
Abstract
Objective:
(1) to describe environmental barriers and participation restrictions experienced by people with spinal cord injury (SCI) from China, (2) to examine associations between lesion characteristics and participation restrictions, considering a mediating role of environmental barriers, (3) to identify those environmental barriers that have the largest influence on participation.
Design:
Cross-sectional study. This study is part of the International Spinal Cord Injury Survey (InSCI).
Setting:
Community, Jiangsu and Sichuan Province, China.
Participants:
1355 persons with SCI.
Interventions:
Not applicable.
Outcome Measures:
Participation restrictions were measured with items from the Model Disability Survey, Environmental Barriers were measured with the Nottwil Environmental Factors Inventory-Short Form.
Results:
Participants experienced a median of five (IQR 1-9) environmental barriers and five (IQR 0-9) participation restrictions. Environmental barriers were mainly reported in relation to climate, insufficient resources and accessibility, and participation restrictions mainly occurred in using public transportation, taking care of others, and getting to places. In an adjusted zero-inflated Poisson model, people with more severe injuries reported a greater number of environmental barriers (complete injury: IRR = 1.31, 95%CI = [1.24,1.38]) and participation restrictions (tetraplegia: IRR = 1.15, 95%CI = [1.10,1.21]; complete injury: IRR = 1.25, 95%CI = [1.18,1.31]). Moreover, environmental barriers (IRR = 1.07, 95%CI = [1.06,1.08]) were a significant predictor of participation restrictions and partially mediated the association of lesion completeness with participation restrictions. Barriers related to accessibility of public places (IRR = 1.47, 95%CI = [1.33,1.62]), accessing homes (IRR = 1.32, 95%CI = [1.21,1.44]), long distance transportation (IRR = 1.11, 95%CI = [1.04,1.20]), communication devices (IRR = 1.07, 95%CI = [1.01,1.15]) and state services (IRR = 1.10, 95%CI = [1.02,1.19]) had the greatest negative impact on participation.
Conclusion:
Social participation of people with SCI is seriously restricted in China. Removing environmental barriers will be an important element of programs to address this problem.
Introduction
Social participation is a central goal of spinal cord injury (SCI) rehabilitation and critical for the health and quality of life of people with SCI.Citation1–4 Restrictions in participation of people with SCI can result from barriers in the environment such as inadequate medical and rehabilitation services, limited community accessibility, and negative attitudes.Citation5–9 Most studies on participation restrictions and environmental barriers encountered by people with SCI have however been conducted in high-resourced countries.Citation6,Citation10–12 Effects of environmental barriers on participation have been less researched in low- and middle-income countries. Two small qualitative studies conducted in Mongolia and Malaysia showed that participation restrictions were associated with insufficient accessibility of the natural and built environments, transportation, and lack of health care services.Citation13,Citation14 A study by Reinhardt and colleagues compared environmental factors reported in low and high resourced settings and found that fewer facilitators and more barriers were experienced in lower-resourced countries.Citation15 More recently, Reinhardt and associates compared environmental barriers experienced by people with SCI across 22 countries including China using data from the International Spinal Cord Injury Community Survey (InSCI) on which also the present study is based, In this study, more barriers were experienced in countries with greater overall income inequality and lower average household income of those with SCI, among others. Within countries, those with low income, paraplegia, complete lesions, and more health problems reported more barriers on average.Citation16 We are aware of only two previous studies specifically focusing on environmental barriers experienced by people with SCI in China. A study of 300 people with SCI from Shanghai showed that environmental barriers were among the most important predictors of decreased quality of life.Citation7 Another study by Xu et al. focused on a small population of earthquake victims with SCI.Citation17 This study found that environmental barriers were strongly associated with reduced physical and mental function and quality of life. While also utilizing data from China, the above quoted study by Reinhardt et al.Citation16 more broadly compared the situation in different countries and not specifically addressed the situation in China. Moreover, the effect of environmental barriers on other health-related outcomes including participation was not investigated.
Since little attention has been paid to participation restrictions and environmental barriers experienced by people with SCI in ChinaCitation18 as well as interactions between impairment, environmental barriers and participation restrictions, research in this area is urgently needed in order to raise awareness and identify intervention targets to promote community and social participation of people with SCI.Citation18 We hypothesized (1) that more participation restrictions were experienced by participants with more severe SCI, i.e. people with tetraplegia (vs. paraplegia) and those with complete lesions (vs incomplete), and (2) that environmental barriers were a mediator of relation of SCI characteristics and participation restrictions ().
Figure 1 Model illustrating research hypotheses.
Note: “+” represents positive association.
This study aimed (1) to describe environmental barriers and participation restrictions experienced by people with SCI who live in the community in China, (2) to examine the association between SCI severity, and participation restrictions, and if this association was mediated by environmental barriers, and (3) to identify those environmental barriers which had the largest influence on participation.
Materials and methods
Design
This cross-sectional study was implemented in Jiangsu and Sichuan Province of the People's Republic of China according to a protocolCitation18 developed within the design of the InSCI.Citation19 The International Classification of Functioning, Disability and Health (ICF) which describes functioning as a dynamic interaction between people's health status, personal factors and environmental factorsCitation20–22 was used as conceptual framework for this study.
Procedures and participants
The data used in this study were collected in Jiangsu and Sichuan Province, China, and represented the Chinese contribution to InSCI,Citation19 an international initiative implemented in 22 countries with the goal to better understand problems and needs of community-dwelling individuals with SCI.Citation23–25 Details on recruitment and composition of the overall cohort from all 22 countries are reported by Fekete and colleagues.Citation26 In both participating Chinese provinces recruitment was based on databases from large university and province level hospitals (level III) with catchment areas encompassing the whole province. In addition, city (level II and III) and county level (level I and II) hospitals were selected based on stratified random sampling. City level hospitals are regional hospitals providing health services across several communities and technical centers for regional medical treatment. County level hospitals are primary health care institutions that provide comprehensive services of medical treatment and health care directly to the community. People with SCI who had been treated in these hospitals were identified by systematically searching these databases for Chinese SCI-related terms in diagnosis (free text) and ICD-10 or ICD-9 codes (see Appendix 1). People on the lists were contacted by telephone to confirm consent and where applicable determine time and location of the investigation. The survey was then conducted by telephone interview, online self-report, or face-to-face interview. The contact rate was 33.5%, the cooperation rate (those who could be contacted and consented to participate) was 68.3% and the gross response rate was 22.1 (percentage of those surveyed from all attempted to contact).Citation26
The interviewers in this study were all postgraduates from universities with majors in Rehabilitation, Nursing, or Public Health. Before the start of the survey, the interviewers participated in unified training sessions, which required them to master background, purpose and significance of this study, as well as matters needing attention during interviews, such as avoiding leading questions. Data were collected between January and December 2018. On average, it took about 30–45 min for respondents to complete the questionnaire. All data were treated confidentially, and the assigned InSCI ID was used as a unique identification code. Data that had been collected on print (paper-pencil) questionnaires during face to face or telephone interview were entered into the electronic database jointly by two investigators and double-checked by a third investigator afterwards.
The inclusion criteria as defined per InSCI protocolCitation19 were: adults 18 years or older (in China: 16 years), having sustained a traumatic SCI (including cauda equina syndrome) or non-traumatic SCI (vascular, infection or tumor), and living in the community. Congenital diseases (such as spina bifida), progressive diseases (such as autoimmune diseases, toxic factors, radiation-induced diseases, multiple sclerosis and amyotrophic lateral sclerosis), peripheral nerve injury (such as Guillain-Barré syndrome) and people with newly diagnosed spinal cord injury (acquired SCI less than 3 months before data collection) who had been hospitalized for the first time were excluded.
There were 1366 completed questionnaires. Of those four were excluded because respondents were younger than 16 years old at the time of the survey, one was excluded because of a congenital condition (congenital atlantooccipital malformation), and six were excluded because of progressive diseases (five with encephalomyelitis, and one with Amyotrophic Lateral Sclerosis). Data from 1355 eligible participants were analyzed.
Measures
Data model and items of the InSCI questionnaire were based on the brief ICF Core Set for SCI in the long-term context and the international SCI Data Set as described in more detail elsewhere.Citation27 Items and scales from standardized international instruments linked to the relevant ICF categories were used wherever possible. Translation into Chinese was conducted as prescribed by the international protocolCitation19 if validated Chinese versions of the respective items had not been developed previously.
Participation restrictions
The Model Disability Survey (MDS)Citation28 is an ICF-based tool recommended by the World Health Organization to collect data on disability at the population level. It was developed based on an analysis 179 disability surveys used in different countries. Expert consultations were used to ensure the MDS's content validity. The MDS was furthermore piloted and has undergone cognitive testing in multiple countries including China.Citation29 Thirteen MDS items (such as “carrying out daily routine”, “handling stress”) were selected for the InSCI survey.Citation19,Citation27 For each item, participants were asked the question “In the last 4 weeks, how much of a problem have you had in … ?”. The responses to each item were measured by a 5 point Likert-Scale ranging from “1-no problem” to “5-extreme problem”. In our analyses, we dichotomized the respective variables (no or mild problem = 0, moderate to extreme problem = 1) with 1 or 2 indicating no or insignificant problem and 3, 4, 5 indicating having at least a moderate problem. The rationale for dichotomization was to minimize the effect of differential interpretation of response options by the participants and increase reliability. A count index of the number of all reported participation restrictions was then calculated. This was done since a common metric for the selected MDS items applicable to all InSCI countries has yet to be developed. Cronbach's alpha for the count index was 0.94 in the analyzed Chinese sample.
Environmental barriers
The Nottwil Environmental Factors Inventory-Short Form (NEFI-SF)Citation30 is a 14-item scale used to measure the extent that environmental barriers make people's daily life more challenging. Items relate to climatic conditions, the built environment, transportation, attitudes, devices and medical supplies, financial resources and services. Participants were asked how much these environmental barriers influenced them during the last four weeks. Answers options were “not applicable”, “no influence”, “made my life a little harder” and “made my life a lot harder”. For our analyses, we considered the former two options (i.e. “not applicable” and “no influence”) as no barriers experienced in the respective area (0), while the latter two answers were recoded as experienced barrier (1). Validity and reliability of the NEFI-SF have been established in previous studies.Citation30,Citation31 An index representing the number of environment barriers experienced by participants was calculated by summing the scores of all dichotomized items. This index solution has produced good internal consistency in previous Chinese studies using NEFI-SF.Citation17,Citation32 Here Cronbach's alpha was 0.92.
Lesion characteristics
Lesion characteristics were assessed based on self-report. Participants were asked to describe the type of their spinal cord injury: paraplegia (normal movement and feeling in the upper limbs) or tetraplegia (absent or abnormal movement or feeling in the upper and lower limbs) and whether their injury was complete (unable to feel and move any part of your body below injury level) or incomplete (able to feel or move some part/s of your body below injury level).
Control variables
Sex (female = 1), ethnic group (minorities = 1, majority [Han] = 0), marital status (married = 1, else = 0), living alone (Yes = 1), age (years), education level (primary or below vs. higher), duration of SCI (years), household income, subjective social status and province (Jiangsu = 0, Sichuan = 1) were used as control variables in our analysis. Those variables were chosen since participation is likely influenced by demographic factors and socioeconomic status. The total household income on average per month was classified by deciles of the Chinese Household Income Panel (CHIP). Subjective social status was described with the McArthur Scale of subjective social status, using a 10-rung ladder to visualize social position with 1 the lowest and 10 representing the highest subjective social status.Citation33
Sample size calculation
For each of the two participating Chinese Provinces sample size was calculated so that we would be able to detect a small to medium effect of Cohen's f = 0.15 when comparing four groups (complete tetraplegia, complete paraplegia, incomplete tetraplegia, incomplete paraplegia) with a power of 80% and an alpha error of 5%.Citation34 This yielded a minimum sample size of 492 for each Province.
Statistical analysis
Stata/MP 14.0 (College Station, Texas, USA) was used for data analysis. We report descriptive statistics for all variables. Since data showed an excess of zeros in the two count indices (24.65% for participation restrictions and 18.52% for environment barriers), zero-inflated Poisson (ZIP)Citation35,Citation36 regression was adopted in the analysis of determinants of environmental barriers and participation restrictions We estimated the effect of lesion characteristics (X) on participation restrictions (Y) and whether such effect was mediated by environmental barriers (M). Specifically, Baron and Kenny's four steps of mediation test was conductedCitation37: estimation of (1) the effect of X on Y, (2) the effect of X on M, (3) the effect of M on Y while controlling for X, and (4) the effect of X on Y while controlling for M. Under the following assumption mediation is present according to this approach: there is a significant effect of X and Y when M is not taken into account, there is significant effect of X on M, there is a significant effect of M on Y, and the effect of X on Y declines or disappears when M is taken into account.Citation37 We calculated unadjusted models and models adjusted for confounders comprising all control variables. In addition, additional ZIP regression analysis, unadjusted and adjusted for above given covariates, was conducted to further estimate which individual barriers mostly affect participation.
ZIP fitted the data better than regular Poisson regression (z = 8.75, P < 0.001) according to the Vuong test.Citation38 ZIP regression assumes that there are two processes underlying the data, one responsible for the inflated zeros, and one responsible for the actual count (including the zeros), e.g. people may not report problems in activities because they did not perform the respective activities or people may report no problems because they had no problem when performing the activity. The classic example for this is fishing. There are two possible reasons for not having caught any fish at the end of the day, you did not go fishing or you went fishing but did not catch any. It is easy to see that the processes and determinants involved in the decision to go fishing, are different from those leading to not catching fish while trying to do so. Therefore, ZIP simultaneously performs logistic and Poisson regression and makes two types of predictions: (1) prediction of the inflated zeros assuming a binary dependent variable (e.g. no participation restrictions = 1 versus experienced any problem = 0), and (2) prediction of the count portion (e.g. how many participation restrictions were experienced including those who did not experience any problem). For the inflated part of the model odds ratios (ORs) are reported with ORs < 1 indicating decreased odds of reporting no restriction or barrier, and ORs > 1 indicating increased odds of reporting no restriction or barrier (note that ORs have the opposite interpretation as in regular logistic regression). For the count part of the model Incidence Rate Ratios (IRRs) were reported. IRRs indicate the factor with which the expected count of the outcome is multiplied when the predictor variable increases by one unit.
Ethics approval
This study was registered with chictr.org.cn, number ChiCTR1800018559, and was approved by Ethics committees of the first affiliated hospital of Nanjing Medical University, Nanjing, Jiangsu Province (No.2018-SR-004) and West China Hospital, Chengdu, Sichuan Province (No.2017-469). The study was conducted according to the principles of the declaration of Helsinki. Informed consent was obtained from all participants. Participants were informed about the purpose of the research and could withdraw from the study at any time.
Results
Of the 1355 respondents, about two thirds were male and about three percent belonged to ethnic minority groups. A large majority of the participants was married, and about six percent lived alone. About 85% of the participants had less than high school education. The median age of the sample was 50 years with interquartile range (IQR) between 41 and 59, and the median length of time since injury was 4 years (IQR 2-5). About two thirds of the participants had paraplegia and a large majority had incomplete SCI. Participants experienced a median of 5 moderate to extreme participation restrictions and 5 environmental barriers. That means that at least half of the participants experienced 5 restrictions respectively 5 barriers or more ().
Table 1 Characteristics of participants (N = 1355).
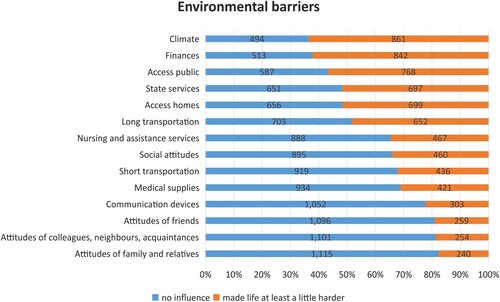
gives a detailed overview of experienced environmental barriers. More than sixty percent of the participants reported that their life was negatively influenced by climatic conditions (63.54%) and insufficient financial resources (62.14%), and more than half of the respondents experienced lack of or insufficient accessibility of public (56.68%) and private places (51.59%) and lack of or insufficient state services (51.71%).
Figure 2 Prevalence of perceiving environmental barriers (N = 1355).
Note: Blue and red bars indicate percentages, numbers inside bars indicate frequencies.
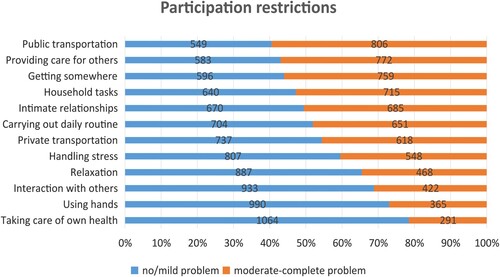
Participation restrictions () in the following areas were experienced by more than half of the sampled population: using public transportation (59.48%), providing care or support for others (56.97%), shortness of breath during physical exertion (56.68%), getting where one wants to go (56.01%), getting household tasks done (52.77%), and intimate relationships (50.55%).
Figure 3 Prevalence of experiencing participation restrictions (N = 1355).
Note: Blue and red bars indicate percentages, numbers inside bars indicate frequencies.
The results of the four steps ZIP regressions are shown in . Regarding the count portion, people with tetraplegia (unadjusted IRR = 1.10, 95% CI: 1.05–1.16; adjusted IRR = 1.15, 95% CI: 1.10–1.21) and those with complete lesions (unadjusted IRR = 1.47, 95% CI: 1.40–1.54; adjusted IRR = 1.42, 95% CI: 1.35–1.50) reported an increased number of participation restrictions in the models 1–3 of step 1 establishing the association of participation restrictions with lesion characteristics. In models 4 and 5 of step 2 both lesion level and completeness were significant predictors of environmental barriers, with people with paraplegia and those with complete lesions reporting more barriers. However, in the adjusted model 6 of step 2, only the association with lesion completeness remained statistically significant (IRR = 1.31, 95% CI: 1.24–1.38). In the models 7–8 of step 3 and 4 establishing mediation, all associations between lesion characteristics, environmental barriers and participation restrictions were significant. After adjustment for control variables (model 8), respondents with tetraplegia (IRR = 1.15, 95% CI: 1.10–1.21) and those with complete injury (IRR = 1.25, 95% CI: 1.18–1.31), and participants who perceived more environment barriers reported more participation restrictions. Specifically, a seven percent increase in participation restrictions per barrier was found (IRR = 1.07, 95% CI: 1.06–1.08), while the IRR for lesion completeness decreased as compared to the models of step 1 but remained significant.
Table 2 Four Steps Mediation Test based on ZIP Regressions (N = 1355).
In the inflated portion of the model, people with complete lesions (OR for fully adjusted model 8 = 0.36, 95% CI: 0.16–0.79) had lower odds of not experiencing participation restrictions; each reported environmental barrier reduced the probability of not reporting any participation restrictions by about 30% (OR for model 8 = 0.71, 95% CI: 0.66–0.77). Again, the effect size for complete lesions decreased when the model contained the effect of environmental barriers at the same time in models 7–8 of step 3–4.
Accordingly, based on the results of the three models 3, 6, and 8 adjusted for covariates representing steps 1–4 of Baron and Kenny's approach to test for mediation,Citation37 a partially mediating role in environmental barriers was confirmed for the association between completeness of SCI and participation restrictions:We found (1) a significant effect of degree of injury on participation restrictions without considering environmental barriers, (2) a significant effect of degree of injury on barriers, (3) a significant effect of environmental barriers on restrictions, and (4) a decline of the effect of degree of injury on restrictions when adjusting for barriers. However, again following Baron and Kenny,Citation37 environmental barriers did not mediate the relation between type of injury and participation restrictions due to the non-significant association of type of injury with environmental barriers in model 6 and lack of influence of adjustment for environmental barriers on the effect of type of SCI on participation restrictions when comparing models 3 and 8.
indicates the relations between specific environmental barriers and participation restrictions. Results from an unadjusted and an adjusted model were very similar with directions of effects pointing in the same direction in most of the cases. In the count portion, participants experiencing barriers with regard to accessing public places (adjusted IRR = 1.47, 95%CI = [1.33,1.62]), accessing homes (adjusted IRR = 1.32, 95%CI = [1.21,1.44]), long-distance transportation (IRR = 1.11, 95%CI = [1.04,1.20]), communication devices (adjusted IRR = 1.07, 95%CI = [1.01,1.15]) and state services (adjusted IRR = 1.10, 95%CI = [1.02,1.19]) reported a higher number of participation restrictions, while people who experienced barriers due to climatic conditions (adjusted IRR = 0.93, 95%CI = [0.88,0.99]) reported a lower number of participation restrictions. In the inflated portion, people experiencing barriers due to inaccessible public places (adjusted OR = 0.25, 95%CI = [0.09,0.67]) and long transportation (adjusted OR = 0.41, 95%CI = [0.17,0.96]) had lower odds of reporting zero participation restrictions, while those who reported barriers due to attitudes of acquaintances, colleagues, and neighbors had six times increased odds of not reporting any problems with participation (adjusted OR = 6.11, 95%CI = [1.44,25.91]).
Table 3 ZIP regression of Number of Participation Restrictions on Lesion Characteristics and Specific Environmental Barriers (N = 1348).
Discussion
This study provided an initial attempt to comprehensively describe the relationship among impairment, environmental barriers and participation restrictions in a community-dwelling population with SCI from two provinces in China. The study featured a large community sample that included people with traumatic and non-traumatic SCI. The survey respondents experienced a median of five environmental barriers and five participation restrictions. The most frequently reported barriers were due to problems with climatic conditions, finances, accessibility, and government services. In a qualitative study about people with SCI living in Mongolia the most frequently mentioned barriers were the lack of relevant medical resources such as inadequate health and rehabilitation services and lack of access to assistive devices and medicines due to financial limitations or legal issues.Citation14 Participation restrictions were frequently experienced in public transportation, providing care or support for others, getting where one wants to go, getting household tasks done, intimate relationships, and carrying out daily routine.
We found that respondents with complete SCI experienced more participation restrictions and environmental barriers than those with incomplete SCI, confirming previous research.Citation10,Citation39 This effect could be partially explained by an increased amount of environmental barriers reported by those with complete lesions. Fellinghauer et al.Citation40 also suggested that environmental barriers could be a mediator between impairment characteristics and participation restrictions. Targeting environmental barriers in a way that reduces them for groups with the most severe impairments may have a beneficial effect for all people with SCI. People with tetraplegia reported less environmental barriers (though this effect was not statistically significant) but more participation restrictions. The effect of tetraplegia on participation restrictions could not be explained by a mediating role of environmental barriers. One explanation may be the so called paradox of barriersCitation41,Citation42: people with tetraplegia may experience less environmental barriers then they would otherwise because their participation is restricted. When looking at the effect of individual barriers on reported participation restrictions, we found that lack of accessibility had the strongest influence followed by long distance transportation and insufficient state services. A surprising finding, however, was that reporting barriers due to climatic conditions was associated with less experienced participation restrictions when adjusting for the other barriers and demographic and injury characteristics. This again points to the so called paradox of barriers,Citation41,Citation42 i.e. only those who are less restricted in in outdoor activities will experience adverse climatic conditions. Another surprising finding was that people who reported attitudinal barriers with regard to acquaintances, colleagues, or neighbors had highly increased odds of reporting no participation restrictions at all. Again it is possible, that these people refrain from participation exactly because they anticipate negative attitudes and thus do not experience restrictions. This interpretation is somewhat supported when we look at the count portion of the model where the opposite (though not statistically significant) effect is observed, i.e. those who report barriers with regard to attitudes report more participation restrictions. Here the usefulness of ZIP regression becomes obvious: We observe two different processes: Those who experience (anticipate) barriers may be less prone to participating at all, but if they participate the experience of those barriers is possibly reinforced.
As a result of our findings, rehabilitation services for people with SCI in these areas should become more community-oriented and consider people's immediate environment and its effect on social participation. The problem needs also be brought to the attention of policy makers in order to better implement and enforce existing laws on accessibility and equal opportunities to participation.Citation43
Study limitations
Our study has several limitations. The cross-sectional design makes it impossible to draw causal conclusions and to model how participation restrictions interact with environmental barriers over time. Juvalta et al.Citation31 have for instance suggested that encountering barriers during unsuccessful attempts to participate in life situations may lead to avoidance of these situations over time. This may mean that people who attempt to participate may first perceive an increased amount of barriers which may later be reduced because their participation declines. It is not possible to determine if such process exists with the present data. The contact rate in this study was low which reduced the gross response rate. Hospitals do not regularly follow-up with patients and central registries are absent in China. Since the only way to initially contact patients was by telephone, people who had been hospitalized more recently could be better reached due to up to date telephone numbers. People with more recent SCI are thus overrepresented in the sample limiting generalizability. In addition, survival biasCitation44 is an issue that may have led to an underestimation of environmental barriers and participation restrictions. It is recommended to establish a stable spinal cord injury registry system in China which is regularly updated to support long-term follow-up. The study protocol further did not account for a distinction between urban and rural participants which is however important in many development issues in China and likely affects the experience of environmental barriers and participation restrictions. We used items from the WHO MDS to construct a count index for the number of moderate to extreme participation restrictions, assuming a cut-off in the middle of the items’ response scale for dichotomization. While this index showed good internal consistency, further metric properties need yet to be established and the strategy for dichotomization needs to be confirmed. Moreover, structural equation modeling (SEM) is preferable to test for mediation. However, ZIP regression is not readily implemented in SEM software. Therefore, the classic method proposed by Baron and Kenny was utilized here in spite of inherent limitations.Citation45 Finally, we studied mediation, i.e. the role environmental barriers play in the translation of impairment into restrictions, and did not account for a potential moderation of the effect of environmental barriers on participation by impairment, i.e. for those with more severe impairments environmental barriers may have a more pronounced effect on participation.
Conclusion
The people living with SCI in Jiangsu and Sichuan Province of China surveyed in this study experienced a significant amount of environmental barriers and participation restrictions. The effect of severity of impairment on participation restrictions was partially mediated by environmental barriers. It is hoped that this study will draw attention to the needs of people with SCI living in the community in China and help developing community-based health care and rehabilitation systems, services, and policies. Removing environmental barriers should be an important element in corresponding programs. Key issues that need addressing according to this study are community accessibility, transportation, government support systems, and financial protection.
Abbreviations
SCI Spinal cord injury
InSCI International Spinal Cord Injury Community Survey
ICF The International Classification of Functioning, Disability and Health
MDS The Model Disability Survey
NEFI-SF The Nottwil Environmental Factors Inventory-Short Form
CHIP The Chinese Household Income Panel
ZIP Zero-inflated Poisson
ORs Odds ratios
IRRs Incidence Rate Ratios
Disclaimer statements
Contributors None.
Conflicts of interest Authors have no conflict of interests to declare.
Ethnic approval This study is registered with chictr.org.cn, number ChiCTR1800018559, and was approved by Ethics committees of the first affiliated hospital of Nanjing Medical University, Nanjing, Jiangsu Province (No.2018-SR-004) and West China Hospital, Chengdu, Sichuan Province (No.2017-469). The study was conducted according to the principles of the declaration of Helsinki. Informed consent was obtained from all participants. Participants were informed about the purpose of the research and could withdraw from the study at any time.
Clinical Trial Number ChiCTR1800018559.
Acknowledgements
This study is based on data from the International Spinal Cord Injury (InSCI) Community Survey, providing the evidence for the Learning Health System for Spinal Cord Injury (LHS-SCI, see Am J Phys Med Rehabil 2017;96(Suppl):S23–34).The LHS-SCI is an effort to implement the recommendations described in the WHO report International Perspectives on Spinal Cord Injury (Bickenbach J et al. Geneva: WHO Press; 2013). The members of the InSCI Steering Committee are: Julia Patrick Engkasan (ISPRM representative; Malaysia), James Middleton (ISCoS representative; Member Scientific Committee; Australia), Gerold Stucki (Chair Scientific Committee; Switzerland), Mirjam Brach (Representative Coordinating Institute; Switzerland), Jerome Bickenbach (Member Scientific Committee; Switzerland), Christine Fekete (Member Scientific Committee; Switzerland), Christine Thyrian (Representative Study Center; Switzerland), Linamara Battistella (Brazil), Jianan Li (China), Brigitte Perrouin-Verbe (France), Christoph Gutenbrunner (Member Scientific Committee; Germany), Christina-Anastasia Rapidi (Greece), Luh Karunia Wahyuni (Indonesia), Mauro Zampolini (Italy), Eiichi Saitoh (Japan), Bum Suk Lee (Korea), Alvydas Juocevicius (Lithuania), Nazirah Hasnan (Malaysia), Abderrazak Hajjioui (Morocco), Marcel W.M. Post (Member Scientific Committee; The Netherlands), Johan K. Stanghelle (Norway), Piotr Tederko (Poland), Daiana Popa (Romania), Conran Joseph (South Africa), Mercè Avellanet (Spain), Michael Baumberger (Switzerland), Apichana Kovindha (Thailand), Reuben Escorpizo (Member Scientific Committee; USA). We would further like to acknowledge the continuous support of Prof. Gretchen Kalonji, Dean of the Institute for Disaster Management and Reconstruction at Sichuan University.
Additional information
Funding
References
- World Health Organization (WHO). Fact sheets: spinal cord injury. September 19, 2013. Available at: https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury.
- World Health Organization (WHO). World Report on Disability. Geneva: WHO Press; 2011.
- World Health Organization (WHO). International Perspectives on Spinal Cord Injury. Geneva: WHO Press; 2013.
- Divanoglou A, Augutis M, Sveinsson T, Hultling C, Levi R. Self-reported health problems and prioritized goals in community-dwelling individuals with spinal cord injury in Sweden. J Rehabil Med. 2018;50(10):872–8.
- Kashif M, Jones S, Darain H, Iram H, Raqib A, Butt AA. Factors influencing the community integration of patients following traumatic spinal cord injury: a systematic review. J Pak Med Assoc. 2019;69(9):1337–43.
- Cobb JE, Leblond J, Dumont FS, Noreau L. Perceived influence of intrinsic/extrinsic factors on participation in life activities after spinal cord injury. Disabil Health J. 2018;11(4):583–90.
- Wang Y, Zhao X, Xie H. Quality of life and its predictors in people with traumatic spinal cord injury in mainland China. Spinal Cord. 2019;57(9):739–46.
- Norin L, Slaug B, Haak M, Jorgensen S, Lexell J, Iwarsson S. Housing accessibility and its associations with participation among older adults living with long-standing spinal cord injury. J Spinal Cord Med. 2017;40(2):230–40.
- Barclay L, McDonald R, Lentin P, Bourke-Taylor H. Facilitators and barriers to social and community participation following spinal cord injury. Aust Occup Ther J. 2016;63(1):19–28.
- Reinhardt JD, Ballert C, Brinkhof MW, Post MW. Perceived impact of environmental barriers on participation among people living with spinal cord injury in Switzerland. J Rehabil Med. 2016;48(2):210–8.
- Tsai IH, Graves DE, Chan W, Darkoh C, Lee MS, Pompeii LA. Environmental barriers and social participation in individuals with spinal cord injury. Rehabil Psychol. 2017;62(1):36–44.
- Smith EM, Sakakibara BM, Miller WC. A review of factors influencing participation in social and community activities for wheelchair users. Disability Rehabil Assistive Technol. 2016;11(5):361–74.
- Hanapi NHM, Zainin ES, Aziz MHA, Darus D. The impact of personal and environmental factors on the rehabilitation of persons with neglected spinal cord injury in Malaysia. Spinal Cord Series Cases. 2019;5:10.
- Dorjbal D, Prodinger B, Zanini C, Avirmed B, Stucki G, Rubinelli S. Living with spinal cord injury in Mongolia: a qualitative study on perceived environmental barriers. J Spinal Cord Med. 2020;43(4):518–31.
- Reinhardt JD, Mansmann U, Fellinghauer BA, Strobl R, Grill E, von Elm E, et al. Functioning and disability in people living with spinal cord injury in high- and low-resourced countries: a comparative analysis of 14 countries. Int J Public Health. 2011;56(3):341–52.
- Reinhardt JD, Middleton J, Bokel A, Kovindha A, Kyriakides A, Hajjioui A, et al. Environmental barriers experienced by people With spinal cord injury across 22 countries: results from a cross-sectional survey. Arch Phys Med Rehabil. 2020;101(12):2144–56.
- Xu M, Li H, Zhao Z, Yang Y, Sun Z, Han H, et al. Environmental barriers, functioning and quality of life in 2008 Wenchuan earthquake victims with spinal cord injury eight years after the disaster: A cross-sectional study. J Rehabil Med. 2018;50(10):866–71.
- Reinhardt JD, Zheng Y, Xu G, Lu X, Yin Y, Liu S, et al. People with spinal cord injury in China. Am J Phys Med Rehabil. 2017;96(2 Suppl. 1):S61–S5.
- Gross-Hemmi MH, Post MW, Ehrmann C, Fekete C, Hasnan N, Middleton JW, et al. Study protocol of the International Spinal Cord Injury (InSCI) community survey. Am J Phys Med Rehabil. 2017;96(2 Suppl. 1):S23–S34.
- Rimmer JH. Use of the ICF in identifying factors that impact participation in physical activity/rehabilitation among people with disabilities. Disabil Rehabil. 2006;28(17):1087–95.
- World Health Organization (WHO). International Classification of Functioning, Disability and Health. Geneva: WHO Press; 2001.
- Yeung P, Towers A. An exploratory study examining the relationships between the personal, environmental and activity participation variables and quality of life among young adults with disabilities. Disabil Rehabil. 2014;36(1):63–73.
- Cieza A. The International Spinal Cord Injury Survey and the learning health system for spinal cord injury. Am J Phys Med Rehabil. 2017;96(2 Suppl. 1):S1.
- Stucki G, Bickenbach J. The International Spinal Cord Injury Survey and the learning health system for spinal cord injury. Am J Phys Med Rehabil. 2017;96(2 Suppl. 1):S2–4.
- Stucki G, Bickenbach J. The implementation challenge and the learning health system for SCI initiative. Am J Phys Med Rehabil. 2017;96(2 Suppl. 1):S55–60.
- Fekete C, Brach M, Ehrmann C, Post MWM, Stucki G. Cohort profile of the International Spinal Cord Injury (InSCI) community survey implemented in 22 countries. Arch Phys Med Rehabil. 2020;101(12):2103–11.
- Fekete C, Post MW, Bickenbach J, Middleton J, Prodinger B, Selb M, et al. A structured approach to capture the lived experience of spinal cord injury: data model and questionnaire of the International Spinal Cord Injury Community survey. Am J Phys Med Rehabil. 2017;96(2 Suppl. 1):S5–16.
- The World Bank: Model Disability Survey. World Health Organization, 2016.
- World Health Organization (WHO). Model Disability Survey: Providing evidence for accountability and decision-making. 2014. Available at: https://www.who.int/disabilities/data/mds_v4.pdf.
- Ballert CS, Post MW, Brinkhof MW, Reinhardt JD, Swi SCISG. Psychometric properties of the Nottwil Environmental Factors Inventory Short form. Arch Phys Med Rehabil. 2015;96(2):233–40.
- Juvalta S, Post MW, Charlifue S, Noreau L, Whiteneck G, Dumont FS, et al. Development and cognitive testing of the Nottwil Environmental Factors Inventory in Canada, Switzerland and the USA. J Rehabil Med. 2015;47(7):618–25.
- Reinhardt JD, Zhang X, Van Dyke C, Ehrmann C, Li L, Zhao Z, et al. Post-traumatic stress disorder in a population of 2008 Wenchuan earthquake survivors with disabilities: the role of environmental barriers. Disabil Rehabil. 2020:1–9. doi:10.1080/09638288.2020.1714756.
- Ballert CS, Adler NE, Kawachi I, Frazier AL, Huang B, Colditz GA. Adolescents’ perceptions of social status: development and evaluation of a new indicator. Pediatrics. 2001;108:E31.
- Cohen J. The Statistical Power Analysis for the Behavioral Sciences, 2nd ed. New York: Taylor & Francis Group; 1988.
- Lambert DJT. Zero-inflated poisson regression, with an application to defects in manufacturing. Technometrics. 1992;34(1):1–14.
- Famoye F, Singh K. Zero-inflated generalized poisson regression model with an application to domestic violence data. J Data Sci. 2006;4(1):117–30.
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
- Ridout M, Hinde J, Demetrio CG. A score test for testing a zero-inflated poisson regression model against zero-inflated negative binomial alternatives. Biometrics. 2001;57(1):219–23.
- Ripat JD, Woodgate RL. Self-perceived participation among adults with spinal cord injury: a grounded theory study. Spinal Cord. 2012;50(12):908–14.
- Fellinghauer B, Reinhardt JD, Stucki G, Bickenbach J. Explaining the disability paradox: a cross-sectional analysis of the Swiss general population. BMC Public Health. 2012;12:655.
- Magasi S, Wong A, Gray DB, Hammel J, Baum C, Wang CC, et al. Theoretical foundations for the measurement of environmental factors and their impact on participation among people with disabilities. Arch Phys Med Rehabil. 2015;96(4):569–77.
- Whiteneck G, Dijkers MP. Difficult to measure constructs: conceptual and methodological issues concerning participation and environmental factors. Arch Phys Med Rehabil. 2009;90(11 Suppl.):S22–35.
- Law of the People's Republic of China on the protection of people with disabilities. Labor security in China, 2008. (7): p. 53–6.
- Oderud T. Surviving spinal cord injury in low income countries. African J Disability. 2014;3(2):80.
- Hayes AF. Beyond Baron and Kenny: statistical mediation analysis in the new millennium. Commun Monogr. 2009;76(4):408–20.
Appendix 1:
Search terms for initial identification of patients with SCI from hospital records
1. Hanyu (simplified Chinese) characters for free text search in fields diagnosis, complications, etc.
脊髓
OR 脊神经
OR 截瘫
OR 四肢瘫
OR 马尾
OR 椎管内
OR [脊柱 AND [骨折 OR 破裂 OR 扭伤 OR 脱位 OR 挤压伤 OR 震荡 OR 水肿]]
OR [颈 AND [骨折 OR 破裂 OR 扭伤 OR 脱位 OR 挤压伤 OR 震荡 OR 水肿]]
OR [胸 AND [骨折 OR 破裂 OR 扭伤 OR 脱位 OR 挤压伤 OR 震荡 OR 水肿]]
OR [腰 AND [骨折 OR 破裂 OR 扭伤 OR 脱位 OR 挤压伤 OR 震荡 OR 水肿]]
OR [下背 AND [骨折 OR 破裂 OR 扭伤 OR 脱位 OR 挤压伤 OR 震荡 OR 水肿]]
OR [骶椎 AND [骨折 OR 破裂 OR 扭伤 OR 脱位 OR 挤压伤 OR 震荡 OR 水肿]]
2. ICD codes with definitions in English and Chinese
C72 脊髓、颅神经及中枢其他部位的恶性肿瘤
OR C72.0Spinal cord 脊髓恶性肿瘤
OR C72.1Cauda equina 马尾恶性肿瘤
OR D33.4Spinal cord 脊髓良性肿瘤
OR G04Encephalitis, myelitis and encephalomyelitis脑炎、脊髓炎、脑脊髓炎
OR G05*Encephalitis, myelitis and encephalomyelitis in diseases classified elsewhere脑炎、脊髓炎和脑脊髓炎
OR G06.1Intraspinal abscess and granuloma椎管内脓肿
OR G37.3Acute transverse myelitis in demyelinating disease of central nervous system 中枢神经系统脱髓鞘病的急性横贯性脊髓炎
OR G37.4Subacute necrotizing myelitis亚急性坏死性脊髓炎
OR 或者G82.0,Flaccid paraplegia 迟缓性截瘫
OR 或者G82.1 Spastic paraplegia 痉挛性截瘫
OR 或者G82.2 Paraplegia, unspecified 截瘫,未特指
OR 或者G82.3 Flaccid tetraplegia 迟缓性四肢瘫痪
OR 或者G82.4 Spastic tetraplegia 痉挛性四肢瘫痪
OR 或者G82.5 Tetraplegia, unspecified四肢瘫,未特指
G95Other diseases of spinal cord 脊髓的其他疾病
G95.0Syringomyelia and syringobulbia 脊髓空洞症
G95.1Vascular myelopathies 血管性脊髓病
G95.2Cord compression, unspecified 脊髓受压,未特指
G95.8Other specified diseases of spinal cord 脊髓特指疾病
G95.9Disease of spinal cord, unspecified 脊髓病,未特指
M47.1Other spondylosis with myelopathy特指脊椎关节强硬伴脊髓病
OR 或者S12 Fracture of the neck颈部骨折
OR 或者S12.0 Fracture of first cervical vertebra第一颈椎骨折
OR 或者S12.2 Fracture of other specified cervical vertebra 其他特指颈椎骨折
OR 或者S13.0 Traumatic rupture of cervical intervertebral disk 颈部椎间盘创伤性破裂
OR或者S13.2 Dislocation of other and unspecified parts of neck 颈部其他未特指部位脱位
OR 或者S13.4 Sprain and strain of cervical spine 颈椎扭伤拉伤
OR 或者S14 Injury of nerves and spinal cord at neck level 颈部神经损伤和脊髓损伤
OR 或者S14.0 Concussion and edema of cervical spinal cord 颈部脊髓的震荡和水肿
OR 或者S14.1 Other and unspecified injuries of cervical spinal cord 其他未特指颈脊髓损伤
OR 或者S17 Crushing injury of neck颈部挤压伤
OR 或者S19 Other and unspecified injuries of neck 其他未特指颈部损伤
OR 或者S22 Fracture of rib(s), sternum and thoracic spine 肋骨、胸骨以及胸椎骨折,
OR 或者S22.0 Fracture of thoracic vertebra 胸椎骨折
OR 或者S23.1 Dislocation of thoracic vertebra胸椎脱位
OR 或者S24 Injury of nerves and spinal cord at thorax level 胸部神经损伤和脊髓损伤
OR 或者S24.0 Concussion and edema of thoracic spinal cord胸部脊髓的震荡和水肿
OR或者S24.1 Other and unspecified injuries of thoracic spinal cord 其他未特指的胸部脊髓损伤
OR 或者S28 Crushing injury of thorax and traumatic amputation of part of thorax胸部挤压伤,胸的部分创伤性切断
OR 或者S29 Other and unspecified injuries of thorax胸部其他未特指损伤
OR 或者S32 Fracture of lumbar spine and pelvis 腰椎和骨盆骨折
OR 或者S32.0 Fracture of lumbar vertebra 腰椎骨折
OR 或者S33.1 Dislocation of lumbar vertebra 腰椎脱位
OR 或者S34.0 Concussion and edema of lumbar spinal cord腰部脊椎的震荡和水肿
OR 或者S34.1 Other injury of lumbar spinal cord其他腰部脊髓损伤
OR 或者S34.3 Injury of cauda equine马尾损伤
OR 或者S38 Crushing injury and traumatic amputation of part of abdomen, lower back and pelvis腹部、下背以及骨盆部分挤压伤、外伤性截肢
OR 或者S39 Other and unspecified injuries of abdomen, lower back and pelvis腹部、下背和骨盆其他未特指部位的损伤
OR 或者T02.0 Fractures involving head with neck头和颈的骨折
OR 或者T02.1 Fractures involving thorax with lower back and pelvis 胸伴下背和骨盆的骨折
OR 或者T04.1 Crushing injuries involving thorax with abdomen, lower back and pelvis 胸伴有腹、下背和骨盆的挤压伤
OR 或者T04.2 Crushing injuries involving multiple regions of upper limb(s)上肢多个部位挤压伤
OR 或者T06.0 Injuries of brain and cranial nerves with injuries of nerves and spinal cord at neck level 脑和颅神经损伤,伴有颈水平的神经和脊髓损伤
OR 或者T06.1 Injuries of nerves and spinal cord involving other multiple body regions 身体其他多个部位的神经和脊髓损伤
OR 或者T09.3 Injury of spinal cord, level unspecified脊髓损伤,未特指水平
OR 或者T09.4 Injury of unspecified nerve, spinal nerve root and plexus of trunk 未特指神经伤,脊神经根和神经丛的损伤
OR 或者T91.1Sequelae of fracture of spine 脊柱骨折后遗症
OR 或者T91.3 Sequelae of injury of spinal cord 脊髓损伤后遗症