
ABSTRACT
Increased demand for interprofessional collaboration within the educational field also increases the need for the development and evaluation of interventions to improve collaboration. In Norway, the LOG model was developed and implemented in compulsory schools to facilitate interprofessional collaboration by increasing arenas for more efficient use of existing interprofessional resources. We evaluate the effects of the model on teachers’ perceptions of interprofessional collaboration in a cluster-randomized trial, with 19 schools randomized to the experimental group and 16 schools to the control group. We use data from 5th–7th grade teachers in the 35 participating schools (N = 157) prior to randomization and one-year into the implementation. Response rates were 70% and 74%, respectively. The PINCOM-Q scale was used to analyze effects of the model on various dimensions of interprofessional collaboration. At the one-year follow-up, the LOG model demonstrates no significant effects on teachers’ perceptions of interprofessional collaboration. However, there is an indication of effect on the organizational aim dimension (ES = −0.39, CI = −0.82–0.03), but the evidence is not conclusive.
Introduction
The problems schools and pupils are facing require collaboration between different professions. The idea is to be able to respond to pupils with complex needs, facilitate adapted education where all pupils can be a part of the classroom and the school community, and to relieve teachers from tasks not related to teaching (Norwegian Ministry of Education and Research, Citation2009, Citation2010, Citation2011, Citation2017). Schools are traditionally a “one profession organization” where teachers have dominated (Dahl, Citation2016). However, teachers alone cannot solve the problems pupils are facing; thus, interprofessional collaboration in the school context can contribute to more effective problem solving than a single profession would manage (Green & Johnson, Citation2015). The idea is that other professionals, such as school nurses and child welfare professionals, complement teachers in solving problems, for instance, related to antisocial behavior or learning difficulties. Together with teachers, other professionals can contribute to strengthening the learning environment and pupils’ development (Dahl, Citation2016). However, existing studies have mainly focused on the collaboration between one professional actor and the school, while there is a lack of research on collaborative practices involving several professionals at the same time (e.g., Allen-Meares, Montgomery, & Kim, Citation2013; Farrell, Alborz, Howes, & Pearson, Citation2010; Kvarme et al., Citation2010). Further, only a limited number of studies have assessed the benefits or disadvantages of interprofessional collaboration for teachers (Bagley & Pritchard, Citation1998).
The call for interprofessional collaboration is not new. As early as in 1986, The Ottawa Charter for Health Promotion emphasized that interprofessional collaboration between health-care services, community groups, and governments is necessary to deliver welfare services suited for children’s needs (World Health Organization, Citation1986). Within a European context, increasing interprofessional collaboration in schools is a key political priority. For the European Commission, the report by Edwards and Downes (Citation2013) pinpoints that as the school is a part of children’s daily life, it is also an important arena for early intervention, where vulnerable children can be reached and supported (Edwards & Downes, Citation2013). Through its work, the European Commission emphasizes the importance of interprofessional collaboration in the work against early school leaving. A central idea is that strengthening interprofessional collaboration among actors within schools, families, and external stakeholders will enhance the quality of school-related services through improving schools’ abilities to respond to pupils needs (European Commission, Citationn.d.).
Collaboration between different professionals is described using various terms and definitions, depending on the field of interest. Interprofessional collaboration, multiprofessional collaboration, interdisciplinary collaboration, interagency collaboration, and integrated care are some of the definitions used (e.g., Ødegård, Citation2006; Reeves, Lewin, Espin, & Zwarenstein, Citation2010). In our study, we use the term interprofessional collaboration, defined as collaboration between individuals with different professional backgrounds with a goal to solve joint tasks (Reeves et al., Citation2010). Seen from this view, the concept also entails the integration of different professionals’ knowledge and skills (Willumsen, Citation2009).
In Norway, the government has funded the development and implementation of a specific model for increasing interprofessional collaboration within the school context, the LOG model. LOG is a Norwegian abbreviation for leadership, organization, and implementation (Saltkjel et al., Citation2018). The main idea of the model is to facilitate more efficient use of existing interprofessional resources in the school context, reducing barriers between various professionals and increasing the role of management in supporting interprofessional collaboration. The aim of this study is to evaluate the effects of the LOG model on teachers’ perceptions of interprofessional collaboration. As the LOG model is an intervention for school development, we apply a cluster-randomized design with schools as entities for randomization. We expect a higher level of interprofessional perceptions among teachers within schools randomized to experimental condition compared to their counterparts in schools randomized to control condition.
Background - Interprofessional collaboration for children and youth
A number of studies have examined the benefits of interprofessional collaboration for the development of children and youth, mainly within the health-care field (e.g., Cooper, Evans, & Pybis, Citation2016; Fiks & Leslie, Citation2010). Furthermore, the use of different professions within the school context and the positive effects of their presence in the classroom have been frequently studied (Bagley & Pritchard, Citation1998; Cappella, Jackson, Bilal, Hamre, & Soule, Citation2011; Westhues, Hanbidge, Gebotys, & Hammond, Citation2009). In addition to these single empirical studies, there are also literature reviews on the effects of interprofessional collaboration on pupils. In these reviews, the collaboration is mainly between a specific professional group and the school, such as school social workers (Allen-Meares et al., Citation2013; Franklin, Kim, & Tripodi, Citation2009), teaching assistants (Farrell et al., Citation2010; Lindsay, Citation2007), and school nurses (Kvarme et al., Citation2010; Maughan, Citation2003).
The effects of these interventions have been studied on a multitude of outcomes for pupils, such as pupils’ academic achievements, school performance, and mental health outcomes, with effect sizes varying from zero to medium size (Allen-Meares et al., Citation2013; Franklin et al., Citation2009). Nevertheless, when it comes to studies analyzing the effects on teachers of interventions delivered by various professionals, the research is limited. One of a few studies investigating the effects of school social workers on both pupils and teachers was the randomized study conducted by Bagley and Pritchard (Citation1998). In the study, the school social workers’ tasks were primarily to work with and supervise pupils, support teachers in their work, and promote a tighter collaboration between school and home. Results show that teachers at schools with school social workers scored higher on staff morale and work motivation and were more confident in coping with difficult pupils after the three-year follow-up period, compared to teachers at schools that did not have a school social worker.
Barriers and facilitators of interprofessional collaboration in the school context
Although positive effects of interprofessional collaboration have been demonstrated in the school context, the implementation of interventions to improve collaboration is demanding. Research has identified a number of factors that can promote or hinder interprofessional collaboration, such as unclear professional roles and responsibilities, lack of leaders supporting interprofessional collaboration in the organization, duty of confidentiality, and lack of time or resources to practice collaboration across professionals from different agencies (Andersson, Citation2005; Rose, Citation2011; Widmark, Sandahl, Piuva, & Bergman, Citation2011). Also, insufficient communication and information flow between participants in interprofessional teams are barriers to interprofessional collaboration (Widmark et al., Citation2011). Furthermore, the study by Freeth (Citation2001) named several barriers for interprofessional collaboration, such as conflicting agendas and poor communication between team members.
According to the literature review by Cameron, Lart, Bostock, and Coomber (Citation2014), there are also several factors that can contribute to achieving efficient and successful interprofessional collaboration. The involvement of staff in the development of policies and procedures, understanding of the roles and responsibilities individuals and agencies have, effective communication, and strong and supportive management are among factors that promote collaboration between different professionals and agencies. A qualitative study by Altshuler (Citation2003) among students, educators, and caseworkers pinpoints definition of roles, guidelines regarding confidential information, and supportive networks at schools as important to obtaining successful collaboration. Accordingly, the study conducted by Hesjedal, Hetland, and Iversen (Citation2015) revealed that personal commitment, equality, and common goals also facilitate interprofessional collaboration.
Among the various factors that facilitate interprofessional collaboration, the literature review by Cameron et al. (Citation2014) emphasized a strong and supportive leadership as one of the most important factors. The reason is that a strong and supportive leadership contributes to better understanding of and confidence in ones’ own and other professionals’ roles, decreasing hindrances for interprofessional collaboration.
Leadership, organization, and implementation – the LOG model
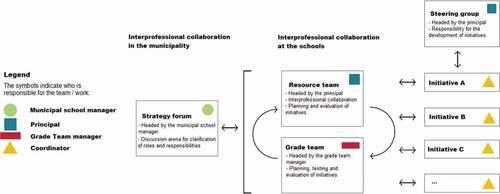
The aim of the LOG model is to facilitate interprofessional collaboration within schools (e.g., between collaborators such as school nurses and teachers), and across organizational levels (e.g., between municipal leaders, principals, and Child Welfare Services), by increasing the efficiency of already existing interprofessional resources within schools and municipalities (Saltkjel et al., Citation2018). The various actors involved are municipal school managers, school principals, and leaders of various municipal agencies such as Child Welfare Services, Public Health Services, and Educational Psychological Counseling Services. The LOG model builds on four existing arenas, a steering group, a resource team, and a grade team at the school level, and a strategy forum at the municipal level (see ). To enhance the collaboration between these arenas, the LOG model includes dialogue conferences at school and municipal levels. These are a vital part of the model, as they are expected to enhance communication between schools and various actors at the municipality level. The aim of this organizational structure is to develop existing meeting arenas at both the municipal and school levels, and increase the effect of these meeting arenas on interprofessional collaboration. The implementation of the LOG model is supported by a manual and a team of trainers. More detailed information regarding the tasks and responsibilities of each arena can be found in the study protocol (Saltkjel et al., Citation2018). According to the registration at clinicaltrials.gov (Identifier: NCT03248245), the primary outcomes are interprofessional collaboration at schools and in the municipality, as well as perceptions of interprofessional collaboration. The secondary outcomes are teacher self-efficacy, learning environment, teaching practices, and special needs education.
Figure 1. Meeting arenas in the LOG model, with communication and feedback loops on both the municipal and school levels
Methods
Research design
The study is funded by the Norwegian Directorate for Education and Training and runs from 2017 to 2020. The research design and the LOG model have been described in the study protocol (Saltkjel et al., Citation2018), and the study has been preregistered in ClinicalTrials.org (Identifier NCT03248245); however, we give a shorter description here. The Norwegian Center for Research Data has granted ethical permissions for the study (case no. 54470). All invited teachers were informed about the purpose of the research at data collection. The data collection was administered by online-surveys to all teachers at 5th to 7th grades in all participating schools. Participation in the surveys was voluntary and teachers could at any point withdraw. The researchers are under professional secrecy, and all data are stored on a secure server. Prior to the surveys, all teachers received an e-mail in which we briefly informed them about the project, the importance of responding, and the approval from the Norwegian Center for Research Data, as well as information on how the data will be managed.
The study has a cluster-randomized design, implying that participating schools are assigned either to the experimental condition or the control condition (Eldridge & Kerry, Citation2012). The population of this study is 5th to 7th grade teachers in all the primary schools in four Norwegian municipalities. The randomization process was stratified, that is, we randomized schools within each of the four municipalities. Half of all schools in each municipality were randomized to experimental group. In municipalities with odd numbers of schools, the odd numbers of schools were randomized to experimental condition. After randomization, 19 schools were assigned to the experimental condition and 16 to the control condition, with total 35 schools participating in the study. The randomization was conducted by means of randomization syntax in Stata version 14.2 (Saltkjel et al., Citation2018).
Schools randomized to the experimental group are implementing the LOG model, while schools randomized to the control group continue to work as they did before randomization. The teachers are aware of their status in this study, meaning that the study is not blinded. shows the flow chart of the cluster-randomized study.
Figure 2. Flow chart of the study
Aim of study and hypothesis
The aim of the study is to evaluate the effects of the LOG model on teachers’ perceptions of interprofessional collaboration. The hypothesis is that teachers within the experimental condition demonstrate a higher level of interprofessional perceptions compared to teachers within the control condition.
Data
We conducted a baseline and a one-year follow-up survey to all 5th–7th grade teachers in the 35 participating schools. The baseline (T1) survey was conducted prior to the randomization of the schools, autumn 2017. We invited the entire population of 225 teachers in 5th–7th grade to participate. Of the teachers, 70% (157 teachers) responded. The follow-up survey (T2) was conducted one year later, autumn 2018. At that point in time, 76 of the teachers no longer taught in the 5th–7th grades.
The main reason for the turnover was that teachers swap classrooms; however, some also had changed jobs or retired. We sent the T2 survey to the 149 teachers who were still teaching in 5th–7th grades. Of these teachers, 79% (117 teachers) responded to the T2 survey. We consider the response rates as satisfactory; however, the response rate at T2 was significantly higher (p = .047) in the experimental group (85%) than in the control group (72%).
Analyses
To determine the effect of the LOG model, we apply a two-level linear model, with teachers nested within schools. Two models are used to determine the effects. Both models follow an intention-to-treat principle (Gupta, Citation2011), and are hence restricted to teachers enrolled before randomization. Model 1 does not control for baseline and includes all T2 respondents from the population. Model 2 controls for baseline outcomes, and hence restricts the analyses to teachers who responded to both surveys. Thus, Model 2 encompasses a smaller sample but minimizes the chance of the results being biased by baseline differences.
We report coefficients and corresponding p-values for the treatment variable from all models. To ease the interpretation of the results, we have calculated standardized effects sizes by dividing each coefficient on the standard deviation (at T2) of the particular outcome. This gives an interpretation of the effect size in standard deviations, with 0 as no effect. We present these standardized effect sizes and corresponding confidence intervals as forest plots.
Prior to the onset of the study, we conducted power calculations based on pupil outcomes. The power calculations were conducted according to Donner, Birkett, and Buck (Citation1981), through the sample size calculator for cluster-randomized studies provided by the University of Aberdeen (Citation1999), applying a conventional 0.05 significance level and 80% statistical power. For a sample of 3965 pupils, power calculations suggest that the smallest identifiable effect size is 0.182, when ICC = 0.03 (Saltkjel et al., Citation2018).
Outcomes
To study interprofessional collaboration we used a validated scale, Perception of Interprofessional Collaboration Model (PINCOM-Q), developed by Ødegård (Citation2005, Citation2006). The PINCOM-Q comprises six dimensions measuring the perceptions of interprofessional collaboration at three levels - organizational-, group-, and individual. Organizational culture and organizational aim relates to aspects at organizational level, interprofessional climate, and leadership on group level, while professional power and motivation measure aspects at the individual level. Of 48 items, we included the 22 most relevant items for our study and adjusted a few to suit the school context. The 22 items chosen belonged to the strongest PINCOM-Q dimensions based on the Ødegård (Citation2006) study.
demonstrates the various items and scale reliability analyses. All the items were rated on a 7-point scale, from 1 = strongly agree to 7 = strongly disagree. Our results will be interpreted in the same way as in Ødegård and Strype (Citation2009), where a lower score indicates a higher perception of interprofessional collaboration.
Table 1. Items included in six dimensions of interprofessional collaboration, based on PINCOM-Q. Means and standard deviation
Background measures
We measured background variables used to study the similarities between teachers in schools randomized to the experimental and to the control condition. Sex was measured as 1 = man and 2 = woman. Academic degree was measured as 1 = not finished teacher’s education, 2 = general teacher’s education, 3 = preschool teacher, 4 = primary school teacher’s education, 5 = education from university, eventually with pedagogical specialization and 6 = other education. The variable was later recoded into a dichotomous variable to determine whether they had teachers’ education (1) or not (0). In addition, we measured years of work experience as a teacher.
Participating teachers and the success of randomization
At T1, 72% of the teachers were women, and all of them had an academic degree with a majority who had completed teachers’ education (78%). The average time working as a teacher was 17 years.
After randomization, the experimental and control groups were comparable on baseline data, such as sex, years of experience as a teacher, or educational level (). Furthermore, teachers from the experimental and the control condition were comparable on five out of six dimensions of interprofessional collaboration: organizational culture, organizational aim, interprofessional climate, professional power, and motivation. However, groups differed on leadership, with a higher mean score in the experimental group.
Table 2. The success of randomization based on T1 survey (N = 152–157)
Results
Scale reliability
displays the various items included in the six dimensions of interprofessional collaboration, based on the PINCOM-Q items, and scale reliability tests (Cronbach’s alpha). The responses vary from 1 = strongly agree to 7 = strongly disagree, and a higher value means a lower perception of interprofessional collaboration. This is the conventional way of presenting results from the PINCOM-Q. While three of the scales demonstrate a satisfactory Cronbach’s alpha above 0.62, the Cronbach’s alphas of the rest of the scales are above 0.70, indicating a high reliability. While the respondents disagree more often with the items in the dimensions of professional power and organizational aim, they agree more often with items within the dimensions of leadership, motivation, and interprofessional climate. The single items people disagree most often with are the items “Occasionally, professional groups do not work because some professionals dominate the meetings” and “Sometimes I am not able to present my perspectives because other high-status professionals talk all the time.” Respondents agree most often with the items “It is important that the group leader arrange the work in ways that help the group reach their goals” and “I find that I am appreciated by other professionals in the interprofessional groups I participate in”.
Correlation between outcomes
shows the means, standard deviations, and bivariate correlations for all variables at T1. A strong and significant correlation was observed between the dimensions of interprofessional climate and organizational culture (r = 0.66) and between interprofessional climate and motivation (r = 0.56). A medium strong and significant negative correlation was found between interprofessional climate and professional power (r = −0.36). As professional power is based on negatively formulated statements, it correlates negatively with other dimensions. Medium strong and positive correlations were found between interprofessional climate and organizational aim (r = 0.34), organizational culture and organizational aim (r = 0.47), organizational culture and motivation (r = 0.49), and leadership and motivation (r = 0.38). A small, however significant, correlation was observed between organizational culture and leadership (r = 0.28), while no significant correlations were observed between the rest of the dimensions of interprofessional collaboration.
Table 3. Means, standard deviations (SD), and bivariate intercorrelations for the six dimensions of interprofessional collaboration, based on T1 data
Effects
presents the effects of the LOG model on teacher perceptions of interprofessional collaboration (PINCOM-Q) derived from Model 1, a two-level model without control for baseline. Of the study population, 117 teachers responded to the T2 survey. However, as some teachers did not respond to all items included in the PINCOM-Q, analyses using Model 1 include 112–113 teachers. The results show no significant effects of the LOG model on five out of six dimensions of interprofessional collaboration: interprofessional climate, organizational culture, professional power, leadership, and motivation. Nevertheless, teachers from the experimental group scored significantly lower than the control group on the organizational aim dimension (p = .006), indicating that the LOG model contributed to more positive perceptions on the dimension of organizational aim. The dimension of organizational aim includes four items; thus, the experimental group agreed significantly more with three out of four items: “Interprofessional work is an area of priority in our school” (p < .001), “Interprofessional collaboration is well described in our school’s plans” (p = .005) and “Our school has definite and clear aims regarding interprofessional collaboration” (p = .019).
Table 4. T2 effects of the LOG model derived from Model 1, a two-level model without control for T1
displays the standardized effect sizes (ES) of the coefficients from Model 1 (reported in ). This analysis includes T2 responses only from teachers enrolled before randomization. The standardized effect of the LOG model on organizational aim is −0.63 (CI = −1.08 – −0.18), which is considered a medium effect size (Cohen, Citation1988; Shavelson, Citation1988). The standardized effect sizes for organizational culture (ES = −0.24), interprofessional climate (ES = −0.15), leadership (ES = −0.25), and professional power (ES = −0.11) are small, but all in the same direction. The effect size on the dimension of motivation is close to zero (ES = −0.03).
Figure 3. The standardized effects from Model 1, with 95% confidence intervals
presents the effects of the LOG model on teacher perceptions of interprofessional collaboration (PINCOM-Q) derived from Model 2, a two-level model where we control for baseline. In Model 2 we restrict the analyses to teachers with valid observations at T1. Some of the 91 teachers who did respond to both surveys did not respond to all questions. Hence, the statistical models include 84–85 teachers. The estimated effects size of Model 2 are similar to the ones derived from Model 1, but the effect on the organizational aim dimension is no longer significant (p = .070).
Table 5. T2 effects of the LOG model derived from Model 2, a two-level model with control for T1. Coefficients and 95% confidence intervals (CI 95%)
shows the standardized effect sizes (ES) of the coefficients from Model 2 (reported in ). The standardized effect of the LOG model on organizational aim is somewhat smaller than medium size (ES = −0.39, CI = −0.82–0.03). The standardized effect sizes on the remaining outcomes are small, and the effects on interprofessional climate (ES = 0.02) and motivation (ES = 0.07) are very small.
Figure 4. The standardized effects from Model 2, with 95% confidence intervals
To sum up, the results show a significant effect on organizational aim (p = .006); however, this result is no longer significant when we control for baseline (p = .070). This means that we should be careful in concluding that the LOG model has increased the feeling of organizational aim among teachers exposed to the LOG model. The LOG model might lead to an increased focus on the organizational aspects of interprofessional collaboration, however, the evidence is not conclusive.
Discussion
The aim of this study was to evaluate the effects of the LOG model on teachers’ perceptions of interprofessional collaboration after one year of implementation. The hypothesis was that teachers within the experimental condition demonstrate a higher level of interprofessional perceptions compared to teachers within the control condition. Our findings show that there are no effects of the intervention on four out of five dimensions measuring interprofessional perceptions. Earlier research has pinpointed that it takes time before complex interventions will produce measurable effects, and it can be difficult improving interprofessional collaboration at schools (Edwards & Downes, Citation2013). Nevertheless, there might be an effect of the LOG model on one out of five dimensions of interprofessional collaboration, i.e., organizational aim, but this effect is only significant without control for baseline.
Teachers from experimental schools report a significantly stronger perception of organizational aim, particularly when assessing the statements “Interprofessional work is an area of priority in our school,” “Interprofessional collaboration is well described in our school’s plans,” and “Our school has definite and clear aims regarding interprofessional collaboration”. The results show that the model has a potential to promote teachers’ perceptions of interprofessional collaboration at the organizational level (Larzelere, Kuhn, & Johnson, Citation2004).
Furthermore, teachers from schools randomized to the experimental group worked on improving interprofessional collaboration for one school year. Teachers were aware of this being a priority area at their school, which could have influenced their responses. Hence, the effect of the intervention could both be on actual collaboration, and may also create optimistic perceptions of collaboration. This means that we cannot disentangle a possible placebo effect from real effects of the intervention. Only by investigating the effects at the pupil level, one can judge whether the LOG model has improved collaboration in meaningful and real ways.
At this point in time, it seems that the intervention has not reached the group or individual levels of interprofessional collaboration. For instance, we did not find any effects on the interprofessional climate dimension, which includes statements about communication and information exchange between professionals within interprofessional groups. Effective communication has been mentioned in several articles as an important factor in achieving interprofessional collaboration (Altshuler, Citation2003), and lack of it has been described as a hindrance (Cameron et al., Citation2014; Widmark et al., Citation2011). The LOG model did not produce evidence of improved communication between teachers and other professionals, and might lack the ability to activate this prerequisite for interprofessional collaboration. Hence, we might not be surprised that there was no perceived improvement at the individual levels of interprofessional collaboration.
Further, no effect has been observed on the professional power measure, which involves the influence of other professionals on the processes within the interprofessional groups. The leadership and the motivation dimensions imply whether interprofessional groups have a successful management and give participants opportunities to develop and do something valuable through participation in interprofessional collaboration. These dimensions have been mentioned by previous research as important in achieving a successful interprofessional collaboration (Cameron et al., Citation2014; Hesjedal et al., Citation2015). Again, teachers have been in a limited degree included in the work with the LOG model. Their perceptions of these dimensions of interprofessional collaboration could therefore not change dramatically. As long as teachers are not a part of interprofessional groups it will be difficult to see visible effects the LOG model may have on the interprofessional collaboration at schools.
Strengths and limitations
The study has several strengths, and a clear one is that the T1 data were collected before the randomization. As shown in , the experimental and the control groups did not differ from each other on background variables or on most of the investigated dimensions of interprofessional collaboration. This is essential to measure the effects of an intervention. Use of the cluster-randomized design allowed us to evaluate the effect of the LOG model implemented by experimental schools.
Some limitations in this study need also to be mentioned. First of all, one should be careful in generalizing beyond the participating schools and municipalities. Furthermore, our population of teachers differed between the two measure points. Only 91 out of 153 teachers responding to T1 also responded at T2. This can be explained by usual movement, as teachers work with pupils at different grades each year, some retire, and some change their workplaces. This means that we expected some exchange among teachers between two measure points. We have therefore excluded new teachers from our primary analysis. Another limitation is that the response rate varied between the experimental and the control groups at T2. Significantly lower number of teachers at control schools responded to the one-year follow-up survey. It was challenging to motivate teachers from control schools to respond at T2, which resulted in a distinct difference in response rates between these two groups. Third, some arenas and activities are introduced at the municipal level, which introduces a risk of contamination from treatment to control condition. This means that our treatment estimates are downward biased.
Conclusion
We did not find earlier research evaluating interprofessional collaboration in the same way as we have. The limited amount of research we found showed that other professionals at schools might have positive effects on both pupils and teachers. Our research shows also that the LOG model has the potential to have positive effects for teachers. The results show an effect on the organizational aim measure, implying that the LOG model has made the interprofessional collaboration a part of the organization. Nevertheless, there is a need for further inclusion of teachers in interprofessional groups and activities in order to observe whether the LOG model or its components can enhance interprofessional collaboration at schools and in municipalities.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
Notes on contributors
Kamila Angelika Hynek
Kamila Angelika Hynek is a PhD candidate, currently working at the department of Mental Health and Suicide at the Norwegian Institute of Public Health. Her primary focus is mental health among young migrant women. In the LOG study, Hynek was responsible for the collection and analysis of data.
Ira Malmberg-Heimonen
Ira Malmberg-Heimonen is a professor in Social Work at Oslo Metropolitan University. She has a lead a number of RCT-studies within the social and educational fields. Her interest areas are intervention studies, program theory and fidelity, and the implementation of evidence-based practices. In addition to the large-scale evaluations, she has also studied poverty, unemployment and the effects of activation programs for long-term social assistance recipients, also in comparative settings.
Anne Grete Tøge
Anne Grete Tøge holds a PhD in Social Work and Social Policy. She is engaged in several cluster-randomised trials (C-RCT) in Norway, including evaluations of measures to improve the situation of low-income families (the HOLF study), students (the IKO study) and pupils (the LOG study). In the LOG study her primary responsibility has been to prepare and analyse data.
References
- Allen-Meares, P., Montgomery, K. L., & Kim, J. S. (2013). School-based social work interventions: A cross-national systematic review. Social Work, 58(3), 253–262. doi:10.1093/sw/swt022
- Altshuler, S. J. (2003). From barriers to successful collaboration: Public schools and child welfare working together. Social Work, 48(1), 52–63. doi:10.1093/sw/48.1.52
- Andersson, H. W. (2005). Kunnskapsstatus om det samlede tjenestetilbudet for barn og unge [Status of Knowledge About the Total Services for Children and Youth]. (Rapport 3/05). Retrieved from https://www.sintef.no/globalassets/upload/helse/psykisk-helse/pdf-filer/rapport_03-05_kunnskapsstatus_barn_og_unge.pdf
- Bagley, C., & Pritchard, C. (1998). The reduction of problem behaviours and school exclusion in at-risk youth: An experimental study of school social work with cost–Benefit analyses. Child & Family Social Work, 81(2), 74–80.
- Cameron, A., Lart, R., Bostock, L., & Coomber, C. (2014). Factors that promote and hinder joint and integrated working between health and social care services: A review of research literature. Health & Social Care in the Community, 22(3), 225–233. doi:10.1111/hsc.12057
- Cappella, E., Jackson, D. R., Bilal, C., Hamre, B. K., & Soule, C. (2011). Bridging mental health and education in urban elementary schools: Participatory research to inform intervention development. School Psychology Review, 40(4), 486–508.
- Cohen, J. (1988). Statistical power analysis for the behavioural sciences (2 ed.). Hillsdale: NJ: Lawrence Erlbaum Associates.
- Cooper, M., Evans, Y., & Pybis, J. (2016). Interagency collaboration in children and young people’s mental health: A systematic review of outcomes, facilitating factors and inhibiting factors. Child: Care, Health and Development, 42(3), 325–342. doi:10.1111/cch.12322
- Dahl, T. (2016). Om lærerrollen: Et kunnskapsgrunnlag [The teacher role: A basis of knowledge]. Retrieved from https://www.regjeringen.no/contentassets/17f6ce332c47437c8935d7ccc0a72769/rapport-om-laererrollen.pdf
- Donner, A., Birkett, N., & Buck, C. (1981). Randomization by cluster. Sample size requirements and analysis. American Journal of Epidemiology, 114(6), 906–914. doi:10.1093/oxfordjournals.aje.a113261
- Edwards, A., & Downes, P. (2013). Alliances for inclusion. Cross-sector policy synergies and interprofessional collaboration in and around schools. Brussels, Belguim: European Commission. Retrieved from https://www.researchgate.net/publication/304571167_Alliances_for_Inclusion
- Eldridge, S., & Kerry, S. (2012). A practical guide to cluster randomised trials in health services research. West Sussex, UK: John Wiley & Sons.
- European Commission. (n.d.). Strategic Partnerships in the field of education, training and youth. Retrieved from https://ec.europa.eu/programmes/erasmus-plus/programme-guide/part-b/three-key-actions/key-action-2/strategic-partnerships-field-education-training-youth_en
- Farrell, P., Alborz, A., Howes, A., & Pearson, D. (2010). The impact of teaching assistants on improving pupils’ academic achievement in mainstream schools: A review of the literature. Educational Review, 62(4), 435–448. doi:10.1080/00131911.2010.486476
- Fiks, A., & Leslie, L. (2010). Partnership in the treatment of childhood mental health problems: A pediatric perspective. School Mental Health, 2(2), 93–101. doi:10.1007/s12310-010-9037-2
- Franklin, C., Kim, J. S., & Tripodi, S. J. (2009). A meta-analysis of published school social work practice studies: 1980-2007. Research on Social Work Practice, 19(6), 667–677. doi:10.1177/1049731508330224
- Freeth, D. (2001). Sustaining interprofessional collaboration. Journal of Interprofessional Care, 15(1), 37–46. doi:10.1080/13561820020022864
- Green, B. N., & Johnson, C. D. (2015). Interprofessional collaboration in research, education, and clinical practice: Working together for a better future. Journal of Chiropractic Education, 29(1), 1–10. doi:10.7899/JCE-14-36
- Gupta, S. K. (2011). Intention-to-treat concept: A review. Perspectives in Clinical Research, 2(3), 109–112. doi:10.4103/2229-3485.83221
- Hesjedal, E., Hetland, H., & Iversen, A. C. (2015). Interprofessional collaboration: Self reported successful collaboration by teachers and social workers in multidisciplinary teams. Child & Family Social Work, 20(4), 437–445. doi:10.1111/cfs.12093
- Kvarme, L. G., Helseth, S., Sørum, R., Luth-Hansen, V., Haugland, S., & Natvig, G. K. (2010). The effect of a solution-focused approach to improve self-efficacy in socially withdrawn school children: A non-randomized controlled trial. International Journal of Nursing Studies, 47(11), 1389–1396. doi:10.1016/j.ijnurstu.2010.05.001
- Larzelere, R. E., Kuhn, B. R., & Johnson, B. (2004). The intervention selection bias: An underrecognized confound in intervention research. Psychological Bulletin, 130(2), 289–303. doi:10.1037/0033-2909.130.2.289
- Lindsay, G. (2007). Annual review: Educational psychology and the effectiveness of inclusive education/mainstreaming. British Journal of Educational Psychology, 77(1), 1–24. doi:10.1348/000709906X156881
- Maughan, E. (2003). The impact of school nursing on school performance: A research synthesis. The Journal of School Nursing, 19(3), 163–171. doi:10.1177/10598405030190030701
- Norwegian Ministry of Education and Research. (2009). Læreren: Rollen og utdanningen [Teacher: Role and education]. Oslo, Norway: Kunnskapsdepartementet.
- Norwegian Ministry of Education and Research. (2010). Tid til læring [Time for learning]. Oslo, Norway: Departementenes servicesenter. Retrieved from https://www.regjeringen.no/contentassets/e09a8895e0ac4e36ab2565ec5e59f804/no/pdfs/stm200920100019000dddpdfs.pdf
- Norwegian Ministry of Education and Research. (2011). Læring og fellesskap: Tidlig innsats og gode læringsmiljøer for barn, unge og voksne med særlige behov [Learning and fellowship. Early effort and good learning environment for children, youth and adults with particular needs]. Oslo, Norway: Departementenes servicesenter.
- Norwegian Ministry of Education and Research. (2017). Lærelyst – Tidlig innsats og kvalitet i skolen [Desire to learn - early effort and quality in school]. Retrieved from https://www.regjeringen.no/contentassets/71c018d2f5ee4f7da7df44a6aae265bc/no/pdfs/stm201620170021000dddpdfs.pdf
- Ødegård, A. (2005). Perceptions of interprofessional collaboration in relation to children with mental health problems. A pilot study. Journal of Interprofessional Care, 19(4), 347–357. doi:10.1080/13561820500148437
- Ødegård, A. (2006). Exploring perceptions of interprofessional collaboration in child mental health care. International Journal of Integrated Care, 6, 4. doi:10.5334/ijic.165
- Ødegård, A., & Strype, J. (2009). Perceptions of interprofessional collaboration within child mental health care in Norway. Journal of Interprofessional Care, 23(3), 286–296. doi:10.1080/13561820902739981
- Reeves, S., Lewin, S., Espin, S., & Zwarenstein, M. (2010). Interprofessional Teamwork for Health and Social Care. Oxford, UK: Wiley‐Blackwell.
- Rose, L. (2011). Interprofessional collaboration in the ICU: How to define? Nursing in Critical Care, 16(1), 5–10. doi:10.1111/j.1478-5153.2010.00398.x
- Saltkjel, T., Tøge, A. G., Malmberg-Heimonen, I., Borg, E., Lyng, S. T., Wittrock, C., … Lund, T. (2018). Research protocol: A cluster-randomised study evaluating the effects of a model for improving inter-professional collaboration in Norwegian primary schools. International Journal of Educational Research, 91, 41–48. doi:10.1016/j.ijer.2018.07.001
- Shavelson, R. J. (1988). Statistical reasoning for the behavioral sciences (2 ed.). Boston, USA: Allyn and Bacon.
- University of Aberdeen. (1999). Cluster sample size calculator. User manual. Aberdeen, UK.
- Westhues, A., Hanbidge, A. S., Gebotys, R., & Hammond, A. (2009). Comparing the effectiveness of school-based and community-based delivery of an emotional regulation skills program for children. School Social Work Journal, 34(1), 74–95.
- Widmark, C., Sandahl, C., Piuva, K., & Bergman, D. (2011). Barriers to collaboration between health care, social services and schools. International Journal of Integrated Care, 11, 3. doi:10.5334/ijic.653
- Willumsen, E. (2009). Tverrprofesjonelt samarbeid i praksis og utdanning i helse-og sosialsektoren. In Tverrprofesjonelt samarbeid i praksis og utdanning (pp. 16–32), Oslo, Norway: Universitetsforelaget.
- World Health Organization. (1986). Ottawa charter for health promotion, 1986. Retrieved from http://www.euro.who.int/en/publications/policy-documents/ottawa-charter-for-health-promotion,-1986