
Abstract
Purpose
The clinical benefits of microprocessor-controlled prosthetic knees (MPKs) in community ambulators have been well-established. A systematic review in limited community ambulators published in 2014 found benefits in safety, performance-based, and patient-reported outcomes. This work updates the previous analysis to the current state of the published evidence.
Methods
Systematic review and meta-analysis of the effect of MPKs in limited community ambulators.
Results
Thirteen research projects presented in 15 publications were identified. Overall validity was “high” in nine studies, “moderate” in three, and “low” in one. The literature described a total of 2366 patients, with 704 classified as limited community ambulators. The use of MPKs in limited community ambulators led to a reduction in falls (SMD g: –0.59; 95% confidence interval (CI) [–0.85, –0.32; I2=0%]), fear of falling (SMD g: 1.2; 95%CI [0.55, 1.85; I2=80%]), risk of falling as indicated by the TUG (SMD g: –0.45, 95%CI [–0.87, –0.02; I2=0%]), an improvement in mobility grade (0.51; 95%CI [0.47,0.55]), self-selected walking speed (SMD g: 0.47; 95%CI [0.14,0.81; I2=0%]), and patient-reported ambulation (MD 9.32; 95%CI [3.61, 15.02; I2=7%]), and utility (MD 7.76; 95%CI [2.05–13.47; I2=0%]). Other outcomes exhibited trends in favor of MPK use or remained insensitive. No outcome was identified favoring non-MPKs.
Conclusions
These results suggest that MPKs may be considered a valuable therapeutic option in limited community ambulators with a transfemoral amputation.
Above knee amputees may be treated with a large variety of artificial exo-prosthetic knee components.
Microprocessor-controlled prosthetic knees have proven to be advantageous and cost effective for community ambulators.
The current analysis shows similar effects in safety, mobility, and patient perception also for limited community ambulators.
Microprocessor-controlled prosthetic knees are a viable therapeutic option for limited community ambulators.
Implications for rehabilitation
Introduction
Absence of a lower limb may be the consequence of congenital deformities, trauma, cancer, peripheral vascular disease (PAD), diabetic neuropathy, or other conditions. In a transfemoral prosthesis, the knee joint has to provide stability to prevent collapse during weight-bearing as well as enough toe clearance and speed adaptation during swing to prevent tripping [Citation1]. Controlled knee functions need to allow knee stance flexion for shock absorption and reciprocal gait on slopes, stairs, and uneven terrain. Microprocessor-controlled prosthetic knees (MPKs) resolved many challenges to ambulation with non-microprocessor-controlled prosthetic knees (NMPKs) that are struck with an inherent conflict between weight-bearing stability and safety on one side and support of knee function during stance on the other. The majority of clinical studies with MPKs have been conducted with unlimited community ambulators (Medicare Functional Classification Level (MFCL)-3) [Citation2] or higher. These studies have demonstrated improved safety, increased function and mobility [Citation3–5] during over-ground walking [Citation6–10], ambulation on uneven terrain [Citation6,Citation7,Citation9,Citation10], slopes [Citation6,Citation9,Citation11–13], stairs [Citation4,Citation9,Citation14–16], and in activities of daily living (ADL) with a high risk of falling [Citation4,Citation5]. Studies have shown a significant reduction in falls and improvement in balance compared to NPMK use [Citation4,Citation6,Citation9,Citation12,Citation13,Citation17,Citation18]. Cost-effectiveness of MPK use in individuals with MFCL-3 mobility has also been demonstrated [Citation19,Citation20].
Kannenberg et al. [Citation21] published a systematic review on the benefits of MPKs compared to NMPKs in limited community ambulators (MFCL-2) in 2014. They reported a reduction in falls by up to 80% and improvement in the risk of falling when using an MPK. Performance-based outcome measures showed that with MPKs, individuals with MFCL-2 mobility could walk 14–25% faster on level ground, 20% faster on uneven terrain, and 30% faster descending slopes. In addition, these subjects were capable to doing ADL that were considered typical for community ambulators with MFCL-3 mobility. The clinically meaningful improvements in performance-based safety, function, and mobility were mirrored by a high preference for the MPK in 90% of subjects but only in part by other patient-reported outcomes.
In the past years, MPKs have further evolved to better accommodate the needs of limited community ambulators [Citation22,Citation23]. Clinical investigations of increasing quality have been performed to address gaps in the clinical evidence [Citation24,Citation25]. Furthermore, results have been published from observational settings in larger cohorts in Germany, where the mobility grade is not a limiting factor for component selection [Citation26–28].
Even in high-income countries, such as the U.K. and the U.S., advanced prosthetic components are still reserved for physically more capable individuals [Citation29,Citation30]. However, the majority of individuals with transfemoral amputation in most countries is older than 65 years [Citation31] and does not usually reach the mobility level of a community ambulator [Citation32]. While budgetary aspects play an important role in technology access, healthcare payers often argue that there is a lack of sufficient clinical evidence for advanced componentry in this population. Recent recommendations suggest that subjects with lower mobility should be trialed with an MPK to assess their individual potential to benefit [Citation2].
In light of the diversity of treatment options for transfemoral amputees, it was the aim of the present work to appraise the current state of the published clinical evidence for benefits of the MPK technology in limited community ambulators.
The objective of the current analysis was to:
Provide an update of the systematic review published in 2014 [Citation21] comparing the effects of MPKs in transfemoral amputees with MFCL 2 or equivalent mobility grade (limited community ambulators) on safety, performance-based function, and patient-reported outcomes.
Assess the effect of MPK use by performing a meta-analysis of the existing published data.
Methods
Search strategy
A preparatory systematic literature search was conducted on 13 January 2020 [Citation33]. The final analysis was conducted on 5 July 2021, in the scientific literature databases Medline, Cochrane Library, CINAHL Complete, EMBASE, and Google Scholar. Search terms used were related to MPKs and individuals with unilateral knee disarticulation or transfemoral amputation and MFCL-2 or low mobility as well as peripheral arterial disease (PAD). Databases DARE, Cirrie (now NARIC Rehab Database), PEDRO, and OT Seeker were also searched with the search term logic adapted to their specific search structure. Full search terms are presented in the Supplementary material.
The literature search was limited to English- and German-language publications. The references of the analyzed papers were searched for additional relevant publications. The authors of identified studies were contacted and invited to indicate in alignment with the PRISMA reporting statement [Citation34] whether they were aware of unpublished work confirming or conflicting their publications. If ambiguity in the published literature required attention, selected authors were invited to make their data available for the meta-analysis.
Selection procedure
Titles and abstracts of identified publications were reviewed by AH and AK independently and screened for inclusion and exclusion criteria.
Inclusion criteria
Randomized or non-randomized comparative study that compared the outcomes with use of one or more MPKs to those with one or more NMPKs.
Study with results for subjects with knee disarticulation or above knee or transfemoral amputation and MFCL-2 or equivalent mobility grade. Limited community ambulators either had to be the primary study group or their results had to be presented as a separate subgroup analysis or as raw data that allowed for a post hoc statistical analysis.
Study reported quantitative and comprehensible results of validated outcome measures for safety, function, and mobility with prosthesis use and/or of patient-reported outcomes for perceived safety, function, and satisfaction with the prosthesis.
Exclusion criteria
Study with implantable knee joints (total or partial knee replacement).
Study that reported only opinions or qualitative evaluations of the authors rather than concrete quantitative results that allowed for an independent evaluation.
Duplicate, citation, content unrelated to objective of this investigation.
Evaluation of methodological quality
AH and AK independently rated relevant publications for their methodological quality. Any difference in rating or evaluation was discussed until mutual agreement was reached. The assessment was based on the State of the Science Evidence Report Guidelines as recommended by the American Academy of Orthotists and Prosthetists (AAOP) [Citation35] Internal validity assessment was based on 18 and external validity assessment on eight items.
Analysis
Results allowing a direct comparison of subjects fitted with an MKP and an NMPK were extracted. Data from mixed populations but sufficient reporting of individual results to allow for a comparison were re-analyzed. For some of the studies, the authors had direct access to the data, either as it stemmed from their own research or as other original study authors kindly supplied de-personalized data for re-analysis. If not indicated differently in this paper, absolute and relative differences and effect sizes and significance levels for suitable paired hypothesis tests were calculated using either a two-tailed paired t-test or Wilcoxon’s signed rank test. In case relative differences are presented, the 95% confidence interval (CI) was determined to check for statistical significance.
All data handling was performed in accordance with all applicable data protection legislation.
Outcomes were categorized as to whether they favor the use of MPKs, NMPKs, or none of the components. In case a suitable parameter was used in at least three independent studies, a meta-analysis of the parameter was conducted.
Measures of treatment effect in the meta-analysis
The mean differences (MDs) or standardized mean differences (SMDs) with 95%CIs were calculated for continuous outcomes that were measured in the studies for MPKs and NMPKs. Whenever possible, the MDs were presented, but many of the studies did not allow for direct comparison of similar outcomes. The differences between studies usually related to measured distances, times or measurement scales of outcomes, albeit the outcomes related to the same principal construct. Hedges’ g with an approximate bias correction as described by Hedges [Citation36] was calculated as the selected measure of effect size for SMDs.
Pooled estimates of overall differences for an outcome were calculated with both a fixed-effect and a random-effects model using inverse variance weighting and the DerSimonian and Laird method [Citation37] for estimating the between-studies variance within the random-effects model. For both models, a t-test was used for the pooled effect estimate.
Besides the outcomes reported as MD or SMD, change of mobility grade made up a special case of meta-analysis for a single proportion to calculate an overall proportion. A random intercept logistic regression model was utilized for the meta-analysis of this outcome [Citation38].
Assessment of heterogeneity
Heterogeneity was assessed using Cochrane’s Q-test (p value <0.10 is indicative of heterogeneity) and Higgins I2 statistic (low heterogeneity, <25%; moderate heterogeneity, 25–75%; and high heterogeneity, >75%) [Citation39].
Presentation of results
Meta-analysis results are presented in forest plots. The studies were sorted in order of decreasing standard error and, regardless of detected statistical heterogeneity, pooled estimates are presented for fixed-effect and random-effects models. Displaying both pooled estimates as opposed to choosing one model on the basis of heterogeneity was done because the differences in patient characteristics between the studies, which could not be controlled for, would be better generalized by a random-effects model than a fixed-effect model, even if low heterogeneity was detected.
However for the sake of transparency, fixed-effect model estimates were still included.
All analyses were conducted in R [Citation40] with the packages meta [Citation41] and metafor [Citation42].
Results
Literature search
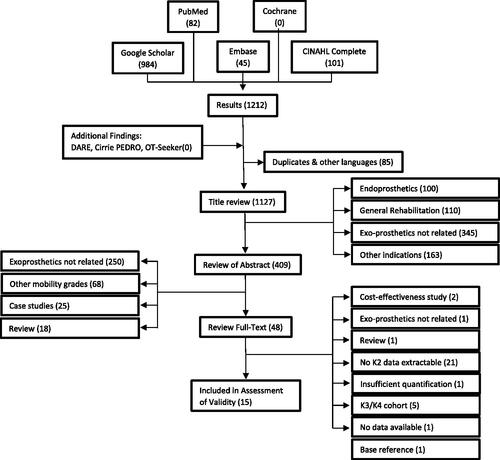
The numerical results of the literature search are shown in . After removal of empty links, citations, other language entries, and duplicates, 1127 items remained for title and, thereafter, 409 items for abstract review. Forty-eight publications were reviewed in full text. Fifteen publications met the inclusion criteria.
Figure 1. Flowchart of literature review process and results. Final analysis run on 5 July 2021. Search strings and further information are presented in the Supplementary material.
Davie-Smith and Carse [Citation43] reported on a retrospective cohort analysis in low mobility amputees characterized by an Amputee Mobility Predictor score of 40 or lower. Jayaraman et al. [Citation44] described a randomized cross-over trial in MFCL-2 subjects and vascular etiology while using the C-Leg. Lansade et al. [Citation25] performed a randomized cross-over study in low mobility amputees utilizing the MPK Kenevo. Kaufman et al. [Citation24] reported a prospective cross-over study in MFCL-2 amputees with four different MPKs (C-Leg Compact, Rheo Knee 3, Plie 3, Orion 2) whose results were pooled for analysis. Wong et al. [Citation45] studied the impact of the C-Leg on individuals with vascular amputation in a prospective cohort study. Mileusnic et al. [Citation23] described a prospective observational study on the first clinical use of the MPK Kenevo with limited community ambulators. Hasenoehrl et al. [Citation22] reported a pilot study with prospective A-B-A design to evaluate an MPK prototype for limited community ambulators with motion analysis and clinical outcome instruments. Hahn et al. [Citation26–28] published two independent retrospective analyses of results of 1223 or 899 trial fittings with C-Leg or Genium, respectively.
Already discussed by Kannenberg et al. [Citation21] were Kahle et al. [Citation9], Hafner and Smith [Citation46], Theeven et al. [Citation47,Citation48] including the respective study report by Seelen et al., provided as Supplementary material [Citation49], Burnfield et al. [Citation50] and Eberly et al. [Citation51].
Authors of all but one study answered the invitation to respond following the PRISMA statement. Hemmen responded on behalf of Theeven et al. and identified the work by Telgenkamp et al. as relating to the subject investigated here. Their randomized cross-over pilot study has been registered at the Netherlands Trial Register under no. NTR6456. The results have been submitted for publication and do not contradict the work presented earlier by the authors.
We are also aware of the work of Morgan [Citation52] relating in parts to the subject matter addressed here. No results have been published thus far.
Evaluation of methodological quality
The results of the evaluation of methodological quality of the publications included in this review are presented in and .
Table 1. Assessment of internal validity according to AAOP SoSc evidence report guidelines.
Table 2. Assessment of external validity and overall assessment assignment.
The rating according to the AAOP SoSc Evidence Report Guidelines identified the number of threats to internal validity ranging from 2 to 7. One study had a threat to external validity. The overall validity was assessed as “high” in nine studies, “moderate” in three, and “low” in one.
A further specification of the study design and a summary of the demographic information on the subjects are depicted in . The meta-analysis included those subjects who had an assigned mobility grade of MFCL-2 or equivalent or lower and for whom outcomes could be compared between MPKs and NMPKs. No attempt was made to further stratify for hip as an amputation level or for bilateral amputations.
Table 3. Design and demographic data of the MG2 subgroup analyzed.
Results of the performance-based and patient-reported outcomes regarding safety, subjects’ performance, usually denoted by functional outcome measures or prosthetists’ assessments, and patient-reported outcomes are depicted in . Outcomes were identified as eligible for the meta-analysis, if a comparison was possible with results of at least two other studies. Outcomes favoring MPKs are displayed with their respective absolute and/or relative magnitude, effect sizes and statistical significances, wherever possible. Outcomes are categorized as related to (a) safety (number of falls, fear of falling, risks of falling, etc.), (b) performance, function, and mobility, and (c) subjects’ perception. Outcomes that did not show statistical significance were listed separately.
Table 4. Subgroup analysis for subjects with MCFL-2.
Table 5. Hafner et al. report on the MFCL-2 subgroup separately.
Table 6. Theeven et al. investigated the impact of C-Leg (CL) and C-Leg Compact (CPCT) on MCFL-2 subgroups with high, intermediate (int) and low activity level.
Table 7. As only relative differences were reported, TUG, ABC, and Houghton scores could not be utilized for the meta-analysis.
Table 8. Subgroup analysis on original data.
Table 9. Subgroup extracted from publication.
Table 10. Subgroup extracted from original data.
Table 11. The exploratory pilot study by Hasenoehrl et al. showed high heterogeneity of subjects’ baseline status and subsequent performance.
Table 12. Analysis from publication.
Table 13. The authors kindly provided their de-personalized data set for meta-analyses.
Table 14. Data extracted from original publication.
Table 15. Jayaraman et al. provide both groups with the same foot component.
Table 16. Davie-Smith et al. applied 18 times Bonferroni’s correction to significance level.
With use of an MPK, significant reductions in falls were found by five studies [Citation9,Citation24,Citation43,Citation45,Citation46], significant improvements in indicators for the risk of falling in six studies [Citation25,Citation43–46,Citation50], significant improvements in the fear of falling by five studies [Citation23,Citation26,Citation44–46], and significant improvements in patients’ perception of safety in three studies [Citation26,Citation28,Citation47]. The latter were combined in the meta-analysis.
Significant improvements in performance-based outcomes with an MPK were reported for walking speed on level ground in five studies [Citation9,Citation43,Citation44,Citation46,Citation51], for slope ambulation in three studies [Citation9,Citation46,Citation50], for stair ambulation and uneven terrain mobility in two studies each [Citation9,Citation46], for ADL performance in one study [Citation47–49], and for activity [Citation24] and multitasking ability [Citation46] in one study each. In addition, five studies [Citation9,Citation26,Citation28,Citation44,Citation46] reported significant improvements in functional level from MFCL-2 to MFCL-3 in about 50% of subjects.
Significant improvements in patient-reported prosthetic function and mobility when using an MPK were found in seven studies [Citation9,Citation23–26,Citation28,Citation43,Citation44,Citation47–49] and for quality of life in one study [Citation25].
It is especially noteworthy that across all 13 studies, not a single outcome measure showed a significant benefit of NMPKs over MPKs in subjects with MFCL-2 mobility.
Results of the meta-analysis
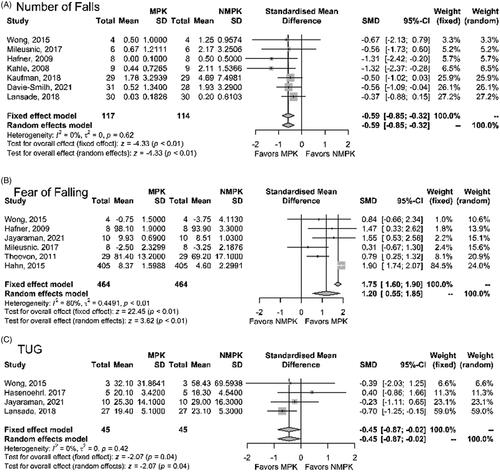
Safety-related outcomes demonstrating significant effects of MPK in the meta-analysis are shown in . Standardized mean differences were used to represent the significant reductions in number of falls, fear of falling, and TUG completion time.
Figure 2. Results of meta-analysis of safety-related outcomes. (A) The number of falls presented as standardized mean difference between MPK and NMPK. (B) The fear of falling presented as standardized mean difference between MPK and NMPK. (C) The “timed up and go” completion time presented as standardized mean difference between MPK and NMPK.
Results related to performance-based function and mobility are depicted in . The change in mobility grade was observed in six of the analyzed studies. The Houghton Scale analysis remained inconclusive (g: 0.01, p = 0.96).
Figure 3. Results of meta-analysis of outcomes related to function, performance and mobility. (A) Change of mobility grade from 2 to 3 with MPK fitting. (B) Change in self-selected walking speed presented as standardized mean difference between MPK and NMPK. (C) Change in fastest possible walking speed presented as standardized mean difference between MPK and NMPK.

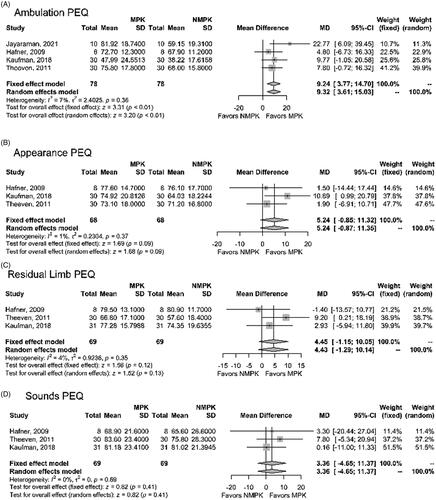
The meta-analysis of the patient-reported outcomes is shown in . The results of the PEQ domains of ambulation and utility indicate favorable results for the MPK, whereas the subdomains of appearance, residual limb health and well-being exhibited favorable trends. The ABC scale exhibits favorable effects in the fixed effect model.
Figure 4. Results of meta-analysis of patient-reported outcomes (PEQ domains). (A) The PEQ domain ambulation presented as mean difference between MPK and NMPK. (B) The PEQ domain appearance presented as mean difference between MPK and NMPK. (C) The PEQ domain residual limb health presented as mean difference between MPK and NMPK. (D) The PEQ domain sounds presented as mean difference between MPK and NMPK. (E) The PEQ domain utility presented as mean difference between MPK and NMPK. (F) The PEQ domain well-being presented as mean difference between MPK and NMPK. (G) The activity-based balance confidence (ABC) scale presented as mean difference between MPK and NMPK.

Discussion
The number of studies addressing the effectiveness of MPKs in limited community ambulators has increased notably over the past years. We identified publications relating to a total of 13 research projects, with nine publications expanding on the findings of Kannenberg et al. [Citation21].
Designs and outcomes utilized in these studies varied widely and covered a broad range of research approaches. This variability also poses a challenge and limitation to a comparative meta-analysis.
The meta-analysis provided clear insights that the use of MPKs in limited community ambulators led to a reduction in falls, fear of falling, an improvement in walking speed, mobility grade and patient-reported ambulation, utility and activity-based balance confidence.
Results on safety
Performance-based and patient-reported safety is the basis for comprehensive prosthesis use in everyday life and improvements in function and mobility [Citation54,Citation55]. The extent of improvements found in safety was comparable to those known for subjects with higher mobility levels. Fear of falling and safety perception has a severe impact on lifestyle as individuals usually actively avoid activities that they perceive as associated with a higher fall risk. That may result in social withdrawal and considerable decline in quality of life. In this context, Kaufman et al. reported that 30% of their subjects refused to revert from the MPK to their original NMPK due to fear of falling.
The reduction of TUG time indicates a reduced risk of falling [Citation56]. Earlier findings of Burnfield et al. [Citation50] were confirmed by Lansade et al. [Citation25] with the magnitude of the group effect equaling the minimal detectable change (MDC) identified by Resnik and Borgia [Citation57].
Across the 13 research projects, over 15 different outcome parameters were chosen to characterize safety. Most parameters indicated a favorable effect of MPKs. Fewer parameters indicated trends or remained insensitive. Not a single parameter hinted toward a decline of safety associated with the use of MPKs in limited community ambulators. The technical differences between MPK and NMPK that result in different safety profiles were described earlier by Blumentritt et al. [Citation4] and Kannenberg et al. [Citation21]. It may be noted that there are remarkable differences in design, safety, and functionality of the MPKs available [Citation58–60]. The study results presented in this review were predominantly generated with MPK with linear hydraulic units for comprehensive stance and swing phase control, namely C-Leg, C-Leg Compact (no longer available), Genium, and Kenevo. Few studies have attempted to identify the differential clinical effectiveness of different MPKs with results clearly suggesting significant differences in the capabilities of the various MPK technologies [Citation61–64]. A large cross-sectional study with 602 individuals with unilateral transfemoral amputation and MFCL-3 mobility found that only two of the four MPKs studied were able to significantly reduce the number of injurious falls compared to a historical control group using NMPK. The C-Leg and the Orion significantly prevented injurious falls, whereas the Rheo and the Plié knees did not [Citation64]. Any attempt to further clarify the differential effectiveness of the available MPKs would be commended. Caution is recommended with regards to claims of “parity” of different MPKs as this may lead to improper clinical decisions [Citation64]. Equivalence or non-inferiority between different MPKs has not yet been studied.
The reduction in falls has a major impact on the cost-effectiveness of exo-prosthetic components [Citation19]. Kuhlmann et al. [Citation65] confirmed the cost-effectiveness of the C-Leg in a population with unilateral transfemoral amputation with an average age around 65 years, even after stratification into sub-populations with and without diabetes mellitus. The sensitivity analysis identified that falling had the largest impact on the model outcomes. A further analysis investigating the effects in populations with even higher age and primarily vascular etiology in Sweden confirmed the importance of effective falls prevention [Citation66].
Performance, function, and mobility
The use of MPKs in limited community ambulators may lead to an improvement in mobility grade rating. This effect had first been observed by Kahle et al. [Citation9] and Hafner and Smith [Citation46] and has meanwhile been confirmed by four additional studies [Citation22,Citation26,Citation28,Citation44].
Mobility grade rating is a complex clinical process based to a large extent on a consensus of the clinical team and an extensive assessment of the subject. It includes the evaluation of the subject’s mobility potential. Most studies refer to the definitions of the MFCLs [Citation30]. Alternative rating systems, such as the German “Aktivitätsklassen” (“activity classes”) [Citation67] or the MOBIS system [Citation68] are very similar. Lansade et al. [Citation25] referred to the ICF classification with additional factors to characterize the patient. In the UK, the SIGAM classification is used [Citation29]. Davie-Smith and Carse [Citation43] were utilizing an AMPPro threshold of ≤40 for pragmatic reasons. Jayaraman et al. [Citation44] supported their assessment by measures including gait speed, BBS, and AMPPro measurements. Several attempts have been reported to objectify mobility grade rating and correlations with various clinical instruments were observed [Citation69]. To date, no unambiguous method of objectifying mobility grade has been established. The observation that advanced hydraulic MPKs improve the potential of subjects to exceed the level of limited community ambulators is of utmost importance. It implies that withholding such therapeutic options purely on grounds of the MFCL classification may severely restrict the functional and mobility potential of individuals with a transfemoral amputation, including exposing them to a higher risk of falling. Recent adaptations of treatment guidelines have helped overcome this restriction [Citation70] and expert work groups recommended “that if consideration is to be given to the provision of a microprocessor knee for an individual who currently utilizes his/her prosthesis at the K2 level (…) a trial of usage should be considered…” [Citation2]. However, the restrictions to appropriate access to advanced prosthetic componentry implemented by many healthcare payers have remained unchanged [Citation30].
Theeven et al. [Citation47,Citation48]. characterized limited community ambulator subgroups based on walking speed and activity level. Kannenberg et al. [Citation21] concluded that further research was required for amputees with walking velocities slower than 0.5 m/s. Kaufman et al. [Citation24] reported to have closed this evidence gap by showing significant benefits in this group in their study. The effects on self-selected walking speed improvement are well demonstrated by the meta-analysis.
Most parameters referring to aspects of performance, function, and mobility reflect walking on level ground, stairs, ramps, or uneven terrain. Biomechanical gait analysis was used as well as the characterization of ADL. The finding of Mileusnic et al. [Citation23] of significant reduction in wheelchair use is especially noteworthy. While the individual responses may differ, most studies identified significant benefits of MPK use in limited community ambulators. Not a single parameter indicated significance in favor of NMPKs.
Results on patient-reported outcomes
Kannenberg et al. [Citation21] reported a discrepancy between the results of performance-based and patient-reported outcomes. This was no longer found in this update. The meta-analysis identified that patient-reported outcomes, such as the PEQ domains of ambulation and utility significantly favored MPK use. Other PEQ domains showed trends in the same direction. The ABC scale showed favorable effects in the fixed effect model but remained insensitive in the random effects model.
Lansade et al. [Citation25] demonstrated highly significant improvements in the QUEST 2.0 that measures satisfaction with the fitting process and prosthesis, significant improvements in the LCI-5 for ADL performance, and SF-36 for quality of life and psychological well-being. Hahn et al. [Citation28] presented an improvement in perceived ease of a multitude of ADLs that was independent of the mobility level of the subjects, with toileting being an especially sensitive ADL. Mileusnic et al. [Citation23] reported trends in favor of the MPK for the Houghton Scale, the LCI-5 and the facilitation of a number of specific activities.
It was noticeable that improvements in the LCI-5 primarily occurred in the basic activities. That seems to reflect the basic improvements in safety by an MPK.
Hahn et al. [Citation28] found that toileting and specifically perceived safety while performing it turned out to be a particularly sensitive activity in a regression analysis. The benefit of an MPK in this activity was most clearly perceived by individuals with severe mobility restrictions. It is easily conceivable that an MPK may have a beneficial effect in such a vulnerable situation. This finding may underline that dimensions usually captured by commonly used validated assessment instruments may not be able to cover all important aspects of everyday life in their entirety. Aspects of self-care and maintenance of independence in body hygiene have rarely been studied in prosthesis users.
Methodological aspects
Quality assessment was based on the AAOP SoSc Evidence Report Guidelines. Kannenberg et al. [Citation21] used a procedure also utilized in a Cochrane review as suggested by Hofstad et al. [Citation71]. Preparatory work highlighted the limitations of the latter to appropriately differentiate the variety of research approaches to be analyzed in the current work. Alternative rating approaches, such as CAPS or JBI, allow for evaluating inclusion/exclusion criteria but fall short on assigning an overall quality rating. Generally, the methodology to assess quality of research in exo-prosthetic components remains challenging. While most approaches identify the lack of blinding as an inherent problem not only to this field as a quality limitation, mitigation measures, such as within-subject designs and repeated crossovers, often remain unrewarded.
The wide range of outcome measures used in the different clinical studies was striking. While the studies generally addressed the topics of safety, functional performance and patient-reported outcomes, the number of parameters used to provide quantification was vast.
Limitations
The body of evidence and the number of subjects included in the studies has increased considerably over the past years. Not a single study found any outcomes that demonstrated systematic benefits in favor of NMPK. The studies investigated a multitude of perspectives and covered a variety of settings and aspects of benefits of MPKs in the population of limited community ambulators.
The challenge of effective blinding in prosthetics limits the options for conducting studies to meet the formal criteria of high-quality research. Some studies suffered from high attrition that limits generalizability but also reflects the challenge of natural progression of underlying conditions, such as vascular disease and diabetes, especially during longer observation periods. All studies reported that some outcomes did not improve as expected, or that not all subjects experienced benefits of the intervention. While that reflects the reality of everyday clinical practice, it must also be considered that comorbidities and cognitive restrictions that may affect performance and perception are common in the studied population. In some studies, accommodation and training times may have been too short for these subjects.
These factors limit the universal generalizability of the results of this systematic review and meta-analysis. On the same token, there is no scientific basis for generally withholding MPKs with linear hydraulic units from individuals with low mobility.
The meta-analysis was limited by the vast variety of parameters characterizing clinical outcomes. Exploration of sources of study heterogeneity for an influence that moderator variables, such as the assessed study quality, might have on effect sizes was limited due to the relatively small number of studies that were pooled for the same outcome.
The same problem applied to any exploration of possible publication bias.
Different reporting standards limited the use of important data in a comparative analysis. Kahle et al. [Citation9] reported overall results on PEQ, Burnfield et al. [Citation50] reported on TUG, ABC, Houghton, and PEQ reporting the MD and significance level from paired testing. Hafner and Smith [Citation46] reported on SF-36 as total score. These data could not be transformed to fit the requirements of the meta-analysis as means and group standard deviations were missing. This is particularly regrettable as the results of the publications indicated their informative value leading to the assumption that the data may have helped to further resolve or minimize ambiguity.
Conclusions
The results of this updated systematic review and meta-analysis suggest that limited community ambulators may experience reduced falls, fear of falling, and risk of falling, improve mobility grade and patient-reported of ambulation and utility. The availability of meaningful clinical evidence has increased significantly. A lack of clinical evidence may no longer be used as an argument for withholding MPK technology from individuals with transfemoral amputation and low mobility. Trial fittings of limited community ambulators with MPKs may be considered a means to identify specific responders. Further research to study the specific needs and characteristics of that population may be considered.
Final_Report_Adelante_OB_201010.pdf
Download PDF (1.2 MB)Search_Strings_and_full_txt_rev_17Jul21.pdf
Download PDF (727.3 KB)Acknowledgements
The authors acknowledge authors of the analyzed literature responding to our invitation to comment on the knowledge of further data. We are grateful for depersonalized data being made available for the meta-analysis by Kaufman et al. and re-analyzed anonymous data being made available by Davie-Smith and Carse [Citation43].
Disclosure statement
Andreas Hahn is a full-time employee of Ottobock Healthcare Products GmbH Austria, the manufacturer of C-Leg, C-Leg Compact, Genium, and Kenevo, all MPKs cited in this analysis. Simon Bueschges is a full-time employee of STAT-UP Statistical Consulting & Data Science GmbH, he was contracted by Ottobock as a counselor to oversee the statistical analysis. Melanie Prager is a full-time employee of Ottobock Healthcare Products GmbH Austria. Andreas Kannenberg is a full-time employee of Ottobock Healthcare LP Austin, Texas, a distributor of C-Leg, C-Leg Compact, Genium and Kenevo, all MPKs cited in this analysis.
References
- Nelson VS, Flood KM, Bryant PR, et al. Limb deficiency and prosthetic management. 1. Decision making in prosthetic prescription and management. Arch Phys Med Rehabil. 2006;87(3 Suppl. 1):S3–S9.
- Lower Limb Prosthetic Workgroup. Health technology assessment consensus document. Baltimore (MD): Centers for Medicare and Medicaid Services (CMS); 2017.
- Sawers AB, Hafner BJ. Outcomes associated with the use of microprocessor-controlled prosthetic knees among individuals with unilateral transfemoral limb loss: a systematic review. J Rehabil Res Dev. 2013;50(3):273–314.
- Blumentritt S, Schmalz T, Jarasch R. The safety of C-Leg: biomechanical tests. J Prosthet Orthot. 2009;21(1):2–17.
- Blumentritt S. Biomechanische aspekte zur indikation von prothesenkniegelenken. Orthopäd Techn. 2004;55(6):508–524.
- Berry D, Olson MD, Larntz K. Perceived stability, function, and satisfaction among transfemoral amputees using microprocessor and non-microprocessor controlled prosthetic knees: a multicenter survey. J Prosthet Orthot. 2009;21(1):32–42.
- Kaufman KR, Levine JA, Brey RH, et al. Gait and balance of transfemoral amputees using passive mechanical and microprocessor-controlled prosthetic knees. Gait Posture. 2007;26(4):489–493.
- Segal AD, Orendurff MS, Klute GK, et al. Kinematic and kinetic comparisons of transfemoral amputee gait using C-Leg and Mauch SNS prosthetic knees. J Rehabil Res Dev. 2006;43(7):857–870.
- Kahle JT, Highsmith MJ, Hubbard SL. Comparison of non-microprocessor knee mechanism versus C-Leg on Prosthesis Evaluation Questionnaire, stumbles, falls, walking tests, stair descent, and knee preference. J Rehabil Res Dev. 2008;45(1):1–14.
- Seymour R, Engbretson B, Kott K, et al. Comparison between the C-Leg microprocessor-controlled prosthetic knee and non-microprocessor control prosthetic knees: a preliminary study of energy expenditure, obstacle course performance, and quality of life survey. Prosthet Orthot Int. 2007;31(1):51–61.
- Highsmith MJ, Kahle JT, Miro RM, et al. Ramp descent performance with the C-Leg and interrater reliability of the hill assessment index. Prosthet Orthot Int. 2013;37(5):362–368.
- Hafner BJ, Willingham LL, Buell NC, et al. Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee. Arch Phys Med Rehabil. 2007;88(2):207–217.
- Highsmith MJ, Klenow TD, Kahle JT, et al. Effects of the Genium microprocessor knee system on knee moment symmetry during hill walking. Technol Innov. 2016;18(2–3):151–157.
- Highsmith MJ, Klenow TD, Kahle JT, et al. Effects of the Genium knee system on functional level, stair ambulation, perceptive and economic outcomes in transfemoral amputees. Technol Innov. 2016;18(2–3):139–150.
- Lura DJ, Wernke MW, Carey SL, et al. Crossover study of amputee stair ascent and descent biomechanics using Genium and C-Leg prostheses with comparison to non-amputee control. Gait Posture. 2017;58:103–107.
- Schmalz T, Blumentritt S, Marx B. Biomechanical analysis of stair ambulation in lower limb amputees. Gait Posture. 2007;25(2):267–278.
- Highsmith MJ, Kahle JT, Shepard NT, et al. The effect of the C-Leg knee prosthesis on sensory dependency and falls during sensory organization testing. Technol Innov. 2014;2013(4):343–347.
- Highsmith MJ, Kahle JT, Bongiorni DR, et al. Safety, energy efficiency, and cost efficacy of the C-Leg for transfemoral amputees: a review of the literature. Prosthet Orthot Int. 2010;34(4):362–377.
- Chen C, Hanson M, Chaturvedi R, et al. Economic benefits of microprocessor controlled prosthetic knees: a modeling study. J Neuroeng Rehab. 2018;15:62.
- Cutti AG, Lettieri E, Del Maestro M, et al. Stratified cost-utility analysis of C-Leg versus mechanical knees: findings from an Italian sample of transfemoral amputees. Prosthet Orthot Int. 2017;41(3):227–236.
- Kannenberg A, Zacharias B, Pröbsting E. Benefits of microprocessor-controlled prosthetic knees to limited community ambulators: systematic review. J Rehabil Res Dev. 2014;51(10):1469–1496.
- Hasenoehrl T, Schmalz T, Windhager R, et al. Safety and function of a prototype microprocessor-controlled knee prosthesis for low active transfemoral amputees switching from a mechanic knee prosthesis: a pilot study. Disabil Rehabil Assist Technol. 2017;95:1–9.
- Mileusnic MP, Hahn A, Reiter S. Effects of a novel microprocessor-controlled knee, kenevo, on the safety, mobility, and satisfaction of lower-activity patients with transfemoral amputation. J Prosthet Orthot. 2017;29(4):198–205.
- Kaufman KR, Bernhardt KA, Symms K. Functional assessment and satisfaction of transfemoral amputees with low mobility (FASTK2): a clinical trial of microprocessor-controlled vs. non-microprocessor-controlled knees. Clin Biomech. 2018;58:116–122.
- Lansade C, Vicaut E, Paysant J, et al. Mobility and satisfaction with a microprocessor-controlled knee in moderately active amputees: a multi-centric randomized crossover trial. Ann Phys Rehabil Med. 2018;61(5):278–285.
- Hahn A, Lang M. Effects of mobility grade, age, and etiology on functional benefit and safety of subjects evaluated in more than 1200 C-Leg trial fittings in Germany. J Prosthet Orthot. 2015;27(3):86–95.
- Hahn A, Lang M. Corrigendum to 35. J Prosthet Orthot. 2019;31(1):80.
- Hahn A, Lang M, Stuckart C. Analysis of clinically important factors on the performance of advanced hydraulic, microprocessor-controlled exo-prosthetic knee joints based on 899 trial fittings. Medicine. 2016;95(45):e5386.
- NHS England: clinical commissioning policy: microprocessor controlled prosthetic knees; 2016 [cited 2020 Dec 12]. Available from: https://www.england.nhs.uk/wp-content/uploads/2016/12/clin-comm-pol-16061P.pdf
- Local Coverage Determination (LCD) L33787, lower limb prosthesis; 2020 [cited 2020 Jan 1]
- The Global Lower Extremity Amputation Study Group. Epidemiology of lower extremity amputation in centres in Europe, North America, and East Asia. Br J Surg. 2000;87(3):328–337.
- van Velzen JM, van Bennekom CA, Polomski W, et al. Physical capacity and walking ability after lower limb amputation: a systematic review. Clin Rehabil. 2006;20(11):999–1016.
- Hahn A, Kannenberg A. Zum nutzen mikroprozessorgesteuerter prothesenkniegelenke bei eingeschränkten außenbereichsgehern: eine aktualisierte systematische literaturanalyse (Do limited community ambulators benefit from using microprocessor controlled prosthetic knees? An update of a systematic review of the literature). Orthopäd Techn. 2020;71(5):46–57.
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA); 2020 [cited 2020 Jan]. Available from: http://www.prisma-statement.org/
- Hafner BJ. State-of-the-science evidence report guidelines. Washington (DC): American Academy of Orthotists & Prosthetists (AAOP); 2008.
- Hedges LV. Distribution theory for glass's estimator of effect size and related estimators. J Educ Behav Stat. 1981;6(2):107–128.
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188.
- Stijnen T, Hamza TH, Özdemir P. Random effects meta‐analysis of event outcome in the framework of the generalized linear mixed model with applications in sparse data. Stat Med. 2010;29(29):3046–3067.
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558.
- R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2020.
- Schwarzer G. Meta: an R package for meta-analysis. R News. 2007;7(3):40–45.
- Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48.
- Davie-Smith F, Carse B. Comparison of patient-reported and functional outcomes following transition from mechanical to microprocessor knee in the low-activity user with a unilateral transfemoral amputation. Prosthet Orthot Int. 2021;45(3):198–204.
- Jayaraman C, Mummidisetty CK, Albert MV, et al. Using a microprocessor knee (C-Leg) with appropriate foot transitioned individuals with dysvascular transfemoral amputations to higher performance levels: a longitudinal randomized clinical trial. J Neuroeng Rehabil. 2021;18(1):88.
- Wong K, Rheinstein J, Stern MA. Benefits for adults with transfemoral amputation and peripheral artery disease using microprocessor compared with non-microprocessor prosthetic knees. Arch Phys Med Rehabil. 2015;94(10):804–810.
- Hafner BJ, Smith DG. Differences in function and safety between Medicare Functional Classification Level-2 and -3 transfemoral amputees and influence of prosthetic knee joint control. J Rehabil Res Dev. 2009;46(3):417–434.
- Theeven P, Hemmen B, Rings F, et al. Functional added value of microprocessor-controlled knee joints in daily life performance of Medicare Functional Classification Level-2 amputees. J Rehabil Med. 2011;43(10):906–915.
- Theeven PJ, Hemmen B, Geers RP, et al. Influence of advanced prosthetic knee joints on perceived performance and everyday life activity level of low-functional persons with a transfemoral amputation or knee disarticulation. J Rehabil Med. 2012;44(5):454–461.
- Seelen HAM, Hemmen B, Theeven Patrick JR, et al. Functional added-value of prostheses with an electronically controlled stance and/or swing phase for patients with a unilateral transfemoral, a hip or a knee disarticulation. A clinical study. Final report; 2010.
- Burnfield JM, Eberly VJ, Gronely JK, et al. Impact of stance phase microprocessor-controlled knee prosthesis on ramp negotiation and community walking function in K2 level transfemoral amputees. Prosthet Orthot Int. 2012;36(1):95–104.
- Eberly VJ, Mulroy SJ, Gronley JK, et al. Impact of a stance phase microprocessor-controlled knee prosthesis on level walking in lower functioning individuals with a transfemoral amputation. Prosthet Orthot Int. 2014;38(6):447–455.
- Morgan SJ. Do microprocessor knees improve outcomes in early prosthetic rehabilitation compared to nonmicroprocessor knees. Defence Technical Information Center Technical Report; [updated 2017 Sep 15; cited 2018 Sep 14]. Available from: https://apps.dtic.mil/dtic/tr/fulltext/u2/1063860.pdf
- Theeven P, Hemmen B, Stevens C, et al. Feasibility of a new concept for measuring actual functional performance in daily life of transfemoral amputees. J Rehabil Med. 2010;42(8):744–751.
- Miller WC, Speechley M, Deathe AB. The prevalence and risk factors of falling and fear of falling among lower extremity amputees. Arch Phys Med Rehabil. 2001;82(8):1031–1037.
- Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348(1):42–49.
- Dite W, Connor HJ, Curtis HC. Clinical identification of multiple fall risk early after unilateral transtibial amputation. Arch Phys Med Rehabil. 2007;88(1):109–114.
- Resnik L, Borgia M. Reliability of outcome measures for people with lower-limb amputations: distinguishing true change from statistical error. Phys Ther. 2011;91(4):555–565.
- Thiele J, Schöllig C, Bellmann M, et al. Designs and performance of three new microprocessor-controlled knee joints. Biomed Tech. 2019;64(1):119–126.
- Bellmann M, Köhler TM, Schmalz T. Comparative biomechanical evaluation of two technologically different microprocessor-controlled prosthetic knee joints in safety-relevant daily-life situations. Biomed Tech. 2019;64(4):407–420.
- Bellmann M, Schmalz T, Blumentritt S. Comparative biomechanical analysis of current microprocessor-controlled prosthetic knee joints. Arch Phys Med Rehabil. 2010;91(4):644–652.
- Prinsen EC, Nederhand MJ, Olsman J, et al. Influence of a user-adaptive prosthetic knee on quality of life, balance confidence, and measures of mobility: a randomised cross-over trial. Clin Rehabil. 2015;29(6):581–591.
- Prinsen EC, Nederhand MJ, Sveinsdóttir HS, et al. The influence of a user-adaptive prosthetic knee across varying walking speeds: a randomized cross-over trial. Gait Posture. 2017;51:254–260.
- Hafner BJ, Askew RL. Physical performance and self-report outcomes associated with use of passive, adaptive, and active prosthetic knees in persons with unilateral, transfemoral amputation: randomized crossover trial. J Rehabil Res Dev. 2015;52(6):677–700.
- Campbell JH, Stevens PM, Wurdeman SR. OASIS 1: retrospective analysis of four different microprocessor knee types. J Rehabil Assist Technol Eng. 2020;7:205566832096847.
- Kuhlmann A, Krüger H, Seidinger S, et al. Cost-effectiveness and budget impact of the microprocessor-controlled knee C-Leg in transfemoral amputees with and without diabetes mellitus. Eur J Health Econ. 2020;21(3):437–449.
- Kuhlmann A, Hagberg K, Kamrad I, et al. A microprocessor-controlled prosthetic knee compared to non-microprocessor-controlled knees in individuals aged over 65 in Sweden – a cost-effectiveness and budget-IMPACT analysis; 2020–11, ISPOR Europe 2020; Milan, Italy. Value Health. 2020;23(S2):S576.
- Wetz HH, Hafkemeyer U, Drerup B. Einfluss des C-Leg-Kniegelenk-Passteiles der Fa. Otto Bock auf die versorgungsqualität oberschenkelamputierter: Eine klinisch-biomechanische studie zur eingrenzung von indikationskriterien [The influence of the C-Leg knee shin system of Otto Bock on the care of above-knee amputees: a clinical biomechanical study to define indications]. Orthopäde. 2005;34(4):298–319.
- MOBIS. The Otto Bock Mobility System 646A179 = GB-03-1301. Available from: www.ottobock.com
- Gailey RS, Roach KE, Applegate EB, et al. The Amputee Mobility Predictor: an instrument to assess determinants of the lower-limb amputee's ability to ambulate. Arch Phys Med Rehabil. 2002;83(5):613–627.
- The Rehabilitation of Individuals with Lower Limb Amputation Work Group. 2017. VA/DoD clinical practice guideline for rehabilitation of individuals with lower limb amputation. Version 2.0 – 2017. Available from: https://www.healthquality.va.gov/guidelines/Rehab/amp/VADoDLLACPG092817.pdf
- Hofstad CJ, van der Linde H, van Limbeek J, et al. Prescription of prosthetic ankle-foot mechanisms after lower limb amputation. Cochrane Database Syst Rev. 2004;(1):CD003978.