
Abstract
Antiphospholipid syndrome (APS) is an autoimmune disease mainly characterised by vascular thrombosis and pregnancy morbidity. APS has broad spectrum of clinical manifestations. The digestive system involvement of antiphospholipid syndrome is a critical but under-recognised condition. Digestive system involvement may be the result of direct (autoimmune-mediated) or indirect (thrombotic) mechanisms. Liver is the most commonly involved organ, followed by intestines, oesophagus, stomach, pancreas and spleen. This review describes possible digestive system manifestations in APS patients, and illustrates the epidemiology and possible pathophysiology of APS. The role of different treatment strategies in the management of digestive system manifestations of APS were also discussed.
Antiphospholipid syndrome is a multi-organ, multi-system disease and its clinical manifestation spectrum is gradually expanding. Since the first diagnosis of APS, the clinical manifestations of digestive system have been reported successively. This narrative review describes the major digestive system manifestations of APS and illustrates the epidemiology, pathophysiology and the role of therapeutic strategies of these patients.
Key messages
1. Introduction
Antiphospholipid syndrome (APS) is an autoimmune disease, characterised by presence of antiphospholipid antibodies (aPL) in the bloodstream that leave the patient in a potentially hypercoagulable state, leading to thrombosis at all segments of the vascular bed. It is also associated with pregnancy morbidity (miscarriages, late intrauterine fetal demise, and severe pre-eclampsia especially placental insufficiency) [Citation1]. The clinically significant laboratory tests for aPL include lupus anticoagulants (LA), anti-β2-glycoprotein I antibodies (anti-β2GPI) and anticardiolipin antibodies (ACL) [Citation2].
The diagnosis of APS utilizes the Sapporo criteria, including the presence of at least one clinical event and one durably positive laboratory criteria (over at least 12 weeks). Clinical criteria included [Citation1]: vascular thrombosis events (venous and/or arterial) [Citation2]; and/or pregnancy morbidity along with persistent presence of aPL. While laboratory criteria included [Citation1]: persistently medium/high titer anticardiolipin antibodies (including isotypes IgG and/or IgM) [Citation2]; or medium/high titer anti-β2-glycoprotein I (β2-GPI) antibodies (including isotypes IgG and/or IgM) [Citation3]; or a positive lupus anticoagulant test) with two positive tests, spaced at least 12 weeks apart [Citation3,Citation4].
Based on etiology of other autoimmune diseases, APS is classified as primary and secondary APS. APS with no underlying cause identified is called primary APS (PAPS); while APS with an associated comorbidity, such as systemic autoimmune diseases, or malignancy, or secondary to certain medications, are called secondary APS (SAPS) [Citation4].
APS can affect any organ or system with diverse clinical manifestations. Since the first diagnosis of APS, the clinical manifestations of digestive system have been reported successively [Citation5,Citation6]. The hepatic involvement is reported as the most common manifestation of the digestive system in APS, followed by gastrointestinal tract [Citation7]. Though these clinical features are associated with presence of aPL, they are not necessarily related to thrombosis. Several other mechanisms such as inflammation, complement pathway, and platelet activation have been postulated [Citation4,Citation8,Citation9]. APS-related digestive symptoms are often overlooked by clinicians, and some doctors are even confused during the diagnosis and treatment. This narrative review describes the major digestive system manifestations of APS and illustrates the epidemiology, pathophysiology of these patients. The role of therapeutic strategies is also discussed.
We undertook a computer-assisted search of the literatures in MEDLINE, The National Library of Medicine until 2020, using the search items: antiphospholipid syndrome, anticardiolipin antibodies, lupus anticoagulant, antiphospholipid antibodies, catastrophic antiphospholipid syndrome, liver, hepato-biliary, pancreas, spleen, gastrointestine, and abdomen. The relevant articles were grouped according to the involved organs and further classified by different disease entities in each group.
2. Epidemiology
The prevalence of aPL in the general population ranges between 1% and 5% [Citation2,Citation10]. The positive antibodies may present in the following cases: (1) asymptomatic carriers, (2) patients with non-thrombotic conditions (such as thrombocytopenia, autoimmune hemolytic anemia, livedo reticularis, etc.), (3) patients with thrombosis and (4) health women during pregnancy. However, in general population, the epidemiology of APS is not well established. According to recent estimations, approximately 1–2 APS patients occurred per 100,000 persons per year, and APS may be more common than previously appreciated with a prevalence approximately ranges from 17 to 50 patients per 100,000 persons [Citation11,Citation12].
In the “Europhospholipid” cohort of the 1,000 APS patients, the incidence of gastrointestinal, splenic, pancreatic and hepatic manifestations were 1.5%, 1.1%, 0.5% and 0.7% respectively [Citation6]. The APS associated gastrointestinal symptoms are rarely reported. The true incidence of APS-related digestive system manifestations might be largely underestimated. The main reason is that the APS related digestive system manifestations are diverse, complex, non-specific and often involves multiple organs, making the diagnosis difficult.
3. Pathophysiology
The pathophysiology of APS mainly includes two aspects: thrombotic mechanism and immune mechanism ().
Table 1. Pathophysiological mechanisms mediated by aPL.
Antiphospholipid antibodies plays an important role in thrombotic events in patients with APS. Studies have shown that aPL induces thrombosis mainly against β2-glycoprotein I. The other targeted antigens include prothrombin, protein C, protein S, annexin A5, annexin A2, etc [Citation13]. Anti-β2 GP I binds to the β2 GP I receptor on endothelial cells to induce dimerization. The subsequent interaction between the dimerized β2 GP I and apolipoprotein E receptor 2 mediated the APL induced endothelial nitric oxide synthase (eNOS) inhibition, increases expression of endothelial adhesion molecules, and increases production of endothelin-1 and tissue factors, leading to thrombosis [Citation14,Citation15]. The anti-β2 GP I also binds to the β2 GP I receptor on platelets, leading to overexpression of thrombin, enhanced platelet adhesion to endothelial collagen, increased platelet aggregation, and induced thrombotic events [Citation14,Citation15]. Through the above target antigen, aPL can also activate mononuclear cells, inducing tissue factor, protease activated receptor and proinflammatory cytokines [Citation13]. Neutrophil extracellular traps (NETs) is a key inducer in the process of blood coagulation and endovascular thrombosis. Studies have shown that aPL can further activate neutrophils to release NETs, leading to thrombosis [Citation16]. In addition, the thrombogenic effects of aPL also involve activation of the classical pathway of the complement system [Citation17]. In addition to accelerating the thrombosis, aPL can inhibit fibrinolysis through a variety of mechanisms. Studies have also shown that aPL can inhibit fibrinolysis by inhibiting the binding of plasminogen activators and plasminogen to annexin A2 endothelial surface receptors and activating plasminogen activator inhibitor 1 overexpression [Citation18]. A summary of pathophysiology has been demonstrated in .
Figure 1. Thrombotic mechanisms mediated by aPL. Thrombus formation can be promoted in the different ways [Citation1]: aPL interacts with endothelial cells [Citation2]; aPL activates mononuclear cells, induces expression of tissue factors, proteinase activated receptors and proinflammatory cytokines [Citation3]; aPL interacts with platelets [Citation4]; aPL inhibit fibrinolysis.aPL:antiphospholipid antibodies; β2-GPI:β2-glycoprotein I.
![Figure 1. Thrombotic mechanisms mediated by aPL. Thrombus formation can be promoted in the different ways [Citation1]: aPL interacts with endothelial cells [Citation2]; aPL activates mononuclear cells, induces expression of tissue factors, proteinase activated receptors and proinflammatory cytokines [Citation3]; aPL interacts with platelets [Citation4]; aPL inhibit fibrinolysis.aPL:antiphospholipid antibodies; β2-GPI:β2-glycoprotein I.](/cms/asset/4c06b056-df1b-4749-90b8-6ccc5b058e63/iann_a_1962964_f0001_c.jpg)
Since APS is an autoimmune disease, autoimmune responses through inflammatory mechanisms may also play a role in its pathogenesis. Pathology confirmed evidence of sub endocardial immunoglobulin deposition in the heart valves in APS patients with valvular heart diseases, suggesting that aPL may be involved in the sub endocardial inflammatory process through interaction with valve surface antigens [Citation19]. Similar immune mechanism mediated by aPL occurs in digestive system. LA, as a member of aPL, causes autoimmune esophagitis, resulting in reduced intestinal wall strength and an increased risk of spontaneous esophageal rupture [Citation9]. aPL is also involved in cross-immune responses. There are a large number of mitochondria in the liver, which contain cardiolipin. ACL may cross-react with mitochondria present in the liver [Citation20]. In addition, in some patients with primary sclerosing cholangitis, S. Cerevisiae, as an environmental factor, may cross-react with aPL [Citation21]. The significantly increased rate of positive aPL occur in inflammatory bowel disease, nodular regenerative hyperplasia, pancreatitis and other diseases. It is speculated that the direct effect of aPL may influence the occurrence and development of diseases [Citation22–24].
4. Clinical presentations
Digestive system involvement in APS comprises a wide spectrum of clinical manifestations that include esophageal disease (esophageal necrosis and rupture), gastric disease(gastric ulcer and gangrene), intestinal disease(intestinal infarction and Inflammatory bowel disease), liver disease(thrombotic liver diseases, obstruction of small hepatic veins, hepatic infarction, non-thrombotic liver diseases), splenic disease(splenic infarction, auto splenectomy or functional asplenia) and pancreatic disease(pancreatitis, pancreatic duct injury) [Citation5,Citation7,Citation10]. summarizes the major digestive system manifestations associated with APS.
Table 2. Summary of digestive system manifestations associated with APS.
4.1. Esophageal manifestations
The esophageal diseases associated with APS are esophageal necrosis and rupture. The earliest case, reported by Cappell MS, can date back to 1994 [Citation25], later, related cases of esophageal involvement were also reported by Naitoh H [Citation26] and Padda A [Citation27].
4.2. Gastric manifestations
Two case reports have mentioned APS related gastric lesions, clinical manifestations were giant gastric ulcer [Citation28] and massive gastric gangrene [Citation29]. The main reason for gastric ischemic necrosis as rare manifestation is that the vessel diameter that supply stomach is relatively large and has well collateral circulations [Citation30]. Therefore, extensive occlusion of all major vessels or the coeliac trunk is required to cause gastric ischemia. It is important to note that APS thrombosis tends not to be limited to the large vessels, but also to any small blood vessels (arterioles/venules) supplying the organs [Citation31].
4.3. Intestinal manifestations
A number of APS patients have been reported with intestinal infarction from mesenteric thrombosis [Citation32–35]. Intestinal venous or arterial thrombosis and infarction appear to be prominent features of APS associated small intestinal involvement. However, it should be noted that mesenteric venous thrombosis is the least common cause of mesenteric ischemia [Citation36]. Mesenteric artery thrombosis accounts for 25% to 30% of all ischemic events. Almost all cases of mesenteric ischemia due to arterial thrombosis occur in the context of severe atherosclerotic disease [Citation37].
Inflammatory bowel disease (IBD) includes ulcerative colitis (UC) and Crohn's disease (CD). Since the first reported association between IBD and APS in 1992 [Citation38], few related cases have also been reported [Citation39–42].
4.4. Hepatic manifestations
Hepatic involvement is the most common digestive system manifestation of APS.A wide range of hepatic diseases have been reported in association with APS, that vary from thrombotic diseases (Budd-Chiari syndrome) to non-thrombotic diseases [Citation7]. It has been reported that APS may also cause hepatic artery thrombosis after liver transplantation [Citation43]. This article mainly reviews APS-related digestive system manifestations in clinical background, so we will not summarize the relevant situation here.
4.4.1. Thrombotic liver diseases
Budd-Chiari syndrome (BCS) may be the first clinical manifestation of APS [Citation7]. After Pomeroy C et al [Citation44] published the first case report describing the correlation between BCS and APL, several cases were reported afterwards [Citation45–54]. BCS is a major vascular disorder of the liver, characterised by structural and functional abnormalities of the liver resulting from the obstruction of the hepatic venous outflow from hepatic veins(the small hepatic veins, main hepatic veins and suprahepatic inferior vena cava) [Citation55,Citation56]. Some myeloproliferative diseases (MPDs) and predisposition to thrombotic conditions are considered as possible causes of BCS. In contrast, primary BCS is usually associated with risk factors for thrombosis (e.g. protein C and protein S deficiency, primary thrombocytopenia, etc.) [Citation55,Citation56]. APS may be the second most common cause of non-neoplastic BCS after primary MPDs [Citation49].
Hepatic infarction is a rare disease because of its dual blood supply system (portal vein and hepatic artery) that protects the liver from ischemia. However, in the APS context, cases of hepatic infarction were occasionally reported [Citation57–61], and most of the reported cases were pregnant women, that may be related to physiological characteristics such as venous stasis, coagulation tendency and changes in fibrinolytic system during pregnancy [Citation60,Citation62]. Moreover, most of the reported cases of hepatic infarction in pregnant women with APS were related to HELLP syndrome [Citation63,Citation64]. HELLP syndrome may appear as an initial characteristic of APS and highly suggest the further development of catastrophic antiphospholipid syndrome (CAPS) [Citation65].
4.4.2. Hepatic veno-occlusive disease (obstruction of small hepatic veins)
Hepatic veno-occlusive disease (HVOD) is a rare liver disease and a common life-threatening complication of bone marrow transplantation [Citation66]. It is thought to be caused by direct damage to the sinusoidal endothelium which can lead to non-thrombotic concentric narrowing of the central lobular vena cava, obstructing liver circulation and leading to stem cell necrosis [Citation67]. The association between HVOD and APS was first suggested by Pappas et al [Citation68]. Since then, several cases with HVOD and APL have been reported [Citation69–74].
4.4.3. Non-thrombotic liver diseases
Nodular regenerative hyperplasia (NRH) is often associated with a variety of systemic diseases [Citation75], characterised by diffuse transformation of liver parenchyma into small regenerative nodules in the absence of significant fibrosis [Citation76]. A total of 6 cases about the relationship between NRH and APS have been published [Citation22,Citation77–81].
APS related idiopathic non-cirrhotic portal hypertension (INCPH) cases have been reported [Citation82–87]. Currently, the etiology of INCPH can be divided into five categories, and APS plays an important role in the pathogenesis of autoimmune disease and pre-thrombotic state [Citation88].
Autoimmune liver disease (ALD) includes autoimmune hepatitis (AIH), primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PSC), and overlap syndrome. Few APS-related cases of autoimmune liver disease have been reported recently [Citation89–94].
4.5. Splenic manifestations
The splenic manifestations associated with APS are primarily splenic infarcts which are often associated with vascular damage to other abdominal organs [Citation95–98]. In a study of 89 patients with splenic infarction found that 39% of the patients had APS, especially in young patients under 50 years of age, and APS is the leading cause of splenic infarction [Citation99]. Auto splenectomy or functional asplenia, is a rare complication occurring in APS. Auto splenectomy or functional asplenia usually occurs in patients with SAPS, especially those secondary to systemic lupus erythematosus. Only three cases of APS has been reported with this complication so far [Citation100–102].
4.6. Pancreatic manifestations
A total of 10 APS related pancreatic lesions have been reported to date [Citation24,Citation103–111]. Pancreatitis was the main manifestation in 8 cases and pancreatic duct injury in the other 2 cases. One of these cases was characterised by recurrent acute pancreatitis, therefore special attention should be paid to APL in patients with idiopathic pancreatitis [Citation108].
4.7. The catastrophic antiphospholipid syndrome(CAPS)
Catastrophic antiphospholipid syndrome (CAPS) refers to the widespread thrombosis of small or large and small blood vessels in the body within a short period of time (usually within a few days to a few weeks), resulting in ischemia and necrosis of multiple organs [Citation1]. About 1% of patients with APS will develop CAPS [Citation1]. The main difference between APS and CAPS is the higher incidence of microthrombosis in CAPS patients, meanwhile, the mortality rate of CAPS patients was significantly higher than that of APS patients [Citation112]. Intestinal tract is the most common abdominal organ involved in CAPS patients, mainly presenting with abdominal pain, abdominal distension, nausea, vomiting and other symptoms of intestinal ischemia and necrosis, and in severe cases, diffuse necrosis of large and small intestine may occur. Autopsy of CAPS patients showed intestinal involvement in 30.5%, spleen involvement in 28.8%, liver involvement in 20.3%, pancreas and gallbladder involvement was relatively small [Citation113].
5. Treatment strategies
5.1. Drug treatment
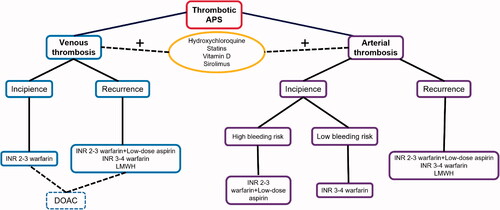
Anticoagulation is the basis of treatment for patients with thrombotic APS. Long-term anticoagulation therapy is recommended for patients with digestive system involvement by thrombotic APS. The target International Normalized Ratio (INR) 2-3 or 3-4 is recommended depending on clinical scenario [Citation114]. Warfarin therapy with target INR of 2-3 is recommended for patients with incipient venous thrombosis. While, for patients with recurrent venous thrombosis, addition of low-dose aspirin (LDA,75-100mg) or upregulated target INR of 3-4 with warfarin therapy or low molecular weight heparin (LMWH) may be considered [Citation114]. With warfarin therapy, target INR is recommended to be 3-4 in patients with low bleeding risk for arterial thrombosis. For patients at high bleeding risk, the target INR can be controlled at 2-3 with a co-administration of LDA (114). It should be noted that APS patients with target INR of 2-3 are more likely to have recurrent thrombosis events than APS patients with target INR of 3-4.And, the mortality of APS patients is higher due to thrombosis compared with bleeding [Citation115]. In patients with recurrent arterial thrombosis despite adequate treatment with warfarin, after evaluating potential causes, an increase of target INR to 3-4or addition of LDA or switch to LMWH can be considered [Citation114].
There are drawbacks of treatment with warfarin, including frequent laboratory monitoring, increased risk of bleeding and many interactions with diet and other medications. The direct oral anticoagulants (DOAC) become more attractive due to lack of dietary restrictions and regular laboratory monitoring, and relative ease of administration. DOAC is a single-enzyme anticoagulant that outperforms warfarin in many ways. It has less interactions with other medications and foods, and it doesn't necessitate INR testing on a regular basis [Citation116]. There is insufficient evidence to endorse or condemn the use of DOAC in thrombotic APS, according to Cochrane systematic review [Citation117]. However, according to recent randomised clinical trials and meta-analyses, in patients with triple positive aPL, there was a higher risk of thromboembolism recurrence and a higher incidence of major bleeding events in APS patients taking DOAC than those taking warfarin [Citation118–120]. The EULAR recommends DOAC as a possible treatment for patients with either absolute contraindication to warfarin or difficulty reaching the goal INR range [Citation114].
In addition, new treatment strategies are proposed recently for thrombotic APS. The anticoagulants are co-administered with hydroxychloroquine, statins, vitamin D and sirolimus. However, further studies are required to know the efficacy of these drugs in thrombotic APS treatment [Citation121]. A flow chart of the drug treatment strategies for thrombotic APS is illustrated in .
Figure 2. Drug treatment strategies for thrombotic APS. APS: antiphospholipid syndrome; LMWH: low molecular weight heparin; DOAC: direct oral anticoagulants.
For non-thrombotic APS patients, active intervention should still be carried out to prevent thrombotic events and accelerated atherosclerosis. Prophylaxis with low-dose aspirin is recommended for asymptomatic aPL patients to reduce the risk of adverse events such as antibody titres and thrombosis [Citation114]. The prophylactic treatment regimen for high-risk asymptomatic aPL patients remains low-dose aspirin. Studies have shown that traditional cardiovascular risk factors(such as hyperlipidemia, hypertension, smoking, obesity, diabetes, etc.) have additional effects on thrombosis and accelerated atherosclerosis in APS patients, therefore, non-thrombotic APS patients should actively control the traditional cardiovascular risk factors by changing their lifestyle and corresponding pharmacological management (such as lipid-lowering drugs, hypoglycemic drugs, antihypertensive drugs, etc.) to prevent accelerated atherosclerosis and arterial thrombosis [Citation114,Citation115].
APS patients generally do not need hormone or immunosuppressive therapy, but for SAPS, the use of hormones or immunosuppressive agents should be considered according to the actual situation [Citation114].As for the APS-related non-thrombotic digestive system manifestations mentioned above, due to the lack of reported cases and the lack of corresponding randomised clinical trials and systematic reviews, it is not clear whether hormones or immuno suppressants are beneficial to the disease progression and prognosis. However, the EULAR recommends the combination of glucocorticoids, heparin, and plasma exchange or intravenous immunoglobulin as the first-line treatment for CAPS patients [Citation114].
5.2. Interventional treatment
In terms of interventional therapy, there are currently no clinical trials to guide clinical decision-making. Only a few active cases of arterial thrombectomy have been documented [Citation122–124]. There are no reported cases of venous thrombectomy. Intravascular interventions such as balloon angioplasty and/or stenting are still controversial because of the hypercoagulability of APS patients and the risk of exacerbating thrombosis with interventional therapy. In addition, intravenous or arterial thrombolytic therapy were reported successfully dissolving venous thrombosis [Citation125] and effectively reducing acute macrovascular thrombosis [Citation126].
5.3. Surgical treatment
Surgical treatment of APS patients should be considered in patients with clinical symptoms, imaging and laboratory findings suggestive of necrosis or perforation of digestive tract [Citation127]. For these patients, open abdominal laparotomy is recommended to determine the viability of the bowel and the necessity of resection [Citation128]. It appears to be feasible to reconstruct arteries, but how to establish optimal anticoagulation regimes and long-term management after surgery is another challenge [Citation129]. There is inadequate large-scale clinical data and retrospective analysis to assess the long-term clinical efficacy and prognosis of surgical intervention in patients with acute thrombosis induced by APS.
6. Conclusion
Antiphospholipid syndrome includes a wide spectrum of thrombotic and non-thrombotic manifestations of the digestive system. The manifestations are diverse, complex and non-specific, easily confused with other abdominal diseases, making diagnosis difficult and leading to misdiagnosis. Attention should also be paid to the digestive system of APS patients, and the possibility of APS should be considered for recurrent multiple digestive organ lesions or multiple organ injuries. Anticoagulant therapy and prophylaxis are the basis of APS treatment. The proper treatment strategy should be considered according to the actual situation of patients to reduce the burden of thrombosis and bleeding. Interventional therapy and surgical treatment may increase the risk of thrombosis in APS patients. The advantages and disadvantages should be recognised and weighed on the basis of adequate anticoagulation.
Acknowledgements
No assistance in the preparation of this article is to be declared.
Disclosure Statement
The authors and reviewers have no relevant financial or other relationships to disclose.
Data availability statement
The data that support the findings of this study are available in [Pubmed] at [DOI:10.1016/s0163-7827(02)00048-6,DOI:10.1002/art.10187,DOI:10.1038/nrrheum.2017.124, DOI:10.1002/art.40901], reference number [2,6,10,11].
Additional information
Funding
References
- Petri M. Antiphospholipid syndrome. Transl Res. 2020;225:70–81.
- McIntyre J, Wagenknecht D, Faulk W. Antiphospholipid antibodies: discovery, definitions, detection and disease. Prog Lipid Res. 2003;42(3):176–237.
- Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4(2):295–306.
- Gomez-Puerta JA, Cervera R. Diagnosis and classification of the antiphospholipid syndrome. J Autoimmun. 2014;48-49:20–25.
- Asherson RA, Cervera R. Unusual manifestations of the antiphospholipid syndrome. Clin Rev Allergy Immunol. 2003;25(1):61–78.
- Cervera R, Piette JC, Font J, et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum. 2002;46(4):1019–1027.
- Uthman I, Khamashta M. The abdominal manifestations of the antiphospholipid syndrome. Rheumatol (Oxford)). 2007;46(11):1641–1647.
- Meroni PL, Borghi MO, Raschi E, et al. Pathogenesis of antiphospholipid syndrome: understanding the antibodies. Nat Rev Rheumatol. 2011;7(6):330–339.
- Fawzy M, Edrees A, Okasha H, et al. Gastrointestinal manifestations in systemic lupus erythematosus. Lupus. 2016;25(13):1456–1462.
- Sciascia S, Amigo M, Roccatello D, et al. Diagnosing antiphospholipid syndrome: 'extra-criteria' manifestations and technical advances. Nat Rev Rheumatol. 2017;13(9):548–560.
- Corban M, Duarte-Garcia A, McBane R, et al. Antiphospholipid syndrome: role of vascular endothelial cells and implications for risk stratification and targeted therapeutics. J Am Coll Cardiol. 2017;69(18):2317–2330.
- Duarte-García A, Pham M, Crowson C, et al. The epidemiology of antiphospholipid syndrome: a population-based study. Arthritis Rheumatol. 2019;71(9):1545–1552.
- Garcia D, Erkan D. Diagnosis and management of the antiphospholipid syndrome. N Engl J Med. 2018;379(13):1290.
- Zhang W, Gao F, Lu D, et al. Anti-β2 glycoprotein I antibodies in complex with β2 glycoprotein I induce platelet activation via two receptors: apolipoprotein E receptor 2' and glycoprotein I bα. Front Med. 2016;10(1):76–84.
- Bontadi A, Ruffatti A, Falcinelli E, et al. Platelet and endothelial activation in catastrophic and quiescent antiphospholipid syndrome. Thromb Haemost. 2013;109(5):901–908.
- Sule G, Kelley W, Gockman K, et al. Increased adhesive potential of antiphospholipid syndrome neutrophils mediated by β2 integrin mac-1. Arthritis Rheumatol. 2020;72(1):114–124.
- Pierangeli S, Girardi G, Vega-Ostertag M, et al. Requirement of activation of complement C3 and C5 for antiphospholipid antibody-mediated thrombophilia. Arthritis Rheum. 2005;52(7):2120–2124.
- Bae S, Lee Y. Association between plasminogen activator inhibitor-1 (PAI-1) 4G/5G polymorphism and circulating PAI-1 level in systemic lupus erythematosus and rheumatoid arthritis: a meta-analysis. Z Rheumatol. 2020;79(3):312–318.
- Kolitz T, Shiber S, Sharabi I, et al. Cardiac manifestations of antiphospholipid syndrome with focus on its primary form. Front Immunol. 2019;10:941.
- La Rosa L, Covini G, Galperin C, et al. Anti-mitochondrial M5 type antibody represents one of the serological markers for anti-phospholipid syndrome distinct from anti-cardiolipin and anti-beta2-glycoprotein I antibodies. Clin Exp Immunol. 1998;112(1):144–151.
- Mankai A, Manoubi W, Ghozzi M, et al. High frequency of antiphospholipid antibodies in primary biliary cirrhosis. J Clin Lab Anal. 2015;29(1):32–36.
- Klein R, Goller S, Bianchi L. Nodular regenerative hyperplasia (NRH) of the liver–a manifestation of organ-specific antiphospholipid syndrome? Immunobiology. 2003;207(1):51–57.
- Sipeki N, Davida L, Palyu E, et al. Prevalence, significance and predictive value of antiphospholipid antibodies in Crohn's disease. WJG. 2015;21(22):6952–6964.
- Nguyen HC, Dimou A, Govil A, et al. Primary antiphospholipid syndrome and necrotizing pancreatitis: a diagnostic challenge. J Clin Rheumatol. 2013;19(6):348–350.
- Cappell MS. Esophageal necrosis and perforation associated with the anticardiolipin antibody syndrome. Am J Gastroenterol. 1994;89(8):1241–1245.
- Naitoh H, Fukuchi M, Kiriyama S, et al. Recurrent, spontaneous esophageal ruptures associated with antiphospholipid antibody syndrome: report of a case. Int Surg. 2014;99(6):842–845.
- Padda A, Mandalia A, Sawalha AH. Clinical images: black esophagus in antiphospholipid syndrome. Arthritis Rheumatol. 2017;69(7):1460.
- Kalman DR, Khan A, Romain PL, et al. Giant gastric ulceration associated with antiphospholipid antibody syndrome. Am J Gastroenterol. 1996;91(6):1244–1247.
- Srivastava V, Basu S, Ansari M, et al. Massive gangrene of the stomach due to primary antiphospholipid syndrome: report of two cases. Surg Today. 2010;40(2):167–170.
- O'Malley J, Anatomy BB. Abdomen and pelvis, stomach gastroepiploic artery. StatPearls. Treasure Island (FL). 2020. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK545306/
- Levine J, Branch D, Rauch J. The antiphospholipid syndrome. N Engl J Med. 2002;346(10):752–763.
- Koenig M, Roy M, Baccot S, et al. Thrombotic microangiopathy with liver, gut, and bone infarction (catastrophic antiphospholipid syndrome) associated with HELLP syndrome. Clin Rheumatol. 2005;24(2):166–168.
- Vacca A, Garau P, Cauli A, et al. Primary antiphospholipid syndrome with mesenteric venous thrombosis presenting with intestinal infarction: a case description. Lupus. 2007;16(6):455–456.
- Wang QY, Ye XH, Ding J, et al. Segmental small bowel necrosis associated with antiphospholipid syndrome: a case report. World J Gastroenterol. 2015;21(13):4096–4100.
- Senatore FJ, McDonald K. Gastrointestinal: ischemic gastrointestinal manifestations in a young adult: Implicating a rare initial presentation of antiphospholipid syndrome. J Gastroenterol Hepatol. 2016;31(8):1381.
- Lock G. Acute intestinal ischemia. Best Pract Res Clin Gastroenterol. 2001;15(1):83–98.
- Kuhn F, Schiergens TS, Klar E. Acute mesenteric ischemia. Visc Med. 2020;36(4):256–262.
- Vianna JL, D'Cruz DP, Khamashta MA, et al. Anticardiolipin antibodies in a patient with Crohn's disease and thrombosis. Clin Exp Rheumatol. 1992;10(2):165–168.
- Kraiem I, Hadhri S, Ben Rejeb M, et al. Antiphospholipid antibodies and procoagulant profile in Tunisians with inflammatory bowel diseases. Clin Appl Thromb Hemost. 2016;22(8):734–742.
- Ates Y, Aslan M, Tuzun A, et al. Ulcerative colitis case beginning during pregnancy in a patient with antiphospholipid antibody syndrome. Turk J Gastroenterol. 2004;15(4):263–265.
- Racine A, Nahon S, Jouannaud V, et al. Portal vein thrombosis in a patient with quiescent crohn's disease associated with hyper homocysteinemia and antiphospholipid antibody syndrome 1-yr after an ileocecal resection. Am J Gastroenterol. 2008;103(2):499–501.
- Choobi Anzali B, Bahreini M, Habibi B, et al. Ischemic colitis due to antiphospholipid antibody syndrome. Turk J Emerg Med. 2019;19(1):36–38.
- Vivarelli M, La Barba G, Legnani C, et al. Repeated graft loss caused by recurrent hepatic artery thrombosis after liver transplantation. Liver Transpl. 2003;9(6):629–631.
- Pomeroy C, Knodell RG, Swaim WR, et al. Budd-Chiari syndrome in a patient with the lupus anticoagulant. Gastroenterol. 1984;86(1):158–161.
- Pati S, Bhattacharya S, Rakshit VM. Pregnancy complicated by Budd-Chiari syndrome and antiphospholipid syndrome. J Obstet Gynaecol. 2009;29(2):145–146.
- Mouelhi L, Chaieb M, Debbeche R, et al. Association Budd-Chiari syndrome, antiphospholipid syndrome and grave's disease. La Tunisie Medicale. 2009;87(2):164–166.
- Sciascia S, Mario F, Bertero MT. Chronic Budd-Chiari syndrome, abdominal varices, and caput medusae in 2 patients with antiphospholipid syndrome. J Clin Rheumatol. 2010;16(6):302.
- Yadav D, Chandra J, Sharma S, et al. Essential thrombocytosis and antiphospholipid antibody syndrome causing chronic Budd-Chiari syndrome. Indian J Pediatr. 2012;79(4):538–540.
- Sebastiani M, Manzini CU, Campomori F, et al. Unusual association between Budd-Chiari syndrome secondary to antiphospholipid syndrome and relapsing polychondritis: a case report and review of the literature. Clin Rheumatol. 2013;32(6):905–907.
- Bunge JJH, Wiersema US, Moelker A, et al. Refractory hypoxemia in a 23-year-old patient with Budd-Chiari syndrome. Chest. 2014;146(5):e149–e52.
- Zhao X, Liu K, Wu J, et al. One case of Budd-Chiari syndrome secondary to antiphospholipid syndrome. Zhonghua Gan Zang Bing Za Zhi. 2016;24(2):140–142.
- Pandiaraja J, Sathyaseelan A. Budd- Chiari syndrome as an initial manifestation of systemic lupus erythematosus. J Clin Diagn Res. 2016;10(4):OD01–2.
- Khan AH, Rahman MM, Rahaman MF, et al. Anti-phospholipid antibody syndrome presenting as huge ascites: a case report. Mymensingh Med J. 2018;27(4):883–887.
- Goldhar HA, O'Meara P, Castellucci LA. A case of antiphospholipid syndrome presenting cryptogenically as Budd-Chiari syndrome, then fulminantly as Libman-Sacks endocarditis. BMJ Case Rep. 2019;12(5):e227450.
- Khan F, Armstrong M, Mehrzad H, et al. Review article: a multidisciplinary approach to the diagnosis and management of Budd-Chiari syndrome. Aliment Pharmacol Ther. 2019;49(7):840–863.
- Van Wettere M, Bruno O, Rautou P, et al. Diagnosis of Budd-Chiari syndrome. Abdom Radiol (NY)). 2018;43(8):1896–1907.
- d'Ythurbide G, Rousset P, Carbonne B, et al. Liver infarcts with early HELLP syndrome and probable catastrophic antiphospholipid syndrome. Rev Med Interne. 2009;30(3):255–259.
- Guiu B, Loffroy R, Cercueil JP, et al. MRI diagnosis and follow-up of hepatic infarction in a patient with antiphospholipid syndrome in early pregnancy. Arch Gynecol Obstet. 2011;283(3):659–662.
- Madsen BS, Havelund T. HELLP in the second trimester in a patient with antiphospholipid syndrome. Ugeskr Laeger. 2011;173(5):357–358.
- Kim JH, Yee C, Kuk JY, et al. Hepatic infarction in a pregnant woman with antiphospholipid syndrome and triple antibody positivity: a case report focusing on catastrophic antiphospholipid syndrome. Obstet Gynecol Sci. 2016;59(5):397–402.
- Li C, Zhao J, Zhao Y. Hepatic infarction caused by antiphospholipid syndrome secondary to systemic lupus erythematosus. J Rheumatol. 2019;46(7):755–756.
- Gomez-Puerta JA, Cervera R, Espinosa G, et al. Catastrophic antiphospholipid syndrome during pregnancy and puerperium: maternal and fetal characteristics of 15 cases. Ann Rheum Dis. 2007;66(6):740–746.
- Le Thi Thuong D, Tieulie N, Costedoat N, et al. The HELLP syndrome in the antiphospholipid syndrome: retrospective study of 16 cases in 15 women. Ann Rheum Dis. 2005;64(2):273–278.
- Appenzeller S, Souza F, Wagner Silva de Souza A, et al. HELLP syndrome and its relationship with antiphospholipid syndrome and antiphospholipid antibodies. Semin Arthritis Rheum. 2011;41(3):517–523.
- Gómez-Puerta J, Sanin-Blair J, Galarza-Maldonado C. Pregnancy and catastrophic antiphospholipid syndrome. Clin Rev Allergy Immunol. 2009;36(2-3):85–90.
- Salman B, Al-Khabori M, Al-Huneini M, et al. Busulfan clearance does not predict the development of hepatic veno-occlusive disease in patients undergoing hematopoietic stem cell transplantation. Int J Hematol. 2020;112(2):210–216.
- Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. 2006;354(17):1813–1826.
- Pappas SC, Malone DG, Rabin L, et al. Hepatic veno-occlusive disease in a patient with systemic lupus erythematosus. Arthritis Rheum. 1984;27(1):104–108.
- Morio S, Oh H, Hirasawa A, et al. Hepatic veno-occlusive disease in a patient with lupus anticoagulant after allogeneic bone marrow transplantation. Bone Marrow Transplant. 1991;8(2):147–149.
- Rio B, Andreu G, Nicod A, et al. Thrombocytopenia in venocclusive disease after bone marrow transplantation or chemotherapy. Blood. 1986;67(6):1773–1776.
- Nakamura H, Uehara H, Okada T, et al. Occlusion of small hepatic veins associated with systemic lupus erythematosus with the lupus anticoagulant and anti-cardiolipin antibody. Hepatogastroenterol. 1989;36(5):393–397.
- Greisman SG, Thayaparan RS, Godwin TA, Lockshin MD. Occlusive vasculopathy in systemic lupus erythematosus. Association with anticardiolipin antibody. Arch Intern Med. 1991;151(2):389–392.
- Inam S, Sidki K, Al-Marshedy AR, et al. Addison's disease, hypertension, renal and hepatic microthrombosis in 'primary' antiphospholipid syndrome. Postgrad Med J. 1991;67(786):385–388.
- Barak N, Orion Y, Schneider M, et al. Case report: hepatic involvement in antiphospholipid syndrome. J Gastroenterol Hepatol. 1999;14(11):1124–1128.
- Bakshi N, Gulati N, Rastogi A, et al. Nodular regenerative hyperplasia - An under-recognized vascular disorder of liver. Pathol Res Pract. 2020;216(4):152833.
- Khanna R, Sarin SK. Non-cirrhotic portal hypertension - diagnosis and management. J Hepatol. 2014;60(2):421–441.
- Keegan AD, Brooks LT, Painter DM. Hepatic infarction and nodular regenerative hyperplasia of the liver with associated anticardiolipin antibodies in a young woman. J Clin Gastroenterol. 1994;18(4):309–313.
- Perez Ruiz F, Orte Martinez FJ, Zea Mendoza AC, et al. Nodular regenerative hyperplasia of the liver in rheumatic diseases: report of seven cases and review of the literature. Semin Arthritis Rheum. 1991;21(1):47–54.
- Morla RM, Ramos-Casals M, Garcia-Carrasco M, et al. Nodular regenerative hyperplasia of the liver and antiphospholipid antibodies: report of two cases and review of the literature. Lupus. 1999;8(2):160–163.
- Perez-Ruiz F, Zea-Mendoza AC. Nodular regenerative hyperplasia of the liver and antiphospholipid antibodies. J Clin Gastroenterol. 1998;27(1):90–91.
- Cadranel JF, Demontis R, Guettier C, et al. Nodular regenerative hyperplasia associated with primary antiphospholipid syndrome. Gastroenterol Clin Biol. 1996;20(10):901–904.
- Mackworth-Young CG, Gharavi AE, Boey ML, et al. Portal and pulmonary hypertension in a case of systematic lupus erythematosus: possible relationship with a clotting abnormality. Eur J Rheumatol Inflamm. 1984;7(3):71–74.
- Ordi J, Vargas V, Vilardell M, et al. Lupus anticoagulant and portal hypertension. Am J Med. 1988;84(3 Pt 1):566–568.
- Takahaski C, Kumagai S, Tsubata R, et al. Portal hypertension associated with anticardiolipin antibodies in a case of systemic lupus erythematosus. Lupus. 1995;4(3):232–235.
- De Clerck LS, Michielsen PP, Ramael MR, et al. Portal and pulmonary vessel thrombosis associated with systemic lupus erythematosus and anticardiolipin antibodies. J Rheumatol. 1991;18(12):1919–1921.
- Lauwerys B, Lambert M, Vanoverschelde J, et al. Myocardial microangiopathy associated with antiphospholipid antibodies. Lupus. 2001;10(2):123–125.
- Cikrikcioglu MA, Erkal H, Hursitoglu M, et al. Idiopathic portal hypertension during a catastrophic attack in a patient with primary antiphospholipid syndrome. Acta Gastroenterol Belg. 2010;73(4):521–526.
- Schouten J, Verheij J, Seijo S. Idiopathic non-cirrhotic portal hypertension: a review. Orphanet J Rare Dis. 2015;10:67.
- Targonska-Stepniak B, Majdan M, Suszek D, et al. Overlap syndrome autoimmune hepatitis and primary biliary cirrhosis associated with antiphospholipid syndrome. Pol Merkur Lekarski. 2006;21(125):480–483. [PMID] [17345845]
- Pamfil C, Candrea E, Berki E, et al. Primary biliary cirrhosis-autoimmune hepatitis overlap syndrome associated with dermatomyositis, autoimmune thyroiditis and antiphospholipid syndrome. J Gastrointestin Liver Dis. 2015;24(1):101–104.
- Hua R, Wu H, Zhang XW, et al. Probable catastrophic antiphospholipid syndrome complicated with primary sclerosing cholangitis. J Dig Dis. 2012;13(11):601–603.
- Rossi FW, Lobasso A, Selleri C, et al. Autoimmune tautology in a complex case of polyautoimmunity: systemic sclerosis, autoimmune liver involvement, antiphospholipid syndrome and hashimoto's thyroiditis. Isr Med Assoc J. 2017;19(3):193–195.
- Fedorchenko SV, Klimenko ZB, Martynovich TL. Antiphospholipid syndrome at the onset of clinical manifestations of chronic autoimmune hepatitis of type I. Ter Arkh. 2009;81(11):14–16.
- Romdhane H, Karoui S, Serghini M, et al. Crohn's disease, primary sclerosing cholangitis and antiphospholipid syndrome: an uncommon association. Tunis Med. 2009;87(5):349–351.
- You HX, Zhao JL, Wang Q, et al. Clinical features and risk factors of portal vein thrombosis in 28 patients with antiphospholipid syndrome. Zhonghua Nei ke za Zhi. 2019;58(12):894–898.
- Junge U, Wienke J, Schuler A. Acute Budd-Chiari syndrome, portal and splenic vein thrombosis in a patient with ulcerative colitis associated with antiphospholipid antibodies and protein C deficiency. Z Gastroenterol. 2001;39(10):845–852.
- Asherson RA, Morgan SH, Harris EN, et al. Arterial occlusion causing large bowel infarction-a reflection of clotting diathesis in SLE. Clin Rheumatol. 1986;5(1):102–106.
- Arnold MH, Schrieber L. Splenic and renal infarction in systemic lupus erythematosus: association with anti-cardiolipin antibodies. Clin Rheumatol. 1988;7(3):406–410.
- Wand O, Tayer-Shifman OE, Khoury S, et al. A practical approach to infarction of the spleen as a rare manifestation of multiple common diseases. Ann Med. 2018;50(6):494–500.
- Santilli D, Govoni M, Prandini N, et al. Autosplenectomy and antiphospholipid antibodies in systemic lupus erythematosus: a pathogenetic relationship? Semin Arthritis Rheum. 2003;33(2):125–133.
- Sheth K, Snyder A, Wu U, et al. Autosplenectomy causing catastrophic pneumococcal meningitis in a patient with lupus/antiphospholipid antibody syndrome. Conn Med. 2016;80(1):37–38.
- Pettersson T, Julkunen H. Asplenia in a patient with systemic lupus erythematosus and antiphospholipid antibodies. J Rheumatol. 1992;19(7):1159.
- Bird AG, Lendrum R, Asherson RA, Hughes GR. Disseminated intravascular coagulation, antiphospholipid antibodies, and ischemic necrosis of extremities. Ann Rheum Dis. 1987;46(3):251–255.
- Wang CR, Hsieh HC, Lee GL, et al. Pancreatitis related to antiphospholipid antibody syndrome in a patient with systemic lupus erythematosus. J Rheumatol. 1992;19(7):1123–1125.
- Chang KY, Kuo YC, Chiu CT, et al. Anti-cardiolipin antibody associated with acute hemorrhagic pancreatitis. Pancreas. 1993;8(5):654–657.
- Yeh TS, Wang CR, Lee YT, et al. Acute pancreatitis related to anticardiolipin antibodies in lupus patients visiting an emergency department. Am J Emerg Med. 1993;11(3):230–232.
- Chang LH, Francoeur L, Schweiger F. Pancreaticoportal fistula in association with antiphospholipid syndrome presenting as ascites and portal system thrombosis. Can J Gastroenterol. 2002;16(9):601–605.
- Spencer HL. Primary antiphospholipid syndrome as a new cause of autoimmune pancreatitis. Gut. 2004;53(3):468.
- Dellamonica J, Tieulie N, Bernardin G. Pancreatitis due to catastrophic antiphospholipid syndrome. Pancreas. 2007;34(3):380–381.
- Vyas A, Kadikoy H, Haque W, et al. Catastrophic antiphospholipid syndrome presenting as ischemic pancreatitis in systemic lupus erythematosus. JOP. 2009;10(5):566–569.
- Savey L, Piette JC, Bellanger J, et al. Catastrophic antiphospholipid syndrome (CAPS)-induced ischemic pancreatic ducts injury mimicking intraductal papillary mucinous neoplasm (IPMN). Semin Arthritis Rheum. 2018;47(4):565–568.
- Cervera R, Espinosa G, Cordero A, et al. Intestinal involvement secondary to the antiphospholipid syndrome (APS): clinical and immunologic characteristics of 97 patients: comparison of classic and catastrophic APS. Semin Arthritis Rheum. 2007;36(5):287–296.
- Bucciarelli S, Cervera R, Espinosa G, et al. Mortality in the catastrophic antiphospholipid syndrome: causes of death and prognostic factors. Autoimmun Rev. 2006;6(2):72–75.
- Tektonidou MG, Andreoli L, Limper M, et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann Rheum Dis. 2019;78(10):1296–1304.
- Chighizola CB, Raimondo MG, Meroni PL. Management of thrombotic antiphospholipid syndrome. Semin Thromb Hemost. 2018;44(5):419–426.
- Burnett AE, Mahan CE, Vazquez SR, et al. Guidance for the practical management of the direct oral anticoagulants (DOACs) in VTE treatment. J Thromb Thrombolysis. 2016;41(1):206–232.
- Bala MM, Celinska-Lowenhoff M, Szot W, et al. Antiplatelet and anticoagulant agents for secondary prevention of stroke and other thromboembolic events in people with antiphospholipid syndrome. Cochrane Database Syst Rev. 2017;10:CD012169.
- Cohen H, Hunt B, Efthymiou M, et al. Rivaroxaban versus warfarin to treat patients with thrombotic antiphospholipid syndrome, with or without systemic lupus erythematosus (RAPS): a randomised, controlled, open-label, phase 2/3, non-inferiority trial. Lancet Haematol. 2016;3(9):e426-36–e436.
- Woller S, Stevens S, Kaplan D, et al. Protocol modification of apixaban for the secondary prevention of thrombosis among patients with antiphospholipid syndrome study. Clin Appl Thromb Hemost. 2018;24(1):192.
- Dufrost V, Risse J, Reshetnyak T, et al. Increased risk of thrombosis in antiphospholipid syndrome patients treated with direct oral anticoagulants. Results from an international patient-level data meta-analysis. Autoimmun Rev. 2018;17(10):1011–1021.
- Chighizola C, Meroni P. Thrombosis and anti-phospholipid syndrome: a 5-year update on treatment. Curr Rheumatol Rep. 2018;20(7):44.
- Chou H, Jang S, Chen C, et al. Limb salvage in antiphospholipid syndrome with repetitive arterial occlusions. Neth J Med. 2019;77(7):264–267.
- Valente M, Saab J, Cordato D, et al. The diagnostic utility of routine clot analysis after endovascular thrombectomy in a patient with systemic lupus erythematosus and antiphospholipid syndrome. J Clin Neurosci. 2019;70:247–249.
- Vergallo R, Aguirre A, Abtahian F, et al. Recurrent myocardial infarctions and premature coronary atherosclerosis in a 23-year-old man with antiphospholipid syndrome. Thromb Haemost. 2016;115(2):237–239.
- Chen C. Direct thrombolytic therapy in portal and mesenteric vein thrombosis. J Vasc Surg. 2012;56(4):1124–1126.
- Nakayama S, Murashima N, Isobe Y. Superior mesenteric venous thrombosis treated by direct aspiration thrombectomy. Hepatogastroenterol. 2008;55(82–83):367–370.
- Brandt L, Boley S. AGA technical review on intestinal ischemia. Am Gastrointest Asso. Gastroenterol. 2000;118(5):954–968.
- Boley S, Kaleya R, Brandt L. Mesenteric venous thrombosis. Surg Clin North Am. 1992;72(1):183–201.
- Hinojosa C, Anaya-Ayala J, Bermudez-Serrato K, et al. Surgical interventions for organ and limb ischemia associated with primary and secondary antiphospholipid antibody syndrome with arterial involvement. Vasc Endovascular Surg. 2017;51(8):550–554.