
Abstract
Background: Driving under the influence (DUI) is a major cause of death and disability. Although a broad array of programs designed to curb DUI incidents are currently offered to both first-time and recidivist DUI offenders, existing evaluations of the effectiveness of these programs have reported mixed results. Objective: To synthesize the results of DUI program evaluations and determine the strength of the available evidence for reducing recidivism for different types of programs. Methods: A systematic review of all EBSCO databases, EMBASE, PubMed, ProQuest, Sociological Abstracts and TRIS was conducted to identify evaluations of treatments/interventions to prevent DUI offenses. Additional articles were identified from reference lists of relevant articles. Results: A total of 42 relevant studies were identified by the search strategy. Of these, 33 utilized non-experimental evaluation designs or reported insufficient data to allow effect sizes to be calculated, making meta-analysis unfeasible. Evaluations of several different program types reported evidence of some level of effectiveness. Conclusion: Because of the general lack of high quality evidence assessing the effectiveness of DUI prevention programs, it is not possible to make conclusive statements about the types of programs that are likely to be most effective. Nonetheless, there was some evidence to support the effectiveness of programs that utilize intensive supervision and education. There is a need for future evaluations to adopt more scientifically rigorous research designs to establish the effects of these programs.
Introduction
Driving under the influence (DUI) is a serious threat to public health and safety. Not only is there a personal risk to the driver, but driving while intoxicated also places others in danger. In 2002 alone, 242,900 people died worldwide from alcohol-related traffic accidents. Further, alcohol-related traffic accidents accounted for 7,447,200 disability adjusted life years (Citation1). Statistics such as these highlight the need to identify interventions that can reduce DUI. One of the most effective means to do this is to target known offenders. Recidivist DUI offenders are responsible for a substantial proportion of all offenses, and some studies have reported that nearly one in three known offenders will be re-arrested (Citation2). Further, it has been established that recidivist DUI offenders are more likely to persist in their DUI behavior than first-time offenders (Citation3,Citation4), particularly after any sanctions are removed (Citation5). Repeat offenders are also more deviant and have higher levels of substance abuse, psychiatric distress, and unemployment, than first time offenders, highlighting the range of factors that may need to be addressed in DUI prevention programs (Citation6). This paper aims to document the strength of evidence that is available to support the design and delivery of these programs.
In their meta-analysis of 215 remedial interventions for DUI offenses, Wells-Parker et al. (Citation7) reported a 7–9% reduction in DUI recidivism and alcohol related crashes as a result of program completion. They discovered larger effect sizes for combined interventions (education and psychotherapy/counselling) than for those that involved only one component. This analysis, however, was conducted almost two decades ago and since then many more evaluations of interventions have been undertaken and new approaches to prevention (such as ignition interlock technology) have been introduced. A 2001 review of DUI interventions evaluating the effects of community-based interventions on alcohol-related motor vehicle crash fatalities (Citation8) found strong support for the 0.08% blood alcohol concentration laws, minimum legal drinking age laws, and sobriety checkpoints. A second review evaluating multi-component programs from a community mobilization perspective (Citation9) concluded that reducing access to alcohol, responsible beverage service training, sobriety checkpoints, and education were effective in reducing alcohol related crashes. However, both of these studies focused on overall reductions in crash fatalities rather than on preventing recidivism and are thus more limited in scope.
The purpose of this paper then is to identify those programs that have been shown to have an impact on reducing DUI offenses and to assess the strength of the evidence underpinning their implementation. Knowledge about those programs that have been shown to work can be used by both policy makers to inform decisions about where to channel resources, and by communities to determine the types of program that are likely to prove the most effective in their local context.
Methods
A systematic review of the literature was conducted to identify relevant studies reporting on the effectiveness of DUI interventions.
Inclusion criteria
Papers were included if they met the following criteria: (i) the paper specifically discussed the evaluation of a DUI intervention for first-time or repeat drink driving offenders; (ii) the paper was peer reviewed; (iii) the full text was accessible; (iv) the outcome measure was based on recidivism or re-arrest; and (v) the paper had been published after the Wells-Parker et al. (Citation7) meta-analysis. Conference papers were considered for inclusion if they were located through the database searches and if a peer reviewed full text of the paper was available. Evaluation data was excluded if it was only available in reports and had not been through a peer-review process, or if this could not be established. While unpublished evaluation reports may be high quality, it is not possible to establish this in the absence of external independent review.
Literature search
A computer database search of all EBSCO databases, EMBASE, PubMed, ProQuest, Sociological Abstracts and Transport Research Information Services (TRIS) was conducted in addition to a Google Scholar search. Reference lists of relevant articles were examined for potentially pertinent articles. The key words used included drink driving, drunk driving, driving under the influence, DUI, driving while intoxicated, DWI, impaired driving, and driving while impaired, in combination with intervention, program and treatment. All keyword combinations were searched simultaneously in each of the databases.
Results
Classification of studies
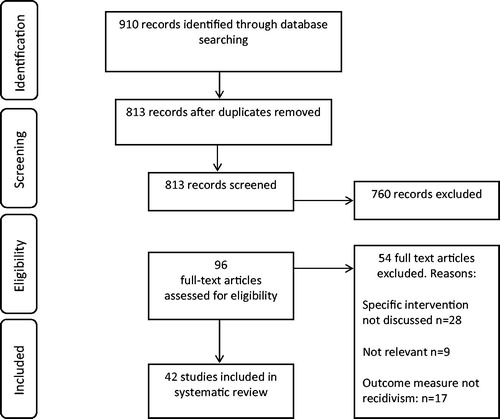
Titles and abstracts of 1610 articles were reviewed to determine if they met the inclusion criteria. After the initial abstract and title search, 96 articles were retained. Only those directly evaluating the effectiveness of interventions for DUI offenders were reviewed, resulting in 42 articles being included in the current study. A coder-comparison was conducted to ensure the inclusion criteria were met, which involved three of the authors reviewing all potential articles for inclusion. demonstrates the search strategy employed according to PRISMA guidelines (Citation10).
Figure 1. Flowchart of studies eligible for inclusion in the current review.
Each article was then summarized according to country of origin, the intervention population under consideration, the intervention type, the evaluation methodology employed, the outcome measures used, follow-up details and the findings. In addition the Maryland Scale for Scientific Rigor was used to determine the quality of the methodology employed (Citation11). The Maryland scale is a measure of the internal validity of scientific methods, which is scored from 1–5, with 1 being the poorest design. Level one of the Maryland Scale states that the level of evidence presented is a correlation between a crime prevention program and a measure of crime or crime risk factors at a single point in time. Level two is achieved if (a) there is a temporal sequence between the program and the crime or risk outcome clearly observed, or (b) a comparison group was used that did not have demonstrated comparability to the treatment group. Level three requires a comparison between two or more comparable units of analysis, one with and one without the program. To achieve level four, a comparison between multiple units with and without the program, controlling for other factors, or using comparison units that have only minor differences must be presented. To achieve level five there must be random assignment and analysis of comparable units to program and comparable groups.
The original intention in this study was to perform a meta-analysis of program evaluation outcomes. To do this, however, studies have to report effect sizes (or provide sufficient statistical information to allow the calculation of effect sizes or confidence intervals) (Citation12). Although some of the identified studies provided this type of data, many utilized different designs (e.g. another treatment type, control group, jail), which rendered them incomparable (Citation13). As such, meta-analysis of the type recommended in the PRISMA guidelines was not viable. Consequently, what is reported below is a systematic review of the literature and a synthesis of past results and conclusions. Further, only statistics which were available from the studies reviewed are reported in the current paper. An overview of each of the studies identified is provided in arranged according to rating of scientific rigor.
Table 1. Summary of articles evaluating DUI Interlock interventions.
Table 2. Summary of articles evaluating DUI education programs.
Table 3. Summary of articles evaluating VIP interventions.
Table 4. Summary of articles evaluating DUI Intensive Supervision Programs.
Table 5. Summary of articles evaluating DUI Drug Courts and other DUI intervention programs.
Study characteristics
The average sample size of the studies was 14,469 with the smallest study containing 63 participants (Citation14) and the largest comprising 204,182 (Citation15). Thirty three of the studies were conducted in the USA, five in Canada, three in Sweden, and one was conducted in Australia. Twenty five of the studies employed a quasi-experimental design, eight had an experimental design, seven had a retrospective design, and two were randomized control trials. Follow up periods ranged from immediately post-intervention through to 15 years post-intervention, and the most common outcome measure was another DUI offense in the time period specified by the authors. Three studies met the criteria for a level five rating on the Maryland scale, eight met the criteria for level four, 15 for level three, 14 for level two, and two met the criteria for level one.
Type of intervention and effectiveness
Ignition interlock
The ignition interlock is a device installed in a car which aims to prevent DUI offenses by requiring the driver’s blood alcohol concentration (BAC) level to be below a set limit, before allowing the car to start (Citation16). If the driver produces a BAC score over the limit, the ignition will lock and the car will be unable to be started. Eleven of the studies evaluated the use of an ignition interlock intervention (Citation17–27). Four of these studies found significant intervention effects of the ignition interlock device while installed and post-intervention (Citation17,Citation18,Citation20,Citation23), three of the studies reported effectiveness of the ignition interlock only while it was installed in the vehicle, with recidivism rates increasing once the device was removed (Citation19,Citation21,Citation22), three reported effectiveness while on the vehicle (Citation24,Citation26,Citation27), and one reported no difference in recidivism for those who voluntarily installed the interlock device and those for whom installation was mandatory (Citation25). For example, Roth et al. (Citation19) compared 1461 first time offenders, who were sentenced to install ignition interlocks for a period of six months, with 17,562 offenders who were convicted but did not have the ignition interlock system installed, over three periods between 2003 and 2005. The groups were compared while the interlock was on the vehicle, after the interlock was removed, and for the two periods combined. When the interlock was installed in the vehicle, the interlock group had a 60% lower recidivism rate than the control group (p < 0.0001), however once the interlock device was removed this difference in recidivism was no longer significant.
Education
Preventative education programs targeting DUI offenses are typically delivered after a person receives a DUI conviction. These programs often focus on increasing the awareness of the specific (e.g. physiological, cognitive, etc.) effects of alcohol/drug use on driving ability, as well as provide information and advice for changing DUI behavior (Citation28). As stand-alone education programs have previously been found to be ineffective, this approach is often included as a component of a larger intervention program (Citation29). Six studies focused on evaluating the impact of education programs on reducing DUI offenses (Citation29–34). Five studies demonstrated a reduction in DUI recidivism after the completion of the education program (Citation29,Citation31–34), although all comprised extra components including motivation enhancement (Citation29) and the development of an avoidance plan (Citation29,Citation32). In addition, one of the studies initially reported a recidivism rate for the treatment group of 26.4% compared to 32.3% of the control group after six months. However after 12 months this effect had decayed entirely (Citation30). Further, Mills et al. (Citation31) assessed the effectiveness of the “Sober Driver Program” (SDP), which includes both educational components and elements of cognitive-behavioral therapy.
Repeat DUI offenders (n = 1740) were allocated to the SDP and 9667 repeat DUI offenders were assigned to the control group and received only legal sanctions. Mills et al. found that after two years 4.9% of the SDP completers had reoffended compared to 10.2% of the comparison group (OR: 0.47, 95% CI: 0.37–0.60).
Victim impact panels (VIP)
VIPs consist of panel members who were seriously injured or who lost loved ones as a result of a DUI offense. The members volunteer to discuss how the DUI offense changed their lives, without placing any blame or judgment on the offenders who are in attendance. Often offenders are court ordered to attend VIPs, with the hope that it will change their attitudes towards DUI offenses, and in turn reduce recidivism (Citation35). VIP have been considered to be quite expensive and require significant effort (Citation36). Seven of the studies utilized an intervention comprising Victim Impact Panels (Citation36–42). Three of these studies reported no differences between the intervention group and their respective control groups (Citation36,Citation37,Citation39), three demonstrated a larger number of rearrests after VIP for those in the control group, compared to those in the VIP group (Citation38,Citation40,Citation41), and one study found that VIP participants were more likely to be re-arrested than control group participants (Citation42). Wheeler et al. (Citation37) investigated the effects of adding a VIP to the standard San Juan Country Driving While Impaired program in order to reduce re-arrest. They compared 56 offenders who received the standard program plus the VIP to 43 who received only the standard program. The standard program consisted of a detention/treatment intervention which included some therapeutic/educational components. After two years there was no difference in recidivism between the groups.
Intensive Supervision Programs (ISP)
ISPs were introduced in 1982 as an alternative sanction to incarceration for DUI offenders (Citation43). ISPs are designed to deal with DUI offenders through various restrictive, therapeutic and control measures. These include screening and assessment of offenders’ substance abuse problems, various treatment and education programs related to drink driving, intensive supervision (such as electronic monitoring), self-help, randomized alcohol and drug testing, license sanctions, interlocks, sale of vehicle, home confinement and community service (Citation15). Four studies investigated the effectiveness of Intensive Supervision Programs (Citation15,Citation43–45). Two of the studies reported a reduction in recidivism up to 5 years post-offense (Citation15,Citation44), one reported a reduction in re-arrest rates after the ISP (Citation43) and one found both no difference in arrest rates, as well as an increase in re-arrest rates for one group (Citation42).
Warchol (Citation43) compared re-arrest rates of 103 repeat DUI offenders who were sentenced to ISP to 111 DUI offenders who were sentenced to incarceration. Only 13% of those who took part in the ISP were re-arrested within the 5-year period after program completion, compared to 23% of those who had been incarcerated. In contrast, Lapham et al. (Citation35) investigated ISP with the inclusion of other forms of intervention. They utilized four groups; group one who were provided with a standard ISP including some treatment for alcohol abuse and court based monitoring, group two who received standard ISP in addition to mandatory vehicle sale, group three which had standard ISP with electronic monitoring, and group four who experienced standard ISP only. The study found that at the end of the probation period those in groups one, two and four had the same level of arrest risk, whereas group three had an increase in re-arrest rates of 96%.
DUI courts
DUI courts were developed as an extension to the drug court model for repeat DUI offenders who suffer from substance issues which are associated with re-offending and a lack of compliance with treatment. It allows close and frequent supervision by members of the judicial system, as well as treatment and punishment for noncompliance (Citation46). Four studies investigated the effectiveness of DUI courts on reducing recidivism (Citation46–49). Two studies found that the DUI court resulted in lower recidivism rates than comparison groups (Citation48,Citation49). One study found that attending a DUI court actually increased the rate of recidivism, with 17.9% of those who completed the program re-arrested for a new DUI offense, compared to only 6.7% of those who completed parole as per usual (Citation47). The remaining study found that the court was not associated with any reductions in self-reported or official reports of drinking and driving (Citation46). However, it is worth noting that DUI courts can be very different and there needs to be clear description of the monitoring and sanction frameworks used.
Other interventions
Other interventions that have been utilized in an attempt to prevent repeat DUI offenses include electronic monitoring (Citation50), fines and mandatory license actions (Citation51), and brief motivational interviewing (Citation52–54).Ten studies evaluated interventions other than those mentioned earlier (Citation14,Citation50–58). One assessed the effectiveness of fines and mandatory license actions (Citation51), one investigated sentence length (Citation56), one investigated sentence type (Citation58), three looked at brief motivational interviewing (Citation52–54), one evaluated a cognitive therapy approach (Citation14), and one assessed electronic monitoring (Citation50). Two of the studies assessed multicomponent treatment programs (Citation55,Citation57).
The combined use of fines and mandatory license withdrawal was found to effectively reduce recidivism, as did the swiftness with which the fines were imposed. However, mandatory license actions alone were not sufficient to reduce recidivism (Citation51). Serving fewer than 120 days in prison was associated with the highest recidivism rate (29%), and the lowest recidivism rate was found for those who served between four and six months in prison (Citation56).
The use of cognitive therapy on 62 repeat DUI offenders resulted in a lower rate of re-arrests for DUI recidivism for completers than non-completers of the program, 12.9% compared to 75% respectively (Citation14). Electronic monitoring as a sole intervention was not effective in reducing the number of new arrests (Citation50). One study found that brief motivational interviewing was more effective than receiving standard care alone (Citation54). Another study, however, found that this method was not effective in reducing rates of reoffending, reporting 24.7% of the 85 offenders who completed the interview being re-arrested, compared to 27.4% of the 95 persons in the control group – a non-significant difference (Citation52).
Another study utilizing brief motivational interviewing found no difference for those receiving the interviewing, compared to those in the comparison group (Citation53). The two studies reporting on multicomponent treatment programs found them to be very effective, with one study reporting a 47% lower risk of recidivism for those who received a pre-trial intervention including diversion into short-term, community-based programs with supervision and supportive services (such as alcohol related classes) compared to the control group (Citation55). The second study investigated whether breathalysing individuals twice daily, mandating them to wear a continuous alcohol monitoring bracelet, and providing swift, certain, and modest sanctions when tests return positive, would reduce DUI re-arrests. They found a 12% reduction in repeat DUI arrests and a 9% reduction in domestic violence arrests (Citation57).
Discussion
It is evident from the current review that there is a dearth of high quality evaluations of DUI interventions. The methodologies utilized across the studies were typically rated as weak, limiting the robustness of the conclusions that can be drawn. Nonetheless, it is reasonable to conclude that evidence exists to suggest that multi-component programs are more effective than those which target only one aspect of the issue. For example, evaluations of the Intensive Supervision Program, which consists of DUI education, substance use treatment, and electronic monitoring (among other forms of monitoring), have consistently reported significant reductions in DUI recidivism (Citation15,Citation43,Citation44). In addition, four out of the five education programs which reported reductions in recidivism included multiple components (Citation29,Citation31–33). The only study that evaluated the effects of education alone found no reduction in recidivism at one-year follow-up (Citation30). The ignition interlock intervention was shown to be effective in reducing recidivism while installed on the offenders car (Citation17,Citation18,Citation20,Citation23); however, three studies reported that recidivism levels returned to pre-intervention levels once it was removed (Citation19,Citation21,Citation22). Further, those studies which evaluated VIP programs reported no effect of such programs on reducing recidivism in DUI offenders.
Of note, for those studies which found a significant effect of intervention, only three reached a Maryland Scale of Scientific Rigor criteria of five, and eight met the criteria for a rating of four. Seven studies reaching these levels reported that the intervention being assessed had no effect of reducing either recidivism or re-arrests. This demonstrates the paucity of adequate studies providing high quality evidence to establish the effectiveness of DUI interventions. Additionally, further research is required among non-US offenders. Of the 42 studies included in the review, 33 originated from the USA. No studies from outside the USA achieved a Maryland rating of higher than three. Without such evidence it is difficult to determine whether such interventions are indeed effective and applicable outside of the US judicial system, and whether current resources are being utilized appropriately. Furthermore, the extent to which these findings are applicable to countries which have different legal limits for driving is unclear. In the US, for example, the legally permitted blood alcohol content is 0.08 mg of alcohol per ml of blood, whereas in countries such as Australia it is 0.05 mg/ml. Future evaluations of DUI interventions would greatly benefit from employing at least experimental designs, if not randomized control trials, to ensure that causality can be accurately determined and comparisons made across studies.
It may be that the apparent effectiveness of multi-component treatment arises from its ability to respond to the complexity and combination of legal, social and psychological factors that are associated with DUI behavior. Further, DUI offenders are a heterogeneous group, who have a range of different characteristics and motivations (Citation6) which need to be considered when designing interventions. These include level of psychiatric distress, substance use problems, and any prior DUI offenses. Multi-component programs may work best as they offer several ways of changing behavior within the same program. This allows those who are unresponsive to one component to benefit from others. Alternatively, a focus on individually tailored programs may be preferable. For example, a person who is diagnosed with an alcohol use disorder might respond best when allocated to a program that has a strong focus on alcohol misuse. Further, there is a need to provide evidence about which interventions are likely to work best with people who are arrested with high blood alcohol content levels, compared to those with lower levels, and for those who are repeat offenders, compared to those who are first time offenders.
Limitations
This review has some limitations that need to be acknowledged, including the use of recidivism or re-arrest as the outcome measures required for papers to be included into the review. Other outcomes, such as reductions in alcohol use, in self-report DUI participation, or in attitudes toward DUI behavior, are clearly important but were not captured in this review.
Conclusion
DUI offenses are a major cause of injury and death worldwide. There appears to be an insufficient evidence base for the effectiveness of DUI interventions, especially regarding which interventions work best for which groups and levels of offenders. Some DUI interventions have shown some promise, especially when they provide intensive supervision and offer a range of different strategies. There is, however, a need to further evaluate such interventions using stronger methodologies and extend evaluation research beyond North American DUI offenders, especially considering the legal blood alcohol content level in the US is 0.08%. The current paper re-emphasizes the importance of the heterogeneity of DUI offenders, and in particular the difficulties associated with developing and evaluating interventions designed for this group. The strength in multi-component interventions and matched treatment lie in their ability to adapt to the differing needs and characteristics of the DUI offenders who will be mandated to, or will voluntarily enter these programs. It is imperative that future research considers the array of needs that the DUI offending group present when developing and evaluating interventions.
Acknowledgements
This study was funded by the Centre for Mental Health and Wellbeing Research within the Faculty of Health at Deakin University. Mr Luke Xantidis provided comments on an earlier version of the manuscript.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this paper.
References
- World Health Organisation (WHO). Alcohol and injuries: Emergency department studies in an international perspective. Toronto: Centre for Addiction and Mental Health 2009:41–51
- Impinen A, Rahkonen O, Karjalainen K, Lintonen T, Lillsunde P, Ostamo A. Substance use as a predictor of driving under the influence (DUI) rearrests. A 15-year retrospective study. Traffic Inj Prevent 2009;10:220–226
- Marowitz LA. Predicting DUI recidivism: Blood alcohol concentration and driver record factors. Accident Analysis Prevent 1998;30:545–554
- Yu J, Williford WR. Drunk-driving recidivism: predicting factors from arrest context and case disposition. J Stud Alcohol 1995;56:60–66
- DeYoung DJ. An evaluation of the implementation of ignition interlock in California. J Safety Res 2002;33:473–482
- Nochajski TH, Stasiewicz PR. Relapse to driving under the influence (DUI): a review. Clin Psychol Rev 2006;26:179–195
- Wells-Parker E, Bangert-Drowns R, McMillen R, Williams M. Final results from a meta-analysis of remedial interventions with drink/drive offenders. Addiction 1995;90:907–926
- Shults RA, Elder RW, Sleet DA, Nichols JL, Alao MO, Carande-Kulis VG, Zaza S, et al. Reviews of evidence regarding interventions to reduce alcohol-impaired driving. Am J Prevent Med 2001;21:66–88
- Shults RA, Elder RW, Nichols JL, Sleet DA, Comptom R, Chattopadhyay SK. Effectiveness of multicomponent programs with community mobilization for reducing alcohol-impaired driving. Am J Prevent Med 2009;37:360–371
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009;151:264–269
- Sherman LW, Gottfredson DC, MacKenzie DL, Eck J, Reuter P, Bushway SD. Preventing crime: what works, what doesn’t, what’s promising. Washington, DC: US Department of Justice; 1998
- Reeves B, Deeks J, Higgins J, Wells G. Chapter 13: Including non-randomized studies. In: Higgins J, Green S, editors. Cochrane handbook for systematic reviews of interventions. Chichester, UK: John Wiley & Sons; 2008:390–432
- Finney JW, Moyer A. Meta-analysis: summarising findings on addiction intervention effects. In: Miller PG, Strang J, Miller PM, editors. Addiction research methods. Chichester, UK: Wiley-Blackwell; 2010:319–336
- Moore KA, Harrison M, Young MS, Ochshorn E. A cognitive therapy treatment program for repeat DUI offenders. J Criminal Just 2008;36:539–545
- Wiliszowski CH, Fell JC, McKnight AS, Tippetts AS, Ciccel JD. An evaluation of Three intensive supervision programs for serious DWI offenders. Ann Adv Automot Med 2010;54:375–387
- Beirness DJ, Marques PR. Alcohol ignition interlock programs. Traffic Inj Prevent 2004;5:299–308
- Rauch W, Ahlin E, Zador P, Howard J, Duncan G. Effects of administrative ignition interlock license restrictions on drivers with multiple alcohol offenses. J Experim Criminol 2011;7:127–148
- Bjerre B, Thorsson U. Is an alcohol ignition interlock programme a useful tool for changing the alcohol and driving habits of drink-drivers? Accident Analysis Prevent 2008;40:267–273
- Roth R, Voas R, Marques P. Interlocks for first offenders: effective? Traffic Inj Prevent 2007;8:346–352
- Bjerre B. Primary and secondary prevention of drink driving by the use of alcolock device and program: Swedish experiences. Accident Analysis Prevent 2005;37:1145–1152
- Raub RA, Lucke RE, Wark RI. Breath alcohol ignition interlock devices: controlling the recidivist. Traffic Inj Prevent 2003;4:28–34
- Voas RB, Marques PR, Tippetts AS, Beirness DJ. The Alberta Interlock Program: the evaluation of a province-wide program on DUI recidivism. Addiction 1999;94:1849–1859
- Weinrath M. The Ignition interlock program for drunk drivers: a multivariate test. Crime Delinquency 1997;43:42–59
- Beck KH, Rauch WJ, Baker EA, Williams AF. Effects of ignition interlock license restrictions on drivers with multiple alcohol offenses: a randomized trial in Maryland. Am J Public Health 1999;89:1696–1700
- Beirness DJ, Marques PR, Voas RB, Tippetts AS. The impact of mandatory versus voluntary participation in the alberta ignition interlock program. Traffic Inj Prevent 2003;4:195–198
- Roth R, Voas R, Marques P. Mandating interlocks for fully revoked offenders: the New Mexico experience. Traffic Inj Prevent 2007;8:20–25
- Bjerre B. An evaluation of the Swedish ignition interlock program. Traffic Inj Prevent 2003;4:17–23
- Wells-Parker E, Williams M. Enhancing the effectiveness of traditional interventions with drinking drivers by adding brief individual intervention components. J Stud Alcohol 2002;63:655–664
- Robertson AA, Gardner S, Xu X, Costello H. The impact of remedial intervention on 3-year recidivism among first-time DUI offenders in Mississippi. Accident Analysis Prevent 2009;41:1080–1086
- Ekeh AP, Hamilton SB, D’Souza C, Everrett E, McCarthy MC. Long-term evaluation of a trauma center-based juvenile driving intervention program. J Trauma 2011;71:223–226; discussion 226–227
- Mills KL, Hodge W, Johansson K, Conigrave KM. An outcome evaluation of the New South Wales Sober Driver Programme: a remedial programme for recidivist drink drivers. Drug Alcohol Rev 2008;27:65–74
- Rider R, Voas RB, Kelley-Baker T, Grosz M, Murphy B. Preventing alcohol-related convictions: the effect of a novel curriculum for first-time offenders on DUI recidivism. Traffic Inj Prevent 2007;8:147–152
- Williams DJ, Simmons P, Thomas A. Predicting DUI recidivism following an alcohol safety action program. J Offender Rehabil 2000;32:129–145
- Deyoung DJ. An evaluation of the effectiveness of alcohol treatment, driver license actions and jail terms in reducing drunk driving recidivism in California. Addiction 1997;92:989–997
- C’De Baca J, Lapham SC, Paine S, Skipper BJ. Victim impact panels: who is sentenced to attend? Does attendance affect recidivism of first-time DWI offenders? Alcohol Clin Exp Res 2000;24:1420–1426
- Crew BK, Johnson SE. Do victim impact programs reduce recidivism for operating a motor vehicle while intoxicated? Findings from an outcomes evaluation. Crim Just Stud 2011;24:153–163
- Wheeler DR, Rogers EM, Tonigan JS, Woodall WG. Effectiveness of customized Victim Impact Panels on first-time DWI offender inmates. Accident Analysis Prevent 2004;36:29–35
- Rojek DG, Coverdill JE, Fors SW. The effect of victim impact panels on DUI rearrest rates: a five-year follow-up. Criminology 2003;41:1319–1340
- Shinar D, Comptom RP. Victim Impact Panels: their impact on DWI recidivism. Alcohol, Drugs Driving 1995;11:73–87
- Sprang G. Victim impact panels. J Soc Serv Res 1997;22:73–84
- Fors SW, Rojek DG. The effect of victim impact panels on DUI/DWI rearrest rates: a twelve-month follow-up. J Stud Alcohol 1999;60:514–520
- C’De Baca J, Lapham SC, Liang HC, Skipper BJ. Victim impact panels: do they impact drunk drivers? A follow-up of female and male, first-time and repeat offenders. J Stud Alcohol 2001;62:615–620
- Warchol GL. Intensive supervision probation: an impact evaluation. Justice Professional 2000;13:219--232
- Lapham SC, Kapitula LR, C’de Baca J, McMillan GP. Impaired-driving recidivism among repeat offenders following an intensive court-based intervention. Accident Analysis Prevent 2006;38:162–169
- Lapham SC, C’De Baca J, Lapidus J, McMillan GP. Randomized sanctions to reduce re-offense among repeat impaired-driving offenders. Addiction 2007;102:1618–1625
- MacDonald JM, Morral AR, Raymond B, Eibner C. The efficacy of the Rio Hondo DUI court: a 2-year field experiment. Evaluat Rev 2007;31:4–23
- Bouffard JA, Richardson KA, Franklin T. Drug courts for DWI offenders? The effectiveness of two hybrid drug courts on DWI offenders. J Crim Justice 2010;38:25--33
- Fell JC, Tippetts AS, Ciccel JD. An evaluation of three driving-under-the-influence courts in Georgia. Ann Adv Automot Med 2011;55:301–312
- Ronan SM, Collins PA, Rosky JW. The effectiveness of Idaho DUI and misdemeanor/DUI courts: outcome evaluation. J Offender Rehabil 2009;48:154–165
- Courtright KE, Berg BL, Mutchnick RJ. Effects of house arrest with electronic monitoring on DUI offenders. J Offender Rehabil 1997;24:35–51
- Yu J. Punishment celerity and severity: testing a specific deterrence model on drunk driving recidivism. J Crim Justice 1994;22:355–366
- Ouimet MC, Dongier M, Di Leo I, Legault L, Tremblay J, Chanut F, Brown TG. A randomized controlled trial of brief motivational interviewing in impaired driving recidivists: a 5-year follow-up of traffic offenses and crashes. Alcoholism 2013;37:1979–1985
- Utter GH, Young JB, Theard LA, Cropp DM, Mhoar CJ, Eisenberg D, Schermer CR, Owens LJ. The effect of problematic drinking behaviour of a brief motivational interview shortly after a first arrest for driving under the influence of alcohol: a randomized trial. J Trauma Acute Care Surg 2013;76:661–671
- Schermer CR, Moyers TB, Miller WR, Bloomfield LA. Trauma center brief interventions for alcohol disorders decrease subsequent driving under the influence arrests. J Trauma 2006;60:29–34
- Lucker GW, Osti JR. Reduced recidivism among first-time DWI offenders as a correlate of pre-trial intervention. J Offender Rehabil 1997;24:1–17
- Weinrath M, Gartrell J. Specific deterrence and sentence length: the case of drunk drivers. J Contemp Crim Just 2001;17:105–122
- Kilmer B, Nicosia N, Heaton P, Midgette G. Efficacy of frequent monitoring with swift, certain, and modest sanctions for violations: insights from South Dakota’s 24/7 Sobriety Project. Am J Public Health 2013;103:e37–e43
- Delaney HD, Kunitz SJ, Hongwei Z, Woodall WG, Westerberg V, Rogers E, Wheeler DR. Variations in jail sentences and the probability of re-arrest for driving while intoxicated. Traffic Inj Prevent 2005;6:105–109