
Abstract
Purpose
To examine the effect of a communication intervention package on expressive communication and visual attention in individuals with Rett syndrome.
Materials and methods
A modified withdrawal (A-B1-A1-B2-A2) single case experimental design with a direct inter-subject replication across three participants was applied. Three women with Rett syndrome participated. The study took place over a six-week period and comprised 32 sessions with each participant. All sessions were video recorded. During the intervention the communication partner used aided language modelling on a gaze-controlled device in combination with using responsive partner strategies. Expressive communication was assessed as synthesised words per minute and unique synthesised words per minute. Visual attention was assessed as rate of focused gazes (1 s or longer) in interaction.
Results
An intervention effect was found on the rate of unique words for all participants. The rate of words increased for two participants when the intervention was introduced but no withdrawal effect could be seen. An intervention effect on visual attention could be seen for one participant. The intervention appeared to have social validity as reported by caregivers.
Conclusion
Aided language modelling (ALM), while using responsive partner strategies and a gaze-controlled device may be used with adult individuals with Rett syndrome to increase their rate of expressive communication. Detailed observational measures revealed individual learning patterns, which may provide clinically valuable insights.
Adults with Rett syndrome may benefit from access to gaze-controlled devices in combination with responsive partner strategies.
Responsive partner communication may be effective for some individuals with Rett syndrome to increase their rate of synthesised utterances.
Rate of focused gazes may be considered as an outcome measure for individuals with oculomotor difficulties when introducing aided language modelling.
Implications for Rehabilitation
Introduction
Communication comprises several functions, such as obtaining social closeness, making requests, making comments or providing information. These functions can be expressed with language or with non-linguistic communication. In 2014, the American National Joint Committee for the Communication Needs of Persons with Severe Disabilities (NJC) presented the revised Communication Bill of Rights in a paper seeking to provide guidance for service and support to individuals with severe disabilities [Citation1]. The committee proposed that the aim should be to use a variety of communicative functions and provide a vocabulary that meets communication needs in several situations. Based on expert consensus, guidelines for communication in Rett syndrome also emphasise the value of a robust vocabulary (i.e., vocabulary for a range of communicative functions, settings and activities) [Citation2]. These guidelines cover numerous aspects of management of communication in Rett syndrome including Augmentative and Alternative Communication (AAC). Specific techniques that the experts agreed could be used in interventions included Aided Language Modelling (ALM), responsive partner strategies, expansions and recasts.
The essential component of ALM is that the partner points at picture symbols while speaking [Citation3,Citation4]. The aim is to support language development by helping the AAC learner to connect the symbol to its meaning. Previous studies of ALM interventions have included participants with autism and developmental delays. The results have been positive regarding various aspects of language and communication, such as turn taking, word comprehension and expression, length and complexity of utterances [Citation5–8]. However, few replications have been conducted across studies and participants, measures and procedures vary between studies. Research is also still needed to confirm the impact of ALM on specific diagnostic groups. The majority of the studies of ALM have included individuals who were able to select target symbols by pointing at them and several of the participants also used gestures to communicate. To our knowledge, only one individual who used alternative symbol selection methods has participated in a study investigating ALM [Citation9]. The ALM studies also often include other strategies, such as responsive partner strategies, which may have mediated the outcome to an as yet unknown extent [Citation3,Citation10].
Responsive partner strategies are considered foundational to development in several respects, for example as a mediating factor for increased communicative and linguistic development of children with little or no speech [Citation11–14]. Examples of responsive partner strategies include providing time for responses, looking for potential communicative actions and responding accordingly [Citation15,Citation16]. Expansions and recasts may also be used which means that the communication partner responds and rewords the AAC user’s communication at a slightly more complex level aiming at developing more complex language [Citation17,Citation18].
Earlier research on ALM and responsive partner strategies is thus limited in terms of participants with significant motor and communicative disabilities such as Rett syndrome. This is a rare disorder that affects approximately 1/9000 to 1/10 000 new-born girls [Citation19,Citation20]. The prevalence for males is not known as the disorder almost exclusively affects females. Diagnostic criteria include regression in acquired motor skills, spoken words and/or babbling. This regression most commonly occurs between 12 and 18 months of age [Citation21]. A mutation in the MECP2 gene often confirms the diagnosis [Citation22]. Although motor function varies in those with Rett syndrome, latency, altered muscle tone, stereotypies and dyspraxia hinder execution and timing of communicative behaviours [Citation2,Citation23]. Most individuals are non-speaking and only a small group rely on signs or gestures to communicate [Citation23,Citation24]. Other features of Rett syndrome and co-existing conditions are also reported to impact communication. These include breathing difficulties and fatigue or reduced alertness. Seizures are commonly occurring [Citation25].
Eye gaze is the most commonly reported communication form for individuals with Rett syndrome [Citation24,Citation26] and when communication aids are used, eye gaze is often the most feasible access option. However, some individuals may experience difficulties with oculomotor control [Citation2]. Moreover, delay in gaze shifts or immature patterns have been reported in earlier studies [Citation27,Citation28]. Gaze duration is reported to be shorter and focused gazes less frequent [Citation29,Citation30]. In a study by Fabio et al. [Citation29], individuals with Rett syndrome spent more time looking at items that were irrelevant to the task or looking at no specific stimuli at all. They also had fewer immediate shifts of gaze focus between the partner and objects. In conclusion, although some individuals with Rett syndrome show difficulties with controlling their eye gaze, it is still an important communication form. It is also an important means to access communication aids as soon as fine motor difficulties limit the variety and complexity of their communication [Citation2].
Eye-gaze technology allows individuals to control a computer through the eye gaze. The gaze-controlled device tracks the movement of the user’s eyes through infra-red cameras. The user can activate an item on the screen by fixating their eyes for a pre-set time on an item (i.e., dwell time). The dwell time must be short enough for the user to be able to hold the fixation to activate the button, yet long enough to not accidentally activate a button [Citation31]. The gaze-controlled device is calibrated for each user’s eyes. For the eye-gaze technology to function properly, the eyes need to be positioned approximately 60 cm from the device.
Previous research shows that gaze-controlled devices can enable assessments of cognitive skills in individuals with Rett syndrome [Citation32,Citation33]. In two survey studies, parents and speech language pathologists (SLPs) reported positive experiences of gaze-controlled devices as a means of communicating for individuals with Rett syndrome [Citation34,Citation35]. Vessoyan et al. [Citation36] reported a series of case studies including four girls with Rett syndrome that aimed to explore how the participants used eye-tracking technology for communication purposes. The outcome measure was Goal Attainment Scaling (GAS) [37] which was also used as a component of the intervention. The strategies used to reach the goals were only loosely described but responsive partner strategies were given as examples. Although the design did not allow for any firm conclusion, three of the four participants achieved a minimal clinically important difference. The intervention appeared to have social validity, i.e., it was socially important and appropriate, which is an important aspect of any support provided [Citation38].
There is clinical consensus on a range of practices and on developing a wider range of communicative functions for individuals with Rett syndrome [Citation2]. The evidence for one of these practices, i.e., ALM, is promising in terms of improving communication skills in individuals with developmental disabilities [Citation3]. However, research is still needed to evaluate if ALM is effective for individuals with Rett syndrome. Moreover, few of the published studies included adults.
The aim of this study was to examine the effect of a communication intervention package on expressive communication and visual attention in individuals diagnosed with Rett syndrome. More specifically, the aims were to examine the effect of Aided Language Modelling (ALM) whilst using responsive partner strategies and a gaze-controlled device, on the participants’ rate of synthesised words per minute, unique synthesised words per minute and visual attention.
Methods
This study complied with the Single-Case Reporting guideline In BEhavioural interventions (SCRIBE) [Citation39].
Research design
A modified withdrawal single case experimental design (A-B1-A1-B2-A2) was used with a direct inter-subject replication for three participants (see ).
Figure 1. Study phases. See Intervention section for details.

In total, 32 sessions were conducted with each participant and the interventionist over a six-week period. To minimise disruption on everyday life (including travel time) the participants attended two sessions on each study day. For practical reasons, each phase involved a pre-set number of sessions. The baseline phase (A) was comprised of six sessions, the withdrawal phases (A1 and A2) were comprised of five sessions while each intervention phase (B1 and B2) were comprised of eight sessions. The sessions lasted between 15–41 min and data from the whole session was included in the analysis (see Procedures).
Participants
Three women diagnosed with Rett syndrome participated in the study. They were recruited through the national family association in conjunction with a centre that specialises in the diagnosis. Convenience sampling was used i.e., only women living within one hour’s travel of the study site were included. Inclusion criteria were a) 18 years of age or above, b) reported to have functional vision and hearing based on caregiver reports, c) no daily use of a gaze-controlled device for communicative purposes, d) not communicating through speech, e) having an interest in social interaction, and f) demonstrating at least some interest in computer or tablet computer screens as reported by caregivers. All participants were dependent on assistance for most of their daily activities. Pseudonyms have been used throughout to protect participant confidentiality. The study included adult participants mainly for methodological reasons as adults are less likely to have other ongoing interventions e.g., from school.
Participant assessments
Ambulatory status was assessed by an external physiotherapist based on caregiver reports using the Modified Hoffer Scale [Citation40] (). The scale’s five levels of ambulatory status range from Community ambulators (level I) to Non-Ambulant (level V). Fine motor skills were assessed by an external occupational therapist based on caregiver reports and video observation (). The levels of the Rett Syndrome Hand Function Scale [Citation41] range from No grasping ability present (level 1) to Able to pick up small objects using a precise pincer grip and to transfer objects from one hand to the other (level 8). The Communication Matrix [Citation42,Citation43] based on caregiver reports was used to obtain an overview assessment of the participants’ communicative skills before the study. Seven levels of expressive communication behaviour are described for nine communicative functions. The seven levels are: (I) pre-intentional behaviour, (II) intentional behaviour, (III) unconventional pre-symbolic communication, (IV) conventional pre-symbolic communication, (V) concrete symbols, (VI) abstract symbols and (VII) language.
Table 1. Participant characteristics.
Prior to the study, the caregiver described the signs they were interpreting to estimate whether the participant’s general health was “better than usual”, “as usual”, or “worse than usual”. Before the first session each study day, the caregiver used a form in which these participant-specific descriptions were used as operationalisations to rate whether the general health of the participant was “better than usual”, “as usual” or “worse than usual”. The participants’ communication and signs of different general health status are described below. For a detailed description of participant characteristics, see .
Diana
Diana, 31 years old, used body movements, sounds and facial expressions to refuse objects and actions and sometimes used sounds to draw attention to herself. Her most common communication form was to look at objects and persons in order to request more actions, objects and attention, as well as to choose. She also looked back and forth between an object and person to draw attention to something. She used a yes/no signal (blinking/moving head to the side) relatively consistently, although the signals could be difficult for non-familiar communication partners to interpret. She also used photos, objects or abstract symbols to request or choose objects and actions that were absent. Moreover, photos, objects or abstract symbols were sometimes used to label things or people and to comment. Diana had been exposed to a low-tech communication book and aided language modelling for about three years before the beginning of the study. She had also been using a gaze-controlled device, mainly for games for a couple of years by the time of the study. However, she was dependent on her communication partners to provide access to relevant symbols and did not use her device to communicate on a daily basis. When her general health was “better than usual” she was described as responding quickly, being alert and able to concentrate. When it was “as usual” she was described as being interested but needing more time to respond. Finally when her general health was “worse than usual” she was described as being tired, not being able to participate, hyperventilating, turning her eyes to the ceiling or closing her eyes more often, and that her eyelids dropped. She suffered from exotropia, i.e., one or both eyes are turned outward, and was reported to switch between her eyes when looking at objects.
Karen
Karen, 27 years old, used facial expressions and body movements to refuse objects and actions, albeit rarely. Her most common communication form was to look at objects and persons to request more of an action, objects or attention, as well as to choose. She looked at symbols for yes/no, which was more pronounced in familiar situations. She requested or chose objects and actions that were absent and sometimes named things, people or activities through photos, objects or some abstract symbols. She had intermittently been exposed to low-tech communication boards and cards but did not have any specific low-tech system. She had a gaze-controlled device which she mostly used for games, although it also contained a symbol and photo-based application that was mainly used to talk about people and to discuss her daily schedule. She was dependent on her communication partners to provide access to relevant symbols and did not use her device on a daily basis. When her general health was “better than usual” she was described as being alert, using her gaze actively, and laughing a lot. When “as usual” she was described as being quiet and looking at what was going on around her, and as being interested in events in the environment. When her state was “worse than usual” she made a specific sound and did not pay attention to events in her environment. In particular when she was low on energy, it was difficult for her to stay awake and she easily fell asleep when “nothing was going on”. She was observed during the sessions as having a distinct gaze and quick gaze shifts.
Sarah
Sarah, 29 years old, used body movements, simple hand gestures (pushing away), sounds and facial expressions to refuse or request present objects and ongoing actions. She sometimes used sounds to draw attention to herself. She used photos and a few abstract symbols for choice making and, in a few situations when asked, chose from two symbols to comment. She inconsistently and very rarely used spoken words. She looked at symbols for yes/no, although inconsistently and less often in unfamiliar situations and environments. A couple of years before the study, she received a gaze-controlled device that she used for playing games and for choice making. In her “as usual” general health state she was described as having quick mood swings and quickly becoming dissatisfied. When “better than usual” she was described as being alert, happy, curious and in a stable mood, and when “worse than usual” (often after a seizure) she was described as being tired, very dissatisfied or only satisfied when resting.
Setting
All sessions took place at a specialist centre for assistive technology and AAC. The participants and the interventionist (i.e., communication partner) sat at a table in a room with few competing stimuli. One person, familiar with the participant, was present in the room but was instructed not to take part in the interaction.
Measures
Rate of synthesised words per minute
To assess the rate of synthesised words, the words that the participants expressed using the gaze-controlled device in each session were counted. When a word was repeated within four seconds, without gaze shifts in between, it was classified as a repetition and not included. The coding was performed from the video-recorded session, and the words spoken with the gaze-controlled device were noted in a table along with the time point at which the synthesised message was finished with a precision of a hundredth of a second. Finally, the total rate was divided by the minutes of the session.
Rate of unique synthesised words per minute
The rate of the unique synthesised words was assessed by counting the number of unique words from the table of words described above during each session. Finally, the total rate was divided by the minutes of the session.
Visual attention
To assess visual attention, the rate of focused gazes was recorded using Assessment of Visual Attention in Interaction (AVAI) [Citation44]. This tool was specifically developed to assess visual attention in individuals with Rett syndrome when using AAC with a communication partner during interactions in clinical settings. Focused gazes are operationalised in AVAI as gaze fixations that last for one second or longer. In a previous study, the tool had acceptable reliability (κ = 0.79–0.86) [Citation37,Citation44]. The coding of the video-recorded sessions in the present study was carried out using video editing software (described below). Identification of gaze shifts was carried out by placing a marker at each onset of the target action on the timeline in the software. For each marker, a notation of the gaze focus was made. As soon as the gaze was shifted from the communication partner, an object or the symbol set, a marker was placed with the notation: “gaze without any specific focus”. Once the coding was complete, the markers and notations for each clip were exported into a spreadsheet showing when the marker was placed (minutes, seconds, hundredths of a second) and the categorisation of gaze focus. A total visual attention score consisting of a rate per minute of all focused gaze types was used as a dependent measure in the current study.
Equipment
A set of vocabulary was used that was specifically designed for the study. The vocabulary consisted of pages with core words such as “more”, “finished” and “I”, pages for comments such as “good”, “fantastic” and “boring”, and activity specific pages. Each page consisted of 15 Picture Communication Symbols (PCS)1 including buttons for navigating to other pages. The vocabulary was programmed in a gaze-controlled device (Tobii I12+2) and the communication software used was Communicator 53.
For the activities during the sessions, games, books that are regularly used during assessments, as well as the participants’ own books and games, were used. A tablet computer (iPad™) with game apps, music and video clips was also used during the sessions. The material was chosen according to the participant’s reported interests as well as what they showed special interest in during the sessions.
A Panasonic HCx9201™ video camera was used for video recording of the setting (i.e., the table, participant and interventionist) during data collection and a Sony HC22E™ camera was used for video recording the screen of the gaze-controlled device. The coding of the recorded interactions was carried out using the video editing software Adobe Premiere Pro CC3™.
Interventions
The overall study phases are presented in . The interventionist was an AAC educational specialist with many years of training and experience in responsive partner strategies and aided language modelling (ALM). The person had extensive experience of working with individuals who use AAC to communicate and was not part of the research team. The same person acted as interventionist with all three participants.
Baseline phase
All sessions including the baseline phase (A) comprised of interaction in motivating activities. Responsive partner strategies [Citation15] were used (including pacing the communication, giving space to communicate, attending to and confirming the participants’ expressions in any modality) in all five phases. Responsive partner strategies are considered foundational for AAC-supported interaction and it was considered unethical to omit responsive partner strategies in any of the phases. The gaze-controlled device was placed within the participant’s field of vision, slightly to the side and accessible to the participant. Track status was used to check that the participant’s eyes could be tracked accurately by the gaze-controlled device before each session and when considered necessary during sessions. The dwell time (the length of time the user needs to focus his/her gaze to activate a choice on the screen) was set at 1 s. This dwell time was estimated to ensure that the symbols would not be activated accidentally but that the buttons would be able to activate for the participants.
Intervention phases
In the intervention phases (B1 and B2), the interventionist used aided language modelling (ALM) i.e., pointed at symbols on the computer screen approximately twice each minute while speaking. There were no specific target words. The interventionist was instructed to use the activity pages corresponding to the current activity, and to navigate to other pages when appropriate for the conversation, a minimum of five times per session. In addition, an individually adjusted dwell time was introduced in the first intervention phase. The dwell time for each individual was estimated during a session before the baseline (see Procedures). An individualised dwell time was chosen to ensure that the symbols could be selected with little effort from each participant.
Withdrawal phases
In the modified withdrawal phases (A1 and A2), ALM was not used but responsive partner strategies and an individualised dwell time were still kept. It was deemed that withdrawal of the individually set dwell time would possibly cause frustration and it was therefore not considered to comply with the ethical regulation.
Procedure
Before the baseline session (A), the primary investigator met the participants in their homes. A calibration of the gaze-controlled device was made. A training page-set was used to ensure that the participants could access all buttons on the screen and to estimate the individualised dwell time. On the same occasion, a caregiver was interviewed to obtain information about participant’s characteristics, i.e., day-to-day communication using the Communication Matrix [Citation43], and signs of different levels of general health status as described earlier. After the last session, the primary investigator informally interviewed the caregivers and carers present at the intervention to explore social validity. The open questions covered their general impression of the intervention and whether they noticed any differences at home that they related to participating in the study. The answers were noted in writing.
The data collection took place over approximately 30 days for each participant. For practical reasons there was a ten-day break for each participant. Two sessions per day were conducted and between the sessions, the participants and their caretakers were encouraged to engage in any preferred restorative activity, such as going for a walk. Each session was recorded with two video cameras, see Equipment, above. The recording started as soon as the participant and interventionist were seated, and ended when the activities were terminated. Each session lasted 20–30 min. The length of the session depended on the interest of the participant as judged by the interventionist. A minimum of 20 min was set which was considered to provide the participants with enough time to become engaged and communicate, given possible fluctuations in alertness, latency and dyspraxia. Once the participant showed little interest after 20 min had passed, the interventionist ended the session.
Inter-rater reliability
The primary investigator coded all the video-recorded sessions. Inter-rater agreement (IRA) was calculated for 22% of the clips (N = 21). The video clips were selected through stratified random sampling (selected from each participant and study phase). The video clips were coded in a random order by an external coder with experience of assessing individuals with motor and communication disabilities. The external coder had no information about which phase the clips were selected from.
Ethical approval
This study obtained ethical approval from the Regional Ethical Review Board (Dnr 2018/079) and ethical regulations and guidelines complied with Swedish law. The caregivers and the interventionist were instructed to be attentive to any displays of discomfort inflicted by the situation. In such cases, the activity was changed, or the session would be terminated. The participants’ guardians were given written information about the confidentiality of the study and gave their written informed consent on behalf of the participants. The guardians were informed that they were free to withdraw on behalf of the participants at any stage without any adverse consequences.
Statistical analyses
The rate of synthesised words and the rate of unique synthesised words for each session were converted into a rate per minute and the rate of focused gazes was calculated by adding all focused gazes on the communication partner, an object and the symbol set (i.e., the gaze-controlled device). The results were plotted on a graph and visually analysed for trend levels and variability within and across phases following the procedure outlined in Lane and Gast [Citation45]. Effect size was calculated using Tau-U since this method controls for positive baseline trends [Citation46] which were present in several of the baseline phases. A Tau-U score of 0–0.20 is considered to indicate a small effect, 0.21–0.60 is considered a moderate effect and 0.61–1.0 is considered a large effect [Citation47].
Kappa was used to assess IRA for synthesised words and unique synthesised words and IntraClass Correlation (ICC) was used to assess IRA for visual attention. A 2-way mixed model, single rater and absolute agreement ICC was used [Citation48]. The calculator available on the website single-caseresearch.org was used to calculate Tau-U scores. SPSS version 25.0 was used for all IRA analyses.
Results
Graphs for all the three outcome measures throughout the phases for the participants are shown in . Most trends are variable, and all participants show a pattern of rates that varies every two sessions. Calculations for assessing data variability, trend directions and level changes throughout the phases and per participant [Citation45] can be found in Supplement 1. Tau-U data are presented in . For all participants, there were occasions when the eye-gaze technology did not seem to work optimally, despite acceptable calibrations and the use of track status to check that the device was positioned well. This appeared to be frustrating for the participants. Otherwise, no adverse events were reported related to participation in the study.
Figure 2. Synthesised words per minute expressed by Diana. Between session 16 and 17 there was a ten-day break. The dotted line = median score.
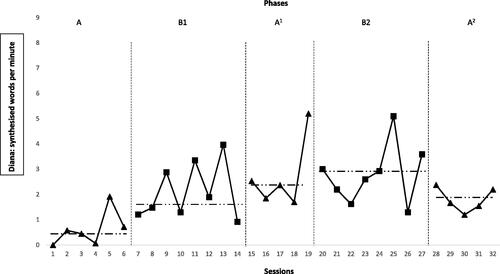
Figure 3. Unique synthesised words per minute expressed by Diana. Between session 16 and 17 there was a ten-day break. The dotted line = median score.
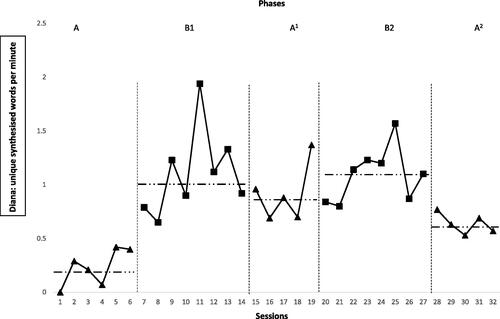
Figure 4. Rate of Diana’s focused gazes. Between session 16 and 17 there was a ten-day break. The dotted line = median score.
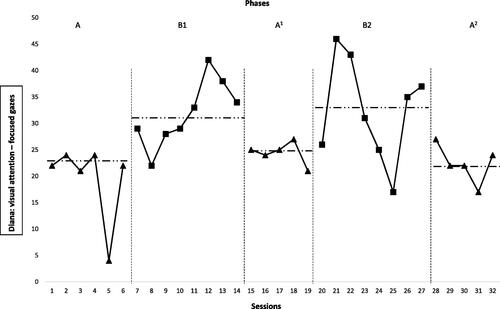
Figure 5. Synthesised words per minute expressed by Karen. Between session 16 and 17 there was a ten-day break. The dotted line = median score.
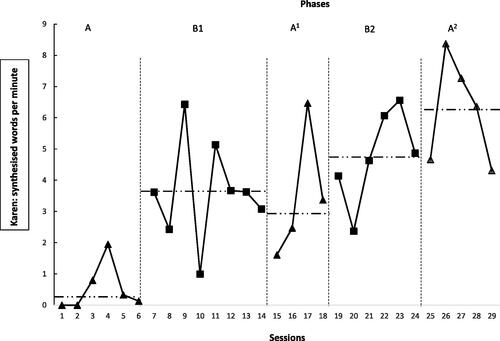
Figure 6. Unique synthesised words per minute expressed by Karen. Between session 16 and 17 there was a ten-day break. The dotted line = median score.
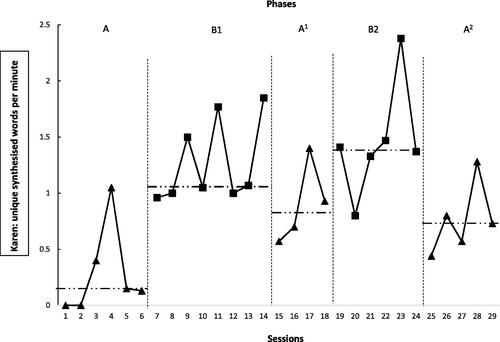
Figure 7. Rate of Karen’s focused gazes. Between session 16 and 17 there was a ten-day break. The dotted line = median score.
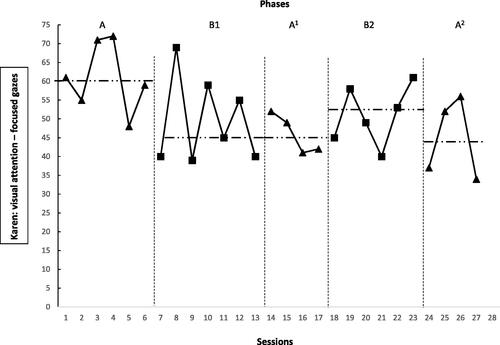
Figure 8. Synthesised words per minute expressed by Sarah. Between session 10 and 11 there was a ten-day break. The dotted line = median score.
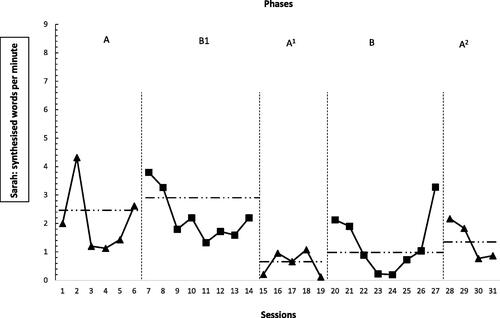
Figure 9. Unique synthesised words per minute expressed by Sarah. Between session 10 and 11 there was a ten-day break. The dotted line = median score.
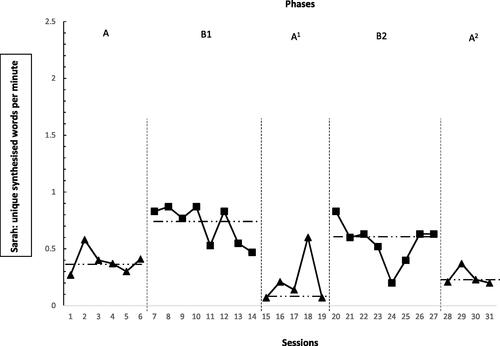
Figure 10. Rate of Sarah’s focused gazes. Between session 10 and 11 there was a ten-day break. The dotted line = median score.
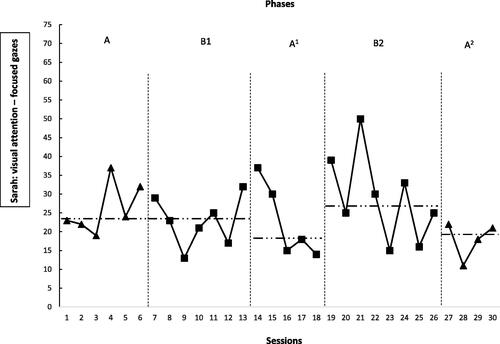
Table 2. Tau-U across all phases and Tau-U comparing phase A and B1.
Diana
Rate of synthesised words per minute
The baseline was variable and had an accelerating trend. There was a large intervention effect from the baseline (A) to Phase B1. No effect from ALM alone could be seen between A1 and B2. The rate then decreased from the intervention Phase B2 to Phase A2 when ALM was not used, thus indicating a large withdrawal effect. There was a moderate intervention effect in all phases. (See ).
Rate of unique synthesised words per minute
The baseline (A) was variable and had an accelerating trend. The rate of unique synthesised words increased from the baseline phase to Phase B1 when ALM and an individualised dwell time were introduced. Visual inspection did not reveal a clear withdrawal effect when ALM was not used in Phase A1. However, there was a moderate effect when ALM was re-introduced in Phase B2 and the rate decreased in Phase A2 when ALM was not used, thus indicating that there was a withdrawal effect. The overall effect size was large (See ).
Rate of focused gazes
The baseline was stable and flat. The rate of focused gazes increased when ALM and an individualised dwell time were introduced in Phase B1 and decreased in Phase A1 when ALM was not used. When ALM was re-introduced, there was a moderate intervention effect and in the last phase when ALM was not used the rate decreased, demonstrating that there was an effect from ALM on Diana’s rate of focused gazes. The overall effect size was large (See ).
Additional results
Diana’s general health was rated to be “as usual” prior to 30 of the sessions and “worse than usual” prior to two of the sessions. Her general health or the ten-day break was not reflected in the rate of the dependent measures. The dwell time was set at 770 milliseconds for the first four intervention sessions and at 500 milliseconds for the remaining sessions. The dwell time was decreased because at times she appeared to fixate on symbols on the screen without being able to activate the symbol button. In the interview after the last baseline session, the caregiver’s perception was that the carers who were present during the sessions subsequently used the gaze-controlled device more often at home and that they had learnt how to support aided communication better by observing the sessions. The family and carers appreciated that Diana’s aided expressive communication had increased. Diana, who was present during part of the informal interview, used her gaze-controlled device to initiate a request for more symbols.
Karen
Rate of synthesised words per minute
The baseline (A) was variable and had an accelerating trend. There was a large effect from ALM and an individualised dwell time. No withdrawal effect could be seen in Phase A1 when ALM was not used. The rate of aided words per minute increased even further in the second intervention phase when ALM was used and in the last phase when it was not. There was no reversal effect and no effect from ALM alone on Karen’s rate of aided words per minute. The overall effect size was moderate (See ).
Rate of unique synthesised words per minute
The baseline was variable and had an accelerating trend. There was a large effect when ALM and an individualised dwell time were introduced. There was no clear withdrawal effect in Phase A1 when ALM was not used. However, the rate increased (Tau-U = 0.50) when ALM was re-introduced again in Phase B2 and decreased in Phase A2 when ALM was not used. This therefore indicated that there was an effect from ALM. The overall effect size was large (See ).
Rate of focused gazes
The baseline (A) was stable with a decelerating trend. The rate decreased, contrary to the expected direction, when ALM and an individualised dwell time were introduced in Phase B1. There was no difference between B1 and A1, hence no withdrawal effect could be shown. The rate increased when ALM was re-introduced in Phase B2 and decreased when ALM was not used in Phase A2. However, none of the changes were significant (at the .05 level). The overall effect size was small (See ).
Additional results
Karen’s general health was rated to be “better than usual” prior to 26 of the sessions, “as usual” prior to four sessions and “worse than usual” prior to two sessions. Due to technical errors, three datapoints are missing for Karen (one from Phase A1 and two from Phase B2). Two of these sessions occurred when Karen’s general health was worse than usual. The dwell time was set at 800 milliseconds for the first intervention session and then remained the same throughout the study. In the informal interview after the intervention, the caregiver reported that Karen generally was more alert. She did not fall asleep as often and she generally used her gaze more actively. The caregiver reported that they had also learnt to support the aided communication better by observing the sessions, for example by using responsive partner strategies. Both the caregiver and the carers where Karen lived also used the gaze-controlled device more often in conversations with Karen.
Sarah
Rate of synthesised words per minute
The baseline (A) trend was stable and had a decelerating trend. There was no intervention effect and displays a pattern of high rates during the first two phases and then a quick decrease during Phase A1. This level remained for the last three phases. The overall effect size was moderate (See ).
Rate of unique synthesised words per minute
The baseline (A) was variable and had an accelerating trend. ALM and an individualised dwell time in combination (B1) influenced Sarah’s rate of different synthesised words per minute. The rate increased in Phase B1 (Tau-U = 0.88) and a withdrawal effect was demonstrated in Phase A1 and A2 when ALM was not used. The overall effect size was large (See ).
Rate of focused gazes
The baseline (A) was variable and had an accelerating trend. There was no effect on visual attention when ALM and an individualised dwell time were introduced. A small difference in median levels were seen with slightly higher rates during Phase B2 when ALM was used, compared with the adjacent phases when ALM was not used. The overall effect size was moderate (See ).
Additional results
Sarah could sometimes use her hands to point at the communication symbols and reject or reach for objects. Sarah’s general health was rated to be “better than usual” prior to 20 sessions, “as usual” prior to nine sessions and “worse than usual” prior to two sessions. Her general health did not correspond to the rate of the dependent measures. Due to illness, Sarah’s participation was delayed and only four sessions were completed during Phase A2. The dwell time was set at 800 milliseconds for the first intervention session and then remained the same throughout the study. In the informal interview after the last session, Sarah’s caregiver stated that Sarah had been in a very good mood during the study days.
Treatment fidelity
The Responsive Augmentative and Alternative Communication Style Scale (RAACS) Version 3 [Citation15], originally developed for assessing parents’ communicative styles with children with communication difficulties, was used to assess the interventionist’s responsiveness as a measure of treatment integrity. The coding procedure is described in more detail in a different publication [Citation49]. Based on earlier studies of responsivity, a threshold was set at a score of 15. The interventionist’s RAACS score was above this pre-set threshold in all 96 sessions.
To check the rate of ALM (twice per minute), all the interventionist’s aided language models were transcribed and the rate per minute for each session was calculated. The average rate was 2.26 models per minute during the intervention sessions (range = 1.06–3.13). In 25% of the intervention sessions the rate of ALM did not reach two models per minute, for example when the participant used the gaze-controlled device frequently. For the following events, the instructions were not adhered to: in two withdrawal sessions the interventionist pointed at the screen once by mistake. In one withdrawal session when the participant showed signs of discomfort, the interventionist navigated to a page with vocabulary for expressing wants and needs.
Inter-rater agreement (IRA)
Agreement between the two coders for synthesised words was κ = .91, (p < .001) and for unique synthesised words it was κ = .99, p < .001 which can be interpreted as almost perfect agreement. Regarding visual attention, the ICC for the partner was .78, p < .001, 95% CI [.74, .82], for objects .90, p < .001, 95% CI [.87, .91], and for symbols .88, p < .001, 95% CI [.86, .90]. The ICC values thus indicate good reliability.
Discussion
The current study aimed to examine the effect of a communication intervention package on expressive communication and visual attention in individuals diagnosed with Rett syndrome. The results were mixed in that they did not show a clear intervention effect in all dependent variables, i.e., rate of synthesised words, rate of unique synthesised words and visual attention (rate of focused gazes) in all three participants. However, all three participants increased their rate of expressive communication in at least one aspect. Individual learning patterns were revealed through the detailed measures, which may provide clinically valuable insights.
Rate of synthesised words per minute
For Karen and Diana, the individual dwell time in combination with ALM had a large effect on the rate of words in B1 compared to the baseline. Chen et al. [Citation31] emphasise the importance of monitoring the dwell time and recommend a dwell time of as short as 0.5 s. The individualised dwell time thus enabled Karen and Diana to access the computer. The lack of stable withdrawal effects for Diana and Karen may reflect that their behaviour repertoire was expanded and generalised and therefore not highly sensitive to the withdrawal of ALM. Responsive partner strategies and access to the gaze-controlled device alone seemed to be effective for increasing the rate of synthesised utterances.
For Sarah, the intervention did not have any effect at all on the rate of synthesised words. This may be explained by her communicative profile. She had a larger repertoire of unaided communicative forms, such as reaching towards objects to request, and did not communicate to provide and seek information including commenting, according to the Communication Matrix assessment [Citation42,Citation43]. A large part of the interventionist’s responses to Sarah’s synthesised utterances were comments or were otherwise information-based. These responses were potentially not effective enough to keep the rate at a higher level throughout the phases. Sarah was also able to request and reject present objects and activities through body movements and hand gestures and may have preferred that mode.
Rate of unique synthesised words per minute
ALM had an effect on the rate of unique synthesised words, i.e., the variation of synthesised expressions, for all participants. ALM included the interventionist navigating to new pages. Even though the participants sometimes spontaneously navigated to new pages, ALM provided more page turns which provided them access to a more varied vocabulary, and may also have drawn attention to new symbols that were relevant for the activity or topic. A larger variation of utterances that the communication partner can recast, expand and map meaning to potentially results in a more linguistically stimulating environment [Citation17].
Visual attention
The intervention had a large effect on Diana’s rate of focused gazes but no effect on the other two participants’ visual attention. One possible explanation is that the outcome measure is more sensitive for individuals that have difficulties to shift gaze focus. Diana had more difficulties with eye motor control than the other participants, partly due to exotropia. In a pilot study including a small group of women diagnosed with Rett syndrome, the rate of focused gazes was higher when the communication partner used aided language modelling [Citation44]. Although the results from these two studies can not be generalised due to small groups, it may be important to assess and evaluate visual attention when introducing aided communication.
General discussion
Using the gaze-controlled device may in itself be reinforcing, and responsive partner strategies may also reinforce any communicative attempt. This could explain the lack of withdrawal effect when ALM was not used. For ethical reasons, it was not deemed to be feasible to withdraw either the responsive partner strategies or the individualised dwell time. Within the design of the current study, it was not possible to establish the degree to which ALM alone, or ALM and the individualised dwell time combined, contributed to the increased rate of synthesised communication.
Although not measured systematically, the participants appeared to be frustrated when the gaze control did not work well. Access to symbolic communication and responsive partner strategies may increase potential communicative behaviours and thus increase active participation in conversations. Previous research indicates that ALM has an impact on language acquisition [Citation6,Citation50]. However, this was not a focus in the current study.
The detailed assessment revealed information about individual variations that could be of clinical value. The phase-trend patterns varied between the participants and for Diana and Karen, whose rates of words increased across both intervention phases, it would have been of interest to further examine specific functions and linguistic goals. For Sarah, it may be of interest to assess more thoroughly the communication partner responses that would influence her aided communication.
To hold social validity, the goals of an intervention should have social significance, the procedures should be socially appropriate, and the effects of the intervention should be socially important [Citation38]. Although social validity was not included in the aims of this study and data pertaining to it was not collected in a structured way, the responses in the informal interview indicate that the intervention and the procedures were appreciated by the caregivers and carers. They also perceived that the sessions were appreciated by the participants. The reports that the carers used the eye-gaze device for communication purposes more often after the study, and perceived that they had learnt to support aided communication better, are important for long-term implementation.
To the best of our knowledge, this is the first experimental intervention study of aided language modelling (ALM) for adults with Rett syndrome. The intervention was the same for all three participants and the training period relatively short. Although there are limitations (discussed below), all three participants increased their rate of at least one of the targeted outcome areas. This highlights the potential for positive communication development even for adults and thus the need for intervention for adults with Rett syndrome. It would be valuable to conduct further studies which span over an even longer time-period, and also include teaching and training for the primary communication partners in responsive strategies and ALM. It would also be important to learn more about responsive communication partner strategies as these strategies are combined with the use of ALM in several studies, including this study. Finally, it would be of interest to study whether synthesised communication increases the rate of the communication partner’s responses.
Limitations
A number of limitations should be considered when interpreting the results of this study. Data was highly variable, and the results fluctuated between the first and second sessions of the day. Potential explanations for this are that it is tiring to use gaze-controlled devices [Citation51,Citation52] and performance is generally highly variable in individuals with Rett syndrome [Citation2]. Information on the general health status of the day was gathered, however this was not for each session, which would have been useful.
The variability in phase trends indicates that each phase could possibly be longer to reach stability. However, it should also be considered that longer study phases may also cause strain on the participants, for example due to travel and disrupted daily schedules.
Generally, there was a large effect between the baseline phase and the first intervention phase. However, the experimental control between Phase A and the intervention phases was not complete as the participants started the study at the same time. A multiple baseline design would have been necessary to rule out confounders such as maturation and factors in the everyday environment that could have influenced the result. Factors in the everyday environment were unlikely to be confounders as the participants did not live in the same place or visit the same day care centres. Neither is maturation a probable confounder considering the short time frame. Additionally, the ten-day break did not appear to influence the result. Possible confounders that remain are factors related to the interventionist and the setting. Even though treatment fidelity was checked, there is a possibility that unknown factors relating to the interventionist style or the setting may have influenced the results.
The participants’ receptive language was not assessed and may thus have influenced the results to some extent. Although recent studies indicate that eye-gaze technology is a promising way to test cognitive functions [Citation32,Citation33], less than half of the participants completed the test procedure in one of the studies [Citation33].
The caregivers reported that the participants were given the opportunity to use the eye-gaze technology more often during the study period. While this strengthens the social validity, it is also a potential confounder. It should also be pointed out that social validity data was only collected through informal interviews. Future studies should collect data more systematically, for example through a questionnaire [Citation38].
Conclusions
Aided language modelling (ALM), while using responsive partner strategies and a gaze-controlled device may be used with adult individuals with Rett syndrome to increase their rate of expressive communication. All participants increased their expressive communication in at least one aspect, highlighting the need for intervention options for adults. Furthermore, detailed observational measures revealed individual learning patterns, which may provide clinically valuable insights. Considering the life-long need for communication support for individuals with Rett syndrome, and the paucity of research in the area, further communication intervention studies are crucial for this group.
Supplement_1_Analysis_Lane_Gast_revised_clean.docx
Download MS Word (49 KB)Acknowledgements
The authors wish to thank the participants and their caregivers, the interventionist and everyone who helped in the recruitment process. We would also like to thank the external coder who assisted in the inter-rater reliability process; Kajsa Skytt, Östersund city council. Thanks also to Lisa Cockette for language checking.
Disclosure statement
The authors report no conflicts of interest. This study is a part of the first author’s doctoral dissertation.
Additional information
Funding
References
- Brady NC, Bruce S, Goldman A, et al. Communication services and supports for individuals with severe disabilities: guidance for assessment and intervention. Am J Intellect Dev Disabil. 2016;121(2):121–138.
- Townend GS, Bartolotta TE, Urbanowicz A, et al. Development of consensus-based guidelines for managing communication of individuals with Rett syndrome. Augment Altern Commun. 2020;36(2):71–81.
- Sennott S, Light JC, McNaughton D. AAC modeling intervention research review. Res Pract Persons Severe Disabil. 2016;41(2):101–115.
- Allen AA, Schlosser RW, Brock KL, et al. The effectiveness of aided augmented input techniques for persons with developmental disabilities: a systematic review. Augment Altern Commun. 2017;33(3):149–159.
- Binger C, Berens J, Kent-Walsh J, et al. The effects of aided AAC interventions on AAC use, speech, and symbolic gestures. Semin Speech Lang. 2008;29(2):101–111.
- Dada S, Alant E. The effect of aided language stimulation on vocabulary acquisition in children with little or no functional speech. Am J Speech Lang Pathol. 2009;18(1):50–64.
- Bruno J, Trembath D. Use of aided language stimulation to improve syntactic performance during a weeklong intervention program. Augment Altern Commun. 2006;22(4):300–313.
- Kent-Walsh J, Binger C, Buchanan C. Teaching children who use augmentative and alternative communication to ask inverted yes/no questions using aided modeling. Am J Speech Lang Pathol. 2015;24(2):222–236.
- Flores JL. Examining aided input intervention in a classroom setting for children labeled with significant disabilities [electronic theses and dissertations]. University of Northern Iowa; 2016.
- Biggs EE, Carter EW, Gilson CB. Systematic review of interventions involving aided AAC modeling for children with complex communication needs. Am J Intellect Dev Disabil. 2018;123(5):443–473.
- Haebig E, McDuffie A, Ellis Weismer S. Brief report: parent verbal responsiveness and language development in toddlers on the autism spectrum. J Autism Dev Disord. 2013;43(9):2218–2227.
- Karaaslan O, Mahoney G. Mediational analyses of the effects of responsive teaching on the developmental functioning of preschool children with disabilities. J Early Interv. 2015;37(4):286–299.
- Madigan S, Wade M, Plamondon A, et al. Birth weight variability and language development: risk, resilience, and responsive parenting. J Pediatr Psychol. 2015;40(9):869–877.
- Warren SF, Brady NC. The role of maternal responsivity in the development of children with intellectual disabilities. Ment Retard Dev Disabil Res Rev. 2007;13(4):330–338.
- Broberg M, Ferm U, Thunberg G. Measuring responsive style in parents who use AAC with their children: development and evaluation of a new instrument. Augment Altern Commun. 2012;28(4):243–253.
- Medeiros KF, Cress CJ. Differences in maternal responsive and directive behavior during free play with and without aided AAC. Augment Altern Commun. 2016;32(2):151–161.
- Cleave PL, Becker SD, Curran MK, et al. The efficacy of recasts in language intervention: a systematic review and meta-analysis. Am J Speech Lang Pathol. 2015;24(2):237–255.
- Soto G, Clarke M, Nelson K, et al. Recast type, repair, and spontaneous use of linguistic targets in AAC mediated interaction. J Child Lang. 2019;47(1):250–264.
- Fehr S, Bebbington A, Nassar N, et al. Trends in the diagnosis of Rett syndrome in Australia. Pediatr Res. 2011;70(3):313–319.
- Laurvick CL, de Klerk N, Bower C, et al. Rett syndrome in Australia: a review of the epidemiology. J Pediatr. 2006;148(3):347–352.
- Neul JL, Kaufmann WE, Glaze DG, et al. Rett syndrome: revised diagnostic criteria and nomenclature. Ann Neurol. 2010;68(6):944–950.
- Amir RE, Van den Veyver IB, Wan M, et al. Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat Genet. 1999;23(2):185–188.
- Urbanowicz A, Downs J, Girdler S, et al. An exploration of the use of eye gaze and gestures in females with Rett syndrome. J Speech Lang Hear Res. 2016;59(6):1373–1383.
- Didden R, Korzilius H, Smeets E, et al. Communication in individuals with Rett syndrome: an assessment of forms and functions. J Dev Phys Disabil. 2010;22(2):105–118.
- Glaze D, Percy A, Skinner S, et al. Epilepsy and the natural history of Rett syndrome. Neurology. 2010;74(11):909–912.
- Bartolotta TE, Zipp GP, Simpkins SD, et al. Communication skills in girls with Rett syndrome. Focus Autism Other Dev Disabl. 2011;26(1):15–24.
- Rose SA, Djukic A, Jankowski JJ, et al. Rett syndrome: an eye-tracking study of attention and recognition memory. Dev Med Child Neurol. 2013;55(4):364–371.
- Tetzchner S, Jacobsen KH, Smith L, et al. Vision, cognition and developmental characteristics of girls and women with Rett syndrome. Dev Med Child Neurol. 1996;38(3):212–225.
- Fabio RA, Antonietti A, Castelli I, et al. Attention and communication in Rett syndrome. Res Autism Spectr Disord. 2009;3(2):329–335.
- Rose SA, Djukic A, Jankowski JJ, et al. Aspects of attention in Rett syndrome. Pediatr Neurol. 2016;57:22–28.
- Chen SHK, O'Leary M. Eye gaze 101: what speech-language pathologists should know about selecting eye gaze augmentative and alternative communication systems. Perspect ASHA Sigs. 2018;3(12):24–32.
- Ahonniska-Assa J, Polack O, Saraf E, et al. Assessing cognitive functioning in females with Rett syndrome by eye-tracking methodology. Eur J Paediatr Neurol. 2017;22(1):29–35.
- Clarkson T, LeBlanc J, DeGregorio G, et al. Adapting the mullen scales of early learning for a standardized measure of development in children with Rett syndrome. Intellect Dev Disabil. 2017;55(6):419–431.
- Townend GS, Marschik PB, Smeets E, et al. Eye gaze technology as a form of augmentative and alternative communication for individuals with Rett syndrome: experiences of families in The Netherlands. J Dev Phys Disabil. 2016;28(1):101–112.
- Wandin H, Lindberg P, Sonnander K. Communication intervention in Rett syndrome: a survey of speech language pathologists in swedish health services. Disabil Rehabil. 2015;37(15):1324–1333.
- Vessoyan K, Steckle G, Easton B, et al. Using eye-tracking technology for communication in Rett syndrome: perceptions of impact. Augment Altern Commun. 2018;34(3):230–241.
- Kiresuk T, Smith A, Cardillo J. Goal attainment scaling: applications, theory, and measurement. Hillsdale (NJ): Lawrence Erlbaum Associates; 1994.
- Ferguson JL, Cihon JH, Leaf JB, et al. Assessment of social validity trends in the journal of applied behavior analysis. Eur J Behav Anal. 2019;20(1):146–157.
- Tate RL, Perdices M, Rosenkoetter U, et al. Reprint of “the Single-Case reporting guideline in BEhavioural interventions (SCRIBE) 2016: explanation and elaboration. Pratiques Psychol. 2019;25(2):119–151.
- Vogel LC, Mendoza MM, C SJ, et al. Ambulation in children and youth with spinal cord injuries. J Spinal Cord Med. 2007;30(Suppl 1):S158–S164.
- Downs J, Bebbington A, Jacoby P, et al. Level of purposeful hand function as a marker of clinical severity in Rett syndrome. Dev Med Child Neurol. 2010;52(9):817–823.
- Rowland C, Fried-Oken M. Communication matrix: a clinical and research assessment tool targeting children with severe communication disorders. J Pediatr Rehabil Med. 2010;3(4):319–329.
- Rowland C. Communication matrix. rev. ed. Oregon: Design to Learn Projects; 2004. (University OHS, editor.).
- Wandin H, Lindberg P, Sonnander K. Development of a tool to assess visual attention in Rett syndrome: a pilot study. Augment Altern Commun. 2020;36(2):118–127.
- Lane JD, Gast D. Visual analysis in single case experimental design studies: brief review and guidelines. Neuropsychol Rehabil. 2014;24(3–4):445–463.
- Parker RI, Vannest KJ, Davis JL, et al. Combining nonoverlap and trend for single-case research: Tau-U. Behav Ther. 2011;42(2):284–299.
- Vannest KJ, Ninci J. Evaluating intervention effects in single‐case research designs. J Couns Dev. 2015;93(4):403–411.
- Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163.
- Wandin H, Lindberg P, Sonnander K. An exploratory case study of a trained communication partner’s use of responsive and scaffolding partner strategies in aided communication with adults with Rett syndrome. [work in progress].
- Binger C, Kent-Walsh J, Berens J, et al. Teaching latino parents to support the multi-symbol message productions of their children who require AAC. Augment Altern Commun. 2008;24(4):323–338.
- Borgestig M, Sandqvist J, Parsons R, et al. Eye gaze performance for children with severe physical impairments using gaze-based assistive technology-A longitudinal study. Assist Technol. 2016;28(2):93–102.
- Karlsson P, Allsop A, Dee-Price B-J, et al. Eye-gaze control technology for children, adolescents and adults with cerebral palsy with significant physical disability: findings from a systematic review. Dev Neurorehabil. 2018;21(8):497–505.