
Abstract
Ectodermal dysplasia (ED) consists of many different combinations of irregularities that include developmental defects that occur in two or more of the following tissues: teeth, nails, skin, hair and sweat glands. The aim of this study was to evaluate the possible carries risk, perform scanning electron microscopy (SEM) mineral analysis in ectodermal dysplasia cases and describe the oral aspects. Ectodermal dysplasia cases, 41 patients (22 males and 19 females, aged 1.5 to 45 years), had a clinical examination. SEM analyses were performed from teeth that had to be extracted from ED cases for various reasons. Forty-one patients had tooth agenesis (from hypodontia to anodontia), multiple caries, hair and nail dystrophy. Also, extra orally they had sparse or absent hair, a short face, an unusual facial concavity, maxillary retrusion and relative mandibular protrusion. Differences between tooth samples were determined by SEM analyses. SEM analyses showed that the mineral content of ED teeth was lower than that of normal teeth and the surface properties of dentin and enamel were different. It is necessarily to support this observation with more comprehensive research. When dentists examine ED patients, they should consider the oral mucosa for excessive dryness and increased dental caries and should conduct a comprehensive, multidisciplinary approach to these patients in order to improve their dental, masticatory and caries conditions.
Keywords:
Introduction
Ectodermal dysplasias (ED) are a large complex group of genetic disorders. The characteristic features affect the ectodermal structures, including the central nervous system, peripheral nervous system, teeth, skin, nails, sweat glands and hair. The most common form of ectodermal dysplasia, previously referred to as Christ–Siemens–Touraine syndrome, is inherited as an X-linked condition. It is caused by mutations in the EDA gene located at Xq13.1. The EDA gene codes for the ectodysplasin protein, a critical signaling unit involved in the interaction between the ectoderm and the mesoderm [Citation1–6].
ED cases exhibit the following clinical signs: hypotrichosis, hypohidrosis (characterized by reduced sweating ability and/or a reduced sweat duct count), and cranial abnormalities. The face is usually smaller than normal because of frontal bossing, with a depressed nasal bridge. Patients have smooth dry skin and/or hyperkeratosis of hands and feet. Oral traits include anodontia, hypodontia, a wide range of tooth anomalies, reduced tooth size and conical or peg-shaped teeth. Anodontia also manifests itself by a lack of alveolar ridge development [Citation1,Citation3,Citation6–8].
The earliest records of ED cases date back to 1792 (1). Since then, more than 170–200 different pathologic clinical conditions have been recognized and defined as ED. These disorders are relatively rare, 1 in 10,000 to 1 in 100,000 births [Citation1–4,Citation6,Citation7,Citation9–11].
Oral signs and symptoms are often seen in rare disorders and can be significant clues in establishing a diagnosis [Citation12].
Early detection is important for individual symptom management and for prevention of morbidity and mortality associated with hypohidrosis [Citation1]. Early diagnosis is also important in family planning counseling, particularly with clinical trials working toward successful treatment of ED. The literature has demonstrated the benefits that corrective dentistry and medical management have for the self-esteem, comfort and social well-being of these cases [Citation1,Citation6].
The periodontal problems in ED patients mostly result from decreased salivary secretion. Excellent oral hygiene is very important for the successful treatment of these patients. Mechanical obstructions, such as gingival fibrosis and tooth compression as a result of malocclusion, may also delay the eruption of teeth [Citation13].
Most ED cases have a normal intelligence and normal life expectancy, so ED cases were clinically examined according to their age and anomaly status, and all caries teeth were treated.
The aim of this study was to evaluate the possible carries risk, perform scanning electron microscopy (SEM) mineral analysis in ectodermal dysplasia cases, and describe and summarize the oral aspects in ED. The study focused on the dental manifestations that can be crucial for diagnosis of ED among individuals with abnormalities in number, size and shape of teeth, and reduced salivary secretion, possible carries risk, SEM mineral analysis and surface properties of dentin and enamel in ectodermal dysplasia cases.
Subjects and methods
Ethics statement
Approval for this study was given by the Harran University Clinical Research Ethics Committee (decision no: HRU/21.17.21).
Subjects
This retrospective/prospective study was carried out on all the ED cases from 1997 to 2021 in South-East of Turkey. A total of 41 cases (22 males and 19 females, aged from 1.5 to 45 years) with a diagnosis of ED were included.
Clinical examination
All dental signs of ED were studied. Every patient had a rigorous clinical examination for diagnosis and caries therapy: minor or major abnormalities had to be detected in cases. Examination included the caries status, teeth capital, teeth shape abnormalities, skull, face, hair, nails, skin, sweat glands, etc.
Microscopy and analytical analysis
ED cases had a clinical examination. Analyses were performed on teeth that had to be extracted from ED cases for various reasons. Scanning electron microscopy (SEM) was performed using an FEI Quanta 250 FEG field scanning microscope. Differential Scanning Calorimetry (DSC) data were collected on a SHIMADZU DSC-60 Differential Scanning Calorimeter under N2 atmosphere.
Comparisons were made between ED and healthy groups by using the obtained SEM images and mineral amounts measurements. SEM analyses were performed by SEM-EDX (Energy Dispersive X-Ray).
Data analysis
The data obtained were assessed with frequency analysis using SPSS v. 17.0.
Results
Forty-one cases (22 males and 19 females, aged from 1.5 to 45 years) had tooth agenesis (all cases: from hypodontia to anodontia), caries experiences, hypohidrosis and decreased saliva from moderate to severe. With respect to sex differentiation, there was no differentiation between the two sexes. Some of the cases were related to each other and they had similar features of ED in their parents. The findings of ED cases who participated in the study are shown in .
Table 1. Findings of ectodermal dysplasia cases participating in the study.
Overall, 41 cases had hypodontia; 15 cases were with fewer than 10 teeth, and 26 cases with more than 10 teeth.
Clinical view of increased number of dental caries, missing teeth and shape anomalies in ED cases is shown in –c.
Figure 1. (a,b,c) Increasing number of teeth with caries, missing teeth and shape anomalies in ED cases.

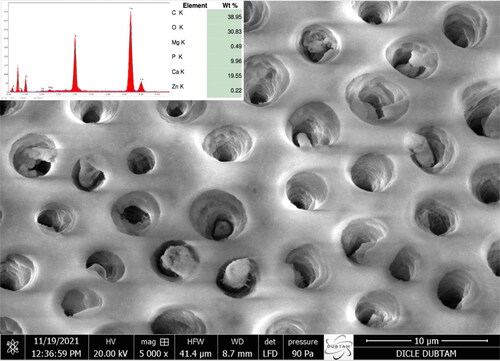
The results from the SEM and mineral analyses are shown in . As a control for enamel structure and mineral analysis, a normal healthy case was enrolled (). shows the appearance of the dentin canals (3 µm − 4 µm) and dentin mineral measurements in the normal healthy case. presents the appearance of irregular enamel prisms and enamel mineral measurements in an ectodermal case. illustrates the appearance of the large formed dentin canals (4 µm − 5 µm) and dentin mineral measurements in an ectodermal dysplasia case.
Figure 2. Appearance of enamel prisms and enamel mineral measurements in a normal healthy case as a control case.
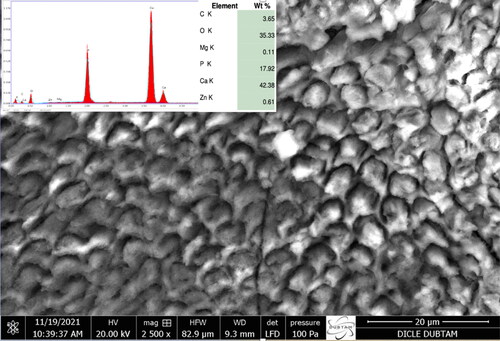
Figure 3. Appearance of dentin canals (3 µm – 4 µm) and dentin mineral measurements in the dentin of a normal healthy case.
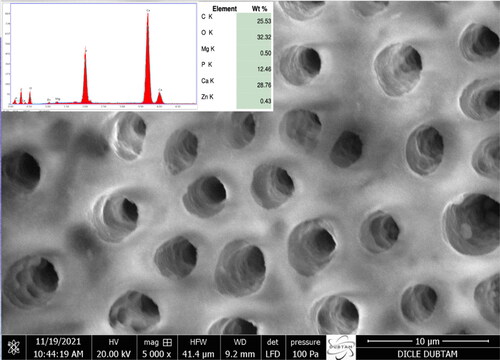
Figure 4. Appearance of irregular enamel prisms and enamel mineral measurements in an ectodermal case.
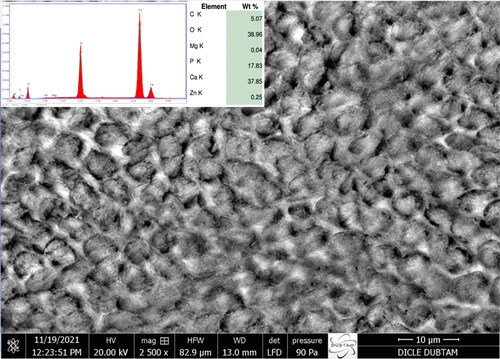
Figure 5. Appearance of large formed dentin canals (4 µm – 5 µm) and dentin mineral measurements in an ectodermal dysplasia case.
Discussion
Disturbances in tooth development – such as tooth agenesis, variations in size and shape of teeth, defects in the mineralized tissues, and problems in the number, size and shape of teeth, and reduced low salivary secretion – can compromise tooth health, chewing, swallowing and speech [Citation1–8,Citation12–14].
The most common form of ED, X-linked hypohidrotic ED (HED, involves defects in teeth, sweat glands and hair. A few reports have associated HED with dramatically reduced salivary fluid. Computed tomography indicates that submandibular gland and parotid glands are hypoplastic, whereas the right submandibular gland seems to be absent [Citation15]. These observations are in agreement with a general developmental disturbance that also involves the salivary glands [Citation5,Citation15].
We support the suggestion that dentists should evaluate the salivary secretion in persons with ED routinely, to prevent a possible negative impact on oral health in an early stage [Citation15].
ED is a rare, inherited, complex multi-system disorder. In some of our patients, there was parental consanguinity (26 patients). In these cases, the features of ED were similar in the parents, confirming the hereditary nature of ED.
Diagnosis of ED is difficult because the identification of the precise type of disorder could be a challenge [Citation16,Citation17]. Correct diagnosis requires the collaboration of medical specialists with different specialties.
Typically ED affects the hair, teeth, nails and/or skin. Some primary characteristics of ED include: partial or complete absence of some sweat glands (eccrine glands), resulting in anhidrosis or hypohidrosis (37 out of 41 patients in this study); heat intolerance and fever; hypotrichosis, and hypodontia (41/41, all patients). Certain facial abnormalities are also characteristic of ED, for example, a prominent forehead, sunken nasal bridge (saddle nose), unusually thick lips, and/or large chin [Citation3,Citation4,Citation8,Citation13,Citation16–20]. This study agrees with past research.
Here we report 41 cases and all of them had hypodontia; 15 cases were with fewer than 10 teeth, and 36 patients with more than 10 teeth. This observation is consistent with other reports [Citation6,Citation13,Citation21,Citation22]. For example, Till and Marques [Citation21] similarly reported that approximately 25% of HED patients present anodontia, whereas 75% present oligodontia.
A published study reported that submandibular and/or parotid salivary gland parameters were correlated with quantitative and qualitative salivary secretion in the ED group, with low unstimulated and/or chewing-stimulated full salivary flow being significantly reduced [Citation23].
Patients with dry mouth for different reasons are at higher risk of developing caries due to loss of saliva and lack of its benefits. The development of caries is attributed to various reasons such as loss of saliva, proliferation of acid-producing bacteria, lack of buffering of the acid from the bacteria or from the food, insufficient demineralization and remineralization from the tooth surfaces and increased oral acidity [Citation24]. In addition, caries control will be inadequate due to the lack of saliva and loss of many useful functions of saliva [Citation24]. This report describes the increased number of caries formation in ED cases where salivary secretion is reduced and mineral measurement percentages are low.
Another study emphasized that the secretion rate and quality of saliva is important not only for caries development but also for remineralization [Citation25]. Since saliva provides a general protective effect, clinically significant decrease in salivary functions can be considered as an etiologic factor [Citation25].
Affected infants and children often have hypoplasia or aplasia of mucous glands within the respiratory tract and, sometimes, decreased lung capacity and function, potentially causing an increased susceptibility to teeth caries [Citation6]. Many ED patients experience multiple caries, recurrent attacks of wheezing and breathlessness (asthma) and respiratory infections. Our study suggested that caries susceptibility in ED cases was most probably due to low saliva secretion and relative lack of buffering capacity, as some of studies have reported before [Citation6,Citation24,Citation26,Citation27].
Increasing the salivary flow rate is of high importance in individuals with low salivation and dry mouth. Product studies related to this have been carried out [Citation26,Citation27].
Accumulating data about the inheritance patterns of ED indicate that it is usually an X-linked recessive trait. Thus, there is full expression of ED in males only. Females who are heterozygote carriers may have some of the characteristic signs and findings of this disorder. There are also some case reports of ED inheritance as an autosomal recessive genetic trait. In such cases, ED signs are fully expressed in both males and females [Citation6,Citation19,Citation20].
Molecular genetic analysis has identified the causative gene in only a limited number of ED cases. Of all the ED cases reported so far, fewer than 30 have received molecular genetic explanation. ED may be inherited by autosomal-dominant, autosomal-recessive or x-linked genetic transmission [Citation3,Citation4,Citation6,Citation7].
Based on the current knowledge about the molecular basis and biological functions of ED, Priolo and Lagana [Citation10] proposed a new classification that combines both molecular-genetic data and relevant clinical findings. They propose two distinct groups, each likely to result from mutations in genes with similar functions and possibly sharing the same developmental and/or pathogenesis pathway [Citation10]. This understanding allows clinicians to redefine ED, not simply as a result of general ‘ectodermal’ abnormal development, but more precisely as systemic pathological conditions [Citation6]. To date, however, the diagnosis of ED is still difficult because it involves specific molecular and biochemical background, with a scientific multidisciplinary approach and specialized equipment.
The participants in this study were referred to a restorative dentistry specialist for caries management, prosthetist, orthodontist and pedodontist according to their clinical findings and age. Treatment plans were made with a multidisciplinary approach, and regular visits to a dental specialist were recommended.
Usually, permanent teeth in children become visible on x-rays around the age of 5 years. Reportedly, late mineralization of teeth is associated with oligodontia, so it is possible that the number of missing teeth in young participants in the studies was not seen on X-rays and was overestimated [Citation6].
We found multiple dental caries, odontodysplasia, partial anodontia, microdontia, and enamel hypoplasia in the studied patients.
In a study, dental implants were combined with retaining teeth and telescopic partial removable dentures. The strategy used with soft tissue grafting to increase vestibular depth and keratinized gingival width was stable for 2 years and provided patient satisfaction [Citation29].
A research reported that the presence of a high-density dental material in digital radiographic systems can be calculated by adjusting dental tissue-equivalent grey values [Citation30]. Therefore, using Hu scale, the differentiation can show in clinical manifestations [Citation31]. This prompted us to perform comparisons between ED and healthy groups by using SEM images and mineral content measurements.
The percentages of mineral measurement values obtained from the enamel and dentin of a healthy case and an ED case were compared. The enamel and dentin mineral percentages of the ED case were lower than the values obtained from the teeth of the healthy case. This was thought to be the reason why more caries occurred in ED cases than in the control group.
In SEM image examinations, enamel prisms were observed irregularly on the tooth enamel surfaces of the ED case (), and the dentin canals were wider (4 µm − 5 µm) when compared to the dentin canals of the healthy case (3 µm − 4 µm) (). We believe that the presence of these wider dentin canals, microorganisms and harmful wastes in ED cases could progress through the dentin tissue and reach the pulp more easily than in the control group, thus causing more caries.
All ED patients were referred for treatment and management of the oral findings. There was low mineralization of teeth in patients affected by ED and susceptibility to dental caries.
We believe that future research should be conducted to elucidate dry mouth, tooth mineralization percentages, enamel surface structures, structure of dentin canals, and their relationship with carious teeth and oral health in ED.
Conclusions
When faced with more than one dental agenesis, the dentist should look for a relationship with the patient’s ED findings, as an undiagnosed case of ED may be detected. Dental treatments can help patients achieve optimal oral and dental health, chewing and speaking function, so that ED cases have the opportunity to develop physically, emotionally and socially like other healthy individuals. This paper stepped on the current knowledge of oral manifestations in ED, and focused on the dental manifestations for diagnosis of ED among individuals with abnormalities in number, size, shape of teeth, and reduced salivary secretion, possible carries risk, SEM mineral analysis in ectodermal dysplasia cases. Excellent oral hygiene is very important for the successful treatment of these patients. Dentists should perform preventive dental measures and fluoride prophylaxis against new caries attacks. In our opinion, dentists and parents should be aware of possible tooth loss and the necessity of preserving existing teeth. Overall, the data we obtained in our study indicate that the high number of decayed teeth in ectodermal dysplasia cases, dry mouth, the irregularity of the enamel prisms, the wider dentin canals and the low percentage of mineral measurement values obtained from enamel and dentin likely play an important role. We suggest that future research will be beneficial to improve the knowledge about the tooth mineralization structures, caries and oral health.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement (DAS)
Data are available upon reasonable request due to privacy if necessary.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
References
- Anbouba G, Carmany E, Natoli J. The characterization of hypodontia, hypohidrosis, and hypotrichosis associated with X-linked hypohidrotic ectodermal dysplasia: a systematic review. Am J Med Genet A. 2020;182A:(4):831–841.
- Swathi G, Ramesh T, Sravani KB. Ectodermal dysplasia-a report of two cases. Ind J Clin Dent. 2020;1(1):10–13.
- Abadi B, Herren C. Clinical treatment of ectodermal dysplasia: a case report. Quintessence Int. 2001;32(9):743–745.
- Lamartine J. Towards a new classification of ectodermal dysplasias. Clin Exp Dermatol. 2003;28(4):351–354.
- Mohan N, K Rathore P. Ectodermal dysplasia with classical clinical presentation: a rare case report. JDPO. 2020;5(4):441–445.
- Yavuz I, Baskan Z, Ulku R, et al. Ectodermal dysplasia: retrospective study of fifteen cases. Arch Med Res. 2006;37(3):403–409.
- Priolo M, Silengo M, Lerone M, et al. Ectodermal dysplasias: not only ‘skin’ deep. Clin Genet. 2000;58(6):415–430.
- Geza T, William S, Samir A. Ectodermal dysplasia. Qintessence Int. 2003;34:482–483.
- Buyse M. Birth defects encyclopedia. Vol. I. USA: Blackwell Scientific Publications Inc, 1990.
- Priolo M, Lagana C. Ectodermal dysplasias: a new clinical-genetic classification. J Med Genet. 2001;38(9):579–585.
- García-Martín P, Hernández-Martín A, Torrelo A. Ectodermal dysplasias: a clinical and molecular review. Actas Dermosifiliogr. 2013;104(6):451–470.
- Bergendal B. Orodental manifestations in ectodermal dysplasia-a review. Am J Med Genet A. 2014;164A(10):2465–2471.
- Esen İ, Çay ÖÖ. Hipohidrotik ektodermal displazi: Olgu sunumu. Fırat Tıp Derg/Firat Med J. 2015;20(2):116–118.
- Altun S, Altun SE, Yavuz I, et al. Ectodermal displasia: Report of 3 cases. T Klin J Dental Sci. 2001;7:154–160.
- Nordgarden H, Johannessen S, Storhaug K, et al. Salivary gland involvement in hypohidrotic ectodermal dysplasia. Oral Dis. 1998;4(2):152–154.
- Pinheiro M, Freire-Maia N. Ectodermal dysplasias: a clinical classification and a causal review. Am J Med Genet. 1994;53(2):153–162.
- Ruhin B, Martinot V, Lafforgue P, et al. Pure ectodermal dysplasia: Retrospective study of 16 cases and literature review. Cleft Palate-Craniof J. 2001;38(5):504–518.
- Vieruci S, Baccetti T, Tollaro I. Dental and craniofacial findings in hypohidrotic ectodermal displasias during the primary dentition phase. J Clin Pediatr Dent. 1994;18:291–297.
- Hypohidrotic Ectodermal Dysplasia. Available from: http://www.peacehealth.org/kbase/nord/nord804.htm.
- Al-Ghamdi K, Crawford PJM. Focal dermal hypoplasia – oral and dental findings. Int J Paed Dent. 2003;13(2):121–126.
- Till MJ, Marques AP. Ectodermal dysplasia: treatment considerations and case reports. Northwest Dent. 1992;14:99–109.
- Nordgarden H, Jensen JL, Storhaug K. Oligodontia is associated with extra-oral ectodermal symptoms and low whole salivary flow rates. Oral Dis. 2001;7(4):226–232.
- Nordgarden H, Storhaug K, Lyngstadaas SP, et al. Salivary gland function in persons with ectodermal dysplasias. Eur J Oral Sci. 2003;111(5):371–376.
- Su N, Marek CL, Ching V, et al. Caries prevention for patients with dry mouth. J Can Dent Assoc. 2011;77:b85.
- Gopinath VK, Arzreanne AR. Saliva as a diagnostic tool for assessment of dental caries. Arch Orofac Sci. 2006;1:57–59.
- Tenovuo J. Antimicrobial function of human saliva-how important is it for oral health? Acta Odontol Scand. 1998;56(5):250–256.
- Yarat A, Akyüz S, Koç L, et al. Salivary sialic acid, protein, salivary flow rate, pH, buffering capacity and caries indices in subjects with down’s syndrome. J Dent. 1999;27(2):115–118.
- Kaya S, Zortuk M, Adiguzel O, et al. Clinical presentation and management of ectodermal dysplasia. Biotechnol Biotechnol Equip. 2006;20(1):139–143.
- Galvão NS, Nascimento EHL, Lima CAS, et al. Can a high-density dental material affect the automatic exposure compensation of digital radiographic images? Dentomaxillofac Radiol. 2019;48(3):20180331.
- Panda SP. Ectodermal dysplasia: an overview. Indian J Forens Med Toxicol. 2020;14(4):9071–9074.