
Abstract
Physical inactivity, diabetes, hypertension, dyslipidemia, smoking and obesity were associated with imbalance in oxidative stress, leading to endothelial dysfunction. Such dysfunction is present in both cardiovascular disease (CVD) and erectile dysfunction (ED). ED is the persistent inability to achieve or sustain an erection sufficient for satisfactory sexual performance and is one of the first manifestations of endothelial damage in men with CVD risk factors. The purpose of this article is to review the results of studies involving physical activity, CVD, endothelial dysfunction and ED in order to verify its applicability for improving the health and quality of life of men with such disorders. There is consistent evidence that endothelial damage is intimately linked to ED, and this manifestation seems to be associated with the appearance CVDs. On the other hand, physical activity has been pointed out as an important clinical strategy in the prevention and treatment of CVDs and ED mainly associated with improvement of endothelial function. However, further experimental and clinical prospective investigations are needed to test the role of physical exercises in the modulation of endothelial function and their implications on erectile function and the appearance of CVDs.
Introduction
Endothelium is an endocrine organ that plays an important role in maintaining vascular homeostasis. This role is not restricted to maintenance of vascular tone, as it also regulates inflammation, platelet activation and thrombosis [Citation1–3]. Substances produced by the endothelium may have vasodilating properties, such as nitric oxide (NO), prostacyclin, endothelium-derived hyperpolarizing factor and kinins, or vasoconstriction properties, such as endothelin, prostaglandins, angiotensin II and reactive oxygen species [Citation1–3]. When the endothelium is preserved, there is a balance between the productions of these substances [Citation3].
Hypertension, diabetes, dyslipidemia, smoking and overweight may trigger increased oxidative stress, thus contributing to endothelial dysfunction, which has been associated with some pathophysiologic processes, e.g. myocardial infarction, peripheral vascular disease, renal disease and erectile dysfunction (ED). In this sense, oxidative stress seems to be a basic common denominator in endothelial dysfunction in cardiovascular diseases (CVDs) [Citation4].
ED is the persistent inability to achieve or sustain an erection sufficient for satisfactory sexual performance [Citation5]. It is highly prevalent and the cause may be neurologic, endocrine, psychogenic, or vascular, the latter being the most common etiology. The incidence of ED increases with the number of comorbidities such as hypertension, diabetes, dyslipidemia, smoking, atherosclerosis and CVDs [Citation6]. ED is one of the first manifestations of endothelial damage in men with vascular risk factors and the first clinical manifestation of these comorbidities [Citation6].
The metabolic, cardiovascular, autonomic and anti-inflammatory benefits of changes in nutritional habits and increase in physical activity time have led many researchers to suggest these approaches as important non-pharmacologic tools in the prevention and treatment of CVD, as well as on DNA damage [Citation7–9]. The purpose of this article is to review the results of studies involving physical activity, CVD, endothelial dysfunction and ED in order to verify its applicability for improving the health and quality of life of men with such disorders.
Methods
We evaluated clinical trials using PUBMED as our database. The key words used in the search were: endothelial dysfunction, erectile dysfunction, physical activity and sildenafil. The collected articles are from 1953 to 2013. All texts included in the review were assessed and compiled.
Results and discussion
Endothelial damage and ED
Endothelial dysfunction is an abnormal response that leads to a lower bioavailability of NO and impairs vasodilation, thus promoting the development of atherosclerosis and acute coronary syndromes. Endothelial dysfunction has been linked with the incidence of risk factors, modifiable or not, as age, smoking, dyslipidemia, diabetes, obesity, etc. [Citation1]. In this sense, Wonisch et al. [Citation10] investigated the relationship between body mass index (BMI), age and oxidative stress on 2190 subjects. The authors evidenced that oxidative stress increases with increasing BMI and age, as a sequel to an impaired antioxidant status, the consumption of autoantibodies against oxidized, an increase of peroxides and uric acid, and a disadvantaged lipid profile.
The reduction in NO bioavailability may affect platelet aggregation, vascular wall inflammation and proliferation of smooth muscle cells [Citation3]. Accumulated evidence seem to indicate that NO is the main regulator of blood pressure and this control is achieved through the production of NO in endothelial cells. In this process, several chemical messengers, including hormones and acetylcholine, may activate endothelial NO synthase, binding it to appropriate receptors on endothelial cell membrane [Citation11,Citation12].
The activation of pelvic nerves through sexual arousal results in the release of NO, which acts as a neurotransmitter, leading to the relaxation of smooth muscles of the penile vessels and to the engorgement of the cavernous and spongy bodies (the phenomenon of penile erection) [Citation13]. The key role of NO in protecting the cardiovascular system in general and promoting penile erection, in particular, was first acknowledged in the mid-90 s [Citation14], and the discovery led to a race to develop new drugs which would act modulating and stimulating the l-arginine–NO and cGMP. These were found to have potentially beneficial vasodilating antihypertensive effect, and would even be effective in the treatment of ED.
Pathophysiology of ED shows that organic substrates are present in ∼80% of all cases of ED, and most of them are related to mostly vascular changes. Additionally, ED is considered an early marker of cardiovascular risk, and may also precede clinical manifestations of atherosclerosis and reveal a broader systemic vasculopathy in men [Citation15].
The increasing occurrence of ED and its severity are associated with male aging and accompanied by changes in atherosclerotic vascular beds. Most men with ED of vascular origin have at least one significant cardiovascular risk factor [Citation15]. Several hypotheses have attempted to explain the pathophysiology of ED in CVD, and the role of oxidative stress in the endothelium in the pathogenesis of ED has been confirmed. Studies have also demonstrated that adequate treatment may reverse the condition [Citation16–18].
Functional abnormality is clinically manifested in the difficulty in vasodilation and the resulting increased blood flow, which would affect the penile circulation, thus compounding a systemic vascular disease. Nevertheless, erection is a psychoneurovascular phenomenon involving the interaction of multiple systems, culminating in an increase in blood flow in the penile hypogastric bed, with the subsequent activation of the veno-occlusive mechanism of the corpus cavernosum.
Increased blood flow into the corpus cavernosum is needed for a successful erection, and any relatively small change is sufficient to cause hemodynamic ED [Citation19]. This is further supported by the strong correlation found in research between baseline levels of asymmetric dimethylarginine and cardiovascular risk factors, such as lipoprotein A and inflammatory markers in patients with ED [Citation16]. Men displaying evidence of penile arterial disease (mild and severe arterial insufficiency) were characterized by elevated C-reactive protein levels compared to men with no evidence of arterial abnormalities in the penis, as measured by penile Doppler [Citation20]. In addition, endothelial progenitor cells changes in patients with ED has been pointed out as an important diagnostic marker, which in clinical practice can be used together with penile Doppler [Citation21].
Some years ago, ED treatments included vacuum constriction devices, intracavernous self-injections of vasoactive agents (alprostadil, prostaglandin E1) [Citation22] and transurethral insertion of alprostadil [Citation23], in addition to the deployment of penile prostheses or venous/arterial surgery, all of which were widely used in the management of ED. Currently, the treatment is carried out using 5-hydrolase phosphodiesterase (PDE-5) inhibitors. The main drugs of this category are sildenafil, vardenafil and tadalafil.
Sildenafil has important vascular effects, since it acts competing with PDE-5, thus leading to a reduction in the degradation of cGMP, and a consequent increase in this tissue, thus promoting vasodilation, which, in turn, improves ED. Furthermore, this drug has been considered safe in different clinical conditions [Citation24].
Sildenafil has cardiovascular effects on heart rate, blood pressure, pulmonary and coronary circulation, as well as on endothelium of patients with chronic heart failure, and submitted to cardiac repolarization [Citation25]. More recently, a cardioprotective effect of PDE-5 inhibitors have been described in the context of cardiac ischemia, highlighting their role in decreasing infarct size, improving left ventricular function, decreased incidence of ventricular fibrillation and reduced myocardial necrosis [Citation26,Citation27].
Eleven families of PDEs have been identified in mammalian tissues [Citation28], and the distribution of the various PDEs varies between different tissues and cell types [Citation29]. Importantly, accumulating data show that the therapeutic potential extends to the cardiovascular, gastrointestinal, cutaneous and nervous system and that these agents may be beneficial in a multitude of conditions such as Raynaud’s phenomenon, heart failure, essential hypertension and stroke. PDE-5 inhibitors are a conceptually attractive therapeutic class of agents with pleiotropic effects [Citation30].
On the other hand, Frantzen et al. [Citation31] have observed that following the introduction of sildenafil, ED ceased to mean an increased risk of cardiovascular events among those who seek treatment. However, if ED diagnosis is accurately established and vascular etiology is dominant, the condition warrants, for many researchers, a complete cardiovascular evaluation, seeking to identify the associated risk factors and encourage changes in lifestyle (along with drug therapy, if needed) to modify cardiovascular risk and produce beneficial effect on erectile function and sexual health [Citation32].
Physical activity and endothelial dysfunction
Several epidemiologic studies designed to investigate the association between physical activity and CVD have been carried out since the mid-twentieth century. The first registered correlation was found in 1953 in London workers. This British study demonstrated that physically active men at work had half the mortality rates from coronary heart disease than those listed as sedentary men [Citation33].
As early as the sixties, a study undertaken in USA showed that men who died of heart disease were 40–50% less active than men who were still alive [Citation34]. Some years later, another study sought to correlate the level of physical activity during leisure time with the risk of coronary heart disease and death in adult males. The results indicated there is a modest inverse relationship between the level of physical activity during leisure time and risk of coronary heart disease and overall mortality in middle-aged men [Citation35].
In order to verify the impact of physical activity on cardiovascular health, a study revealed that regular physical activity may prevent CVD in healthy young men, since exercise improved vascular function through the amelioration of endothelium-dependent vasodilation [Citation36]. Higashi et al. [Citation37] found similar results in normotensive men.
A cross-sectional study involving healthy volunteers assessed the number of endothelial progenitor cells when they underwent three levels of intensity running, high, moderate, and moderate in short running time. Both moderate and high intensity running promoted an increase in the number of circulating endothelial progenitor cells, which is an important benefit of physical activity. The quantification of circulating endothelial progenitor cells was shown to be an important parameter in the evaluation of the vascular effects of exercise [Citation38]. Another similar study concluded that the increase in the number of endothelial progenitor cells appears to be higher in individuals with a less favorable lipid profile [Citation39].
Seeking to determine the influence of physical activity on specific diseases or medical conditions, several studies were conducted involving patients with hypertension [Citation33], congestive heart failure (CHF) [Citation40,Citation41], metabolic syndrome [Citation42], diabetes [Citation43], myocardial infarction [Citation44] and coronary heart disease [Citation45]. Higashi et al. [Citation37] have found that physical activity undertaken for a 12-week period improved endothelium-dependent vasodilation by increasing NO release both in normotensive patients and in hypertensive patients.
In patients with CHF, physical activity corrected the existing endothelial dysfunction and improved exercise tolerance, since exercise training ameliorated endothelial-dependent vasodilation and NO endothelium in skeletal muscle of patients [Citation40]. Supplementation with l-arginine in patients with CHF undergoing physical activity seemed to promote additional benefits on the endothelium, as demonstrated by the improvement in endothelium-dependent vasodilation of patients who underwent both interventions [Citation41].
Similarly, 3 months in a physical activity program resulted in an improvement in flow-mediated dilation, resulting in an increase in the maximum capacity of exercises in patients with metabolic syndrome [Citation42]. The combination of resistance training and aerobic exercise contributed to the improvement of glycemic index and endothelial function in patients with type 2 diabetes, indicating that the practice of physical activity can be an integral component in the management of the disease in patients who can perform physical exercises [Citation43].
In a study designed to assess the effect of moderate aerobic exercise on endothelial function in patients after myocardial infarction, physical activity was found to contribute to increase both endothelium-dependent vasodilation and tolerance to exercise in newly infarcted patients [Citation44]. Furthermore, regular physical activity increased the number of circulating endothelial progenitor cells in addition to improving vascular function and NO synthesis in patients with coronary artery disease and multiple cardiovascular risk factors [Citation45].
A survey conducted with participants from the Framingham study concluded that aging, systolic pressure, BMI and smoking are associated with decreased flow-mediated dilation, whereas physical exercise was related to an increase in flow-mediated dilation [Citation46]. Given that, it can be stated that regular physical activity consistently improves the bioavailability of NO and increases the number of endothelial progenitor cells [Citation45,Citation47–49] and also decreases the level of inflammatory markers: proinflammatory cytokines and C-reactive protein [Citation50].
Physical activity and ED
The practice of physical activity in both experimental and clinical studies has led to a significant improvement in erectile function; thus, physical activity may be regarded as a protective factor for normal erectile function [Citation51–63].
Data from the Massachusetts Male Aging Study, carried out with a sample of 1156 men aged 40–70 years followed for 8.8 years, showed that the lowest risk for ED was among the physically active men, as compared with sedentary men (<200 kcal/day of physical activity) [Citation51]. Detailed guidance on how to lose 10% or more of body weight by reducing caloric intake and increasing physical activity levels in obese men in Italy has resulted, 2 years after the initial intervention, in increased levels of physical activity, BMI reduction and increased erectile function, as assessed by completing a standardized questionnaire to generate a standard index, the International Index of Erectile Function (IIEF) [Citation53].
In this Italian study, it was found that BMI had a greater impact in the ED in patients with low levels of physical activity. In contrast, the level of physical activity had a greater impact when BMI was higher [Citation53]. In a similar study involving the provision of detailed guidelines against general guidelines, the researchers have also concluded that it is possible to achieve an improvement in erectile function without the use of pharmacologic intervention, provided that weight loss is achieved and physical activity is increased [Citation52].
In the Health Professionals Follow-up Study, a cohort study involving 22 086 men, physical activity was associated with lower risk of ED. The multivariate relative risk was 0.7 to >32.6 metabolic equivalents of exercise per week. Interestingly, all types of exercises included in the protocol demonstrated significant benefits [Citation54].
A study conducted in Hong Kong showed that age, level of physical activity and the degree of psychological distress were independently associated with ED. The relationship between BMI and ED was observed only in physically inactive men (<1 time/week), while in physically active men (≥1000 kcal/week) the risk of ED was lower only for obese men [Citation55].
In a study that divided the subjects into active (≥150 min/week), moderately active (30–149 min/week) and inactive (<30 min/week) or moderately active men were 40–60% more likely to present ED than active men. Men with larger waist circumference and low physical activity (inactive, moderately active) were associated with a greater likelihood of having ED, while there was no significant correlation between BMI and ED. Thus, waist circumference below 102 cm and physical activity of moderate intensity (≥150 min/week) are associated with a proper erectile function, regardless of BMI [Citation56].
Kratzik et al. [Citation57] in a cross-sectional study involving 674 men, aged 45–60 years, in their workplace has shown a positive correlation between the IIEF and physical activity generating 1000–4000 kcal/week of energy expenditure. The risk of severe ED was reduced to 82.9% with a minimum of 3000 kcal/week of energy expenditure. The study found that increasing energy expenditure of weekly physical activity from 1000 to 4000 kcal can indeed reduce the risk of ED. In diabetic men aged 35–70 years, physical activity was found to be a protective factor of ED [Citation59].
Middle-aged patients (48–62 years) with ED of vascular origin underwent a protocol of moderate to intense (150 min/week) aerobic activity, and after 3 months physical activity improved the quality of erectile function, probably by reducing endothelial apoptosis [Citation61].
In order to determine whether the appearance of subclinical markers of atherosclerosis was associated with ED, data on patients with metabolic syndrome and healthy subjects were compared. Patients with metabolic syndrome and ED should be considered of high risk for future cardiovascular events. Once again, it was found that physical activity appears to have a protective effect on erectile function [Citation62].
Reinforcing the direct beneficial effects of healthy habits on erectile function, another study sought to associate physical activity and physical fitness level with ED in men between 40 and 75 years. The results showed that younger men with higher levels of physical activity and better conditioning are less likely to present ED [Citation60].
Experimental studies designed to evaluate the effect of physical activity on sexual function had previously been performed in adults already showing some degree of ED; however, the impact of exercise in healthy young people remained unclear. Recently, Hsiao et al. [Citation63] found that an increase in physical activity was associated with better sexual function in the healthy young (under 40 years). A groundbreaking study, performed by Maio et al. [Citation58], aiming determine the effects of physical activity in the treatment of ED, founded that the use of PDE-5 inhibitors combined with physical activity practice (3 h/week) was more effective in treating ED than PDE-5 inhibitors alone.
Physical activity, ED and CVDs
As previously mentioned, ED is predominantly an endothelial vascular disease and there is a consensus to consider that men with ED present elevated risk of CVDs [Citation31,Citation64]. Many patients present with underlying systemic CVD and their first symptom can be ED [Citation64]. On the other hand, physical activity has been considered an important strategy in the prevention and treatment of endothelial dysfunction, ED and CVD [Citation36–45].
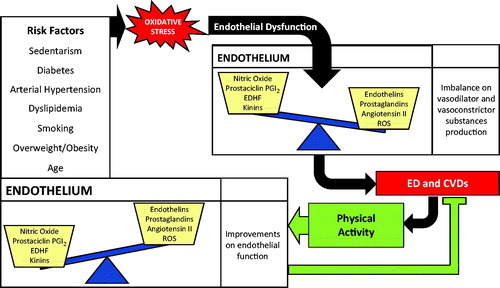
Thus, as shown in , it is possible that most of the modifiable (or not) risk factors lead to an increase in oxidative stress in the vascular endothelium. This increase in oxidative stress would result in an imbalance of vasodilator and vasoconstrictor substances production, conducing to the appearance of the ED and therefore CVDs. Is it possible that a physically active lifestyle improves endothelial function, preventing and/or mitigating the onset of ED and CVDs.
Figure 1. Possible influences of physical activity on endothelial dysfunction: a link between prevention/treatment of erectile dysfunction and cardiovascular diseases. EDHF - Endothelium-derived hyperpolarizing factor; ROS - reactive oxygen species; ED erectile dysfunction; CVDs cardiovascular diseases.
Conclusion
There is consistent evidence that endothelial damage is intimately linked to ED, and this manifestation seems to be associated with the appearance CVDs. On the other hand, physical activity has been pointed out as an important clinical strategy in the prevention and treatment of CVDs and ED mainly associated with improvement of endothelial function. However, further experimental and clinical prospective investigations are needed to test the role of physical exercises in the modulation of endothelial function and their implications on erectile function and the appearance of CVDs. The results of these future studies will improve the management of cardiovascular risk, quality of life and survival of men.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Behrendt D, Ganz P. Endothelial function. From vascular biology to clinical applications. Am J Cardiol 2002;90:40L–8L
- Sudano I, Spieker LE, Hermann F, et al. Protection of endothelial function: targets for nutritional and pharmacological interventions. J Cardiovasc Pharmacol 2006;47:S136–50
- Félétou M, Vanhoutte PM. Endothelial dysfunction: a multifaceted disorder (The Wiggers Award Lecture). Am J Physiol Heart Circ Physiol 2006;291:H985–1002
- Guay AT. ED2: erectile dysfunction = endothelial dysfunction. Endocrinol Metab Clin North Am 2007;36:453–63
- NIH Consensus Conference on Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993;270:83–90
- Kendirci M, Nowfar S, Hellstrom WJ. The impact of vascular risk factors on erectile function. Drugs Today 2005;41:65–74
- Pedersen BK, Saltin B. Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports 2006;16:3–63
- Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol 2012;2:1143–211
- Teng NI, Shahar S, Rajab NF, et al. Improvement of metabolic parameters in healthy older adult men following a fasting calorie restriction intervention. Aging Male 2013;16:177–83
- Wonisch W, Falk A, Sundl I, et al. Oxidative stress increases continuously with BMI and age with unfavourable profiles in males. Aging Male 2012;15:159–65
- Snyder SH, Bredt DS. Biological roles of nitric oxide. Sci Am 1992;266:68–71, 74–77
- Chen K, Pittman RN, Popel AS. Nitric oxide in the vasculature: where does it come from and where does it go? A quantitative perspective. Antioxid Redox Signal 2008;10:1185–98
- Burnett AL. Role of nitric oxide in the physiology of erection. Biol Reprod 1995;52:485–9
- Rongen GA, Smits P, Thien T. Endothelium and the regulation of vascular tone with emphasis on the role of nitric oxide. Physiology, pathophysiology and clinical implications. Neth J Med 1994;44:26–35
- Doumas M, Douma S. Sexual dysfunction in essential hypertension: myth or reality? J Clin Hypertens 2006;8:269–74
- Wierzbicki AS, Solomon H, Lumb PJ, et al. Asymmetric dimethyl arginine levels correlate with cardiovascular risk factors in patients with erectile dysfunction. Atherosclerosis 2006;185:421–5
- Solomon H, Wierzbicki AS, Lumb PJ, et al. Cardiovascular risk factors determine erectile and arterial function response to sildenafil. Am J Hypertens 2006;19:915–9
- Agarwal A, Nandipati KC, Sharma RK, et al. Role of oxidative stress in the pathophysiological mechanism of erectile dysfunction. J Androl 2006;27:335–47
- Sáenz de Tejada I, Angulo J, Cellek S, et al. Pathophysiology of erectile dysfunction. J Sex Med 2005;2:26–39
- Billups KL, Kaiser DR, Kelly AS, et al. Relation of C-reactive protein and other cardiovascular risk factors to penile vascular disease in men with erectile dysfunction. Int J Impot Res 2003;15:231–6
- Condorelli RA, Calogero AE, Vicari E, et al. Endothelial progenitor cells and erectile dysfunction: a brief review on diagnostic significance and summary of our experience. Aging Male 2013;16:29–32
- Linet OI, Ogrinc FG. Efficacy and safety of intracavernosal alprostadil in men with erectile dysfunction. New Engl J Med 1996;334:873–7
- Padma-Nathan H, Hellstrom WJ, Kaiser FE, et al. Treatment of men with erectile dysfunction with transurethral alprostadil. New Engl J Med 1997;336:1–7
- Leoni LA, Leite GS, Wichi RB, Rodrigues B. Sildenafil: two decades of benefits or risks? Aging Male 2013;16:85–91
- Raja SG, Nayak SH. Sildenafil: emerging cardiovascular indications. Ann Thorac Surg 2004;78:1496–506
- Kontaras K, Varnavas V, Kyriakides ZS. Does sildenafil cause myocardial infarction or sudden cardiac death? Am J Cardiovasc Drugs 2008;8:1–7
- Lee TM, Chen CC, Chung TH, Chang NC. Effect of sildenafil on ventricular arrhythmias in post-infarcted rat hearts. Eur J Pharmacol 2012;690:124–32
- Corbin JD, Francis SH. Pharmacology of phosphodiesterase-5 inhibitors. Int J Clin Pract 2002;56:453–9
- Wallis RM, Corbin JD, Francis SH, Ellis P. Tissue distribution of phosphodiesterase families and the effects of sildenafil on tissue cyclic nucleotides, platelet function, and the contractile responses of trabeculae carneae and aortic rings in vitro. Am J Cardiol 1999;83:3C–12C
- Vlachopoulos C, Terentes-Printzios D, Ioakeimidis N, et al. PDE5 inhibitors in non-urological conditions. Curr Pharm Des 2009;15:3521–39
- Frantzen J, Speel TG, Kiemeney LA, Meuleman EJ. Cardiovascular risk among men seeking help for erectile dysfunction. Ann Epidemiol 2006;16:85–90
- Montorsi F, Padma-Nathan H, Glina S. Erectile function and assessments of erection hardness correlate positively with measures of emotional well-being, sexual satisfaction, and treatment satisfaction in men with erectile dysfunction treated with sildenafil citrate (Viagra). Urology 2006;68:26–37
- Morris JN, Heady JA, Raffle PAB, et al. Coronary heart-disease and physical activity of work. Lancet 1953;262:1111–20
- Paffenbarger RS, Wolf PA, Notkin J, Thorne MC. Chronic disease in former college students: I. Early precursors of fatal coronary heart disease. Am J Epidemiol 1966;83:314–28
- Leon AS, Connett J, Jacobs DR Jr, Rauramaa R. Leisure-time physical activity levels and risk of coronary heart disease and death. The Multiple Risk Factor Intervention Trial. JAMA 1987;258:2388–95
- Clarkson P, Montgomery HE, Mullen MJ, et al. Exercise training enhances endothelial function in young men. J Am Coll Cardiol 1999;33:1397–85
- Higashi Y, Sasaki S, Kurisu S, et al. Regular aerobic exercise augments endothelium-dependent vascular relaxation in normotensive as well as hypertensive subjects. Circulation 1999;100:1194–202
- Laufs U, Urhausen A, Werner N, et al. Running exercise of different duration and intensity: effect on endothelial progenitor cells in healthy subjects. Eur J Cardiovasc Prev Rehabil 2005;12:407–14
- Van Craenenbroeck EM, Vrints CJ, Haine SE, et al. A maximal exercise bout increases the number of circulating CD34+/KDR+ endothelial progenitor cells in healthy subjects. Relation with lipid profile. J Appl Physiol (1985) 2008;104:106–13
- Hambrecht R, Fiehn E, Weigl C, et al. Regular physical exercise corrects endothelial dysfunction and improves exercise capacity in patients with chronic heart failure. Circulation 1998;98:2709–15
- Hambrecht R, Hilbrich L, Erbs S, et al. Correction of endothelial dysfunction in chronic heart failure: additional effects of exercise training and oral L-arginine supplementation. J Am Coll Cardiol 2000;35:706–13
- Lavrencic A, Salobir BG, Keber I. Physical training improves flow-mediated dilation in patients with the polymetabolic syndrome. Arterioscler Thromb Vasc Biol 2000;20:551–5
- Maiorana A, O’Discroll G, Cheetham C, et al. The effect of combined aerobic and resistance exercise training on vascular function in type 2 diabetes. J Am Coll Cardiol 2001;38:860–6
- Vona M, Rossi A, Capodaqlio P, et al. Impact of physical training and detraining on endothelium-dependent vasodilation in patients with recent acute myocardial infarction. Am Heart J 2004;147:1039–46
- Steiner S, Niessner A, Zieqler S, et al. Endurance training increases the number of endothelial progenitor cells in patients with cardiovascular risk and coronary artery disease. Atherosclerosis 2005;18:305–10
- Benjamin EJ, Larson MG, Keyes MJ, et al. Clinical correlates and heritability of flow-mediated dilation in the community: the Framingham Heart Study. Circulation 2004;109:613–9
- Adams V, Linke A, Breuckmann F, et al. Circulating progenitor cells decrease immediately after marathon race in advanced-age marathon runners. Eur J Cardiovasc Prev Rehabil 2008;15:602–7
- Möbius-Winkler S, Hilberg T, Menzel K, et al. Time-dependent mobilization of circulating progenitor cells during strenuous exercise in healthy individuals. J Appl Physiol (1985) 2009;107:1943–50
- Navasiolava NM, Dignat-George F, Sabatier F, et al. Enforced physical inactivity increases endothelial microparticle levels in healthy volunteers. Am J Physiol Heart Circ Physiol 2010;299:H248–56
- Ribeiro F, Alves AJ, Duarte JA, Oliveira J. Is exercise training an effective therapy targeting endothelial dysfunction and vascular wall inflammation? Int J Cardiol 2010;141:214–21
- Derby CA, Mohr BA, Goldstein I, et al. Modifiable risk factors and erectile dysfunction: can lifestyle changes modify risk? Urology 2000;56:302–6
- Esposito K, Ciotola M, Giugliano F, et al. Effects of intensive lifestyle changes on erectile dysfunction in men. J Sex Med 2009;6:243–50
- Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA 2004;291:2978–84
- Bacon CG, Mittleman MA, Kawachi I, et al. A prospective study of risk factors for erectile dysfunction. J Urol 2006;176:217–21
- Cheng JY, Ng EM, Ko JS, Chen RY. Physical activity and erectile dysfunction: meta-analysis of population-based studies. Int J Impot Res 2007;19:245–52
- Janiszewski PM, Janssen I, Ross R. Abdominal obesity and physical inactivity are associated with erectile dysfunction independent of body mass index. J Sex Med 2009;6:1990–8
- Kratzik CW, Lackner JE, Märk I, et al. How much physical activity is needed to maintain erectile function? Results of the Androx Vienna Municipality Study. Eur Urol 2009;55:509–16
- Maio G, Saraeb S, Marchiori A. Physical activity and PDE5 inhibitors in the treatment of erectile dysfunction: results of a randomized controlled study. J Sex Med 2010;7:2201–8
- Giugliano F, Maiorino M, Bellastella G, et al. Determinants of erectile dysfunction in type 2 diabetes. Int J Impot Res 2010;22:204–9
- Agostini LC, Netto JM, Miranda MV Jr, Figueiredo AA. Erectile dysfunction association with physical activity level and physical fitness in men aged 40–75 years. Int J Impot Res 2011;23:115–21
- La Vignera S, Condorelli R, Vicari E, et al. Aerobic physical activity improves endothelial function in the middle-aged patients with erectile dysfunction. Aging Male 2011;14:265–72
- Pohjantähti-Maaroos H, Palomäki A, Hartikainen J. Erectile dysfunction, physical activity and metabolic syndrome: differences in markers of atherosclerosis. BMC Cardiovasc Disord 2011;11:36
- Hsiao W, Shrewsberry AB, Moses KA, et al. Exercise is associated with better erectile function in men under 40 as evaluated by the International Index of Erectile Function. J Sex Med 2012;9:524–30
- Billups KL, Bank AJ, Padma-Nathan H, et al. Erectile dysfunction is a marker for cardiovascular disease: results of the minority health institute expert advisory panel. J Sex Med 2005;2:40–50