
ABSTRACT
Continuing medical education is essential to maintain and develop the skills of the healthcare workforce. Engagement with CME is required for maintaining practitioner licence in the United Arab Emirates. The CME environment in Abu Dhabi has been growing quickly, with rising numbers of activities and learner participation. Though Abu Dhabi’s Department of Health(DOH) has a history of regulating CME for its health professionals, it has typically relied on activity audits that have been inefficient and laborious. Consequently, the DOH evaluated and subsequently adopted international standards for provider accreditation and implemented a new model. That system incorporates eligibility standards, a digital system of registration, standards for ensuring learners are protected from advertising and promotion, expectations for educational outcomes, attendance verification, and program evaluation. DOH introduces an accreditation statement, set standards for activity documentation, data protection, and published a limited range of international systems whose credits could be recognized by DOH. Embedded in the new accreditation system is a restructured internal workforce, trained and supported to ensure accurate, consistent, and transparent accreditation decisions. DOH has supported implementation through a revised website, community meetings, provider training, and provider support services. DOH anticipates continuing evolution to support a culture of learning and competency management of the healthcare professionals in its workforce through CME, and in doing so support the delivery of high-quality healthcare to its citizens.
Introduction
Safe and effective clinical care is highly dependent on the complex array of skills being deployed by clinicians and healthcare teams. Their skills are highly determined by their engagement in high-quality training, initially as students in professional schools and training programmes, and subsequently maintained and further developed while in practice. Continuing professional development (CPD) has been shown to effectively improve the quality of clinical practice and, by extension, the quality of care and outcomes patients receive [Citation1].
CPD is growing. A recent study indicates that the global continuing medical education (CME) market value reached $8.24 billion in 2021 and is predicted to reach $11.98 billion by 2027, rising at a compound annual growth rate (CAGR) of over six percent between 2022 and 2027 [Citation2]. Similarly, the Accreditation Council for Continuing Medical Education (ACCME) reported that the number of recognised educational events and physician participation increased by 19% between 2020 and 2022 in the United States, with online learning and team-based educational activities continuing to expand [Citation3].
In this article, we will examine the present status of CME in the Emirate of Abu Dhabi and provide an overview of the system-wide evolution in CPD to meet the vision of Abu Dhabi’s healthcare needs.
History of CME and Its Regulation in Abu Dhabi
The Emirate of Abu Dhabi is the capital of the United Arab Emirates and collaborates with the Dubai Health Authority (DHA) and the Ministry of Health and Prevention (MOHAP) to regulate health professionals across the Emirates. Since 2011, the number of healthcare facilities in Abu Dhabi has increased at a compound annual growth rate of about 9.3%, and by the end of 2020, there were 3021 healthcare facilities licenced in Abu Dhabi. The healthcare workforce increased at a comparable rate, from 21,115 healthcare professionals in 2012 to 57,410 in 2021, with an annual growth rate of 10% [Citation4]. Hospitals, medical facilities, general and specialist clinics, and telemedicine services make up the Abu Dhabi healthcare sector. As the population ages and non-communicable chronic diseases, including cardiovascular and metabolic diseases, become more prevalent, the demand for specialised care services is anticipated to increase [Citation4]. In addition, public-private partnership models are becoming more prominent in Abu Dhabi’s healthcare industry, including becoming clinical sites for international healthcare organisations including Cleveland Clinic, Mayo Clinic, and Imperial College London, each of which has established successful clinical provision services in the Emirate [Citation5].
In parallel, the Abu Dhabi Medical Education System has been advancing over the past decade. Medical education regulation has evolved beyond its traditional undergraduate and graduate foundations to become a vital aspect of both clinical practice and the workforce planning agenda. The establishment of an undergraduate medical school (Khalifa University) and robust internationally affiliated postgraduate residency programmes has created a highly competitive and collaborative environment, resulting in a greater pool of physicians to fulfil the population’s healthcare demands. Similarly, and as a result of the implementation of a number of health professional regulatory frameworks, Continuous Medical Education, CME, is now a mandatory component of healthcare practitioner regulation in the Abu Dhabi health system [Citation6].
Since its establishment in 2000, the Department of Health (DOH) has adopted a progressive agenda for regulating and executing public policies in CME. In 2002, the General Authority of Healthcare Services, then known as DOH, formulated the CME Advisory Committee, which was responsible for overseeing CME requirements in clinical settings. Subsequently, in June 2004, a public policy mandating that all physicians and dentists must earn 50 CME credit hours annually in order to renew their registration or licence, the first policy of its sort in the United Arab Emirates [Citation7]. In 2007, the Department of Health established a CME department, and a new accreditation and quality control procedure was implemented. The accreditation standards include 12 criteria derived from ACCME’s standards [Citation8]. Over time and with experience, the accreditation system procedures progressively included audits of activities and made activity compliance determinations.
MOHAP, DHA and DOH together implemented the Professional Qualified Requirement (PQR) in 2017 as the country’s first unified credentialing and licencing standards. It also involved the maintenance of licencing requirements for all health professionals. Physicians must demonstrate participation in 40 credit hours per year of practice-based learning and development to keep their licences active. Similar requirements were imposed on nurses and allied health personnel (20 and 10 credit hours per year, respectively). Cross-accreditation recognition of CME activities between the regulators in the Emirates was also implemented.
Growth and Change Over Time
In recent years, the number of CME activities held in the emirate has expanded substantially (), particularly since continuing medical education has become a necessity for the renewal of licences and the credentialing of health professionals. Since its inception in 2005 and throughout the subsequent 15 years, the CME office at the DoH has demonstrated an increase in CME adoption with CME activities and the CME hours awarded (), a trend that was interrupted in 2020 and 2021 by the COVID-19 pandemic.
Figure 1. Data related to CME in Abu Dhabi. CME hours refers to the total number of hours awarded to all CME activities submitted and approved for accreditation by DOH.
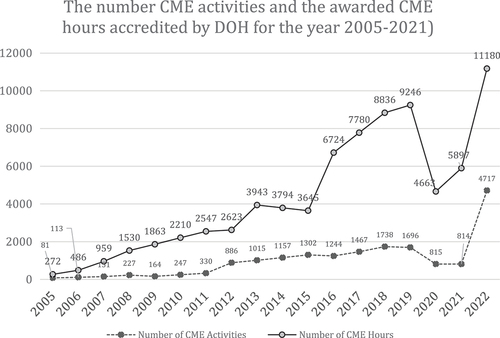
Considering the exceptional difficulties posed by the COVID-19 pandemic, it is evident that there has been a notable surge in the provision and engagement with CME initiatives within the realm of medical education in the year 2022, as has been seen elsewhere [Citation3]. The quantity of CME activities conducted exhibited an exceptional growth of 171% compared to the previous record high in preceding years. Additionally, there was a notable 21% increase in the number of CME hours between 2019 and 2022, indicating substantial engagement by health professionals in their own education, elaborated by the COVID pandemic, as well as their efforts to redesign learning environments to enhance the range of competencies offered within their organisation.
The trend of increased participation and provision of continuing medical education since the COVID-19 pandemic is still being evaluated, and it is premature to ascertain the precise reasons for this surge. One possible explanation is the wide adoption and acceptance of distance and remote learning modalities post COVID-19. This becomes even more appealing due to the fact that virtual platforms can be implemented at a reduced expense and with less logistical strain on both providers and learners.
A potential another rationale for a rise in activities may be attributed to the implementation of a new digital application system for CME accreditation by the DOH within the middle of 2021. The system is distinguished by its user-friendly electronic interface and multiple input fields with predefined navigation menus and options, that expedite the decision-making process for applications within a time frame of 12 minutes. Nonetheless, this trend requires additional research and analysis.
Challenges with Activity Audit as Strategy for Accountability
The DOH’s assessment of CME quality was limited to medical education activity audit visits. The target is to audit 5% of CME activities annually using random sampling. The site visit was done to make sure that the activity complied with the DOH accreditation standards. The eight elements that make up the audit methodology included activity objectives, identification of target audience, appropriate content and speakers, appropriate educational format, absence of promotion and advertisement, effective activity evaluation, attendance verification, and appropriate handling of any sponsorship and commercial support. Compliance with the requirements are graded [Citation9]. Review of those grades has demonstrated substantial national compliance.
From the perspective of the DOH, the current single-activity audit system necessitates a large staff to carry out the auditing procedures. For instance, between January 1st and 31 August 2022, DOH was able to conduct only 60 site audits. This was mainly due to the labour-intensive nature of the DOH audit operations system. Despite 60 audit visits, 37 percent (22 of 60) of the activities were cancelled or rescheduled, resulting in significant operational redundancy. It was evident that this audit system does not adequately serve the CME quality and does not provide providers with guidance to assist them in developing a high-level strategy and a common objective to enhance their CME vision.
Other than staffing, several additional obstacles pertain to activity audit that demonstrate the need for a system evolution. Lack of resources, such as insufficient time, personnel, financial resources, and practical resources, remains the greatest impediment to activity auditing. Auditors must have an appropriate management system for administering the audit schedule, coordinating communication, tracking visits, and monitoring results. The variety of CME providers, their knowledge of the CME activity development process, and the varying nature of CME programmes, such as online courses, conferences, workshops, and seminars, contribute to the lack of standardisation.
Goals for the CME System in Abu Dhabi
Several reports and systematic reviews outline the broad and consistent effectiveness of CPD in changing knowledge, skills, attitudes, and behaviours [Citation10,Citation11]. These findings have been repeatedly reinforced across the health professions, and replicated in other industries which leverage talent management and quality improvement to effect educationally induced change. However effective CME requires that educational organisations evolve to best strategies in learning design that focus on engaging clinicians in collaborative problem-solving that activates learners, facilitates peer norming, self-awareness, and practice-based change and team performance [Citation12,Citation13]. The continuing education infrastructure must connect with and drive towards strategic quality goals for healthcare in UAE. Achieving this goal requires educational providers and employers to develop an educational strategic plan for their hospital, clinic or society, and leverage curricula and learning management systems to track and manage the competencies of their employees [Citation14].
To be a trusted resource for healthcare professionals, CME must be protected from the influence of industry. As a regulator, we seek to create a safe space for learning that ensures healthcare professionals have access to effective learning experiences that are protected from being influenced by agencies that produce, market, resell, or distribute products consumed by or used on patients. This safe space gives learners the confidence that their CME/CPD is based on legitimate best practices, while clarifying to the organisations that provide commercial support to CME/CPD providers, the circumstances in which they can support accredited education, and where and when they can interact with healthcare professionals [Citation7].
Process of Accreditation for Educational Providers and Their Activities
The DOH is responsible for accrediting both CME providers and individual activities in Abu Dhabi. Providers are obligated to comply with a prescribed set of accreditation requirements to maintain their CME accreditation system access. The criteria ensure that CME activities are developed to be educationally robust, to present only valid content, provides a balance of the available diagnostic or treatment options, and are free from commercial influence. A systematic process must be adhered to by the provider in order to independently plan, evaluate, and enhance their continuing medical education (CME) activities over time, and demonstrate continuous improvement as a provider [Citation7].
The process typically involves the provider to submit to DOH application through centralised digital platform, providing detailed information about their CME activities, activities outline and learning objectives. The provider should have a system in place to handle various tasks involved in managing participants, collecting their feedback, track adequate participation, and issue their certificate of credits hours earned.
The provider is required to present all documentation pertaining to commercial support, which encompasses contractual agreements and sponsorships with commercial entities. It is imperative for speakers to provide comprehensive disclosure of their present and recent financial associations with commercial entities.
The DOH efficiently approves the CME activity accreditation application, and the CME registration code is issued following submission, contingent on the provider’s agreement of the comprehensive terms and conditions. Among these conditions are provisions that grant the DOH the authority to investigate providers, programmes, or activities at any time, and to suspend them if they fail to meet DOH accreditation or eligibility requirements.
Ensuring Accurate and Consistent Accreditation Decision-Making
DOH has maintained a staff dedicated to the oversight of the CME system and continues to do so. This staff has recently engaged in a variety of online training programmes and attended a variety of ACCME’s training courses. Case-based decision processing approaches have been used to build and maintain consistency decision-making. The staff leverage the digital registration system of activities to select materials and programmes for audit.
Driving for Quality and Effectiveness in CME
To drive towards best practices in learning and training and protect learners from promotion and marketing by industry, DOH decided to advance standards for eligibility for initial accreditation (including standards that exclude industry or those organisations that are contracted by industry from being recognised as educational providers) and deploy a provider accreditation system. DOH adopted standards for activity and provider accreditation based on the ability to identify educational needs, develop activities that could change behaviour or performance using appropriate design, and measure learning outcomes, consistent with the International Standards and ACCME [Citation8,Citation15]. DOH created expectations for disclosure of commercial relationships by planners and faculty and how those disclosures would be managed to protect the integrity of CME. Sponsorships of meetings and exhibits are to be regulated to ensure sponsors and exhibitors have no ability to influence the meeting, online or in person, guaranteeing an advertisement-free experience for learners who do not want to interact with industry during accredited activities. DOH also introduced an accreditation statement, and set standards for activity documentation, attendance records, and data protection. DOH identified a limited number of international systems whose credits could be recognised by DOH.
Supporting Implementation of New Standards
In addition to hiring and staffing for the accreditation activities, DOH undertook community meetings and focus groups to solicit feedback and develop final standards. Implementation included an online training programme, and several live meetings where standard templates were shared, and case examples were used. DOH established a centralised information technology infrastructure where recognised educational providers could register activities and then report learner completion and credit data in a centralised repository.
The DOH is implementing a retrospective audit based on sampled activities from a provider’s delivered activities. Organisations will have an opportunity to remediate standards that are not met, and if these expectations remain out of compliance the organisation can have restrictions placed on their ability to act as educational providers or lose their accreditation. These audits will account for the known heterogeneity among providers of varying sophistication in their deployment of learning activities. In pursuit of CME audit reform applicable to the current capacity, complexity and capabilities, the DOH has developed a collaborative with the ACCME to support the evolution of its governance competency and therefore the CME quality, educational outcomes and enhance participants’ engagement and learning outcomes.
Anticipating the Future
The delivery of effective healthcare in the Emirate of Abu Dhabi relies on engaging healthcare professionals in ongoing training and support so they can deliver optimal care to our population. DOH’s mission is to meet the needs of the public and the professions and ensure they can have access to and trust their education. We anticipate an increasing reliance of health professional portfolios where we can track and indeed manage individual educational goals and competencies, but this long-term vision will depend on the evolution of the skills and technical capacity of our accredited provider community, and we plan to invest in facilitating and enabling that capacity. Evolving the regulatory landscape will help this system move education away from a focus on compliance and instead augment the value of and promote the development of a culture of learning among our system’s most precious asset, its community of talented health professionals.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
References
- O’Brien MA T, Freemantle N, Oxman AD, et al. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2001(2):CD003030. doi: 10.1002/14651858.CD003030
- IMARC group. Continuing medical education (CME) market: global industry trends, share, size, growth, opportunity and forecast 2023-2028. 2022. (https://www.imarcgroup.com/continuing-medical-education-market).
- ACCME. ACCME Data Report. Renewal and growth in accredited continuing education - 2022. 2023. (https://www.accme.org/sites/default/files/2023-07/2022%20ACCME%20Annual%20Data%20Report%201003_20230713.pdf).
- Abu Dhabi Department of Health. Open Data Dashboards (https://www.doh.gov.ae/en/resources/opendata).
- Koornneef EJ, Robben PB, Al Seiari MB, et al. Health system reform in the emirate of Abu Dhabi, United Arab Emirates. Health Policy. 2012;108(2–3):115–6. doi: 10.1016/j.healthpol.2012.08.026
- Alameri H, Hamdy H, Sims D. Medical education in the United Arab Emirates: challenges and opportunities. Med Teach. 2021;43(6):625–632. doi: 10.1080/0142159X.2021.1908978
- Abu Dhabi Department of Health. Abu Dhabi CME Standards. (https://www.doh.gov.ae/en/programs-initiatives/meed/cme-program).
- ACCME. Standards for integrity and independence. (https://accme.org/accreditation-rules/standards-for-integrity-independence-accredited-ce).
- Abu Dhabi Department of Health. Medical Education Initiatives (https://www.doh.gov.ae/en/programs-initiatives/meed).
- Forsetlund L, Bjorndal A, Rashidian A, et al. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2009;2009(2):CD003030. doi: 10.1002/14651858.CD003030.pub2
- Rozensky RH, Grus CL, Fouad NA, et al. Twenty-five years of education in psychology and psychology in education. Am Psychol. 2017;72(8):791–807. doi: 10.1037/amp0000201
- Reeves S, Pelone F, Harrison R, et al. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6(6):CD000072. doi: 10.1002/14651858.CD000072.pub3
- O’Brien BC, Patel SR, Pearson M, et al. Twelve tips for delivering successful interprofessional case conferences. Med Teach. 2017;39(12):1214–1220. doi: 10.1080/0142159X.2017.1344353
- McMahon GT. What do I need to learn Today?–the evolution of CME. N Engl J Med. 2016;374(15):1403–1406. doi: 10.1056/NEJMp1515202
- Regnier K, Campbell C, Griebenow R, et al. Standards for substantive equivalency between continuing professional Development/continuing medical education (CPD/CME) accreditation systems. J Eur CME. 2021;10(1):1874644. doi: 10.1080/21614083.2021.1874644