Abstract
Corticosteroid joint injections are perceived as being an effective treatment for symptomatic knee osteoarthritis, with a very low risk of complications. While the procedure is often performed in secondary care by orthopaedic surgeons and rheumatologists (and trainees in either specialty), the role of general practitioners (GPs) in chronic disease management has long existed with joint injections also frequently performed in primary care. The perception that serious complications from corticosteroid knee joint injections are rare and that their benefits in treating symptomatic knee osteoarthritis significantly outweigh the risks has not been well addressed. We present a case of a 71-year-old obese female who presented to her general practitioner (GP) with worsening left knee pain and radiographic changes consistent with osteoarthritis. She was administered a corticosteroid joint injection, which gave minimal relief, and over the next few days resulted in worsening severe pain, erythema and swelling. She returned to the GP who commenced oral antibiotics and referred her to casualty. A large knee abscess was diagnosed and intravenous antibiotics were commenced. The patient was admitted under the orthopaedic surgeons with her treatment consisting of multiple surgical procedures over a prolonged duration. Although lengthy, her postoperative recovery was unremarkable. Based on this case report and our review of the literature, we highlight the potential complications associated with corticosteroid knee joint injections and suggest certain patients for whom we would recommend secondary referral before any intervention in primary care.
Introduction
Corticosteroid knee injections are being increasingly used in the conservative management of knee osteoarthritis (OA). The Cochrane collaboration conducted a systematic review in 2006 of 28 RCTs investigating the efficacy and safety of corticosteroid joint injections in knee OA (Citation1). The review confirmed the short-term benefits of corticosteroid joint injections, which were more effective than placebo or hyaluronic acid (HA) with respect to pain relief for up to three weeks. However, longer-term benefits (from four weeks on) of corticosteroids are questionable, as corticosteroids were not statistically proven as effective with respect to function and pain relief as HA. Since this Cochrane meta-analysis, in 2009 Bannuru et al., published a systematic review and meta-analysis yielding similar conclusions; that corticosteroids provide symptomatic relief of pain for up to four weeks, but that HA is superior longer-term (Citation2). While the literature portrays corticosteroid injections for knee OA amounting to a short-term treatment of a chronic problem (Citation3), they nevertheless have a proven and important role in the community as a successful form of conservative treatment prior to the option of arthroplasty.
Case report
An obese 71-year-old female presented to her GP with worsening left knee pain and no history of acute trauma. She described nocturnal pain and difficulty managing stairs. On examination, the knee joint was stable and found to exhibit a full range of motion limited only secondary to an increased body mass index. Inflammatory markers were normal. Weight-bearing knee radiographs noted changes consistent with OA. A corticosteroid joint injection was administered at the general practice via a medial approach. This provided minimal pain relief in the subsequent days. Over the next four days she experienced worsening pain, swelling and erythema of her left knee and re-presented to her GP. Cellulitis was diagnosed and the patient was commenced on oral antibiotics. She was referred to the casualty department and immediately commenced on intravenous antibiotics. After being assessed by the orthopaedic service, a diagnosis of an abscess was made based on clinical findings. These included a large area of cellulites with an underlying anteromedial knee swelling measuring 7 × 5 cm and grossly elevated inflammatory markers. The patient was taken to the operating theatre where the abscess was incised and a copious amount of pus discharged. After drainage, the large remaining abscess cavity was debrided and washed out () and a vacuum assisted closure (VAC) device applied. Two weeks later, the patient was discharged on oral antibiotics and with a portable VAC device. Though lengthy, her postoperative recovery was otherwise unremarkable. Re-admission for definitive closure was organized four weeks later.
Figure 1. Postoperative photograph of both knees (anterior view), illustrating the large cavity following surgical incision, drainage and debridement of the abscess secondary to corticosteroid knee joint injection.

Discussion
The recommendations from the NICE guidelines (Citation4) suggest three core treatments for every patient with osteoarthritis. These are education and advice, strengthening exercises that include aerobic fitness training and weight loss in cases of those who are overweight or obese. When these fail, relatively safe pharmacological options that include paracetamol and topical NSAIDs are second line treatment options. Finally, third line treatment modalities considered to be adjuncts include four groups, namely pharmacological agents (oral NSAIDs, opioids, intra-articular corticosteroid joint injections), self-management techniques (heat or ice packs), non-pharmacological options (supports, braces, TENS) and lastly, surgery (joint arthroplasty). In comparison to the NICE guidelines, the American Academy of Orthopaedic Surgeons clinical practice guideline on the treatment of OA of the knee suggests intra-articular corticosteroids for short-term pain relief for symptomatic patients (Citation5). Their treatment algorithm indicates the use of corticosteroid injections as second line treatment, immediately after a failed initial trial of physical therapy and NSAIDs (Citation6). In Ireland, the injection itself is often performed in secondary care by orthopaedic surgeons and rheumatologists (and trainees in either specialty) with up to 20% of orthopaedic outpatients in our practice having it performed in the clinic at the time of their appointment. As in many European countries, the role of general practitioners (GPs) in chronic disease management has long existed with joint injections also frequently performed in primary care. It is widely perceived that serious complications from corticosteroid knee joint injections are rare, the most serious being joint infection, which can have a mortality of up to 11% (Citation7). It is also broadly perceived that their benefits in treating symptomatic knee osteoarthritis significantly outweigh the risks. While this may be true, potential catastrophic complications include septic arthritis and this may be more common than perceived (Citation8). Reported rates of infection range from 1 in 3000 (Citation9) to 1 in 10 000 (Citation10) to 1 in 50 000 (Citation11). In a survey of 100 surgeons, 100 rheumatologists and 50 GPs conducted by Charalambous et al., 12.6% of those surveyed had ever encountered septic arthritis (which presumably represents only a percentage of overall bacterial infection) following joint injection (Citation8). In the literature, there are several case reports documenting other local and systemic complications (besides infectious) from corticosteroid injections of the knee. Local complications include self-limiting post-injection flare, skin atrophy, tendinopathy, increased risk of patellar tendon rupture, albicans arthritis, asymptomatic hydroxyapatite calcifications, tendon and fascial ruptures in treatment of athletic injuries, Nicolau syndrome and saphenous neuropathy in an obese patient where anatomy was likely obscured. Systemic complications reported include sudden loss of vision, osteonecrosis, adrenal suppression, and transient hyperglycaemia. Most of the above systemic and local complications are isolated case reports, and therefore, can be considered very rare, but nevertheless highlight the importance of an aseptic technique, accurate intra-articular needle placement and awareness of the possible systemic effects when injecting corticosteroids locally. This case report highlights a serious but avoidable complication that most likely arose because of inadequate aseptic technique and inaccurate extra-articular placement of the knee injection.
Performing knee joint injections under aseptic conditions is of utmost importance in minimizing infectious complications. However, in the literature there appears to be wide variation in the degree of precautions used. In a survey by Charalambous et al., only 32.5% of respondents always used sterile gloves, only 16.3% used sterile towels to isolate the injection site, and 8.9% did not change needles between drawing the steroid and injection (Citation8). For standard guidelines on aseptic technique see Neustadt (Citation12).
In the literature, three publications have suggested that correct intra-articular placement may not be entirely necessary for clinical benefit (Citation13–15). However, most authors agree that accurate intra-articular needle placement will both maximize efficacy and minimize procedure-related complications. Several have aimed to evaluate this accuracy by fluoroscopic imaging, and have shown that more than 20% of injections are in fact not intra-articular (Citation14,Citation16).
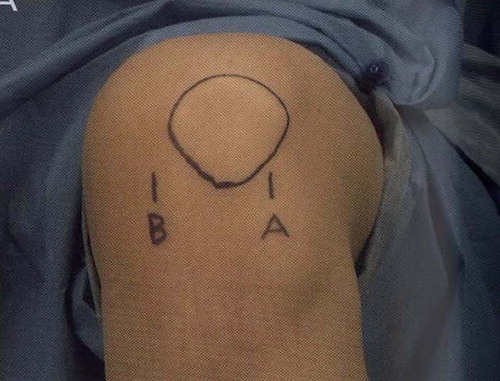
In our experience with knee joint injections, anatomical landmarks and tactile feedback are relied upon to achieve accurate intra-articular needle placement, with a medial approach with the knee in extension being most commonly used. However, there does not appear to be any evidence that a medial approach is the most accurate or effective. It has also been found that accuracy is lowest with a medial mid-patellar approach (56%) and highest with an anterolateral approach () (85%, P < 0.001) (Citation17). In the review paper by Hall and Buchbinder it was concluded that standard landmarks are suitable for most cases, but they advised the use of ultrasound guidance to maximize efficacy in technically difficult cases, such as in obese patients (Citation18).
Figure 2. Illustration depicting the anterolateral entry point for knee injections; with the knee in 90 degrees of flexion, the needle entry point (just above ‘A’) should be in the palpable soft spot between the patella, lateral femoral condyle and proximal tibia (Gerdy's tubercle).
While it appears that those GPs performing most injections in the community have had training presumably under specialist supervision, based on this case report and our review of the literature, there are certain patients for whom we would recommend secondary referral before any intervention in primary care (). It is for these reasons that in our co-author's general practice, these select patients are referred to secondary care for intra-articular knee joint injections.
Table I. For primary care providers: when NOT to inject.
Conclusions
While most joint injections in primary care are performed by a small number of GPs who have prior hospital training in related specialties, based on our review of the literature, we suggest that secondary referral is best advised in certain patients to both maximize efficacy and minimize the risk of complications. In conclusion, to minimize potential catastrophic complications, we must ensure that training methods and good volumes of workload for performing joint injections exist.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database Syst Rev. 2006;19: CD005328.
- Bannuru RR, Natov NS, Obadan IE, Price LL, Schmid CH, McAlindon TE. Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: A systematic review and meta-analysis. Arthritis Rheum. 2009;15:1704–11.
- Hepper CT, Halvorson JJ, Duncan ST, Gregory AJ, Dunn WR, Spindler KP. The efficacy and duration of intra-articular corticosteroid injection for knee osteoarthritis: A systematic review of level I studies. J Am Acad Orthop Surg. 2009;17:638–46.
- National Institute for Health and Clinical Excellence. Osteoarthritis: National clinical guideline for care and management in adults. London: NICE; 2008. Available at http://www.nice.org.uk/CG059 (accessed 28th January 2011).
- Feeley BT, Gallo RA, Sherman S, Williams RJ. Management of osteoarthritis of the knee in the active patient. J Am Acad Orthop Surg. 2010;18:406–16.
- Richmond J, Hunter D, Irrang J, Jones MH, Snyder-Mackler L, Van Durme D, . American Academy of Orthopaedic Surgeons clinical practice guideline on the treatment of osteoarthritis (OA) of the knee. J Bone Joint Surg Am. 2010;92: 990–3.
- Peters RH, Rasker JJ, Jacobs JW, Prevo RL, Karthaus RP. Bacterial arthritis in a district hospital. Clin Rheumatol. 1992;11:351–5.
- Charalambous CP, Tryfonidis M, Sadiq S, Hirst P, Paul A. Septic arthritis following intra-articular steroid injection of the knee – a survey of current practice regarding antiseptic technique used during intra-articular steroid injection of the knee. Clin Rheumatol. 2003;22:386–90.
- Gedda, PO, Juhlin CH. Septic arthritis after intra-articular cortisone injection. Sven Lakartidn. 1959;56:3341–3.
- Fitzgerald RH Jr. Intrasynovial injection of steroids uses and abuses. Mayo Clin Proc. 1976;51:655–9.
- Gray RG, Tenenbaum J, Gottlieb NL. BDG-179-7282481779 Local corticosteroid injection treatment in rheumatic disorders. Semin Arthritis Rheum. 1981;10:231–54.
- Neustadt DH. Intra-articular injections for osteoarthritis of the knee. Cleve Clin J Med. 2006;73:897–8; 901–4; 906–11.
- Sambrook PN, Champion GD, Browne CD, Cairns D, Cohen ML, Day RO, . Corticosteroid injection for osteoarthritis of the knee: Peripatellar compared to intra-articular route. Clin Exp Rheumatol. 1989;7:609–13.
- Jones A , Regan M, Ledingham J, Patrick M, Manhire A, Doherty M. Importance of placement of intra-articular steroid injections. Br Med J. 1993;307:1329–30.
- Cunnington J, Marshall N, Hide G, Bracewell C, Isaacs J, Platt P, . A randomised, controlled, double blinded study of ultrasound guided corticosteroid joint injection in patients with inflammatory arthritis. Arthritis Rheum. 2010;1862–9.
- Bliddal H. Placement of intra-articular injections verified by mini air-arthrography. Ann Rheum Dis. 1999;58:641–3.
- Esenyel C, Demirhan M, Esenyel M, Sonmez M, Kahraman S, Senel B, . Comparison of four different intra-articular injection sites in the knee: A cadaver study. Knee Surg Sports Traumatol Arthrosc. 2007;15:573–7.
- Hall S, Buchbinder R. Do imaging methods that guide needle placement improve outcome? Ann Rheum Dis. 2004;63: 1007–8.
- Toda Y, Tsukimura N. A comparison of intra-articular hyaluronan injection accuracy rates between three approaches based on radiographic severity of knee osteoarthritis. Osteoarthritis Cartilage 2008;16:980–5.
- Schumacher HR, Chen LX. Injectable corticosteroids in treatment of arthritis of the knee. Am J Med. 2005;118: 1208–14.
- Papavasiliou AV, Isaac DL, Marimuthu R, Skyrme A, Armitage A. Infection in knee replacements after previous injection of intra-articular steroid. J Bone Joint Surg Br. 2006;88:321–3.
- Ostensson A, Geborek P. Septic arthritis as a non-surgical complication in rheumatoid arthritis: Relation to disease severity and therapy. Br J Rheumatol. 1991;30:35–8.
- Hall S, Buchbinder R. Do imaging methods that guide needle placement improve outcome? Ann Rheum Dis. 2004; 63:1007–8.