
Abstract
Background and purpose — The PRECICE intramedullary limb lengthening system uses a new technique with a magnetic rod and a motorized external remote controller (ERC) with rotational magnetic field. We evaluated the reliability and safety of the PRECICE system.
Methods — We compared our preliminary results with PRECICE in 24 patients (26 nails) with the known difficulties in the use of mechanical lengthening devices such as the ISKD. We used the Paley classification for evaluation of problems, obstacles, and complications.
Results — 2 nails were primarily without function, and 24/26 nails lengthened over the desired distance. Lengthening desired was 38 mm and lengthening obtained was 37 mm. There were 2 nail breakages, 1 in the welding seam and 1 because of a fall that occurred during consolidation. ERC usage was problematic mostly in patients with femoral lengthening. Adjustment of the ERC was necessary in 10 of 24 cases. 15 cases had implant-associated problems, obstacles were seen in 5 cases, and complications were seen in each of 4 cases.
Interpretaion — The reliability of the PRECICE system is comparable to that of other intramedullary lengthening devices such as the ISKD. The motorized external remote controller and its application by the patients is a weak point of the system and needs strict supervision.
Intramedullary limb lengthening nails are used for distraction of long bones, particularly in the leg. The PRECICE system (Ellipse Technologies, Irvine, CA), a new motor-driven lengthening technique, which has CE certification and Food and Drugs Administration (FDA) approval, has now been available on the world market for 3 years. The PRECICE system differs in several respects from the mechanical systems that one was previously familiar with, both with regard to its handling and implantation and with regard to its use by the patient for daily lengthening. Another system, the intramedullary skeletal kinetic distractor—ISKD (Orthofix International, Verona, Italy)—which is based on a purely mechanical rotatory system, was introduced by Cole et al. (Citation2001) and after revision in 2012 is still available worldwide.
Whereas extensive scientific data are available for the ISKD (Thonse et al. Citation2005, Simpson et al. Citation2009, Burghardt et al. Citation2011, Kenaway et al. 2011, Papanna et al. Citation2011, Schiedel et al. Citation2011, Mahboubian et al. Citation2012, Wang and Edwards Citation2012), there have been no reports in the literature on limb lengthening with the PRECICE system. The technique used for lengthening is based on a system of magnetic expansion control (MAGEC) rods used in spinal surgery (Akbarnia et al. Citation2012, Cheung et al. Citation2012). An external remote controller (ERC) is required, which causes the magnets that are integrated into the drive thread rod to rotate, making a thinner nail element telescope out of a thicker surrounding nail. Descriptions of the mechanism have been published by the manufacturer (CitationEllipse Inc. 2013) and by Akbarnia et al. (Citation2012).
We studied implant-associated difficulties and safety with the PRECICE system and compared our results with published data on the ISKD system.
Patients and methods
Between June 2012 and March 2013, 26 PRECICE nails were implanted for lengthening at our hospital. All the patients were included prospectively in accordance with an epidemiological study design, so that the initial results using lengthening with the PRECICE device could be compared with other familiar methods that have been in use for many years. Radiography with anteroposterior leg views, with the patient standing, were obtained before surgery and during or after consolidation. During the lengthening process, measurement radiographs were taken every 14 days.
Classification of the difficulties during treatment
The occurrence of any problems, obstacles, and complications was recorded after lengthening was completed. The Paley classification was used for comparison with other lengthening procedures and external lengthening procedures (Paley Citation1990). We only analyzed difficulties inherent in the process, caused by the drive mechanism and ERC. For comparison, we used data for ISKD patients that were available in the literature (Schiedel et al. Citation2011).
Problems. A problem in intramedullary lengthening was defined as a possibly expected or observed difficulty that occurred during implantation, the latency phase, distraction, or consolidation that was completely resolved within the normally planned treatment period without any need for a repeat operation or intervention under anesthesia. An example of an implant-associated problem was adjustment of the ERC in the outpatient clinic to carry out further distraction, if there was a difference between the radiograph and the controller setting.
Obstacles. An obstacle was recorded if any intervention under anesthesia was required due to dysfunction of the device, or if problems occurred that could not be resolved without anesthesia.
True complications consisted of all intraoperative and perioperative complications, whether local or systemic, and any subsequent difficulties—either during or after removal of the PRECICE device. Minor complications were defined as having occurred if the initial lengthening goal had been achieved but a complication persisted beyond the normal completion of treatment, even though it was resolved without surgery. From an implant-specific point of view, a nail breakage is a true complication. It depends on the objective of a study whether this would be described as an obstacle. Exchanging the PRECICE device may resolve the obstacle (e.g. no function) with the patient under general anesthesia but without any delay in the treatment, and with the desired lengthening being achieved. Major complications were defined as having occurred if the initial lengthening was achieved, but a complication was still present at the end of the planned treatment and had to be resolved with additional surgery, or remained unresolved; and failing to achieve the planned lengthening, by 1 cm or more.
For this report of results with the PRECICE, a shorter follow-up period of 3 months after the end of consolidation or approval of full weight bearing was regarded as adequate.
Calculated parameters
The reliability of an intramedullary lengthening system is the ratio of the number of implanted lengthening systems and the number of successfully ended treatment courses (lengthening and bony healing) with the lengthening system remaining in place until bony consolidation. Any case with the need for exchange nailing for any reason and any case with switching over to another (external or internal) lengthening method was regarded as an unsuccessful treatment. The accuracy of an intramedullary or external lengthening system was calculated by dividing the length reached by the length planned.
Drive technique
shows a section through a PRECICE nail. The positioning of the magnet on the threaded rod is clearly visible. A ratchet drive based on tensile loading pushes the distal thin core of the nail out of the proximal thicker nail sheath, in which the magnet and the drive rod are firmly anchored.
Figure 1. A PRECICE nail transected with a laser. The integrated magnet (arrow) is visible on the threaded rod.

Surgical technique
In the first-generation PRECICE, which was used in this study, an extension rod, available with nail diameters of 10.7 mm and 12.5 mm, was screwed onto the lengthening unit using a set screw. 6 nail lengths are available (230, 255, 280, 305, 330, and 355 mm). The lengthening capacity is 65 mm in total. The magnet is incorporated into the lengthening unit and can be imaged intraoperatively on the C-arm (CitationEllipse Inc. 2013). A new generation of solid nails has been available from the manufacturer since June 2013, making both custom nail diameters available with various nail lengths and simplifying the surgical technique, without any extension rods and set screws. Minimally invasive implantation is possible. In our patients, osteotomies were performed by the multiple drill-hole technique with subsequent cortical chiselling. The postoperative latency period was 7 days in femoral lengthening and 10 days in tibial lengthening. In programming the ERC, the daily distraction rate was initially set to 1 mm for femur und 0.66 mm for tibia. Postoperatively, it is necessary to know the exact level of the magnet; the position can be drawn on the skin with a permanent marker, relative to position of the skin incision for the osteotomy (often identical).
Manipulation by the patient
The control device of the ERC only measures the number of rotations of the magnets in the ERC, not the rotations of the magnet in the nail. Feedback on whether the rotations have actually been successfully carried out inside the nail is not technically possible. A discrepancy between the lengthening measurable on radiography and the length actually obtained (shown by the ERC) occurs if the patient is uncertain about using the system or if the soft tissue is thicker.
Use in the tibia is simple, as there is almost direct bone contact. For the femur with an antegrade nail, the ERC often has to be pressed onto the skin from the side in the lateral position (). The ventral approach can quickly exceed the effective range of the magnetic field, which is only 5.5 cm. Due to the size of the ERC, it cannot be used proximally enough above the magnet, particularly in more corpulent patients, so they also need help from an assistant. Drawing of the level of the magnet on the skin is necessary for safe application, and this should be explained to the patient relative to a permanent skin mark (such as the osteotomy scar) that can always be reproduced on the radiograph (). The programming of the full possible lengthening distance is set by the therapist before the start, as is the maximum permitted daily lengthening. With optimal adjustment, the patient only has to switch on the ERC at the agreed intervals and activate it by pressing a button. Patients are not then able to alter either the daily lengthening distance or the total distance.
Figure 2. Application of the external remote controller. The weak magnetic field has to be pressed as much as possible into the soft tissue. A range of 5.5 cm is the maximum distance for proper functioning of the magnetic device.
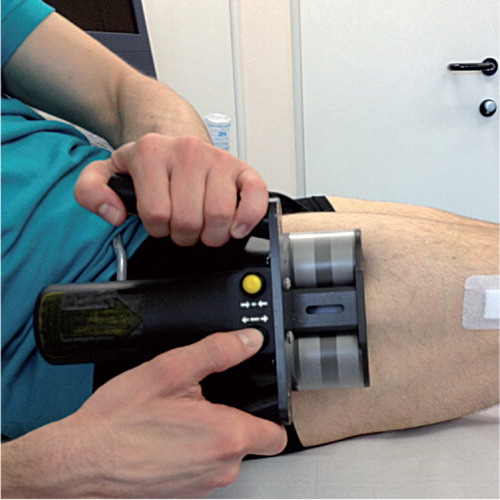
Figure 3. The application level depends on the positioning of the magnet, which can be identified in relation to the osteotomy level on the radiograph (see arrow).
Ethics
We received approval for the study from our institutional review board (2VRö1).
Results
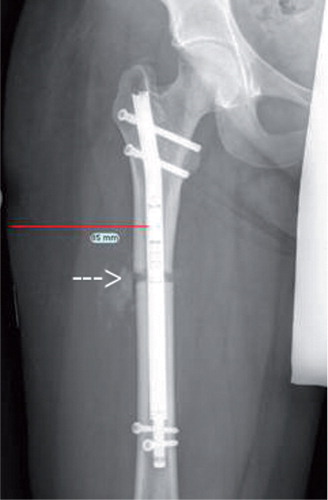
Over 1 year, we implanted 26 PRECICE nails in 24 patients (14 males): 15 were femoral antegrade, 5 were femoral retrograde, and 6 were tibial. At the time of surgery, the average age of the patients was 19 (12–31) years. 2 nails initially failed to function; an exchange was carried out in 1 case, and in the other the procedure was changed and the patient was excluded. 1 patient with short stature received bilateral parallel tibial lengthening, and the other 22 patients were treated for various indications (congenital skeletal dysplasia, longitudinal reduction defects, idiopathic shortening, posttraumatic condition, previous infection, previous resection, and post-tumor resection). Premature consolidation in 1 patient was resolved with a re-osteotomy, classified as a non-implant-associated obstacle. 2 nails broke during the consolidation phase, in 1 case due to a fatigue failure along the welding seam ( and ). The other nail broke at the connection between the lengthening unit and the extension rod when the patient fell accidentally. This was classified as a true complication, since the initial surgical goal with the PRECICE nail (lengthening and providing static stabilization until bone consolidation had been achieved) was not reached. The reliability rate of the PRECICE system—the rate with which it successfully remained in place until bony consolidation—was 22/26 nails overall, 4/6 tibial nails and 18/20 femoral nails.
Figure 4. Radiograph from a 16-year-old boy, 6 months after implantation of a femoral PRECICE with a trochanteric approach for lengthening of 50 mm. After 3 months (35 mm), repeat osteoclasia due to early consolidation had become necessary. Breakage of the welding seam (arrow) occurred a further 3 months later, 1 month after the end of the distraction period.
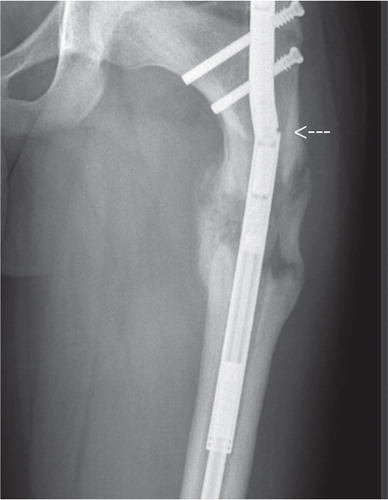
Figure 5. Nail breakage at the welding seam in the PRECICE device in the patient shown in .

The distraction targets were reached following an initial latency period averaging 7 (2–10) days, with an average planned lengthening distance of 38 (20–50) mm within an average of 64 (25–200) days. The mean lengthening achieved was 37 (15–50) mm, which was therefore slightly below the planned amount (). The reasons for failing to reach the planned degree of lengthening varied. The greatest deviation, 8 mm when 23 mm was planned and 15 mm was achieved, was due to omission of radiographic measurement at the end of the calculated lengthening. Problems were noted in 11 of 23 cases, with the ERC being re-programmed—sometimes several times—in order to reach the lengthening goal. Pain and neuromuscular problems during lengthening were rare, occurring in 5 of 23 patients. In comparison with studies including larger groups of ISKD patients, this was an improvement (Simpson et al. Citation2009, Burghardt et al. Citation2011, Kenaway et al. 2011, Schiedel et al. Citation2011). The overall accuracy of the lengthening with the PRECICE system (planned length vs. length reached) was 97% ().
Table 1. Empirical data for the group of 24 patients who underwent surgery with 26 implantations of a PRECICE device, and reliability of the device
Table 2. Results for 23 patients with implantation of 24 PRECICE nails and successful lengthening of the bone: accuracy of lengthening, implant-associated problems, obstacles, and complications
Discussion
In this early series, the reliability rate of the PRECICE system was 0.9 (22 of 26 implanted nails), in comparison to 0.8 (57 of 69) in ISKD patients in a comparable study (Schiedel et al. Citation2011).
There is one substantial difference between the 2 systems with regard to dysfunction. In the “historical” ISKD group, jamming of the mechanism in an excessively antecurved or insufficiently drilled medullary cavity was the most frequent reason for dysfunction, in addition to the choice of inexperienced surgeons of a nail system that was too long. In the PRECICE system, the thinner-thread rod means that it is possible to break. This can happen if the system has to work against incipient premature consolidation or when shortening exceeding the minimum starting position is inadvertently carried out. This is immediately evident during surgery, due to the free telescoping of the inner nail section out of the nail sheath.
The possible direction of applying the ERC, and the gap between the PRECICE nail and the ERC resulting from soft tissue in the thigh—particularly in obese patients—may make magnet-induced rotations difficult. Whereas use of the system is not advised in patients with a BMI of > 35 (Ellipse 2013), we would recommended calculating the thickness of the soft tissue over the bone at the femur preoperatively, since even when the ECR is applied on the side in the lateral position, only a maximum distance of 51 mm can be traversed by the magnetic field. Without any soft tissue in the magnetic field, the maximum dimension would be 100 mm. During the first few days of lengthening, after a latency period of 7–10 days after surgery, the pressure required on the soft tissue with the ECR is often still painful for the patient. In the USA, due to the long delay in FDA approval for outpatient use of the ERC by patients themselves at home, it was possible and necessary for patients to spend the entire lengthening period close to the hospital. This was not necessary initially in Europe following CE approval, so that all patients (and relatives) were able to carry out lengthening at home after successful training in the use of the ERC. This might possibly explain the unexpectedly high rate of patients requiring reprogramming of the ERC, as the distraction lengths achieved on radiography at the time of the expected last day of lengthening did not correspond to the adjustment of the ERC.
This problem occurred in 10 of 23 patients. The radiographs on average showed a regenerate that was 10% shorter than expected. In several cases, reprogramming alone was not sufficient, since insufficient distraction of the bone on the radiograph in comparison to the ERC setting recurred. This may be explained by the fact that during the 7-minute application of the ECR required to achieve 1 mm of lengthening, even slight slippage can cause partial loss of contact with the magnetic field.
The mean accuracy of lengthening with the PRECICE, 97%, is similar to that in the comparable ISKD study (96%) (Schiedel et al. Citation2011), although the accuracy with PRECICE was only achieved as a result of reprogramming of the ERC. A major problem with the ISKD is eliminated by motorization in the PRECICE system: no external, often painful rotational manipulation of the leg is required. The obstacle represented by pole switching no longer being possible due to jamming of the mechanism and premature consolidation is also alleviated.
In view of the continuing improvements to the system by the manufacturer, current problems with the PRECICE system will probably be addressed.
FS and MH conceived the study. FS, BV, HT, and BS assembled and analyzed the data. FS, BV, HT, MH, and RR performed the operations and follow-ups. BV, HT, BS, and RR made the radiographic measurements and arranged data. FS and RR prepared the initial draft and performed the comparison to the historical patient group. GG and RR made substantial changes to the manuscript. BV and RR revised the entire manuscript.
No competing interests declared.
- Akbarnia BA, Mundis G M Jr, Salari P, Yaszay B, Pawelek JB. Innovation in growing rod technique: a study of safety and efficacy of a magnetically controlled growing rod in a porcine model. Spine 2012; 37: 1109–14.
- Burghardt RD, Herzenberg JE, Specht SC, Paley D. Mechanical failure of the Intramedullary Skeletal Kinetic Distractor in limb lengthening. J Bone Joint Surg (Br) 2011; 93: 639–43.
- Cheung KM, Cheung JP, Samartzis D. Magnetically controlled growing rods for severe spinal curvature in young children: a prospective case series. Lancet 2012; 379: 1967–74.
- Cole JD, Justin D, Kasparis T, DeVlught D, Knobloch C. The intramedullary skeletal kinetic distractor (ISKD): first clinical results of a new intramedullary nail for lengthening of the femur and tibia. Injury (Suppl 4) 2001; 32: SD129–39.
- Ellipse Inc., Irvine, California, USA. Remote control technology for the treatment of limb length discrepancies: PRECICE®. Available at: http://www.ellipse-tech.com/pages/PRECICE (accessed 25 May 2013).
- Kenawey M, Krettek C, Liodakis E, Wiebking U, Hankemeier S. Leg lengthening using intramedullary skeletal kinetic distractor: results of 57 consecutive applications. Injury 2011; 42: 150–5.
- Mahboubian S, Seah M, Fragomen AT, Rozbruch SR. Femoral lengthening with lengthening over a nail has fewer complications than intramedullary skeletal kinetic distraction. Clin Orthop 2012; (470): 1221–31.
- Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop 1990; (250): 81–104.
- Papanna MC, Monga P, Al-Hadithy N, Wilkes RA. Promises and difficulties with the use of femoral intra-medullary lengthening nails to treat limb length discrepancies. Acta Orthop Belg 2011; 77: 788–94.
- Schiedel FM, Pip S, Wacker S, Pöpping J, Leidinger B, Rödl R. Intramedullary limb lengthening with the Intramedullary Skeletal Kinetic Distractor in the lower limb. J Bone Joint Surg (Br) 2011; 93: 788–92.
- Simpson AH, Shalaby H, Keenan G. Femoral lengthening with the Intramedullary Skeletal Kinetic Distractor. J Bone Joint Surg (Br) 2009; 91: 955–61.
- Thonse R, Herzenberg JE, Standard SC. Limb lengthening with a fully implantable, telescopic, intramedullary nail. Oper Tech Orthop 2005; 15: 355–62.
- Wang K, Edwards E. Intramedullary skeletal kinetic distractor in the treatment of leg length discrepancy—a review of 16 cases and analysis of complications. J Orthop Trauma 2012; 26: e138–44.