The imperative to doctors of “first, do no harm” does not seem nowadays to be a simple rule to follow (Citation1). While the average number of diagnostic tests and treatment options has increased, newer risks have been added by the use of these novice treatments and diagnostic tests. Medical management is responsible for harming a high proportion of patients (Citation2). In the United States alone, the number of medical errors resulting in the death of a patient is estimated to be up to 98,000 a year, which would make it the eighth most common cause of mortality (Citation3,Citation4).
Family doctors most commonly perceive their causes of medical errors to be distraction, hastiness in completing the diagnostic process, lack of knowledge, and inadequately aggressive patient management (Citation5). Doctors who are aware of common causes of medical errors might be better prepared to face and prevent them. It should also be borne in mind that even good, experienced doctors might be involved in serious medical mistakes (Citation5). In an effort to understand the phenomenon of physician error, we examined a small sample of Turkish family medicine residents’ perceptions and attitudes towards medical errors.
Family medicine residents working in three education and research hospitals in Ankara, Turkey, were asked to participate in this study. Thirty-five out of 51 (68%) answered the anonymous questionnaire. The study questionnaire consisted of 12 questions concerning medical errors and the socio-demographic data of respondents. Free-text questions were analysed qualitatively for common themes.
The mean age of the participants was 35.3 years (SD 3.71, range 26–43 years). Sixteen residents were female, and 19 were male. Participants graduated from medical school 6 (2–22) years prior, and had been working as physicians for 6.0 (1–21) years.
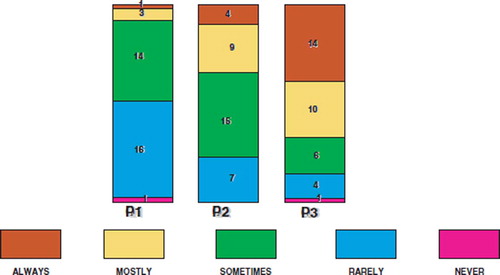
Responses to the questionnaire revealed the following results. Medical errors can sometimes (score 3 [range 1–5]) occur during daily clinical practice. Maltreatment (n=3, 8.6%), misdiagnosis (3, 8.6%), and inappropriate drug dose (1, 2.9%) were stated as possible medical errors. Medical errors could be prevented with education (7, 20%), by being careful (3, 8.6%), by control (2, 5.8%), and by investment (1, 2.9%). Moreover, the perceptions of respondents revealed the following results. Medical errors sometimes (3 [1–5]) affect daily life. Medical errors are serious problems that sometimes threaten patients’ lives (3 [1–5]). Respondents would mostly (4 [1–5]) inform authorities about a medical error (). One (2.9%) resident stated that the type of medical error he was involved in concerned inappropriate drug dose (hypoglycaemia).
Figure 1. Family medicine residents’ perceptions regarding medical errors. Perception 1 (P1): medical errors affect daily life; P2: medical errors are serious problems that threaten patients’ lives; P3: I would inform the authorities immediately if I caused a medical error. Scores: 5=always; 4=mostly; 3=sometimes; 2=rarely; 1=never.
High-quality healthcare requires a lower number of medical errors and an increase in patient safety (Citation6). On the other hand, a culture of blame hinders appropriate reporting of doctors’ medical errors (Citation7). Doctors need to be more open to criticism and to communicate their mistakes. Residents need to be motivated to report medical error sources. As a consequence, we believe this will reduce the number of incidents (Citation1).
The main causes of adverse events are reported to be due to operative errors, drug treatment, procedural interventions, and diagnosis (Citation7). In our study, family medicine residents reported that misdiagnosis, maltreatment, and inappropriate drug use are the main causes of medical error. Drugs remain a major source of error in our study. Possible drug interactions and incorrect dosages of drugs were stated as a main problem. Errors in diagnosis could be minimized by better training and wider use of protocols and algorithms.
In conclusion, in Turkey, more emphasis should be given to the prevention of medical errors in residency. Building a relationship of trust and confidence with residents and protecting potential “whistle-blowers” might also help better train residents to prevent medical errors.
Acknowledgements
This paper was presented at the Wonca Europe regional conference in Amsterdam, 1–4 June 2004. We are grateful to the family medicine residents who participated in the study. This paper was supported by the Akdeniz University Research Management Unit.
References
- McNeill PM, Walton M. Medical harm and the consequences of error for doctors. Med J Aust 2002; 176:222–5.
- Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The Quality in Australian Health Care Study. Med J Aust 1995; 1639:458–71.
- Kohn L, Corrigan J, Donaldson M. for the Committee on Quality of Health Care in America, Institute of Medicine To err is human: building a safer health system. National Academy PressWashington2000.
- Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation. BMJ 2000; 320:745–9.
- Ely JW, Levinson W, Elder NC, Mainous AG, Vinson DC. Perceived causes of family physicians’ errors. J Fam Pract 1995; 40:337–8.
- Committee on Health Care Quality in America Crossing the Quality Chasm. A New Health System for the 21st Century. Washington, DC: National Academy Press .2001.
- Alberti KGMM. Medical errors: a common problem. BMJ 2001; 322:501–2.