
ABSTRACT
Interprofessional collaboration and practice (IPCP) is considered the cornerstone for effective service delivery for children with speech language and communication needs (SLCN). Following Stutsky and Spence Laschinger’s framework, we investigated IPCP-related differences between Dutch and Norwegian professionals in a cross-national comparative survey study. The personal relational skills of communication, trust and situational factor support structures were related to interprofessional collaboration in both countries. Trust was a stronger predictor for the Dutch sample than the Norwegian sample. A moderated moderation analysis revealed that the relationship between IPCP and perceived team effectiveness is moderated by trust for the Dutch professionals but not for their Norwegian colleagues. Trust may play a vital role for interprofessional teams in the Dutch context because service delivery is mainly characterised by the pull-out intervention of specialised professionals. In the integrated early intervention context of Norway, emphasis on professional communication skills seems a fruitful strategy to enhance the effectiveness of teams. Early intervention service delivery may be strengthened by structural facilitation and building networks to develop trust across professionals and organisations, which supports the development of professional competence relevant to IPCP in early intervention service delivery.
Introduction
Global advocacy for optimal developmental and educational outcomes and the close coincidence of mandated policies for inclusive early childhood education and care (ECEC) has stimulated interest in interprofessional collaborative practices (IPCP) in early intervention for young children with speech, language and communication needs (SLCN) (American Speech-Language-Hearing Association Citation2016; European Agency for Development in Special Needs Education Citation2013; UNESCO Citation1994; World Health Organization Citation2010). For young children, the ECEC setting is an important social context for language learning that may serve as a preventive site for intervention for SLCN. Collaborative service delivery is considered a vital part of customised intervention, and the effectiveness of collaborative intervention has been addressed in previous reviews (Archibald, Citation2017). Benefits of a collaborative approach relate to a higher frequency of intervention activities in the regular setting, less time away from peers for the child, the functional use of communication skills in daily settings and a reduced risk of stigmatisation (McKean et al. Citation2019).
To meet the complex needs of children and their families, professionals from different disciplines (e.g. speech-language therapy, early childhood teacher education, special needs education) often need to integrate their complementary competencies. IPCP for young children with SLCN currently occurs in diverse contexts with different organisations and degrees of integration for ECEC systems in different countries (Eurydice Citation2019). From an ecological perspective, interprofessional collaboration is vital to inclusive early childhood education, contributing to children’s development (Bartolo et al. Citation2021). IPCP can be understood as an operating mechanism at the micro-, meso- and/or macro-level of the ecological system. However, IPCP research on children and beneficial conditions for its improvement is limited (Bloom, Tufano, and Perez Citation2022). This study aims to investigate IPCP for children with SLCN in a cross-national comparative study.
Interprofessional collaborative practices: barriers and facilitators
IPCP has been defined as the delivery of comprehensive and integrated child and family services by multiple stakeholders (i.e. professionals with different backgrounds from within education and/or health care and support services as well as family/caregivers) to meet the needs of the child and family (ASHA, WHO, D’Amour and Oandasan Citation2005).
Stutsky and Spence Laschinger (Citation2014) offer a comprehensive model for IPCP, based on reviewing a large body of interprofessional literature. It includes elements relevant to interprofessional competence for intervention (Bruder et al. Citation2019) and considers factors at micro- and meso-level, including contextual conditions for IPCP, components and consequences for professionals and service users. Also, a macro-level is included, specifying conditions of care, service delivery and policy. Therefore, the model provides a valuable framework to identify barriers and facilitators for collaboration practices between professionals from different disciplines working within the ECEC setting and across educational and health support services.
The framework of Stutsky and Spence Laschinger assumes that IPCP is related to contextual factors. Contextual personal and situational conditions, such as relational skills of cooperation, communication and personal trust, and structural resources of time, space and procedures for collaboration, are combined with operating mechanisms in IPCP ().
Figure 1. Part of the conceptual framework for IPCP of Stutsky and Spence Laschinger used in this study.
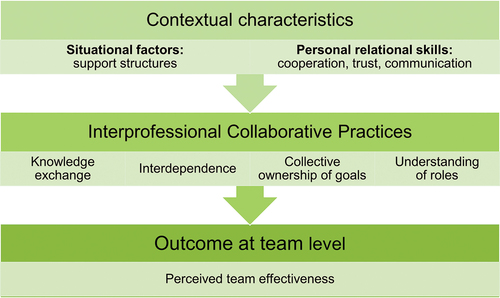
IPCP operating mechanisms involve understanding professional roles and responsibilities, exchanging knowledge, collective ownership of goals and interdependence to achieve professional and service user outcomes. Perceived team effectiveness involves the contribution of all team members to meet the service user’s needs and deliver high-quality services.
Barriers to collaboration in IPCP are related to differences in professional frameworks, perspectives, language, understanding of concepts, intervention approach and prioritisation of outcomes (Gallagher et al. Citation2019). A lack of understanding of professional roles carries the risk of underutilising available professional expertise and competence in a team (Suter et al. Citation2009). Facilitators for IPCP at this level include mutual engagement, shared professional values, understanding and goals, and collective competence and responsibility (Hartas Citation2004; Jacobsson Citation2022). Regarding situational conditions for IPCP, barriers are related to limited time resources and organisational structures for collaboration (Glover, McCormack, and Smith-Tamaray Citation2015; Hartas Citation2004). According to the literature, professionals’ relational expertise, including communication and trust, facilitates collaborative practices (Duhn, Fleer, and Harrison Citation2016; Edwards Citation2010). This implies that optimal structural conditions and high professional relationship skills benefit effective IPCP.
Comparative perspective on interprofessional collaborative practices
Interprofessional collaboration in health support services and educational systems is designed differently across countries and embedded in their specific cultural and social contexts (Garvis, Phillipson, and Harju-Luukkainen Citation2018). Theoretical models (e.g. Mulvale, Embrett, and Razavi Citation2016; Stutsky and Spence Laschinger Citation2014) distinguish between micro, meso and macro levels for IPCP. This comparative study explores how IPCP dynamics may be influenced by their national context.
As developed European OECD countries with high standards for education and health services (OECD Citation2021), Norway and the Netherlands are highly concerned with realising inclusive education and social inclusion for all children, aligned with the shared EU policy vision for ECEC (Cohen and Korintus Citation2017). Both countries aim to provide optimal support for children’s speech, language and communication development at an early age through interprofessional collaboration between teachers and specialised staff. However, the two countries differ regarding the structural and organisational context of ECEC systems and SLCN intervention service delivery (see next section). Studies comparing diverse contexts with various approaches and perspectives on IPCP are of interest because they provide an opportunity to increase understanding of systems across nations and professions (Bray et al. Citation2014; Esser and Vliegenthart Citation2017). Comparative studies help explore how professionals as key stakeholders experience barriers and facilitators for IPCP at individual and team levels by comparing them to peers who work under different conditions. Our cross-national comparative study aims to explore IPCP in intervention for children with SLCN in ECEC, as perceived by professionals in Norway and the Netherlands, to gain insights into IPCP around children with SLCN.
ECEC systems and SLCN support services in Norway and the Netherlands
Norway has a long history of unitary ECEC and an integrated system for inclusion. The Framework Plan (MER Citation2017) and Kindergarten Act (Kindergarten Act Citation2005) provide a holistic and pedagogical approach to care, upbringing and children’s development. In contrast, the Netherlands represents a fragmented and split system, with separate settings for children under/above age three and a focus on educational goals from age four. Only recently has the Netherlands begun to slowly move to a more integrated ECEC system.
National policies in Norway and the Netherlands have emphasised the development of supporting services for children with special needs (The Appropriate Education Act, Citation2014; Parliamentary announcement 6, MER Citation2019).
Within the Norwegian context, access to special education services, including SLCN services, is regulated by law (KA, chapter 7, §31), with service delivery based on the child’s benefit of adapted education. The municipal Educational and Psychological Counselling Service (EPCS) is mandated to assist kindergartens by providing counselling, assessing individual children and making recommendations for intervention. Interventions are often organised within the kindergarten setting and carried out by ECEC teachers, special educational needs teachers and other practitioners, who may receive counselling and advice from the ECPS speech-language therapist (SLT). For complex SLCN, an individual plan may facilitate collaboration, and supplementary direct (i.e. face-to-face working with the child) or indirect services can be provided by a national support system (Vulchanova, Feilberg, and Dahl Citation2019).
Norwegian research has emphasised the importance of communication, knowledge exchange, focus on collective goals for collaboration and clarity of roles regarding responsibility and division of tasks, as well as professional cooperation and trust (Cameron and Tveit Citation2019). Special educational needs assistance for children with language difficulties in Norway has been found to be inadequately supported by insufficient counselling and a lack of understanding of roles (Hannås and Hanssen Citation2016).
The Netherlands only recently focused on inclusive educational systems for all children, including the role of interprofessional collaboration between educational and health support service professionals. Support services related to SLCN are primarily delivered by SLTs working in special day-care groups (age 2–4, with conditional access) or SLT practices and by professionals working within day-care centres, (pre-)primary education or health centres. Service delivery is mostly organised by direct intervention, with approximately 50% of SLT combining a direct and indirect intervention approach, e.g. advising and coaching parents, teachers and pedagogical staff (Gerrits et al. Citation2019).
Present study
In this study, we focus on collaborating professionals, working towards the universal aim of optimal support for children with SLCN in an integrated or fragmented ECEC system. The study aims to investigate IPCP during intervention focusing on speech, language and communication needs in the Norwegian and Dutch ECEC context and its relations with situational and personal context factors. Our study asks two main questions: How do professionals from Norway and the Netherlands perceive IPCP in early intervention for children with SLCN in the ECEC context? Which personal contextual factors from the Stutsky and Spence Laschinger model (2014) moderate outcomes?
Based on the described differences in SLCN intervention service delivery in Norway and the Netherlands, we expected that the level of IPCP and professional benefits would be (slightly) higher in Norway than in the Netherlands (H1). Further, we explored whether self-reported IPCP is positively related to the professional-related outcomes of perceived team effectiveness. Finally, we explored whether personal characteristics relevant to IPCP (i.e. relational skills of communication, cooperation and trust) moderate the association between IPCP and the professional-related outcome of perceived team effectiveness, comparing the two countries.
Method
A comparative survey is a suitable approach for our study; it provides an appropriate and effective way to gather perceptions regarding IPCP and explore their associations with a large group of professionals in both countries. We used subscales of the Interprofessional Collaborative Practice Survey based on the model of Stutsky and Spence Laschinger (Citation2014).
Sample
Professionals from different disciplines (e.g. ECEC teachers, speech-language therapists, special education teachers) working within ECEC institutions and health support services and involved in the intervention phase for children aged 3 to 6 years with speech, language and communication needs were the population of interest. Seventy-one professionals from Norway (NO) and seventy-four professionals from the Netherlands (NL) participated in the survey. The sample was smaller for the questions related to personal and situational factors (NNO = 56/53 and NNL = 45) and professional-related outcomes (NNO = 58 and NNL = 49) due to attrition in the second part of the survey.
The number of participants from different disciplines differed for the two countries, reflecting the national systems pertaining to intervention provision for children with SLCN, including ECEC organisation and health support services (see Results). Specifically, in Norway, a larger part of the sample consisted of special educational teachers (35% in NO vs 18% in NL), while in the Netherlands, the largest part of the sample involved speech-language therapists (39% in NL vs 24% in NO). ECEC teachers represented a larger part of the Norwegian sample (24%) than in the Dutch sample (12%). Regarding the work setting, a larger part of the sample worked in an ECEC setting in Norway (65% vs 27% in NL) or a health support service setting (27% in NO vs 11% in NL). In comparison, the largest part of the sample in the Netherlands worked in a private practice setting (36% vs 6% in NO).
Procedure
Between June and September 2021, participants in Norway and the Netherlands were recruited through local, national and institutional networks by either telephone or email or digital announcements on websites or platforms for professionals. Invitations contained a letter with information about the research project, the purpose of the survey, participation, data management and privacy policy, and a link to the survey. Reminders were sent approximately three weeks after the initial contact.
The first author translated items from the Interprofessional Collaborative Practice Survey (ICPS) from Stutsky and Spence Laschinger (Citation2014; see Measures below) into Norwegian and Dutch. For the current study, terms like ‘health care’ and ‘patient’ from the original measure were replaced with ‘intervention’ and ‘child with SLCN’, respectively. Both Dutch and Norwegian translations were checked for word choice and formulations with native speakers in each language and back translations for some of the items.
Ethical approval for the data collection was received from the Norwegian Center for Research Data (NSD; reference number 295,967) and the ethical commission of the Faculty of Behaviorial Sciences of the University of Amsterdam (file 2021-CDE-13437). An information letter at the start of the survey addressed data management, privacy policy, data storage and ethical issues, including the right to withdraw, beneficence and non-maleficence, confidentiality, anonymity and non-traceability. All participants gave informed consent.
Questionnaire
Participants in both countries were asked to evaluate and categorise their experiences with interprofessional collaboration by answering a digital survey with 42 questions, including closed (39 questions) and open-ended (3 questions). The survey included various subscales of the ICPS from Stutsky and Spence Laschinger (Citation2014) to measure IPCP dimensions (see also ).
Knowledge exchange (3 items) measures profession-specific knowledge sharing between professionals (e.g. ‘When I have learned something new regarding intervention, I share the information with my colleagues in other disciplines’). Participants indicated their responses on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). This Likert scale applies to all Stutsky and Spence Laschinger scales below. The reliability of the knowledge exchange scale was good (Cronbach’s αNO= .67, αNL= .68).
Collective ownership of goals (4 items) focused on shared responsibility by professionals, children and their families in jointly defining, developing and achieving goals (e.g. ‘When professionals from different disciplines make decisions together, they go through a process of examining alternatives’). The scale was reliable (αNO= .52, αNL= .62).
Understanding of roles (3 items) includes items related to the knowledge and understanding of professionals about their own role and that of others (e.g. ‘Professionals from other disciplines with whom I work have a good understanding of the distinction between my role and their role(s)’, ‘Professionals from other disciplines do not treat me as an equal’). Reliability figures were different for the two samples (αNO= .10, αNL= .59), and we only analysed individual items because of the low reliability for the Norwegian sample.
Interdependence (3 items) measures the degree to which professionals have and rely on interactions between them, being dependent on each other for accomplishing goals and tasks (e.g. ‘I view part of my professional role as supporting the role of others with whom I work’, ‘I consult other professionals in different disciplines for their particular expertise’). The reliability of this scale was adequate (αNO = 0.52, αNL: = 0.61).
The four subscales were also aggregated in a measure of overall Interprofessional collaborative practice (13 items; αNO= .70, αNL= .78).
Three subscales were used to measure personal relational skills:
Trust (4 items) measures the confidence and reliance between professionals (e.g. ‘I have full confidence in the skills of my colleagues from other disciplines’). Internal consistency was good (αNO= .65, αNL= .81).
Cooperation (2 items) involves the way professionals work together for a common goal (e.g. ‘I involve professionals from other disciplines to carry out intervention activities’). The reliability of the short scale was good (αNO= .80, αNL= .78).
Communication (4 items) measures how easily and effectively professionals communicate (e.g. ‘I find it easy to ask advice of others in my team’). Reliability is adequate for both Norwegian and Dutch participants (αNO= .81, αNL= .65).
Support structures (4 items) focuses on situational context conditions and measures the availability of resources of time, space, policies, procedures and formal mechanisms to support IPCP (e.g. ‘Within my workday, I have time to meet with professionals from other disciplines to discuss intervention’). This subscale involved situational factors. Internal consistency of this scale was adequate (αNO= .56, αNL= .76). For technical reasons, this subscale was used with one item less than the original version.
Perceived team effectiveness (3 items) focuses on outcomes at team level and measures the perception of the team’s ability to meet service users’ needs and outcomes (e.g. ‘Our team does a good job in meeting the child and family member needs’). Reliability was good (αNO= .76, αNL= .77).
Background variables included professionals’ employment function, work setting, educational background and work experience. Other background variables involved structural characteristics of SLCN and intervention (e.g. regular place of intervention, number of SLCN children involved in intervention).
Analysis
The Norwegian and Dutch datasets were checked, cleaned up and merged into one dataset. Data analysis consisted of descriptive statistics for both samples (means and correlations) and inferential statistics (tests of difference between correlation coefficients). Our first hypothesis regarding higher scores of IPCP for the Norwegian sample was tested with independent t tests. To explore the role of IPCP, we conducted multiple regression analyses with perceived team effectiveness as the outcome variable, IPCP as the predictor, and the personal relational skills trust, communication and cooperation from the Stutsky and Spence Laschinger model as moderators. Our focus on relational skills was based on a first analysis of bivariate correlations that showed stronger correlations between trust and overall IPCP and support structures for the Dutch sample. Also, findings from a previous review study (Langner and Fukkink Citation2023) motivated our choice because this study highlighted the importance of personal factors for IPCP. Next, we analysed the regression model with the personal factors as key predictors. In addition, we investigated whether the moderated relationship between IPCP and perceived team effectiveness was different for Dutch and Norwegian professionals (i.e. a moderated moderation test) to explore country-specific patterns (see ).
Figure 2. Conceptual model for the relationship between IPCP (independent variable) and perceived team effectiveness (PTE), moderated by personal relational skills, moderated by country (moderated moderation).
We tested the models with SPSS and PROCESS, an add-on macro for the SPSS software packages written by Hayes (Citation2022). This tool can simultaneously model main effects, moderation and moderated moderation effects in an integrated model. We selected the moderated moderation model (Model 3) using a bootstrapping procedure (5000 bootstrap samples) and 95% confidence intervals. The three personal factors of interest from Stutsky and Spence Laschinger (Citation2014) were tested in separate models (see ).
Table 1. Descriptives for ICPS subscales (means and standard deviation, min-max: 1–5 for all scales).
Table 2. Pearson correlation matrix for the Dutch (under diagonal) and Norwegian sample (above diagonal).
Table 3. Regression models for perceived team effectiveness: model coefficients (with standard error) and model fit.
Moderation occurs when the size or direction of a predictor variable’s effect on an outcome variable depends on the value of the moderator variable. Significant moderation effects were probed using the pick-a-point techniques via the PROCESS script for SPSS. Significant moderation effects were visualised with moderator values at 16th, 50th and 84th percentiles.
The required sample size is 128 (NNL+NNO = 64 + 64) for a statistical test with adequate power to detect medium-sized differences at the conventional α level of .05 (2-sided) with a statistical power of .80. For testing medium-to-large correlations (i.e. r = .40), a sample size of 44 is required (two-sided test at α = .05, β = .80). Our study sample satisfied these requirements. Statistical power is adequate for testing large differences between correlation coefficients (power is .80, N = 132) but smaller for medium-sized differences. Main effects were tested at the conventional α level of .05 except for tested two-way interactions (i.e. the cross-product of IPCP*Country, IPCP*Personal factor) and three-way interactions (i.e. the cross-product of IPCP*Personal factor*Country), where α = .10was used, taking into account power problems in detecting interaction effects (McClelland and Judd Citation1993).
Results
Descriptive results for teacher, child and intervention characteristics
In Norway and the Netherlands, ECEC teachers, SLTs, counsellors and psychologists worked together around children with SLCN. Norwegian participants often mentioned special educational teachers as collaboration partners. Dutch professionals also mentioned audiologists, physio- and occupational therapists, ECEC centre directors, social workers and different physicians (child-, rehabilitation-, general practitioner, paediatrician, ear-nose-throat doctor). Internal interprofessional collaboration within an institution was rated of higher quality than external collaboration by large proportions (above 70%) of both the Norwegian and Dutch participants.
Participants from both countries were involved in intervention for children with needs related to the different domains of speech, receptive and expressive language and communication. All participants from Norway (100% vs 67% NL) reported the ECEC setting to be an intervention location. In comparison, a large proportion of the Dutch sample (80% vs 51% NO) reported the SLT practice office as the intervention location. Regarding intervention delivery, a larger proportion of the Norwegian sample reported indirect intervention delivery (68% NO vs 45% NL). Direct intervention by the specialist was reported by almost equal proportions of the samples (83% NO vs 89% NL). In addition, the Norwegian professionals reported that the intervention was delivered in small groups (70% NO vs 37% NL) and integrated into daily activities (76% NO vs 39% NL).
Comparative results: means and correlations
The overall mean for IPCP overall was moderate for both subsamples (). Means for the IPCP subscales, personal and situational factors and the perceived team effectiveness outcome were moderate to moderately high. There were no significant differences between the means for the Norwegian and Dutch samples on most subscales except for ‘interdependence’, t(130) = 2,162, p= 0.03, NL>NO, and ‘support structures’, t(76) = −2,844, p= < 0.01, NO>NL.
As shown in , the bivariate correlation between trust and overall IPCP was stronger for Dutch professionals (r = .69) than for their Norwegian peers (.42), p = .026. The correlation between trust and support structures was also stronger for the Dutch sample (.48) compared to the Norwegian sample (.12), p= .027.
Testing moderated relationships for Dutch vs Norwegian context
Finally, we investigated whether personal skills communication, cooperation and trust moderated the association between IPCP and perceived team effectiveness. All three models from showed statistically significant relationships between perceived team effectiveness (PTE) and the included predictors at the model level. The cooperation model did not show significant results at the individual predictor level, whereas the other two models did.
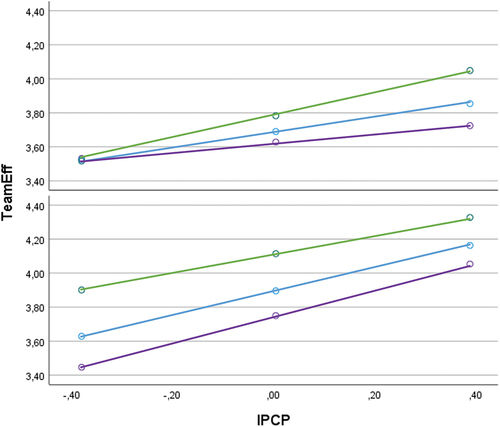
There were three significant predictors for the communication model. First, perceived team effectiveness is higher in Norway. Second, the interaction of IPCP and communication is positively related to PTE, which aligns with our theoretical model. Finally, there is a significant moderated moderation effect, which indicates different patterns for the Dutch and Norwegian participants. shows the positive relationship between IPCP and perceived team effectiveness for all levels of communication in both the Dutch and the Norwegian samples, as indicated by the inclining lines. For the Norwegian sample, the assumed relationship is similar, as indicated by the parallel lines. In contrast, the relationship becomes slightly stronger for the Dutch sample, as the diverging lines show. Hence, a positive relationship between IPCP and PTE for Dutch professionals only exists with higher levels of communication. There is not only a difference in slope but also in the intercepts. For the Norwegian participants, perceived team effectiveness is higher at all distinguished levels of communication.
Figure 3. Moderated moderation analysis with IPCP as independent variable, Perceived Team Effectiveness (PTE) as dependent variable and Communication (COM) as moderator variable for the Dutch (above) and Norwegian sample (below).
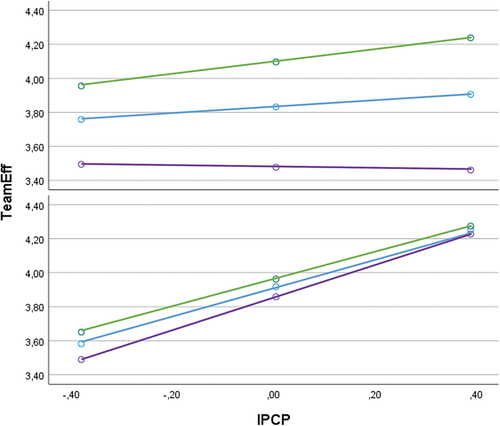
Five significant predictors were identified for the trust model. Trust and the interaction of trust with IPCP were significant, positive predictors of PTE, supporting the assumed relationship from our theoretical model. The significant interaction effects with country, including the moderated moderation effect, indicate country-specific patterns. shows a similar, positive relationship between IPCP and PTE for all levels of trust for the Norwegian sample, indicated by the three parallel, close lines. For the Dutch sample, the three lines show a different pattern. There is no relationship between IPCP and PTE in the Dutch context when trust is low (i.e. a flat line). The assumed positive relationship between IPCP and perceived team effectiveness for Dutch staff was only found at average and higher levels of trust.
Figure 4. Moderated moderation analysis with IPCP as independent variable, Perceived Team Effectiveness as dependent variable and Trust as moderator variable for the Dutch (above) and Norwegian sample (below).
In a final post-hoc analysis, we checked whether controlling for support structures would change the significance of our result for the trust model because of the significantly different correlations between trust and support structures in the two samples. Support structures was a non-significant control variable in this model (p = .805), and the results did not significantly change, confirming the results of the moderated moderation analysis.
Discussion
In our comparative study, we explored possible differences related to the level and the relationships between theoretically important IPCP dimensions for Dutch and Norwegian SLCN professionals. Concerning the organisation of early intervention service for children in ECEC, the Netherlands is dominated by a pull-out delivery, while in Norway, professionals reported an integrated way of working.
In contrast to our expectations, we did not find a significantly higher mean level of IPCP in Norway than in the Netherlands. In fact, we found a higher mean for the Dutch sample for interdependency. A possible explanation for our findings is the mainly pull-out intervention service delivery in the Netherlands, which has a long tradition. Dutch professionals seem to be aware of the need to collaborate, consult and support other professionals to deliver effective long-term intervention in the long-term, even though the professional team is not always co-located around the child. The higher level of support structures for Norway compared to the Netherlands is consistent with Norway’s long tradition of integrated and inclusive ECEC, where support structures have been in place for a long time.
In line with descriptions of professionals’ relational expertise as facilitators for collaboration (Duhn, Fleer, and Harrison Citation2016; Edwards Citation2010), our findings highlight the role of professional relations in the context of intervention for children with SLCN and show national differences between the Netherlands and Norway. Significant differences regarding the relationships between trust and IPCP, as well as between trust and support structures for the two countries, highlighted the moderating role of personal relational skills (trust, communication and cooperation) in the relationship between IPCP and perceived team effectiveness, as assumed by the Stutsky and Spence Laschinger model. The bivariate correlations indicated that trust and support structures were stronger predictors for IPCP for the Dutch staff than for the Norwegian staff. Consistent with findings on IPCP as a mediator between support structures and team effectiveness (Labrague et al., Citation2022), trust emerges as a crucial moderator for Dutch SLCN staff, even when accounting for variations in structural support.
The combination of communication and IPCP seems an important promotive factor for team effectiveness of Norwegian professionals. Our findings suggest that trust may be a more critical factor among professionals working in different settings and collaborating with diverse disciplinary teams around many children (i.e. a pull-out context), while communication is an important facilitator for professionals collaborating in more integrated contexts. Thus, investing in trust seems particularly important for IPCP in the Dutch context, whereas Norwegian staff may benefit more from developing communication. Effective strategies to cultivate trust can focus on either fostering specific relationships among individual professionals involved in IPCP over a longer period (Grimen Citation2008) or fostering general familiarity with other professions, thereby enhancing collaboration abilities and establishing new relations within diverse teams. Improving communication implies creating a common language by sharing disciplinary knowledge, understanding and perspectives on intervention. This, in turn, is beneficial for acknowledging and clarifying professional competence, roles, responsibilities and goals with the aim to improve collective competence and to increase counselling adequacy (Gallagher et al. Citation2019; Hannås and Hanssen Citation2016; Hartas Citation2004; Suter et al. Citation2009). Our findings emphasise relational skills like trust and communication between professionals as beneficial strategies to enhance team effectiveness, supporting previous findings in ECEC settings (Birch et al. Citation2023; Cameron and Tveit Citation2019).
Integrated intervention delivery shows potential for effective practices, recognising the importance of professional communication skills to improve IPCP and make specialised professional competence and tailored intervention available within the child’s daily ECEC context. Consistent with Stutsky and Spence Laschinger’s framework, professionals involved in integrated intervention contexts are encouraged to be aware of and adjust their professional language in interprofessional communication to discuss complementary professional knowledge and perspectives. It seems essential to be interested in others, ask for advice and engage in proactive and transparent communication. Where specialised professional competence through a pull-out intervention approach is available, building trust between professionals seems to be crucial to improving IPCP and the ability to deliver effective services to meet the child’s needs. Professionals should become familiar with and acknowledge other’s professional knowledge and perspectives to create a respectful and collaborative environment (Stutsky and Spence Laschinger Citation2014; Suter et al. Citation2009). Finally, the collaborative role of professionals in intervention emphasises the need for collaboration competence and implies offering interprofessional pre- and in-service programmes to prepare professionals for collaborative practices (Kent and McDonald Citation2021).
Limitations
As we investigated associations between multiple IPCP-related dimensions, we cannot make statements on causal relationships. Further, the subscale ‘understanding of roles’ was not reliable for our Norwegian sample, indicating a low internal consistency among items. This suggests that professionals from different disciplinary backgrounds and countries differently understand this dimension. Additionally, it is not possible to rule out bias as possible misinterpretations of questions, the tendency to provide socially desirable answers, and the influence of question sequence. There was a considerable dropout during answering the questionnaire, possibly attributable to the length of the questionnaire. Finally, we did not conduct a cross-validation study with a formal test of parallel, tau-equivalent or congeneric reliability of our measure (see Graham Citation2006; Jebb, Ng, and Tay Citation2021).
Further research
Despite the study’s limitations, we highlight its value, especially in ECEC, for providing contextualised insights and actionable proposals to improve factors at play while considering relevant factors at micro, meso and macro levels (Sousa and Moss Citation2022). International comparative research requires the development and validation of new IPCP measures that consider different national service delivery systems for early intervention. We also recommend further investigations into IPCP in countries with contrasting conditions for IPCP in early intervention to learn how to tailor IPCP to different contexts. Finally, findings indicate that a further in-depth study with qualitative data is needed to further contextualise the different situations of professionals when they collaborate in interprofessional teams.
Conclusion
Different service delivery systems for early intervention in Norway and the Netherlands imply significant differences related to conditions of support structures, the IPCP subdimension of interdependence and a significantly different role for personal relational skills of trust and communication for the relationship between IPCP and team effectiveness. Our findings suggest that trust is a more critical factor for professionals working in different settings (i.e. the Dutch pull-out context), whereas communication is important for professionals collaborating in an integrated fashion (i.e. Norway). Implications for improvement of team effectiveness and the design of coordinated and collaborative early intervention service delivery are twofold: (a) facilitation of structural support, such as clear policies and sufficient resources, to build social networks and trust between local educational and health support services and their staff, and (b) focus on the development of professional competence relevant for IPCP, to be realised in higher education, ECEC and health settings. Building networks and trust and develop communication competence is important when professionals can meet and collaborate.
Acknowledgments
We would like to thank B.Stutsky for making the Interprofessional Collaborative Practice Survey available to us.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- American Speech-Language-Hearing Association. 2016. Scope of Practice in Speech- Language Pathology. Available: www.asha.org/policy/.
- Archibald, L. M. 2017. “SLP-Educator Classroom Collaboration: A Review to Inform Reason-Based Practice.” Autism & Developmental Language Impairments 2. doi:10.1177/2396941516680369.
- Bartolo, P. A., M. Kyriazopoulou, E. Björck-Åkesson, and C. Giné. 2021. “An Adapted Ecosystem Model for Inclusive Early Childhood Education: A Qualitative Cross European Study.” International Journal of School & Educational Psychology 9 (1): 3–15. https://doi.org/10.1080/21683603.2019.1637311.
- Birch, S., S. Bow, J. Lang, and S. Dunsmuir. 2023. “Interprofessional Collaboration Between Educational Psychologists and Speech and Language Therapists in the UK: Facilitators and Barriers.” European Journal of Special Needs Education 38 (6): 1–16. https://doi.org/10.1080/08856257.2023.2172890.
- Bloom, R. D., V. E. Tufano, and C. T. Perez. 2022. “Registered nurses’ and Speech Language pathologists’ Interprofessional Collaboration: A Systematic Scoping Review of the Literature.” Nursing Forum 57:1129–1136. https://doi.org/10.1111/nuf.12802. 6
- Bray, M., B. Adamson, M. Mason, et al. 2014. “Different Models, Different Emphases, Different Insights.” In Comparative Education Research: Approaches and Methods, M. Bray 417–436. Springer International Publishing.
- Bruder, M. B., T. Catalino, L. A. Chiarello, M. C. Mitchell, J. Deppe, D. Gundler, P. Kemp, et al. 2019. “Finding a Common Lens: Competencies Across Professional Disciplines Providing Early Childhood Intervention.” Infants & Young Children 32 (4): 280–293. https://doi.org/10.1097/IYC.0000000000000153.
- Cameron, D. L., and A. D. Tveit. 2019. “‘You Know That Collaboration Works When … ’identifying the Features of Successful Collaboration on Behalf of Children with Disabilities in Early Childhood Education and Care.” Early Child Development and Care 189 (7): 1189–1202. https://doi.org/10.1080/03004430.2017.1371703.
- Cohen, B. J., and M. Korintus. 2017. “Making Connections: Reflections on Over Three Decades of EU Initiatives in Early Childhood Education and Care (ECEC).” Early Years 37 (2): 235–249. https://doi.org/10.1080/09575146.2016.1181050.
- D’Amour, D., and I. Oandasan. 2005. “Interprofessionality as the Field of Interprofessional Practice and Interprofessional Education: An Emerging Concept.” Journal of Interprofessional Care 19 (sup1): 8–20. https://doi.org/10.1080/13561820500081604.
- Duhn, I., M. Fleer, and L. Harrison. 2016. “Supporting Multidisciplinary Networks Through Relationality and a Critical Sense of Belonging: Three ‘Gardening tools’ and the Relational Agency Framework.” International Journal of Early Years Education 24 (3): 378–391. https://doi.org/10.1080/09669760.2016.1196578.
- Edwards, A. 2010. Being an Expert Professional Practitioner: The Relational Turn in Expertise. Vol. 3. New York: Springer.
- Esser, F., and R. Vliegenthart. 2017. “Comparative Research Methods.” The International Encyclopedia of Communication Research Methods 1–22. https://doi.org/10.1002/9781118901731.iecrm0035.
- European Agency for Development in Special Needs Education, 2013. Organisation of Provision to Support Inclusive Education – Literature Review [Online], Odense, Denmark: European Agency for Development in Special Needs Education: https://www.european-agency.org/resources/publications/.
- European Education and Culture Executive Agency, Eurydice. 2019. Key Data on Early Childhood Education and Care in Europe: 2019 Edition. Publications Office of the European Union. https://data.europa.eu/doi/10.2797/894279.
- Gallagher, A. L., C. A. Murphy, P. Conway, and A. Perry. 2019. “Consequential Differences in Perspectives and Practices Concerning Children with Developmental Language Disorders: An Integrative Review.” International Journal of Language & Communication Disorders 54 (4): 529–552. https://doi.org/10.1111/1460-6984.12469.
- Garvis, S., S. Phillipson, and H. Harju-Luukkainen. 2018. “An Introduction to Early Childhood Education and Care in the 21st Century: An International Perspective.” In International Perspectives on Early Childhood Education and Care, edited by Garvis, Phillipson and Harju-Luukkainen, 1–5, Routledge.
- Gerrits, E., J. de Jong, R. Zwitserlood, and I. Klatte. 2019. “Managing Children with Developmental Language Disorder: The Netherlands (National Vignettes).” In Managing Children with Developmental Language Disorder: Theory and Practice Across Europe and Beyond (Pp, edited by J. Law, C. McKean, C-A. Murphy, and E. Thordardottir, 339–350, London and New York: Routledge.
- Glover, A., J. McCormack, and M. Smith-Tamaray. 2015. “Collaboration Between Teachers and Speech and Language Therapists: Services for Primary School Children with Speech, Language and Communication Needs.” Child Language Teaching & Therapy 31 (3): 363–382. https://doi.org/10.1177/0265659015603779.
- Graham, J. M. 2006. “Congeneric and (Essentially) Tau-Equivalent Estimates of Score Reliability - What They are and How to Use Them.” Educational and Psychological Measurement 66 (6): 930–944. https://doi.org/10.1177/0013164406288165.
- Grimen, H. 2008. “Profesjon og tillit [Profession and trust.” In Profesjonsstudier [Professional Studies], edited by A. Molander and L. I. Terum, 197–212, Oslo: Universitetsforlaget.
- Hannås, B. M., and N. B. Hanssen. 2016. “Special Needs Education in Light of the Inclusion Principle: An Exploratory Study of Special Needs Education Practice in Belarusian and Norwegian Preschools.” European Journal of Special Needs Education 31 (4): 520–534. https://doi.org/10.1080/08856257.2016.1194576.
- Hartas, D. 2004. “Teacher and Speech-Language Therapist Collaboration: Being Equal and Achieving a Common Goal?” Child Language Teaching and Therapy 20 (1): 33–54. https://doi.org/10.1191/0265659004ct262oa.
- Hayes, A. F. 2022. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. 3rd ed. The Guilford Press.
- Jacobsson, A. K. 2022. “Communities of Practice: A Model for Professional Development in Early Childhood Education and Care to Support Children with Communication Barriers?.” In Special Education in the Early Years: Perspectives on Policy and Practice in the Nordic Countries, edited by H. Harju-Luukkainen, N. B. Hanssen, and C. Sundqvist 229–245, Springer International Publishing.
- Jebb, A. T., V. Ng, and L. Tay. 2021. “A Review of Key Likert Scale Development Advances: 1995-2019.” Frontiers in Psychology 12:637547. art. Nr. https://doi.org/10.3389/fpsyg.2021.637547.
- Kent, J., and S. McDonald. 2021. “What are the Experiences of Speech and Language Therapists Implementing a Staff Development Approach in Early Years Settings to Enhance Good Communication Practices?” Child Language Teaching and Therapy 37 (1): 85–97. https://doi.org/10.1177/0265659020974426.
- Kindergarten Act. 2005. Lov Om Barnehager. [Act on Kindergartens]. (LOV-2005-06-17-64) Lovdata. https://lovdata.no/dokument/NLE/lov/2005-06-17-64.
- Labrague, L. J., S. Al Sabei, O. AlRawajfah, R. AbuAlrub, and I. Burney 2022. “Interprofessional Collaboration as a Mediator in the Relationship Between Nurse Work Environment, Patient Safety Outcomes and Job Satisfaction Among Nurses.Journal of.” Nursing management 30 (1): 268–278. doi:10.1111/jonm.13491278.
- Langner, J., and R. G. Fukkink. 2023. “A Realist Synthesis of Interprofessional Collaborative Practices in Early Intervention for Children with Speech, Language and Communication Needs.” International Journal of Language & Communication Disorders 58 (2): 516–541. https://doi.org/10.1111/1460-6984.12789.
- McClelland, G. H., and C. M. Judd. 1993. “Statistical Difficulties of Detecting Interactions and Moderator Effects.” Psychological Bulletin 114 (2): 376–390. https://doi.org/10.1037/0033-2909.114.2.376.
- McKean, C., E. Gerrits, J. Tulip, and A. K. Tolonen. 2019. “Service Delivery for Children with Language Disorders Across Europe and Beyond.” In Managing Children with Developmental Language Disorder: Theory and Practice Across Europe and Beyond, edited by J. Law, C. A. Murphy, and E. Thordardottir, 84–109, London and New York: Routledge.
- MECS [Ministry of Education, Culture and Science]. 2014. MECS [Ministry of Education, Culture and Science].
- MER [Ministry of Education and Research]. 2017. Framework Plan for Kindergartens - Contents and Stasks. https://www.udir.no/contentassets/7c4387bb50314f33b828789ed767329e/framework-plan-for-kindergartens–rammeplan-engelsk-pdf.pdf.
- MER [Ministry of Education and Research]. (2019). Early Intervention and Inclusive Community in ECEC, School and After-School care. (Meld. St. 6 (2019–2020)). https://www.regjeringen.no/en/dokumenter/meld.-st.-6-20192020/id2677025/.
- Mulvale, G., M. Embrett, and S. D. Razavi. 2016. “‘Gearing Up’to Improve Interprofessional Collaboration in Primary Care: A Systematic Review and Conceptual Framework.” BMC Family Practice 17 (1): 1–13. https://doi.org/10.1186/s12875-016-0492-1.
- OECD. 2021. Health at a Glance 2021: OECD Indicators. OECD Publishing. https://doi.org/10.1787/ae3016b9-en.
- Sousa, D., and P. Moss. 2022. “Introducing the Special Issue on ‘Comparative Studies in Early Childhood Education: Past, Present and future’.” Comparative Education 58 (3): 287–296. https://doi.org/10.1080/03050068.2022.2071019.
- Stutsky, B. J., and H. K. Spence Laschinger. 2014. “Development and Testing of a Conceptual Framework for Interprofessional Collaborative Practice.” Health and Interprofessional Practice 2 (2): 7. https://doi.org/10.7710/2159-1253.1066.
- Suter, E., J. Arndt, N. Arthur, J. Parboosingh, E. Taylor, and S. Deutschlander. 2009. “Role Understanding and Effective Communication as Core Competencies for Collaborative Practice.” Journal of Interprofessional Care 23 (1): 41–51. https://doi.org/10.1080/13561820802338579.
- UNESCO (United Nations Educational, Scientific and Cultural Organization). 1994. The Salamanca Statement and Framework for Action on Special Needs Education. Paris: UNESCO.
- Vulchanova, M. D., J. Feilberg, and T. L. Dahl. 2019. “Norway (National Vignettes).” In Managing Children with Developmental Language Disorder: Theory and Practice Across Europe and Beyond, edited by J. Law, C. McKean, C-A. Murphy, and E. Thordardottir, 351–362, London and New York: Routledge.
- World Health Organization. 2010. Framework for Action on Interprofessional Education & Collaborative Practice. WHO. Available: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice.