Abstract
Background Earlier reports on reduced physical performance and osteoporosis-related fractures have mostly been short-term studies. The aim of this investigation was to examine the effects of fractures on physical functioning 3 years after trauma, the latter being stratified for pain.
Participants and methods The study consisted of a population-based case-control study including 289 subjects from the “Good Ageing in Skåne” project. Men and women with fractures, aged 60–93 years, were divided into one group with pain (FP, n = 71) and one without pain (FnP, n = 53). Fractures included vertebrae, hip, pelvis or ankle according to the national medical register. A third group of subjects without fractures or pain (CnP, n = 165) was used as control. Pain during the previous month, health variables, lifestyle, medication, use of a walking aid, and sociodemographic variables were self-reported. Walking 15 m, 2 × 15 m, and timed get-up-and-go (TUG)—all at self-selected and maximum speed—and maximum handgrip strength were assessed objectively.
Results Among the FP patients, almost half of the group suffered pain on a daily basis. The subjects in the CnP and FnP groups performed significantly better than the FP patient group in all functional tests. Median time for walking a distance of 15 m at self-selected speed was 16, 13 and 12 sec for the CnP, FnP and FP groups, respectively. Both fracture and pain independently explained lower walking speed (self-selected and maximum) as well as TUG, adjusted for age, sex and co-morbidity in a multiple regression model. Those who had sustained fractures more than 3 years previously performed significantly better in walking 15 m and 2 × 15 m at both self-elected and maximum speed than those with a more recent fracture, irrespective of pain.
Interpretation After 3 years, patients who had sustained a fracture but who experienced no pain performed almost as well as control subjects. Pain and fracture were independently influenced by physical function.
It is well documented that patients who suffer from pain after osteoporosis-related fracture have reduced physical function up to 1 year after trauma (Nevalainen et al. Citation2004, Osnes et al. Citation2004, Theander et al. Citation2004, Grafe et al. Citation2005). Less has been written about physical performance over a longer period, and to our knowledge there have been no studies published that have explored the independent effect of fracture on physical performance. Differences between the results of physical tests involving fractures accompanied by pain and not accompanied by pain may be of relevance to physiotherapy aimed at rapid recovery, and may help to identify patients at risk of physical decline.
We examined the long-term independent effect of fracture, irrespective of pain, on physical performance tests using walking 15 m and 2 × 15 m at self-selected and maximum speed, Timed Get-Up-and-Go (TUG) at self-selected and maximum speed, and maximum handgrip strength as the dependent variables.
Methods
Study population
The participants were recruited between February 2001 and March 2002 from an ongoing longitudinal Swedish investigation known as Good Ageing in Scania (Gott Åldrande i Skåne; GÅS). GÅS is one of four parts of the Swedish National study on Ageing and Care (SNAC) (Lagergren et al. Citation2004). The GÅS study includes men and women in 9 age cohorts: 60, 66, 72, 78, 81, 84, 87, 90 and 93 years. The subjects are randomized from the municipality registers. The study was approved by the regional ethics committee of Lund University (2002; registration no. LU 744-00) and all participants provided written consent.
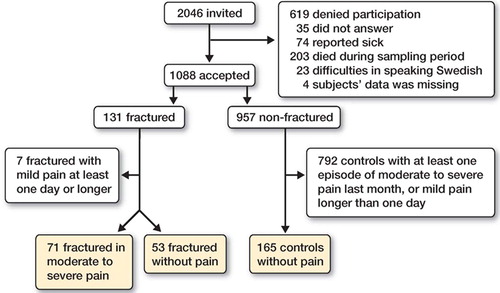
Of 2,046 subjects invited to participate by letter, 1,088 accepted the invitation and they were divided into 131 cases with at least 1 fracture of vertebra, pelvis, hip or ankle, and 956 controls without corresponding fractures (). For identification of fractures, see below. The subjects were divided into (1) one group with fracture less than 3 years previously, and (2) one group with fracture 3 years or more previously, after dichotomization.
Flow chart showing inclusion and dropout of study participants.
In both cases and controls, there were participants with fractured wrists. The proportion of control individuals with fracture was 16%, and the corresponding figures for individuals with fracture and pain and with fracture but no pain were 24% and 25%, respectively. The difference was not statistically significant (p = 0.3).
The cases and controls were further dichotomized regarding whether they had experienced no or little pain, or moderate to severe pain during the previous month. Among the controls, those with at least one episode of moderate to severe pain during the previous month were excluded. Finally, the study consisted of 3 groups: (1) 71 cases with fracture (53 women) with one or more occasions of pain in the previous month, and with a mean age of 82 (SD 8.4) years, (2) 53 cases (42 females) with fracture but no pain or with little pain, and with a mean age of 83 (SD 8.0) years, and (3) a third group of 165 controls without any fracture or pain (112 females), with a mean age of 82 (SD 8.4) years (Figure).
Questionnaire
Questions were asked about medical history of osteoporosis-related fracture, number of fractures, and time since the last fracture (). To assure the correctness of the medical history reported and after the participant had given his/her permission, fractures were identified through the National Diagnosis Registry including diagnosis for all inpatients in Swedish hospitals from 1987 through 2002. Any errors, i.e. reported fractures that could not be verified from registry or records, were excluded and earlier episodes of fractures detected in the records but not registered in the questionnaire were corrected. Patients with fracture of the vertebra, pelvis, hip, ankle or wrist were classified according to the International Classification of Diseases (ICD-10).
Table 1. Comparison of mean age, sex, number and time since last fracture, marital status, education, walking aid, health variables, MMSE, medication and intensity, frequency, duration, location and relief of pain, between fractured in pain, fractured with no or mild pain and controls without pain or with mild pain
Variables that might be associated with or affect limitation of activity were examined through a questionnaire; this included age, sex, marital status, education, co-morbidity, cognitive function, medication and walking aid indoors and outdoors. Walking aid referred to any use of a walking stick, crutch or zimmer frame. To discover any cognitive impairment, a Minimal Mental State Examination (MMSE) was carried out (Folstein et al. Citation1975) ().
Questions were also asked about alcohol consumption, smoking habits, occupation, and physical activity at home and leisure time. Alcohol habits were divided into teetotaler, intake last month, and intake last year. Mean alcohol consumption in grams was calculated. Smoking habits were categorized as current smoker, former smoker or nonsmoker and duration of smoking was asked for. Occupation was referred to as gainfully employed, on sick leave, or housework/retired. The physical activity at work and during leisure time was divided into the following four categories: light, medium, heavy, or very heavy.
Pain
In subjects with fracture and controls without fracture, those with one episode of little pain or with no pain in the previous month were defined as being without pain. Subjects with fracture had to have had more than one episode of moderate or more severe pain in the previous month to be included amongst those with pain.
The participants completed an extensive questionnaire covering questions about pain, including treatment of pain and the degree of pain relief. To assess relief of pain after treatment, a visual analog scale with a range from 0% to 100% was used. The answers were categorized as 100% relief or more than 50% relief. Treatment referred to medication with painkillers or use of painkillers in combination with other treatment(s) such as physiotherapy ().
Physical tests
Activity tests included performance test and handgrip strength. Before testing, the participants were given firm instructions on how to perform the tests and they were accomplished under the supervision of a trained registered nurse. Participants were randomly divided between the nurses, and to control for any differences in the results due to interobserver variation in the physical tests, comparisons between observers were performed. ANOVA analysis did not show any significant differences in registration between observers.
Walking speed
Walking 30 m with flying start, including one turn at 15 m, at maximal and self-selected speed in a hospital corridor. Walking aid was permitted and time was measured after one 15 m and two 15-m walks. The test was performed once. There are several methods to test walking speed, but regardless of the method walking speed measurements are considered to be highly reliable among both healthy individuals and patients (Bramell-Risberg et al. Citation2005). Reliability expressed as intraclass correlation has become common, and several studies have reported high ICC for walking tests. For walking 2 × 15 m with one turn, ICC = 0.90–0.99 (Jarnlo and Nordell Citation2003). Flansbjer et al. (Citation2005) reported an ICC = 0.94 for walking 10 m at comfortable speed and ICC = 0.97 for walking 10 m at maximum speed.
Timed Get-Up-and-Go (TUG)
The participant rose from an armless chair with a seat height of 43 cm, walked 3 m and then turned around, returned to the chair and sat down. The test was performed at maximum and self-selected walking speed. The time from leaving the chair back until being seated again was measured. The participants wore ordinary shoes and walking aids were permitted. The test was performed once.
In earlier studies (Steffen et al. Citation2002) with repeated measurements within the same test situation, TUG has shown high test-retest reliability (ICC = 0.97). In another study, Podsialdo and Richardson (Citation1991) reported excellent intra- and inter-reliability (ICC = 0.99). High intraclass reliability (ICC = 0.96) has also been shown in a study by Flansbjer et al. (Citation2005), and Morris et al. (Citation2001) reported high inter-rater reliability of measurements for both experienced and inexperienced raters (ICC = 0.87–0.99).
Handgrip strength
Grip strength was measured with the Grippit (Nordenskiöld and Grimby Citation1993, Hammer and Lindmark Citation2003), which is a gauge for electronic measurement of the handgrip force. The participant squeezes a grip with maximum force, alternating with left and right hand. The grip consists of an elliptical handle 45 mm in depth and 27 mm wide. To standardize the measuring procedure, the grip handle and the forearm support are fixed on a wooden board. The elbow joint of the tested side is in 90o of flexion and the other hand rests on the table. The participants sit in an upright position in front of the device, with both feet at the same level on the floor. The same chair was used for all participants (Hammer and Lindmark Citation2003). The test was performed twice for both left and right hand, and the mean value was taken.
Statistics
Any differences between observers in registration of physical performance were tested with ANOVA adjusted for age and sex. Results from the activity tests, walking 15 m and 2 × 15 m, TUG, and handgrip strength are given as medians and ranges. Differences in activity were analyzed with Kruskal-Wallis test or Mann-Whitney U-test when analyzing differences between fractured with and without pain respectively fractured with and without pain and controls.
Difference in distribution between the three groups with respect to sociodemographic data, lifestyle habits, walking without walking aid, comorbidity, medication and MMSE of <27 points, pain location, pain treatment and pain relief were tested by chi-square test. Difference in mean age, numbers of fractures, time since last fracture, alcohol consumption, and smoking duration were tested with ANOVA.
A multiple-regression model was constructed to analyze the association between the physical performance tests, walking 15 m and 2 × 15 m, TUG, and both fracture and pain, controlling for the potential confounding effects of age, sex, cardiovascular disease, respiratory disease, hip arthrosis, knee arthrosis and cognitive function. The independent variables excluding age were used as dummies.
In the statistical analyses, differences were considered significant if the p-value was <0.05. The data were analyzed using SPSS for Windows, version 11.5.
Results
Subject characteristics
Subject characteristics for the three groups showing no significant difference regarding age, sex, occupation, marital status, education, smoking and alcohol habits, physical activity at work or leisure time, co-morbidity or MMSE are given in (data on alcohol and smoking habits, activity at work or leisure time, and occupation are not shown). There was a difference between subjects with fracture and pain using a walking aid out of doors or indoors, compared to subjects with fracture but no pain and controls (p < 0.001).
Subjects with fracture and pain took more painkillers than subjects without pain and controls. In the control group, 11% used painkillers and the difference was significantly lower than those with fracture and pain (p < 0.001). In the patients with fracture and pain, about one-third had severe pain in the previous month. About half of the group reported pain every day, and the same proportion had experienced pain for one day or longer. The lower extremities were the most prevalent location of pain. The 2 groups with fracture were not significantly different regarding number of fractures and time since last fracture ().
Physical performance
Subjects with fracture and pain had slower walking speed than controls for all walking tests at selfselected and maximum speed, and TUG at selfselected and maximum speed. Likewise, handgrip strength was reduced for both the right and left hand in subjects with fracture and pain compared to controls ().
Table 2. Comparison of walking 15 m and 2 × 15 m at self-selected and maximal speed, Timed Get-Up-and-Go at self-selected and maximal speed, and maximal hand grip strength between fractured in pain, fractured without pain and controls without pain
Subjects with fracture and pain were also slower than subjects with fracture but no pain in all walking activities at self-selected and maximum speed, and TUG at self-selected and maximum speed. There was no difference in grip strength between the two groups with fracture. Subjects with fracture but no pain were slower than controls in walking 15 m at maximum speed, as well as in TUG at self-selected and maximum speed, but no significant differences could be found for walking 15 m at self-selected speed or 2 × 15 m at both maximum and self-selected speed. A subanalysis comparing 15 m of walking at self-selected speed between subjects with more than 50% pain relief and subjects with fracture and pain (with less than 50% relief) showed that those with less than 50% pain walked faster: median 13 sec compared to 19 sec (p = 0.001) for those with pain relief equal to or less than 50%.
To analyze the independent effects of fracture and pain and to adjust for possible confounders that might influence physical performance, especially walking performance, we examined the relation in a multiple regression model. The variables fracture and pain could independently explain variation of walking 15 m and 2 × 15 m, TUG at self-selected and maximum speed, and hand-grip strength for left and right hand, after adjustment for age, gender, hip arthrosis, knee arthrosis, cardiovascular disease, pulmonary disease and cognitive function (MMSE) (). The variables hip arthrosis, knee arthrosis, cardiovascular disease, pulmonary disease, and cognitive function did not show significant ß-values in any regression model, except for hip arthrosis when TUG at maximum speed was used as dependent variable (data not shown).
Table 3. Multiple linear regression analysis predicting walking ability and, respectively, Timed-Get-Up-and-Go TUG including all the independent variables age, gender, fracture, pain, hip arthrosis, knee arthrosis, cardiovascular disease, respiratory disease, and cognitive function
Time since last fracture
Higher walking speed was noted for subjects with last fracture more than 3 years previously, as compared to subjects with a fracture less than 3 years previously for the groups both with and without pain (). The proportion without pain was not significantly different between individuals with fracture less than three years previously and those with fracture 3 or more years previously.
Table 4. Comparison of walking 15 m and 2 × 15 m at self-selected and maximal speed between groups fractured in pain and fractured without pain, divided into subgroups fractured less than 3 years ago and fractured 3 years ago or more
Discussion
The inclusion criteria for cases were that they should have had at least one fracture of either the vertebra, hip, pelvis or ankle—fractures that often are associated with reduced bone mineral density. Thus, the inclusion criteria did not require that cases should have a reduced bone density as in osteoporosis, but it is most likely that the majority of the fractures were osteoporosis-related due to the advanced age of the study population and also the high age since the last fracture (Karlsson et al. Citation1993). The types of osteoporosis-related fractures were chosen with the intention that they might influence walking performance, and fractures of the radius were therefore not included.
Even though cases who received hospital treat-of the vertebral fractures were given outpatient ment were identified through the National Diagno-care—and thereby not identified. But even so, sis Registry, there may have been a risk that some there is no reason to believe that these participants would not have been evenly distributed among the 3 studied groups, although a fracture is a risk factor for additional fractures. However, the number of fractures was no different between the two fractured groups.
We found that pain was related to reduced performance in physical tests, and pain might have been be one reason for not showing up for a medical examination at the research center. To avoid the possibility that subjects with fractures would decline participation due to pain, they were offered examination at home. Yet there may still have been subjects with fractures who were not able to participate, and who, if included, would have contributed to even greater differences in the physical tests. The physical tests done when visiting the participant at home included TUG at self-selected and maximum speed.
The participants were asked questions about the pain they had experienced in the previous month, and any loss of memory could bias the report. However, the Minimal Mental State examination (MMSE) that was carried out showed no significant differences between the groups. When one considers earlier results on self-selected speed for healthy men and women in the 60–80-year age range, our results for healthy controls are consistent with these previous studies (Bohannon Citation1997, Steffen Citation2002). One weakness, though, when comparing data on walking performance is that the test situation and methodology vary between the tests, and a comparison of data should only be done when the conditions are similar. Bohannon (Citation1997) timed the walking speed for subjects walking 7.62 m (25 feet) while in our study the participants walked 15 m.
One major goal in the rehabilitation of patients suffering from osteoporosis-related fractures is that they should return to their prefracture ambulatory status as soon as possible. Pain during the rehabilitation and after a fracture is common—and one reason why the recovery process might slow down. It is often followed by avoidance of mobility. Our study showed that among those subjects with fractures and in pain, as many as three-quarters underwent some kind of pain treatment, but none were totally without pain and only one-fifth reported more than 50% pain relief.
In the group whose fractures had happened less than 3 years previously, with a mean time to past fracture of 1.8 years, slightly more than one-half reported moderate to severe pain and as many as one-half had some kind of official or private help to manage their personal care or daily chores at home. Thus, in patients with a recent fracture there appears to be a need for better pain treatment and rehabilitation to reduce dependency on external help in managing everyday physical activities.
Functional training for 6–8 weeks has been shown to be a safe and effective method to increase performance such as walking and TUG after hip fracture, and prolonged training is recommended to avoid detraining effects such as atrophy (Hauer et al. Citation2002). This can be interpreted as a possible route to rehabilitation regarding walking performance in individuals with recent fracture.
Apart from pain, the fracture itself was shown to have a negative effect on walking speed. Subjects without pain and who had suffered a fracture 3 or more years previously performed better than those who had suffered a fracture less than 3 years previously. Possible causes for a slower walking speed in the “fractured” group without pain, and less than 3 years since the last fracture, might be atrophy due to prolonged bed rest or inactivity, leading to reduced muscle strength and an impaired balance with postural sway (Sharrington and Lord Citation1998, Janssen et al. Citation2004)—mechanisms that could explain the finding that shorter time to fracture was related to impaired physical function, irrespective of pain. Furthermore, reduced postural and vestibular functions in combination with weak muscular strength have been postulated to be determinants of fracture risk (Kristinsdottir et al. Citation2000).
Gait and balance impairments are predictors of falling, and elderly individuals who fall have been found to have a slower walking speed than individuals who do not fall (Davis et al. Citation1999, Kressig et al. Citation2001). Thus, there is also a possibility that reduced walking speed and balance even before the fracture may partly explain the results of the walking test, as well as the cause of the fracture. Another explanation for slow walking in subjects in general is fear of falling. Fear of falling due to an earlier fall is common, and often results in limited mobility and slower walking speed (Maki Citation1997, Edwards and Lee Citation1998, Ingemarsson et al. Citation2000, Brouwer et al. Citation2004). However, we have no reason to believe that there was an uneven distribution of subjects who were afraid of falling in the subgroups that incurred fractures less than 3 years previously or 3 years or more previously.
The ability to walk has proven to be a useful measure of activity, and limitations in walking ability have in turn been shown to cause restrictions in ordinary life (Guralnik et al. Citation1994, Citation2001)—often leading to reduced quality of life and (in the long run) the need for institutionalized care (Sernbo and Johnell Citation1993, Guralnik et al. Citation1995). Earlier studies have also presented results suggesting that limitation in activity due to illness or disability is associated with reduced independence and thus an increased dependency on others (Gignac Citation2000, Hirvensalo et al. Citation2000, Wang Citation2004).
Our findings suggest that there is rehabilitation potential during the first year after fracture and lack of pain is of great importance when recovering from fracture. One question that must be addressed, however, is whether limitation of physical activity affects life in general—leading among other things to a restriction in social participation.
The project Good Aging in Skåne, part of the Swedish National Study on Ageing and Care (www.snac.org) was supported by the Swedish Ministry of Health and Social Affairs, by Region Skåne, by the Medical Faculty of Lund University, and by the Vårdal Institute.
- Bohannon R. Comfortable and maximum walking speed of adults 20-79 years: reference values and determinants. Age Ageing 1997; 26: 15–9
- Bramell-Risberg E, Jarnlo G, Minthon l, Elmståhl S. Lower speeds in older women with dementia compared to controls. Dement Geriatr Cogn Disord 2005; 20: 298–305
- Brouwer B, Musselman K, Culham E. Physical function and health status among seniors with and without a fear of falling. Gerontology 2004; 50(3)135–41
- Davis J W, Ross P D, Nevitt M C, Wasnich R D. Risk factors for falls and for serious injuries on falling among older Japanese women in Hawaii. J Am Geriat Soc 1999; 47: 792–8
- Edwards B J, Lee S. Gait disorders and falls in a retirement home: A pilot study. Ann Long-Term Care 1998; 6: 140–3
- Flansbjer U B, Holmbäck A M, Downham D, Patten C, Lexell J. Reliability of gait performance tests in men and women with hemipares after stroke. J Rehabil Med 2005; 37: 75–82
- Folstein M F, Folstein S E, McHugh P R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12(3)189–98
- Gignac M A M. Adaptation to chronic illness and disability and Its relationship to perceptions of independence and dependence. J Gerontol B Psychol Sci Soc Sci 2000; 55(6)362–72
- Grafe I A, Da Fonseca K, Hillmeier J, Meeder P-J, Libicher M, Nöldge G, Bardenheuer H, Pyerin W, Basler L, Weiss C, Taylor R S, Nawroth P, Kaspark C. Reducton of pain and frsacture incidence after kyphoplasty: 1-year outcomes of a prospective controlled trail of patients with primary osteoporosis. Osteoporos Int Aug 3, 2005, (Epub ahead of print)
- Guralnik J M, Simonsick E M, Ferrucci L, Glynn R J, Berkman L F, Blazer D G, Scherr P A, Wallace R B. A short physical performance battery assessing lower extremities function: Association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 1994; 49(2)M 85–M 94
- Guralnik J M, Ferrucci L, Simonsick E M, Salive M E, Wallace R B. Lower-extremity function in persons over age of 70 years as a predictor of subsequent disability. N Engl J Med 1995; 2: 556–61
- Guralnik J M, Ferrucci L, Balfour J L, Volpato S, Di Iorio A. Progressive versus catastrophic loss of the ability to walk: implications for the prevention of mobility loss. J Am Geriatr Soc 2001; 49: 1463–70
- Hammer A, Lindmark B. Test-retest intra-rater reliability of grip force in patients with stroke. J Rehabil Med 2003; 35: 189–94
- Hauer K, Specht N, Schuler M, Bärtsch P, Oster P. Intensive physical traning in geriatric patients after servere falls and hip surgery. Age Ageing 2002; 31: 49–57
- Hirvensalo M, Rantanen T, Heikkinen E. Mobility difficulties and physical activity as predictors of mortality and loss of independence in the community-living older population. J Am Geriatr Soc 2000; 48: 493–8
- Ingemarsson A H, Frandin K, Hellstrom K, Rundgren A. Balance function and fall-related efficacy in patients with newly operated hip fracture. Clin Rehabil 2000; 14(5)497–505
- Janssen H C, Samson M M, Meeuwsen I B, Duursma S A, Verhaar H J. Strength, mobility and falling in women referred to a geriatric outpatient clinic. Aging Clin Exp Res 2004; 16(2)122–5
- Jarnlo G B, Nordell E. Reliability of the modified figure of eight-a performance test for elderly women. Physiother Theory Pract 2003; 19: 35–43
- Karlsson M K, Johnell O, Nilsson B E, Sernbo I, Obrant K. Bone mineral mass in hip fracture patients. Bone 1993; 14: 161–5
- Kressig R W, Wolf S L, Sattin R W, O'Grady M, Greenspan A, Curns A, Kutner M. Associations of demographic, functional, and behavioral characteristics with activity related fear of falling among older adults transitioning to frailty. J Am Geriatr Soc. 2001; 49(11)1456–62
- Kristinsdottir E K, Jarnlo G B, Magnusson M. Asymmetric vestibular function in the elderly might be a significant contributor to hip fractures. Scand J Rehabil Med 2000; 32(2)56–60
- Lagergren M, Fratiglioni I, Hallberg I R, Berglund J, Elmståhl S, Hagberg B, Holst G, Rennemark M, Sjölund B M, Thorslund M, Wiberg I, Winblad B, Wimo A. A longitudinal study integrating population, care and social services data. The Swedish National study on Aging and Care (SNAC). Aging Clin Exp Res 2004; 16(2)158–68
- Maki B E. Gait changes in older adults: predictors of falls or indicators of fear. J Am Geriatr Soc 1997; 45(3)313–20
- Morris S, Morris M E, Iansek R. Reliability of measurements obtained with the Timed “Up & Go” test in people with Parkinson disease. Phys Ther 2001; 81(2)810–8
- Nevalainen T H, Hiltunen L A, Jalovaara P. Functional ability after hip fracture among patients home dwelling at the time of fracture. Cent Eur J Public Health 2004; 12(4)211–6
- Nordenskiöld U M, Grimby G. Grip force in patients with rheumatoid arthritis and fibromyalgia and in healthy subjects. A study with the grippit instrument. Scand J Rehabil Med 1993; 30: 113–9
- Osnes E K, Lifthus C M, Meyer H E, Falch J A, Nordsletten L, Cappelen I, Kristiansen I S. Consequences of hip fracture on activities of daily abd residential needs. Osteoporos Int 2004; 15(7)567–74
- Podsialdo D, Richardson S. The timed “Up & Go”: A test of basic functional mobility for frail elderly ersons. J Am Geriatr Soc 1991; 39: 142–8
- Sernbo I, Johnell O. Consequences of a hip fracture: a prospective study over 1 year. Osteoporosis Int 1993; 3: 148–53
- Sherrington C, Lord S R. Increased prevalence of fall risk factors in older people following hip fracture. Gerontology 1998; 44(6)340–4
- Steffen T M, Hacker T A, Mollinger L. Age and genderrelated test performance in community-dwelling elderly people: Six-minute walk test, Berg Balance Scale, Timed Up & Go Test and Gait Speeds. Phys Ther 2002; 82: 128–37
- Theander E, Jarnlo G-B, Orstein E, Karlsson K. Activities of daily living decrease simillary in hospital.treated patients with a hip or a vertebral fracture: a one–year prospective study in 151 patients. Scan J Public Health 2004; 32: 356–60
- Wang P P. Activity limitation, coping efficacy and self-perceived physical independence in people with disability. Disabil Rehabil 2004; 26(13)785–93