
Abstract
Objective
This study aimed to validate the translated Kannada version of the International Outcome Inventory for Hearing Aids (IOI-HA) questionnaire for hearing aid users.
Design
The original (English) and the translated versions of the IOI-HA questionnaire along with the Self-Assessment of Communication (SAC) were self-administered by hearing aid users. To examine test-retest reliability, 50% of the study participants completed the Kannada IOI-HA for a second time approximately 15 days later. The data analyses examined various psychometric properties using a predetermined quality criterion.
Study sample
105 Kannada-English bilingual adults using hearing aids.
Results
Factor analysis indicated a two-factor structure that explained a 61.8% variance in the IOI-HA. A Cronbach’s alpha coefficient of 0.7 indicated acceptable internal consistency. Good test-retest reliability (Interclass Correlation Coefficient > 0.9) was obtained for both conditions (i.e. between the original English and translated Kannada versions and also between two different administrations of the Kannada IOI-HA questionnaire). Divergent validity test results were acceptable, and no ceiling or floor effects were noted. Convergent validity testing of the SAC, however, was poor with small correlation, although the direction of correlation (i.e. negative) was as expected.
Conclusion
Results suggest acceptable psychometric properties of the Kannada version of the IOI-HA questionnaire.
Introduction
Outcome measurement is an important part of the hearing rehabilitation process. Health care providers, including audiologists, must be able to document the positive impacts of their services on their clients’ functional status and quality of life (Uriarte et al. Citation2005). There is an evolving need to document the outcomes of a hearing rehabilitation in a clinic, both as a research instrument and as a clinical tool. Recently, there has been a shift in focus on how the effectiveness of hearing aids in adults is measured (Humes and Krull Citation2012).
Present-day assessments do consider technical evaluations, but it is important to simultaneously consider the viewpoints of individuals living with hearing loss. To that end, patient-reported outcome measures (PROMs) should be considered, as these address individual needs in the rehabilitation process. Studies have indicated that observing practical challenges experienced by individuals with hearing loss (subjective hearing problems) was more useful in terms of predicting hearing aid fitting outcomes in these individuals than their objective impairment (measured using audiometric testing) (Cox, Stephens, and Kramer Citation2002; Jespersen, Bille, and Legarth Citation2014). This reinforces the view held by many professionals that the real-world impact of hearing loss varies significantly across individuals with the same degree of hearing loss and cannot be accurately predicted from hearing thresholds alone (Manchaiah and Stephens Citation2013). This change to an approach that includes an individual patient’s subjective experience will affect all parts of the audiological healthcare process.
Numerous questionnaires have been developed to address patients’ subjective experiences. Also, there are various measures specific to assessing hearing aid outcome, such as the International Outcome Inventory for Hearing Aids (IOI-HA; Cox and Alexander Citation2002), the Abbreviated Profile of Hearing Aid Benefit, (APHAB; Cox and Alexander Citation1995), the Satisfaction with Amplification in Daily Life assessment (SADL; Cox and Alexander Citation2001), and the Client-Oriented Scale for Improvement (COSI; Dillon, James, and Ginis Citation1997). Of these, IOI-HA is the assessment more commonly used internationally to measure hearing aid outcomes (Cox and Alexander Citation2002; Cox, Stephens, and Kramer Citation2002, Cox, Alexander, and Beyer Citation2003). IOI-HA has been translated to over 30 languages across the globe (International Collegium of Rehabilitative Audiology Citation2017).
IOI-HA is a seven-item questionnaire developed for use in both research and clinical settings to subjectively evaluate hearing aid outcomes. The questions focus on: (1) time during which hearing aids have been used; (2) benefit; (3) residual limitation in daily life activities; (4) satisfaction; (5) residual restrictions to participation; (6) impact on other people; and (7) quality of life (Cox and Alexander Citation2002). Each of the items has a five-point response scale, and it is possible to calculate a total score for the measure, with higher scores reflective of more positive outcomes. The response to each question ranges from “poor performance” (score = 1) to “best performance” (score = 5). The IOI-HA is brief enough to be appended to a research protocol without significant cost in time or other resources (Cox, Stephens, and Kramer Citation2002). The psychometric properties of the IOI-HA have been published in various languages including English (Cox and Alexander Citation2002), Dutch (Kramer et al. Citation2002), Danish (Jespersen, Bille, and Legarth Citation2014), Swedish (Brännström and Wennerström Citation2010), Korean (Chu et al. Citation2012), and Portuguese (Paiva et al. Citation2017). However, at the time of publication, the IOI-HA has not yet been psychometrically evaluated in Kannada language.
To compare the data across countries, it is important to have widely accepted standardised PROMs so that researchers and practitioners can use them effectively (Cox et al. Citation2000). Using the same standardised measures in different populations does not result in data that is directly comparable (Hall et al. Citation2018). Hence, it is important that the questionnaire is translated to the regional language and later validated so that the tool can be used to measure the outcome of hearing rehabilitation in individuals across different countries (Hall et al. Citation2018). Ideally, a series of outcome measures focussing on different elements such as hearing disability, hearing aid outcome, social participation, and quality of life should be administered on hearing aid users to assess the benefit holistically.
Kannada is a South Indian Dravidian language spoken by around 38 million people who predominantly reside in the State of Karnataka, India (Census of India Citation2001). In previous studies, we have translated and adapted several English language questionnaires to Kannada, including the Hearing Handicap Questionnaire (HHQ; Thammaiah et al. Citation2017), the Participation Scale (Thammaiah et al. Citation2018), and the Assessment of Quality of Life (AQoL-4D; Thammaiah et al. Citation2019). Furthermore, to add a hearing aid outcome measure to the test battery, we also translated the IOI-HA to Kannada (see Supplementary Appendix 2) using the well-accepted forward-backward translation method (Thammaiah et al. Citation2016). This article reports the psychometric assessment of the Kannada version of the IOI-HA questionnaire for use among Kannada-speaking adults with hearing loss.
Method
Study design
The study used a cross-sectional survey design and was carried out in the state of Karnataka, India. Ethical approval was obtained from the All India Institute of Speech and Hearing (AIISH) based in Mysore City. All participants included in the study provided a written informed consent.
Participants
Participants were invited from a pool of adults (18 years and older) with hearing loss who were attending the local clinics in Mysore to obtain hearing aids. Participants were required to be able to read and write in both Kannada and English. 105 hearing aid users were recruited using a consecutive sampling method. A minimum sample size of 100 participants, or seven times the number of items in the questionnaire, has been indicated as an adequate sample size for questionnaire validation studies. Based on standards for good methodological quality, this sample size has also been deemed adequate for the psychometric evaluation and validation of a questionnaire recommended in the Consensus-Based Standards for the Selection of Health Status Measurement Instruments (COSMIN) checklist (Terwee et al. Citation2012).
The demographic and audiological details of the study participants are provided in . Over 70% of the participants were males, and this represents a hearing-impaired population that does include more males than females. The average age was 59 years (Median = 61 years, Inter Quartile Range = 25.5 years). Participants represented various types and degrees of hearing loss. The four-frequency pure-tone average (PTA) was 63 dB and 61 dB HL in the right and left ears, respectively. The average self-reported duration of hearing loss was 8.9 years, and the majority of participants (96%) had bilateral hearing loss. One-third of the participants used hearing aids bilaterally, whereas the remaining two-thirds used a hearing aid in only one ear. According to data from AIISH, this spread was representative of the hearing aid provision pattern in Mysore City
Table 1. Demographic and audiological details of the study participants.
Translation of IOI-HA questionnaire
The seven questions in the IOI-HA questionnaire (along with the abbreviated form) are listed in Appendix 1. Each of the items was scored using the integers from 1 to 5 for the five response choices. The leftmost response with a score of 1 indicated the poorest outcome, whereas the rightmost response with a score of 5 indicated the best outcome.
The IOI-HA questionnaire, along with four other self-report measures, was translated and adapted into Kannada (for details, see Thammaiah et al. Citation2016; Supplementary Appendix 2). The questionnaires were translated using the standard forward-backward procedure (Beaton et al. Citation2000). The key steps during the translation-adaptation process included: (i) forward translation; (ii) common translation synthesis; (iii) backward translation; (iv) expert committee review; and (v) pre-final testing (Thammaiah et al. Citation2016).
Data collection
The researcher provided necessary instructions about the study to participants and answered their questions. Their questions were mainly about the study process and further explanation of the questionnaire, and these questions were addressed without providing any leading prompts about the individual items. The questionnaires were self-administered by the participants during their visits to the audiology clinics. However, the researcher examined the questionnaires afterward in case any items were left blank and encouraged participants to complete any missing items.
All participants completed both the Kannada and English versions of the IOI-HA questionnaire and the Kannada version of the Self-Assessment of Communication questionnaire (SAC; Schow and Nerbonne Citation1982); each one also provided some demographic details. Nearly half of the participants completed the Kannada version of the IOI-HA questionnaire two weeks after the initial test to examine test-retest reliability. The second questionnaire was either filled in during a second session at the audiology clinic or at the participant’s home.
Data analysis
IOI-HA responses result in an ordinal level of measurement. A general statistical convention is that nonparametric statistics are most appropriate for ordinal data, and using parametric statistics may result in some errors (Bürkner and Vuorre Citation2019; Liddell and Kruschke, Citation2018). However, there is the precedence of using parametric statistics in the behavioural literature, especially when evaluating the psychometric properties of questionnaires. While approaches such as Item Response Theory (IRT; Nering and Ostini Citation2010) are most appropriate for ordinal data (Nering and Ostini Citation2010), some researchers have argued that approaches such as Principal Component Analysis (PCA), which was designed for interval/ratio data, can be used for ordinal data and is very often used in this way (Norman Citation2010).
IOI-HA was developed over 20 years ago without the use of ITI, and all previous studies (Brännström and Wennerström Citation2010; Chu et al. Citation2012; Cox and Alexander Citation2002; Jespersen, Bille, and Legarth Citation2014; Kramer et al. Citation2002; Pavia et al. Citation2017) that examined the psychometric properties of IOI-HA except the recent international study (Leijon et al. Citation2020) have applied parametric methods such as PCA. Considering this, to allow maximum inter-study compatibility, the statistical analysis in this study falls generally in line with the procedure applied by Cox and Alexander (Citation2002) in the original IOI-HA study. However, this study used nonparametric statistical tests where necessary (i.e. making no comparisons with previous studies).
shows the redefined quality criteria recommendations that were used to evaluate the psychometric properties of the questionnaire (Anastasi Citation1976; Terwee et al. Citation2007). The psychometric properties tested included: (i) factor structure analysis, (ii) internal consistency (reliability), (iii) test-retest reliability (stability), (iv) convergent (or construct) validity, (v) discriminant validity, and (vi) floor/ceiling effects.
Table 2. Recommended quality criteria for acceptance of different psychometric properties analysed in the study.
The data were analysed using the International Business Machines Corporation Statistical Package for Social Sciences – Version 20 (IBM Corp. Released Citation2011) and the R (psych package) softwares. PCA was performed to examine the factor structure. Cronbach’s Alpha was calculated to examine internal consistency. The Intra-Class Correlation coefficient (ICC) with a two-way mixed model for an absolute agreement was calculated on the total score of the IOI-HA to examine test-retest reliability. Although ICC was developed for interval/ratio data, it has also been commonly used with ordinal data, especially when the data is reasonably well modelled by a normal distribution (Koo and Li Citation2016; Liljequist, Elfving, and Skavberg Roaldsen Citation2019). Spearman’s correlation coefficient was calculated to examine discriminant and convergent validities.
Results
provides the mean, median, standard deviation, and interquartile range for the Kannada IOI-HA questionnaire. presents the frequency of responses for each IOI-HA item.
Figure 1. Distribution of responses for each IOI-HA item.
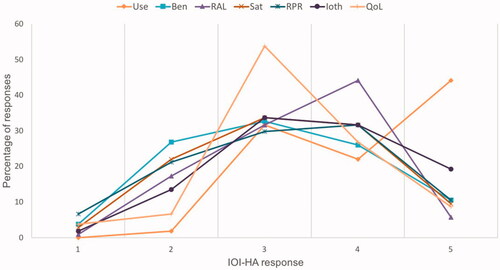
Table 3. Mean, median, standard deviation (SD), and interquartile range (IRQ) for IOI-HA questionnaire in Kannada along with norms from the western population reported by Cox, Alexander, and Beyer (Citation2003).
Factor structure
PCA with Varimax rotation was performed. The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.79 with a reference value of 0–1.0, and Bartlett’s Test of Sphericity was significant [X2(66) = 234.5, p ≤ 0.001], indicating an appropriate study sample. The PCA resulted in a two-factor structure, which explained the 61.8% variance in the seven-question IOI-HA (see ). Cross-loadings were noted for question 6; therefore, we performed PCA with several different rotations to identify better factor structure, although such attempts were not successful.
Table 4. Results of principal components analysis for questionnaire.
Internal consistency (reliability)
Cronbach’s Alpha is a measure of reliability showing the extent to which items in the scale are a consistent measure of a concept (or construct). Cronbach’s Alpha of 0.7 and 0.81 were obtained for the Kannada and English versions of the IOI-HA, respectively. These results indicate acceptable internal consistency.
Test-retest reliability (stability)
The test-retest reliability value of the IOI-HA full scale was calculated for two conditions. The first condition checked equivalence in the results of the original English and translated Kannada versions administered the first time to participants. The ICC value (average measures) was found to be 0.94, indicating good reliability between the original English and the translated Kannada versions. The second condition checked test-retest reliability over time (i.e. stability) between the first and second administrations of the Kannada version. The ICC value (average measures) was found to be 0.93, suggesting acceptable test-retest reliability.
Discriminant validity
presents Spearman’s Correlation among the IOI-HA questions. Significance values were adjusted for False Discovery Rate (FDR) with alpha 0.05 to account for multiple comparisons. The correlations range from negligible (−0.8) to moderately strong (0.77), although most correlations were between 0.3 and 0.7 (i.e. weak to moderate), suggesting good discriminant validity. This means each item is tapping into some aspects of hearing aid outcome, although they may not be measuring the same underlying trait.
Table 5. Spearman’s Correlation between IOI-HA items.
Convergent (or construct) validity
There was a small but statistically significant negative correlation observed between IOI-HA with SAC full scale (r = –0.25, p < 0.05), SAC subscale 1 (r = –0.22, p < 0.05), SAC subscale 2 (r = –0.25, p < 0.01), and SAC subscale 3 (r = –0.33, p < 0.01). These results were not as expected, as the prior hypothesis set up the expectation of a moderate correlation and suggested poor convergent validity for the IOI-HA with the SAC scale. However, having a negative correlation satisfies the prior hypothesis, suggesting that higher hearing aid benefits are correlated with lower communication problems.
Floor and ceiling effects
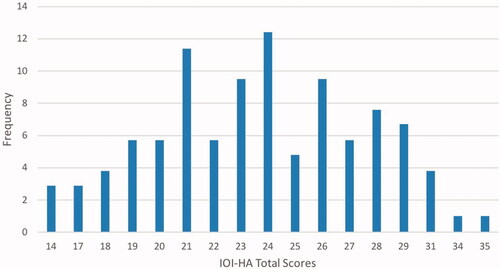
shows the frequency of IOI-HA scores in the current study sample. The floor and ceiling effects were found to be 3% and 1% respectively, which is well below the 15% threshold criteria indicating no floor and ceiling effect ().
Figure 2. Frequency distribution of the Kannada IOI-HA total scores.
Discussion
The present paper reports the psychometric assessment of the Kannada version of the IOI-HA questionnaire for use among Kannada-speaking adults with hearing loss. Thammaiah et al. (Citation2016) has previously reported the translation procedure. The mean values of IOI-HA in the current study were comparable to norms for the U.S. population reported by Cox, Alexander, and Beyer (Citation2003). Also, the psychometric properties of the Kannada version of IOI-HA were found to be acceptable and show resemblance in many aspects to other previously translated versions of IOI-HA including Danish (Jespersen, Bille, and Legarth Citation2014), Swedish (Brännström and Wennerström Citation2010), Dutch (Kramer et al. Citation2002), and Korean (Chu et al. Citation2012).
The Kannada version of IOI-HA had a two-factor structure. Although the two-factor structure was consistent with the original English version (Cox and Alexander Citation2002) as well as other translated versions (Kramer et al. Citation2002; Jespersen, Bille, and Legarth Citation2014), the item loadings into factors differed across studies. For example, in the original publication (Cox and Alexander Citation2002), the items on use, benefit, satisfaction and quality of life were loaded on one factor and the remaining three items loaded to second factor. In the current study, all items except quality of life were loaded into a single factor. Moreover, it is noteworthy that the two factors were not mutually exclusive, and cross-loading was noted in several items, as in previous studies. These observations indicated that several IOI-HA items shared variance with other constructs. This was expected, as the IOI-HA has limited items, and each item measures a unique construct, unlike other PROMs in which several items focus on a single construct. The Kannada version of IOI-HA also had acceptable internal consistency (Cronbach’s Alpha of 0.7) and test-retest reliability (ICC = 0.71). The internal consistency, as measured using Cronbach’s Alpha, was found to be slightly higher; this is similar to the 0.78 consistency in English (Cox and Alexander Citation2002), 0.83 in Korean (Chu et al. Citation2012), 0.82 in Danish (Jespersen, Bille, and Legarth Citation2014), 0.84 in Portuguese (Pavia et al., Citation2017), and 0.77–0.79 in Dutch (Kramer et al. Citation2002). Test-retest reliability in the current study (i.e. 0.93) is comparable to previous studies such as 0.94 in Korean (Chu et al. Citation2012), 0.42–0.82 in Dutch (Kramer et al. Citation2002), and 0.72–0.96 in Portuguese (Pavia et al., Citation2017). It is noteworthy that the statistical approaches such as PCA and Cronbach’s Alpha were designed for interval/ratio data, and although they have been applied for ordinal data in this study, its most appropriate to use them only for comparison with previous studies.
Discriminant validity is an important measure of orthogonality, or whether each subscale and item is measuring a different dimension of IOA-HA. The study results support good discriminant validity of the Kannada version of the IOA-HA questionnaire, as each of the correlations (inter-item) were below 0.60 (see ). These results were consistent with previous studies that showed a good discriminant validity of IOI-HA in English and other translated versions (Cox, Stephens, and Kramer Citation2002; Kramer et al. Citation2002; Pavia et al., Citation2017). The current study showed poor convergent validity (i.e. small correlation) with the communication measure, although the direction of correlation was as expected (i.e. communication problems diminished when hearing aid benefit was better). These results suggest that the benefit noted by IOI-HA might be comparable to other related PROMs, although further research should examine this.
The presence of significant floor or ceiling effects can affect between-group measurements (i.e. not being able to identify the difference between two groups) and within-group measurements (i.e. responsiveness in terms of change over time). For this reason, a good PROM should not have a floor or ceiling effect. Although measures were taken to avoid this during the construction of the original IOA-HA, the original validation study does show a somewhat negative skewness of overall scores (i.e. a larger percentage of people showing higher overall scores (Cox and Alexander Citation2002). However, the Kannada version of IOA-HA did not show any such effects, thereby strengthening the psychometric quality of the measure. Overall, the current study shows acceptable psychometric properties of IOI-HA, suggesting it can be used for research and clinical purposes in Kannada-speaking hearing aid users.
Strengths and limitations of the study
The current study is the first to report psychometric validation of the IOI-HA in an Indian language (Kannada). The main strength of the study is that it used the well-established forward-backward translation procedure (Thammaiah et al. Citation2016) and a predetermined quality criterion to evaluate the psychometric properties. However, the study has a few limitations. First, the study used several statistical procedures that were designed for metric data (e.g. PCA, Cronbach’s Alpha) to ensure comparison to previous studies, although using approaches that were specifically designed for ordinal data (e.g. IRT) may have been more appropriate. Second, the population was not homogenously distributed across demographic factors like gender, education, socio-economic status, and type of hearing loss. There was a high number of participants with tertiary education, although it was a typical sample of hearing aid users in urban India. This may have resulted in some sampling bias. Third, predictive validity and responsiveness (i.e. the ability of a questionnaire to detect clinically important changes over time) were not assessed in the present study.
Supplemental Material
Download PDF (78.3 KB)Acknowledgements
The authors would like to acknowledge Dr. Hansapani Rodrigo for his contribution of statistical input.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Anastasi, A. 1976. Psychological Testing (4th ed). New York: Macmillan Publishing.
- Beaton, D. E., C. Bombardier, F. Guillemin, and M. B. Ferraz. 2000. “Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures.” Spine 25 (24): 3186–3191. doi:https://doi.org/10.1097/00007632-200012150-00014
- Brännström, K. Jonas, and Ingegerd Wennerström. 2010. “Hearing Aid Fitting Outcome: Clinical Application and Psychometric Properties of a Swedish Translation of the International Outcome Inventory for Hearing Aids (IOI-HA).” Journal of the American Academy of Audiology 21 (8): 512–521. doi:https://doi.org/10.3766/jaaa.21.8.3.
- Bürkner, Paul-Christian, and Matti Vuorre. 2019. “Ordinal Regression Models in Psychology: A Tutorial.” Advances in Methods and Practices in Psychological Science 2 (1): 77–101. doi:https://doi.org/10.1177/2515245918823199.
- Census of India. 2001. Abstract of Speakers’ Strength of Languages and Mother Tongues. Accessed 23 June 2020. http://www.censusindia.gov.in/2011-common/censusda-taonline.html.
- Chu, Hosuk, Yang-Sun Cho, Shi-Nae Park, Jae Yong Byun, Jung Eun Shin, Gyu Cheol Han, Byung Chul Cheon, Jun Ho Lee, and Jae Yun Jung. 2012. “Standardization for a Korean Adaptation of the International Outcome Inventory for Hearing Aids: Study of Validity and Reliability.” Korean Journal of Otorhinolaryngology-Head and Neck Surgery 55 (1): 20–25. doi:https://doi.org/10.3342/kjorl-hns.2012.55.1.20.
- Cox, R., and G. C. Alexander. 1995. “The Abbreviated Profile of Hearing Aid Benefit.” Ear and Hearing 16 (2): 176–183. doi:https://doi.org/10.1097/00003446-199504000-00005.
- Cox, R. M., and G. C. Alexander. 2002. “The International Outcome Inventory for Hearing Aids (IOI-HA): Psychometric Properties of the English Version.” International Journal of Audiology 41 (1): 30–35. doi:https://doi.org/10.3109/14992020209101309.
- Cox, R. M., and G. C. Alexander. 2001. “Validation of the SADL Questionnaire.” Ear and Hearing 22 (2): 151–160. doi:https://doi.org/10.1097/00003446-200104000-00008.
- Cox, R. M., G. C. Alexander, and C. M. Beyer. 2003. “Norms for the International Outcome Inventory for Hearing Aids.” Journal of the American Academy of Audiology 14 (8): 403–413.
- Cox, R., M. Hyde, S. Gatehouse, W. Noble, H. Dillon, R. Bentler, D. Stephens, et al. 2000. “Optimal Outcome Measures, Research Priorities, and International Cooperation.” Ear and Hearing 21 (4 Suppl): 106S–115S. doi:https://doi.org/10.1097/00003446-200008001-00014.
- Cox, R. M., D. Stephens, and S. E. Kramer. 2002. “Translations of the International Outcome Inventory for Hearing Aids (IOI-HA).” International Journal of Audiology 41 (1): 3–26. doi:https://doi.org/10.3109/14992020209101307.
- Dillon, H., A. James, and J. Ginis. 1997. “Client Oriented Scale of Improvement (COSI) and Its Relationship to Several Other Measures of Benefit and Satisfaction Provided by Hearing Aids.” Journal of the American Academy of Audiology 8 (1): 27–43.
- Hall, Deborah A., Silvia Zaragoza Domingo, Leila Z. Hamdache, Vinaya Manchaiah, Spoorthi Thammaiah, Chris Evans, and Lena L. N. Wong. 2018. “A Good Practice Guide for Translating and Adapting Hearing-Related Questionnaires for Different Languages and Cultures.” International Journal of Audiology 57 (3): 161–175. doi:https://doi.org/10.1080/14992027.2017.1393565.
- Humes, L. E., and V. Krull. 2012. “Evidence about the Effectiveness of Hearing Aids in Adults.” In: Wong L, Hickson L, (Eds.). Evidence Based Practice in Audiology. San Diego, USA; Plural Publishing.
- IBM Corp. Released. 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.
- International Collegium of Rehabilitative Audiology. 2017. IOI-HA List of Questionnaires. Accessed June 23, 2020 https://icra-audiology.org/Repository/self-report-repository/Survey.
- Jespersen, C. T., M. Bille, and J. V. Legarth. 2014. “Psychometric Properties of a Revised Danish Translation of the International Outcome Inventory for Hearing Aids (IOI-HA).” International Journal of Audiology 53 (5): 302–308. doi:https://doi.org/10.3109/14992027.2013.874049.
- Koo, T. K., and M. Y. Li. 2016. “A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research.” Journal of Chiropractic Medicine 15 (2): 155–163. doi:https://doi.org/10.1016/j.jcm.2016.02.012.
- Kramer, S. E., S. T. Goverts, W. A. Dreschler, M. Boymans, and J. M. Festen. 2002. “International Outcome Inventory for Hearing Aids (IOI-HA): Results from The Netherlands.” International Journal of Audiology 41 (1): 36–41. doi:https://doi.org/10.3109/14992020209101310.
- Leijon, A., H. Dillon, L. Hickson, M. Kinkel, S. E. Kramer, and P. Nordqvist. 2020. “Analysis of Data from the International Outcome Inventory for Hearing Aids (IOI-HA) Using Bayesian Item Response Theory.” International Journal of Audiology 1–8. doi:https://doi.org/10.1080/14992027.2020.1813338.
- Liddell, T. M., and J. K. Kruschke. 2018. “Analyzing Ordinal Data with Metric Models: What Could Possibly Go Wrong?” Journal of Experimental Social Psychology 79: 328–348. doi:https://doi.org/10.1016/j.jesp.2018.08.009.
- Liljequist, D., B. Elfving, and K. Skavberg Roaldsen. 2019. “Intraclass Correlation – A Discussion and Demonstration of Basic Features.” PLoS One 14 (7): e0219854. doi:https://doi.org/10.1371/journal.pone.0219854.
- Manchaiah, V. K. C., and D. Stephens. 2013. “Perspectives on Defining ‘Hearing Loss’ and Its Consequences.” Hearing, Balance and Communication 11 (1): 6–16. doi:https://doi.org/10.3109/21695717.2012.756624.
- Nering, M.L., & Ostini, R. (Eds). 2010. Handbook of Polytomous Item Response Theory Models. New York, NY: Routledge.
- Norman, G. 2010. “Likert Scales, Levels of Measurement and the ‘Laws’ of statistics.” Advances in Health Sciences Education Theory Practice 15 (5): 625–632. doi:https://doi.org/10.1007/s10459-010-9222-y.
- Pavia, S. M., J. F. Simões, A. M. Paiva, F. J. Sousa, and J. P. Bébéar. 2017. “Translation of the International Outcome Inventory for Hearing Aids into Portuguese from Portugal.” British Medical Journal Open 7 (3): e013784. doi:https://doi.org/10.1136/bmjopen-2016-013784.
- Schow, R., and M. Nerbonne. 1982. “Communication Screening Profile: Use with Elderly Clients.” Ear and Hearing 3 (3): 135–147. doi:https://doi.org/10.1097/00003446-198205000-00007.
- Terwee, C. B., S. D. Bot, M. R. de Boer, D. A. van der Windt, D. L. Knol, J. Dekker, L. M. Bouter, and H. C. de Vet. 2007. “Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires.” Journal of Clinical Epidemiology 60 (1): 34–42. doi:https://doi.org/10.1016/j.jclinepi.2006.03.012.
- Terwee, C. B., L. B. Mokkink, D. L. Knol, R. W. Ostelo, L. M. Bouter, and H. C. de Vet. 2012. “Rating the Methodological Quality in Systematic Reviews of Studies on Measurement Properties: A Scoring System for the COSMIN Checklist.” Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation 21 (4): 651–657. doi:https://doi.org/10.1007/s11136-011-9960-1.
- Thammaiah, S., V. Manchaiah, V. Easwar, and R. Krishna. 2016. “Translation and Adaptation of Five English Language Self-Report Health Measures to South Indian Kannada Language.” Audiology Research 6 (1): 153. http://dx. doi:https://doi.org/10.4081/audiores.2016.153.
- Thammaiah, S., V. Manchaiah, V. Easwar, R. Krishna, and B. McPherson. 2018. “The Participation Scale: Psychometric Properties of a South Indian Translation with Hearing-Impaired Respondents.” Disability and Rehabilitation 40 (22): 2650–2657. doi:https://doi.org/10.1080/09638288.2017.1347208.
- Thammaiah, S., V. Manchaiah, V. Easwar, R. Krishna, and B. McPherson. 2017. “Psychometric Properties of the Hearing Handicap Questionnaire: A Kannada (South-Indian) Translation.” International Journal of Audiology 56 (3): 194–201. doi:https://doi.org/10.1080/14992027.2016.1247500.
- Thammaiah, S., V. Manchaiah, R. Krishna, A. A. Zekveld, and S. E. Kramer. 2019. “Assessment of the Psychometric Properties of the AQoL-4D Questionnaire in Kannada Language for Use with Adults with Hearing Loss.” International Journal of Audiology 58 (6): 326–332. doi:https://doi.org/10.1080/14992027.2019.1587181.
- Uriarte, M., L. Denzin, A. Dunstan, J. Sellars, and L. Hickson. 2005. “Measuring Hearing Aid Outcomes Using the Satisfaction with Amplification in Daily Life (SADL) Questionnaire: Australian Data.” Journal of the American Academy of Audiology 16 (6): 383–402. doi:https://doi.org/10.3766/jaaa.16.6.6.