alcohol metabolism from alcohol dehydrogenase (ADH), superoxide dismutase (SOD), aldehyde dehydrogenase (ALDH) and aspartate aminotransferase (AST). The other was a short-answer question: ‘Why are there differences in sensitivity of different individuals to alcohol?’ aimed at the understanding of why chemicals affect people variously. Then, exams were scored by faculties in a double-blinded manner. Correct answers should say that alcohol tolerance is influenced by three critical biological mechanisms, gene polymorphisms at ADH/ALDH loci, protein mutations resulted from gene mutation, and accumulation of acetaldehyde. Points were given according to the number of correct answers.
Table 3. Questions in the final examination.
Statistical analysis
Statistical analysis was performed with the GraphPad Prism 6 software. Levene’s Test showed that the requirement of homogeneity was met (p = 0.911). Normality was ensured by the K-S test, with results showing that the requirements for T-tests were met. The continuous variables were expressed as mean ± SD and compared using T-tests. The categorical variables were expressed by numbers and percentages. The chi-square test was used to test the differences for categorical variables between groups. P < 0.05 was considered statistically significant.
Results
Correlation of phenotype of alcohol tolerance and gene polymorphisms in student volunteers
To improve understanding of the complex relationship between genotype and phenotype in MG teaching, we set out to find out a phenotype that could be appreciated by students via daily experience and could be easily explained by genotypes after genetic testing. Alcohol exposure results in various personal feelings and behaviour changes in a population. Weakly tolerant individuals show flushing earlier and for longer duration, accompanied by dizziness and excitement or depression after intake of a small amount of liquor, while strongly tolerant people do not exhibit this phenotype even after intaking a larger amount of alcohol (Edenberg Citation2007; Ehlers, Liang, and Gizer Citation2012). The phenotype is a result of acetaldehyde accumulation in blood, and the difference in alcohol tolerance is roughly determined by variations in the two enzymes responsible for alcohol metabolism, ADH and ALDH.
In this study, the genotype was determined by genetic tests on ADH1B and ALDH2 genes. As the first step, students in SEBT class were given an announcement about SEBT at the beginning of the MG course, together with a brief introduction of ethics rules about genetic testing. Then, a survey on alcohol tolerance phenotypes in randomly recruited volunteers was conducted () and saliva samples were collected for further genetic testing. The phenotype and genotype data are anonymous in the following classroom content, although the genetic testing results are presented to the volunteers him- or herself. The results of genotyping and phenotype survey are summarised in . The genotyping data showed that different genotypes of ADH1B and ALDH2 loci were identified in the volunteers of SEBT. These data were presented to the whole class, and discussed as examples of genotype-phenotype relationship in the pharmacogenetics course, in which drug metabolism constitutes an important content ().
Table 4. Genotype and phenotype of volunteers.
The classroom activities of SEBT
The pharmacogenetics unit of the MG course uses two class-hours (totally 80 minutes). The ordinary classroom activity in the pharmacogenetics unit is basically a lecture with contents including an introduction of pharmacogenetics and its clinical application, drug metabolism (pharmacokinetics) and effects (pharmacodynamics), polymorphism of pharmacokinetics/pharmacodynamics-related genes/enzymes and drug administration, genetic tests in helping precision drug administration. Examples are given in each part of the lecture contents, and alcohol metabolism is used as an example to explain the effects of genetic polymorphism on pharmacokinetics variations. In the LBT class, the teacher explained the molecular mechanism of alcohol metabolic and relevant genetic polymorphisms using PPT, and encouraged classroom interactions by raising questions such as ‘why do people become flushed after drinking alcohol?’ and ‘Why is there a difference in response among people?’, followed by short student discussion individually or in groups. In the SEBT class, the lecture contents were kept but the teacher explained the molecular mechanism of alcohol metabolism and relevant genetic polymorphisms using PPT showing the genotypes and reported phenotypes collected from the volunteers (retaining anonymity). The teacher presented the data in a manner of interacting with students, and discussed the following areas.
Firstly, techniques used in SEBT, including sampling, DNA extraction, PCR and sequencing, were explained in the class. The results of sequencing were also presented in the class to show the single nucleotide polymorphism (SNP) of the ADH1B and ALDH2 loci (). The results showed that at the polymorphic ADH1B locus (rs1229984), #5, #6, #7, and #10 were homozygous for CGC (GG, high metabolism), #2, #4, and #9 were homozygous for CAC (AA, low metabolism), while #1, #3, and #8 were heterozygous (GA, intermediate). The percentage of GG, GA, or AA genotype was 40%, 30%, and 30%, respectively. At the ALDH2 locus (rs671), #1, #3, #4, #7, #8, and #10 were homozygous for GAA (GG, high metabolism), and #2, #5, #6, and #9 were heterozygous for GAA and AAA (GA, intermediate), no homozygous for AAA (AA, low metabolism). The percentage of GG, GA, or AA genotype was 60%, 40%, and 0%, respectively.
Figure 2. Performance of students from the LBT class and the SEBT class. (A) Illustration of genetic polymorphism in human ADH1B and ALDH2 genes. Thin lines, open boxes, and filled boxes indicate introns, untranslated regions, and coding regions, respectively. The two polymorphic sites are indicated. (B) Students were given multiple-choice and short-answer questions. Percentages of students with correct answers and incorrect answers are plotted.
The central question discussed in the class was the genotype-phenotype relationship. Alcohol tolerance is expected to be dependent on acetaldehyde concentration in blood. If considering ALDH2 only, #1/3/4/7/8/10 were GG genotype and high metabolic for acetaldehyde, and should be more tolerant than #2/5/6/9. However, acetaldehyde concentration is also influenced by its source, the ADH activity, which was expected to be #5/6/7/10 > #1/3/8 > #2/4/9. Therefore, when both loci were taken into consideration, the #5/6 would be most intolerant, and the #7/10 should be the most tolerant. The #2/9’s bad feeling might have persisted longer because they could not metabolise both alcohol and acetaldehyde in a short period of time. Other individuals in this group would have intermediate tolerance to alcohol. These deduced phenotypes were compared with the reported phenotypes, and the consistency and inconsistency were discussed in the class.
One more question discussed in the class was the relationship between alcohol tolerance and health. For example, GG genotype of ADH1B likely leads to stronger tolerance, but people with this genotype are more susceptible to alcohol-related diseases, such as certain types of cancers including oesophagus cancer and colorectal cancer (Druesne-Pecollo et al. Citation2009; Edenberg and McClintick Citation2018). This also suggests that phenotype is not simply a result of genotype, but it is also heavily influenced by environmental elements.
Ethics concerns were also mentioned with the genetic testing in SEBT class as an example. Detailed ethics principles and rules will be presented later in the MG course.
Comparison of the examination performance between the two classes
To evaluate whether SEBT could improve the learning of MG with respect to the genotype-phenotype relationship, we included two test questions in the final examination of MG. The multiple-choice question was aimed at evaluating memory of the knowledge, while the short-answer question was used to assess understanding of the knowledge. The key answer points about the short-answer question were to illustrate the causal relation between genotypes and phenotypes. Specifically, gene polymorphism causes differences in coding amino acids, differences in coding amino acids causes differences in protein structure and thus results in the difference of metabolic enzyme activity. The accumulation of acetaldehyde, an intermediate of alcohol metabolism, results in the difference of phenotype. Marks were given based on the pointed listed above. As shown in , there was no significant difference between the two classes in correctly answering the multiple-choice question, which means there was no significant difference in knowledge memory. The students in the SEBT class, however, provided more detailed information to the short-answer question. As a result, they got more points compared to the LBT class. The analysis indicated that significantly more students received a full mark in the SEBT class compared to the LBT class (73.1% and 62.7%, respectively, P < 0.05). In a nut shell, these results suggested that SEBT could improve the students’ comprehensive understanding of the knowledge.
Discussion
In the era of personalised and precision medicine, knowledge of MG is increasingly important for the prevention, diagnosis, and treatment of complex diseases. Medical students usually possess limited background in medicine in their early undergraduate stages, although they may have learned general genetics in high school. This situation has raised challenges to both teachers and students in MG classroom. To help students better understand genomics and personalised medicine, some universities have offered some elective courses. However, in many medical institutions, the conventional teaching model for MG is still lecture-based without a practical course. For example, pharmacogenetics is complex and abstract for both teaching and learning. Although clinical cases are often introduced into conventional lectures to explain drug metabolic enzymes and drug targets, these cases are not experienced by undergraduates and therefore difficult to understand.
Experiential education is a teaching philosophy that, by using many disciplines and settings, educators purposefully engage with learners in direct experience and focused reflection in order to increase knowledge, develop skills, clarify values, and develop people’s capacity to contribute to their communities (Yardley, Teunissen, and Dornan Citation2012). To overcome the difficulties in MG teaching, in this study, we have tried to select practical and perceivable teaching instances. We suppose that this SEBT might have several advantages. First, the teaching instances are more attractive to students because they come from their real life, leading to better understanding of the knowledge of genotype-phenotype relationship and personalised medicine, and effectively enhancing the initiative and enthusiasm of study. This indeed stimulated more discussion about how genotypes influenced the phenotypes as we observed during the class. It has also been observed that students in the SEBT class were more motivated. Students in the SEBT class with an instance of alcohol tolerance exhibit better performance in the final examination of MG course. This suggested that selection of better learning instances could reliably improve learning.
Second, this teaching approach may promote students’ understanding of the technology of clinical genetic tests. SEBT in MG teaching involves the usage of advanced clinical genetic technology, such as PCR, sequencing, genotyping and so on. These techniques are already popular in clinical practice. Thus, SEBT will also be very helpful for students to get acquaintance with these techniques, which they will use frequently in their future clinical practice (Witt and Jankowska Citation2018).
And third, medical ethics is getting more and more important in medical education in the genome era. It is important to follow the medical ethics rules before and during genetic tests. It is also important to learn skills to explain the result of genetic tests to subjects accepting the test, and provide genetic counseling. In this study, signing of consent forms by every volunteer is required. Moreover, this teaching model can provide a platform of practicing genetic counseling, another learning content of MG.
A better understanding of the relationship between genotype and phenotype would be more helpful for doctors to devote into future personalised medicine. On this point of view, the SEBT model of MG teaching would let medical students have a chance of being on the side of patients to experience how their phenotypes are determined by genetic constitution. However, it should be noticed that genotype is not the only determinant of phenotype. Many human phenotypes, especially those involving cognition and behaviour, such as alcohol tolerance, are influenced by environmental elements at different levels and extents. Overemphasising the dependence of phenotype on genotype in teaching may lead to essentialism that, by focusing on differences, artificially simplifies individual and group identities and interactions (Dar-Nimrod and Heine Citation2011; Heine, Cheung, and Schmalor Citation2019). This problem could be more obvious for MG education, which deals with human nature and its inheritance (Fuller Citation2002; Braun and Saunders Citation2017). Incorrect teaching activity in MG may result in deleterious ethnic consequences. It should be the teacher’s duty to correctly organise and perform a discussion of the results of SEBT with students in class and in the later course of medical ethnics. More studies are needed to eradicate genetic essentialism in MG teaching under different education methodologies including SEBT.
The essence of initiating this SEBT is to engage students in a more elaborative learning experience partly by involving students in the alcohol gene test and partly by providing them with a more real-life instance, which could also be used in team-based learning or flipped classroom (Burgess et al. Citation2020; Hermsen et al. Citation2019). This elaborative learning experience would motivate students, thus resulting in more active class performance and better recall of the content discussed in the class, which was then confirmed by the results of the final examination.
In summary, the SEBT in this study could facilitate the learning of complex and abstract content in medical education by using student-derived real-life instances. The approach is relatively less funding- and time-consuming, and could be practiced more easily. It could also be extended to other medical courses such as Biochemistry and Molecular Biology. Finally, SEBT comprehensively provides students with chances to learn knowledge deeply, become familiar with the genetic test procedure, analyse the results, and practice genetic counseling, which will likely increase students’ competence in their future clinical studies.
Conflicts of interest
No potential conflict of interest was reported by the authors.
Acknowledgments
This work was supported by Project on Teaching Reform of High Education from the Shaanxi Provincial Government (2015-222) and Teaching-Improving Project from FMMU (BL201604).
Additional information
Funding
References
- Agarwal, D. P. 2001. “Genetic Polymorphisms of Alcohol Metabolizing Enzymes.” Pathologie Biologie 49 (9): 703–709. doi:10.1016/S0369-8114(01)00242-5.
- Braun, L., and B. Saunders. 2017. “Avoiding Racial Essentialism in Medical Science Curricula.” AMA J Ethics 19: 518–527. doi:10.1001/journalofethics.2017.19.6.peer1-1706
- Burgess, A., C. Van Diggele, C. Roberts, and C. Mellis. 2020. “Team-based Learning: Design, Facilitation and Participation.” BMC Medical Education 20 (Suppl 2): 461. doi:10.1186/s12909-020-02287-y.
- Crabb, D. W., H. J. Edenberg, W. F. Bosron, and T. K. Li. 1989. “Genotypes for Aldehyde Dehydrogenase Deficiency and Alcohol Sensitivity. The Inactive ALDH2(2) Allele Is Dominant.” Journal of Clinical Investigation 83 (1): 314–316. doi:10.1172/JCI113875.
- Daly, A. K. 2014. “Is There a Need to Teach Pharmacogenetics?” Clinical Pharmacology & Therapeutics 95 (3): 245–247. doi:10.1038/clpt.2013.184.
- Dar-Nimrod, I., and S. J. Heine. 2011. “Genetic Essentialism: On the Deceptive Determinism of DNA.” Psychological Bulletin 137 (5): 800–818. doi:10.1037/a0021860.
- Druesne-Pecollo, N., B. Tehard, Y. Mallet, M. Gerber, T. Norat, S. Hercberg, and P. Latino-Martel. 2009. “Alcohol and Genetic Polymorphisms: Effect on Risk of Alcohol-related Cancer.” The Lancet Oncology 10 (2): 173–180. doi:10.1016/S1470-2045(09)70019-1.
- Duan, X., T. Markello, D. Adams, C. Toro, C. Tifft, W. A. Gahl, and C. F. Boerkoel. 2013. “Cultural Differences Define Diagnosis and Genomic Medicine Practice: Implications for Undiagnosed Diseases Program in China.” Frontiers of Medicine 7: 389–394 doi: 10.1007/s11684-013-0281-3.
- Edenberg, H. J. 2007. “The Genetics of Alcohol Metabolism: Role of Alcohol Dehydrogenase and Aldehyde Dehydrogenase Variants.” Alcohol Research & Health : The Journal of the National Institute on Alcohol Abuse and Alcoholism 30 (1): 5–13.
- Edenberg, H. J., and J. N. McClintick. 2018. “Alcohol Dehydrogenases, Aldehyde Dehydrogenases, and Alcohol Use Disorders: A Critical Review.” Alcoholism, Clinical and Experimental Research 42 (12): 2281–2297. doi:10.1111/acer.13904.
- Ehlers, C. L., T. Liang, and I. R. Gizer. 2012. “ADH and ALDH Polymorphisms and Alcohol Dependence in Mexican and Native Americans.” The American Journal of Drug and Alcohol Abuse 38 (5): 389–394. doi:10.3109/00952990.2012.694526.
- Fuller, K. 2002. “Eradicating Essentialism from Cultural Competency Education.” Academic Medicine 77 (3): 198–201. doi:10.1097/00001888-200203000-00004.
- Harris, P., L. Snell, M. Talbot, and R. M. Harden. 2010. “Competency-based Medical Education: Implications for Undergraduate Programs.” Medical Teacher 32 (8): 646–650. doi:10.3109/0142159X.2010.500703.
- Heine, S. J., B. Y. Cheung, and A. Schmalor. 2019. “Making Sense of Genetics: The Problem of Essentialism.” Hastings Center Report 49 (Suppl 1): S19–S26. doi:10.1002/hast.1013.
- Hermsen, J. L., N. A. Mokadam, E. D. Verrier. 2019. “Flipping the Classroom: How to Optimize Learning in the Didactic Setting.” Thoracic Surgery Clinics 29 (3): 279–284. doi:10.1016/j.thorsurg.2019.04.002.
- Hodgson, S. V., V. Eng, and E. R. Maher. 2007. A Practical Guide to Human Cancer Genetics, 3rd Edn. Cambridge University Press.
- Knox, J., J. Schneider, E. Greene, J. Nicholson, D. Hasin, T. Sandfort. 2019. “Using Social Network Analysis to Examine Alcohol Use among Adults: A Systematic Review.” PLoS One 14 (8): e0221360. doi:10.1371/journal.pone.0221360.
- Lawal, O., A. Ramlaul, and F. Murphy. 2021. “Problem based learning in radiography education: A narrative review.”Radiography (Lond)“ 27(2):727–732. doi: 10.1016/j.radi.2020.11.001
- Liu, R., X. Wang, K. Aihara, and L. Chen. 2014. “Early Diagnosis of Complex Diseases by Molecular Biomarkers, Network Biomarkers, and Dynamical Network Biomarkers.” Medicinal Research Reviews 34 (3): 455–478. doi:10.1002/med.21293.
- Neville, A. J., and G. R. Norman. 2007. “PBL in the Undergraduate MD Program at McMaster University: Three Iterations in Three Decades.” Academic Medicine 82 (4): 370–374. doi:10.1097/ACM.0b013e318033385d.
- Peng, G.-S., and S.-J. Yin. 2009. “Effect of the Allelic Variants of Aldehyde Dehydrogenase ALDH2*2 and Alcohol Dehydrogenase ADH1B*2 on Blood Acetaldehyde Concentrations.” Human Genomics 3 (2): 121–127. doi:10.1186/1479-7364-3-2-121.
- Perry, C. G., K. A. Maloney, A. L. Beitelshees, L. Jeng, J. N. P. Ambulos, A. R. Shuldiner, and M. G. Blitze. 2016. “Educational Innovations in Clinical Pharmacogenomics.” Clinical Pharmacology and Therapeutics 99: 582–584.
- Plunkett-Rondeau, J., K. Hyland, and S. Dasgupta. 2015. “Training Future Physicians in the Era of Genomic Medicine: Trends in Undergraduate Medical Genetics Education.” Genetics in Medicine 17 (11): 927–934. doi:10.1038/gim.2014.208.
- Salari, K., K. J. Karczewski, L. Hudgins, K. E. Ormond. 2013. “Evidence that Personal Genome Testing Enhances Student Learning in a Course on Genomics and Personalized Medicine.” PLoS One 8 (7): e68853. doi:10.1371/journal.pone.0068853.
- Vernez, S. L., K. Salari, K. E. Ormond, and S. S. Lee. 2013. “Personal Genome Testing in Medical Education: Student Experiences with Genotyping in the Classroom.” Genome Medicine 5 (3): 24. doi:10.1186/gm428.
- Witt, M. M., and K. A. Jankowska. 2018. “Breaking Bad News in Genetic Counseling-problems and Communication Tools.” Journal of Applied Genetics 59 (4): 449–452. doi:10.1007/s13353-018-0469-y.
- Yardley, S., P. W. Teunissen, and T. Dornan. 2012. “Experiential Learning: Transforming Theory into Practice.” Medical Teacher 34 (2): 161–164. doi:10.3109/0142159X.2012.643264.