

Abstract
Background:
Patients with unresectable, metastatic colorectal cancer with wild type Kirsten ras mutational status are eligible for sequential treatments which include monoclonal antibodies as first line (1L), second line (2L), or third line (3L) regimens.
Objective:
To compare the economic outcomes of different sequences which include monoclonal antibodies for the treatment of unresectable metastatic colorectal cancer.
Methods:
Individual drug regimens for 1L, 2L, and 3L treatments were compiled according to the clinical studies in the Summary of Product Characteristics for monoclonal antibodies. They were combined into plausible treatment sequences. Health outcomes were approximated using additive median PFS benefit, and economic outcomes were calculated with a treatment sequencing costing tool. Limitations of the analysis include the clinical trial data sources, cost assumptions, and the additive PFS approach.
Results:
Seventeen sequences were evaluated. Results of the analysis show that sequences including 1L anti-EGFRs generally have relatively low-to-medium health outcomes at the highest comparative sequence costs compared to sequences including 2L anti-EGFRs, which have lower health outcomes at the lowest cost. Sequences including 3L anti-EGFRs (sequential bevazicumab-based 1L and 2L) have the highest health outcomes, with potential cost savings of €5972–€11,676 if replacing 2L anti-EGFRs or an additional cost of €5909–€12,708 if replacing 1L anti-EGFR regimens.
Conclusion:
Clinical sequences consisting of 1L and 2L line bevacizumab followed by 3L anti-EGFR potentially yield the greatest health outcomes associated with a reasonable trade-off in additional cost when replacing 1L anti-EGFRs and are potentially cost-saving if replacing 2L anti-EGFRs, per patient per lifetime. To maximize health outcomes, optimal sequences include anti-EGFRs as 3L regimen, with an approximately equivalent trade-off in costs between the most costly (anti-EGFR 2L) and least costly (anti-EGFR 1L) sequences.
Introduction
Colorectal cancer (CRC) is the second and third most common cancer for women and men, respectively, accounting for ∼8% of all cancer deaths worldwide. Estimates indicate that there were 1,233,000 new cases and 608,000 deaths worldwide in 2008 due to CRCCitation1. Up to 20% of patients present with metastatic colorectal cancer (mCRC)Citation2, of which a minority are eligible for resectionCitation3. In unresectable patients, goals of treatment include stopping tumor progression and prolonging overall survival (OS), while controlling for symptoms and sustaining quality-of-lifeCitation3.
Previously, cytotoxic agents (e.g. fluoropyrimidines: 5-fluorouracil or capecitabine, oxaliplatin, irinotecan) as single agents and (mostly) chemotherapy combination regimens such as folinic acid/5-fluorouracil/oxaliplatin (FOLFOX); folinic acid/5-fluorouracil/irinotecan (FOLFIRI) and capecitabine/oxaliplatin (XELOX) were the mainstay of treatment. Nowadays, monoclonal antibodies against vascular endothelial growth factor (VEGF) or epidermal growth factor receptor (EGFR) are used in combination with chemotherapy to further improve patient outcomesCitation3. Two anti-VEGFs (bevazicumab, aflibercept) and two anti-EGFRs (cetuximab, panitumumab) are potentially available for the treatment of unresectable metastatic CRC.
Cetuximab (CET) is a monoclonal antibody against EGFR indicated for the treatment of KRAS WT patients only. In 1L regimens it is used in combination with irinotecan or FOLFOX; or as monotherapy in patients failing oxaliplatin and irinotecanCitation4. CET + FOLFIRI has demonstrated statistically significant improvement in PFS and OS vs FOLFIRI aloneCitation5, and inconsistent evidence suggests an improvement in PFS for CET + fluoropyrimidine/oxaliplatin regimensCitation5–8. In 2L regimens: CET + irinotecan demonstrated a statistically significant improvement in PFS vs irinotecan aloneCitation9. In 3L regimens CET + BSC demonstrated a statistically significant improvement in PFS and OS vs BSC aloneCitation10,Citation11.
Panitumumab (PAN) is a monoclonal antibody indicated for the treatment of KRAS WT patients in combination with FOLFOX as 1L, with FOLFIRI in 2L and as monotherapy for patients failing fluoropyrimidine, oxaliplatin, and irinotecanCitation12. PAN + FOLFOX (1L) and PAN + FOLFIRI (2L) demonstrated a statistically significant improvement in PFSCitation13,Citation14. For 3L regimens, PAN + BSC demonstrated a statistically significant improvement in PFS vs BSC aloneCitation15. At the time of this analysis, the sequential use of anti-EGFRs (i.e. as 1L followed by 2L treatment) had not been evaluated in clinical studies.
Bevacizumab (BEV) is a monoclonal antibody against VEGF indicated in the treatment of mCRC patients regardless of KRAS mutation status. In 1L regimens, BEV demonstrated a statistically significant improvement in OS and PFS in combination with 5-fluorouracil (5FU)/leucovorin/irinotecanCitation16, and a statistically significant improvement in PFS in combination with fluoropyrimidines plus oxaliplatinCitation17. In 2L therapy BEV high dose (10 mg) demonstrated a statistically significant improvement in OS and PFS in combination with FOLFOX4Citation18. Bevacizumab low dose (5 mg) 2L beyond 1st progression in patients pre-treated with bevacizumab in 1L has been evaluated in a phase III randomized controlled trialCitation19.
Aflibercept is a recombinant fusion protein consisting of VEGF -binding portions from the extracellular domains of human VEGF Receptors 1 and 2 fused to the Fc portion of the human IgG1Citation20,Citation21. In 2L regimens, aflibercept demonstrated a statistically significant improvement in OS and PFS in combination with FOLFIRICitation20,Citation21. There is currently no randomized phase III data for aflibercept in 1L.
The fundamental differences between anti-VEGFs and anti-EGFRs are their mode of action. All patients are eligible for treatment with anti-VEGFs independent of RAS status, and no sub-group of patients with more pronounced clinical outcomes in terms of progression-free survival (PFS) and overall survival (OS) has been identified. In contrast, KRAS Wild-Type (WT) status is a mandatory feature for the use of cetuximab and panitumumab. Out of all patients with mCRC, up to 60% will test positive for KRAS WT disease and be eligible for anti-EGFR therapyCitation22. Patients testing positive for KRAS Mutant-Type (MT), which account for up to 50% of all tumors, may not respond to treatment.
Oncologists are increasingly required to consider the economic impact of different treatment sequences in addition to patient health outcomes. This analysis seeks to evaluate and compare the health and economic impacts of a range of sequences which include anti-VEGFs and anti-EGFRs for the treatment of unresectable metastatic colorectal cancer.
Objective
The objective of the research was to compare the health and economic outcomes of different sequential treatment approaches which include monoclonal antibodies against vascular endothelial growth factor and/or epidermal growth factor receptor for the treatment of unresectable metastatic colorectal cancer.
Methods
The following terminology is used in the analysis: drug regimens are combinations of drugs generally consisting of a biologic and backbone chemotherapy; therapy lines refers to first, second, and third line drug regimens; sequences(ing) refer to combinations of first, second and third therapy lines.
To achieve the objective, the research set out to:
Identify drug regimens available for the treatment of mCRC from the pivotal studies referenced in the Summary of Product Characteristics of the biologic agents.
Compare the monthly cost of different drug regimens for first, second, and third therapy lines.
Combine 1L, 2L, and 3L drug regimens into clinically plausible treatment sequences which were verified by clinical oncologists.
Compare different sequences with respect to health and cost outcomes. In the analysis, the term ‘health outcomes’ was used to represent the clinical outcomes and approximated by progression-free survival data.
To identify drug regimens, a list of pivotal studies was compiled from the efficacy section of each summary of product characteristics (SmPCs) for BEV, CET, and PAN, respectively, in addition to the ML18147 studyCitation4,Citation12,Citation19,Citation23. Drug regimens, dosing schedules, and median PFS outcomes were extracted from each study to be used for calculation of costs and comparison of health outcomes. First, second, and third line drug regimens were combined into plausible treatment sequences for three possible scenarios: where an anti-EGFR is used as 1L, 2L, or 3L treatment, respectively. Treatment sequences were constructed on the basis of licensed indications (SmPCs accessed December 2012)Citation4,Citation12,Citation23, feasibility of combinations (example anti-EGFRs cannot be used in sequence; chemotherapy backbones crossover from one treatment line to the next) and expert opinionCitation24–26. The validity of the clinical sequences was verified by clinical oncologists who contributed to this analysisCitation24–26. To compare health outcomes, progression-free survival (PFS) was selected as a proxy for clinical benefit. Due to the absence of sequential randomized control trial data for biologics, median PFS values were added according to the corresponding clinical trial data.
To compare costs, the total monthly cost and total sequence cost per patient per lifetime according to 1L, 2L, and 3L combinations were calculated for the base case country Germany using a statutory health insurance (Gesetzliche Krankenversicherung) perspective. The focus of the analysis was direct drug and administration costs, indirect costs due to adverse events were not included, as detailed in the discussion section. A Treatment Sequencing Costing (TSC) model was developed in Microsoft Excel (Microsoft, Redmond, WA) to calculate the monthly and sequence costs of different drug regimens. It consists of user input sheets which can be customized with user-input drug and administration cost data to perform analyses consistently across different countries and which form the basis for the calculation of the individual drug regimens per line of therapy. A bottom up (micro-costing) approach is used for each therapy line to calculate the monthly cost per drug regimen based on the German drug dosage, drug cost per milligram, cycle length, and administration cost information. Total sequence cost per patient lifetime was calculated as the product of the monthly drug regimen cost and the treatment duration for 1L, 2L, and 3L therapies, respectively. The products of drug regimen and monthly cost per duration of treatment were summed for all therapy lines.
Evidence
Drug regimens were derived from the clinical studies presented in the efficacy sections of the summary of product characteristics (SmPCs) for the biologic drugs. Study references and their related publications are listed in .
Table 1. Studies referenced in SmPCs for bevacizumab, cetuximab, and panitumumab.
Drug acquisition and administration costs were derived from country-specific sources summarized in . Median PFS values were extracted from the pivotal studies shown in .
Table 2. Drug and administration cost data for Germany.
Table 3. Median PFS (proxy health outcome and treatment duration) from pivotal studies.
Assumptions
All regimens included in the analysis are sourced from the pivotal studies referenced in the respective SmPCs, except for two regimens which needed to be added. Specifically, to enable cross-over chemotherapy from 1L to 2L, the first regimen added was 2L Bev 10 mg + FOLFIRI, for which no efficacy (PFS) data was available in a study and, therefore, was estimated as follows. To avoid biasing the analysis, the assumed drug regimen was duplicated: for the first entry efficacy was assumed equivalent to the ML18147 study (BEV 5 mg + FOLFIRI)Citation19 with Median PFS equal to 5.7 months (assumed to be a minimum estimate which biases costs in favor of BEV and efficacy against BEV), for the second entry efficacy was assumed equivalent to BEV 10 mg + FOLFOXCitation18, with Median PFS equal to 7.4 months (assumed to be a maximum estimate which biases costs against BEV and efficacy in favor of BEV). All results are presented. The second regimen added was 3L BSC, for which the efficacy was based on the CO17 studyCitation11.
Backbone chemotherapies were restricted to FOLFOX, FOLFIRI, or XELOX, based on the assumption that these are the most commonly used backbones. Calculations are based on the average patient weight of 70 kg and height 170 cm (body surface area 1.8 m2). Administration costs are calculated assuming that, if drugs are administered simultaneously (equal or corresponding cycle lengths), a single administration cost is applied per administration.
Median PFS was used as a proxy for treatment duration and health benefit (discussed in detail in the Discussion section). Median PFS outcomes of the ML18147 study were applied to all 2L BEV (5 mg) regimens regardless of backbone chemotherapy. In the absence of an alternate approach, median PFS was summed across 1L, 2L, and 3L regimens as a proxy for total treatment duration for all sequences.
Best supportive care (BSC) was assumed to exclude active chemotherapy and was approximated at a fixed monthly cost of €100 per month, covering palliative care for each month of treatment duration.
Results
First, second, and third line drug regimens (monthly costs)
The calculated total monthly cost for each drug regimen for each therapy line is shown in . In first line, the least costly biological drug regimens are bevazicumab-based followed by cetuximab-based and Panitumumab-based regimens. Similar results are seen for second line, except for high dose (10 mg) BEV-based regimens which are comparatively costly. In third line, the least costly regimens are ones in which biologics are combined with BSC instead of a cytotoxic drug.
Table 4. Calculated monthly drug costs by line of therapy.
Treatment sequences
To combine the drug regimens for each line of therapy into plausible treatment sequences, three potential scenarios were: where an anti-EGFR is used in first, second, or third line treatment. Where an anti-EGFR is used in 1L, the 2L option is generally BEV (10 mg), leaving the remaining 3L option of BSC. Where an anti-EGFR is used in 2L; sequences may begin with BEV (5 mg) 1L regimen followed by 2L anti-EGFR and again leaving the remaining 3L option BSC. Where an anti-EGFR is used in 3L, sequences begin with bevacizumab 1L followed by bevacizumab 2L. A list of sequences used in this analysis along with the respective median PFS is shown in .
Table 5. Potential treatment sequences based on studies referenced in SmPCs.
Comparison of clinical outcomes
The sequences were evaluated to determine the maximum combined PFS benefit for different combinations of 1L, 2L, and 3L regimens. All results are shown in arranged in ascending order of combined PFS.
Table 6. Sequences arranged in ascending order of health outcomes (sum of median PFS).
Under the assumptions of the analysis, the sequence with the minimum expected PFS health outcomes uses an anti-EGFR in 2L (BEV 5 mg + FOLFOX4▸CET 250 mg weekly + IRI▸BSC) with a total combined PFS of 15.2 months. In comparison the sequence with the maximum expected PFS health outcomes uses an anti-EGFR in 3L (BEV 7.5 mg + XELOX▸BEV 5 mg + simplified FOLFIRI▸PAN + BSC) with a maximum benefit of 23.1 months. The large difference in outcomes is driven by the favorable results of the 3L PAN studies compared to the use of BSC alone in 3L. Four out of the top five sequences where health outcome is maximized include sequential bevacizumab-based regimens with an expected combined median PFS of 18.8; 20.5; 23.1; and 23.1 months, respectively. Note that, even for BEV (10 mg) + FOLFIRI (assumed regimens) with maximum estimated PFS 7.4 months (least conservative estimate), the health outcomes are less favorable than regimens where anti-EGFR is used in 3L therapies.
Comparison of cost outcomes
In the results above, the sequences with the longest combined median PFS will appear more costly, simply due to the longer treatment duration. Therefore, to directly compare the cost of sequences, all treatment durations were standardized to 6.1, 4.0, and 2.7 months for 1L, 2L, and 3L, respectively, based on estimates from clinical oncologistsCitation24. Total sequence costs per patient per lifetime were compared and results are shown in .
Table 7. Sequences arranged in ascending order of cost outcomes with standardized treatment duration.
The sequences with the lowest total sequence cost per patient lifetime and average monthly cost are those where an anti-EGFR is used in 2L and BSC is used in 3L, with costs in the range of €55,394–€57,288. The sequences with the highest total sequence cost per patient lifetime and average monthly cost are those where anti-EGFR is used as 1L therapy, BEV (10 mg) is used in 2L therapy and BSC is used in 3L with costs in the range of €67,275–€74,074. Sequences including sequential bevacizumab-based therapy with an anti-EGFR in 3L have a mid-range total sequence cost per patient lifetime in the range of €61,366–€67,070 and mid-range average monthly cost.
Robustness
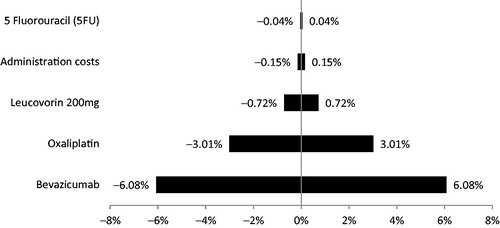
The total sequence cost per patient per lifetime is dependent on the monthly cost of the drug regimen in each line (1L, 2L, 3L) of therapy and the treatment duration. The drug regimen cost is determined by the drug dosage, cycle duration, drug, and administration costs. The drug dosage and cycle duration are not expected to vary, one-way deterministic sensitivity analysis was undertaken at drug regimen level to evaluate the effect of varying the drug acquisition and administration costs by a range of 10%. Using the base case regimen BEV 5 mg + FOLFOX4Citation17 1L, the maximum variation occurred for the drug cost BEV and varied by 6%. Since each drug regimen in each therapy line is calculated using the same methods, these results are replicable across therapy lines. Results are shown in .
Figure 1. One-way deterministic sensitivity analysis for drug regimen BEV 5 mg + FOLFOX4.
Discussion
The sequences were compiled according to the drug regimens included in the studies referenced in the SmPCs as at December 2012, and have been verified by clinical oncologistsCitation24–26. The rationale for this approach is that there is variation in 1L, 2L and 3L drug regimens and dosing schedules across and within countries/treatment centers and using clinical trial protocols seems a reasonable method to compare a range of sequences in an unbiased manner. Evidence suggests that these drugs combined with chemotherapy regimens are representative of clinical practice. A study evaluated the use of therapies in mCRC across four European countriesCitation33. It demonstrated that the proportion of patients receiving 1L BEV and 1L CET (in KRAS WT) is 41.5% and 7.4% in France; 37% and 9.6% in Germany; 44.3% and 7.2% in Italy, and 30.2% and 14.4% in Spain. The majority of patients receive backbone FOLFIRI, FOLFOX, or other oxaliplatin regimens (Italy 78.6%; Germany 78.3%; Spain 66.0%; and France 60%)Citation33. The proportion of patients receiving 2L BEV and 2L CET is 37.8% and 17.3% in France; 36.6% and 20.3% in Germany; 33.3% and 26.2% in Italy; and 29.5% and 29.5% in Spain. The proportion of patients receiving backbone FOLFIRI, FOLFOX, or other oxaliplatin regimens is 51.1% in Italy; 61.7% in Germany; 49.5% in Spain; and 48% in FranceCitation33.
Bevacizumab is indicated irrespective of KRAS status, and the reader should note that PFS results from published studies have been used not specific to KRAS status. In addition to KRAS status, the optimum treatment strategy depends on a number of factors which include the patient’s general condition, performance status, and the availability of drug regimens in the treatment context. The reader should consider that the results presented are dependent on the drug dosing schedules and the assumptions made regarding administration and that the same analysis based on different dosing schedules would likely yield different results in terms of incremental costs.
This analysis uses the median PFS to approximate health outcomes or clinical benefit. Although a novel approach, Saad et al.Citation34 assessed the validity of PFS (defined by Saad et al. as time elapsed between treatment initiation and tumor progression or death from any cause with censoring of patients lost to follow-up) as a surrogate end-point in CRC and found it to be a level-2 validated surrogate end-point for OSCitation34,Citation35. Saad et al.Citation34 concluded that
while it seems clear that extending survival remains the principal treatment goal in advanced cancer, the best way to achieve this goal may be the sequential use of treatments with demonstrated superiority in terms of time to disease progression as the chief indicator of therapeutic efficacy in an era of active subsequent-line therapies (p. 5),
The analysis also uses median PFS as a proxy for treatment duration (a similar approach has been used elsewhere)Citation36,Citation37. Ideally, the average duration of treatment or time to treatment failure could be used, but this is not reported consistently across all clinical trials and this is also difficult to ascertain when stop–go strategies are used by oncologists. The monoclonal antibodies (BEV, CET, PAN) are all licensed to be administered until disease progressionCitation4,Citation23,Citation38. However, in clinical practice, depending on the safety profiles of the drugs, some patients may stop prior to progression, suggesting that the approach used in this analysis over-estimates the duration and, therefore, treatment cost. In this analysis, the median treatment duration is reported for 11 out of the 19 regimens used, and is, on average, 68% of the median PFS, suggesting that the true cost is probably 30% less than shown in the analysis and is assumed to apply to all sequences in equal measure.
Furthermore, the analysis sums median PFS values across 1L, 2L, and 3L regimens, which are then used as a proxy of total treatment duration for sequences. Although this approach has limitations, in the absence of clinical studies it is necessary to assume that it serves as an adequate proxy. A similar approach has been used for sequences in renal cell carcinomaCitation37. The reader should consider that, ideally, when modeling sequential treatments (and summing PFS), the eligibility criteria of patients from one therapy line to another will be consistent. This consistency in evidence is not available from clinical trials and, therefore, not possible in the current analysis, which introduces uncertainty around the summed PFS estimates as a result of the different patient characteristics (eligibility criteria) for each of the different lines of therapy.
In the analysis presented, using sequential BEV 1L and 2L results in the option of patients being eligible for 3L anti-EGFR. Using the approach of summing PFS, these sequences have the highest PFS outcomes which equate to the longest treatment durations. This appears to disadvantage them from a payer perspective; however, it is important to keep in mind that this incremental cost is due to prolongation of survival outcomes (improved efficacy). In comparison, in sequences where anti-EGFRs are used as 1L or 2L, the only available 3L options are BSC and CET. These sequences have the lowest summed PFS values approximated with the shortest treatment durations (). This may make them appear economically favorable; however, it is important to note that this apparent economic advantage is a result of reduction in survival outcomes. Therefore, it is useful to compare costs when standardizing for treatment duration, as shown in .
The analysis presented uses an estimated average monthly cost for best supportive care, but BSC is generally difficult to define and therefore cost. Best supportive care is inconsistently defined in the literature and often not defined at all in clinical trialsCitation39. There appear to be no published studies evaluating the cost of BSC, probably due to this lack of consistency. The only clear distinction is between active supportive care and best supportive care, with the latter excluding chemotherapyCitation40. The assumption in the analysis is that BSC incurs a monthly treatment cost of a maximum €100 per month, which is considered to be a conservative estimate so as not to bias results against sequences including BSC. A cost-effectiveness analysis comparing BSC to active treatment in CRC suggests that the monthly cost of BSC is far greater than €100 per monthCitation40. The reader should consider that all sequences evaluated in this analysis include 3L BSC (with the exception of Cet + Iri); therefore, any change in cost estimate will influence all sequences equally ().
Adverse event costs have not been included in the analysis because of discrepancies in the availability of adverse event data, that is: the frequency of adverse events is not available for all drugs across the spectrum of all potential adverse events, biasing the analysis in favor of drugs with incomplete data sets. When complete and compatible data sets are available on the frequencies of adverse events this can potentially be included in future analysis.
The current analysis does not include sequences for aflibercept because this analysis was completed prior to the licensing of aflibercept for the treatment of mCRC in the European Union. In addition, the licensing status of panitumumab was updated in August 2013, and regorafenib is now a licensed treatment option. An update of this analysis to include these changes is an area of ongoing research.
Conclusion
Sequential treatment in metastatic colorectal cancer using the full armamentarium of biological and chemotherapeutic agents represents today’s gold standard in prolonging the lives of patients. Clinical sequences consisting of 1L and 2L line bevacizumab followed by 3L anti-EGFR potentially yield the greatest health outcomes associated with a reasonable trade-off in additional cost when replacing 1L anti-EGFRs and are potentially cost-saving if replacing 2L anti-EGFRs, per patient per lifetime. To maximize health outcomes, optimal sequences include anti-EGFRs as a 3L regimen, with an approximately equivalent trade-off in costs between the most costly (anti-EGFR 2L) and least costly (anti-EGFR 1L) sequences.
Transparency
Declaration of funding
The analysis was funded by F Hoffmann-La Roche with the agreement that the contract research organization could publish the results unaltered.
Declaration of financial/other relationships
TR has acted as a consultant for F. Hoffmann-La Roche. DA, JB, SK, and SW have acted as consultants/advisors and received speaker’s bureau from F. Hoffmann-La Roche. SW is a former employee of F. Hoffmann-La Roche (>12 months) and currently holds stocks in the company. CN is a current employee of F. Hoffmann-La Roche. US has no conflicts of interest to declare relating to colorectal cancer.
This analysis has not been previously published. The Treatment Sequencing Costing (TSC) model has been used for alternate analysis, the results of which have been presented as posters at the Annual Meeting of the German, Austrian and Swiss Societies for Hematology and Oncology, 19–23 October 2012, Stuttgart, Germany and the 4th Latin American Conference, International Society for Pharmacoeconomic Outcomes Research, 12–14 September 2013, Buenos Aires, Argentina.
Acknowledgments
No medical writing services have been used in the production of this manuscript. Thank you to Mrs Schalk and Dr Scherer (both F. Hoffmann-La Roche AG, Germany) for providing German drug and administration costs.
References
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893-917
- Segal NH, Saltz LB. Evolving treatment of advanced colon cancer. Annu Rev Med 2009;60:207-19
- Van Cutsem E, Nordlinger B, Cervantes A. Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment. Ann Oncol 2010;21:v93-7
- Erbitux: EPAR - Product information - Summary of product characteristics (SmPC). European Medicines Agency (EMA), 2012. http://www.emea.europa.eu/ema/index.jsp?curl=pages/includes/document/document_detail.jsp?webContentId=WC500029119&mid=WC0b01ac058009a3dc. Accessed December 2012
- Van Cutsem E, Kohne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med 2009;360:1408-17
- Maughan TS, Adams RA, Smith CG, et al. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet 2011;377:2103-14
- Bokemeyer C, Bondarenko I, Hartmann JT, et al. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: the OPUS study. Ann Oncol 2011;22:1535-46
- Tveit KM, Guren T, Glimelius B, et al. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: the NORDIC-VII study. J Clin Oncol 2012;30:1755-62
- Sobrero AF, Maurel J, Fehrenbacher L, et al. EPIC: phase III trial of cetuximab plus irinotecan after fluoropyrimidine and oxaliplatin failure in patients with metastatic colorectal cancer. J Clin Oncol 2008;26:2311-19
- Jonker DJ, O'Callaghan CJ, Karapetis CS, et al. Cetuximab for the treatment of colorectal cancer. N Engl J Med 2007;357:2040-8
- Karapetis CS, Khambata-Ford S, Jonker DJ, et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N Engl J Med 2008;359:1757-65
- Vectibix: EPAR - Product information - Summary of product characteristics (SmPC). European Medicines Agency (EMA), 2012. http://www.emea.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000741/human_med_001128.jsp&mid=WC0b01ac058001d124. Accessed December 2012
- Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28:4697-705
- Peeters M, Price TJ, Cervantes A, et al. Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J Clin Oncol 2010;28:4706-13
- Van Cutsem E, Peeters M, Siena S, et al. Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol 2007;25:1658-64
- Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335-42
- Saltz LB, Clarke S, Diaz-Rubio E, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol 2008;26:2013-19
- Giantonio BJ, Catalano PJ, Meropol NJ, et al. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. J Clin Oncol 2007;25:1539-44
- Arnold D, Andre T, Bennouna J, et al. Bevacizumab (BEV) plus chemotherapy (CT) continued beyond first progression in patients with metastatic colorectal cancer (mCRC) previously treated with BEV plus CT: results of a randomized phase III intergroup study (TML study). 48th Annual ASCO Meeting 2012. Journal of Clinical Oncology 2012;30:suppl:abstr CRA3503). http://www.asco.org. Accessed June 1, 2012
- Zaltrap (aflibercept) - Summary of opinion (initial authorisation). European Medicines Agency (EMA), 2012. http://www.emea.europa.eu/docs/en_GB/document_library/Summary_of_opinion_-_Initial_authorisation/human/002532/WC500134834.pdf. Accessed February 18, 2013
- Zaltrap - Highlights of prescribing information. U S Food and Drug Administration (FDA), 2012. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/125418s000lbl.pdf. Accessed February 8, 2013
- Van CE, Kohne CH, Lang I, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol 2011;29:2011-19
- Avastin: EPAR - Product information - Summary of product charcteristics (SmPC). European Medicines Agency (EMA), 2012. http://www.emea.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000582/WC500029271.pdf. Accessed December 2012
- Arnold D. Electronic and teleconference communication. Freiburg, Germany: Clinic for Medical Oncology, Tumor Biology Center, 2012
- Bennouna J. Electronic and teleconference communication. Nantes, France: Institut de Cancérologie de l'Ouest, 2012
- Kubicka S. Electronic and teleconference communication. Reutlingen, Germany: German Cancer Center, 2012
- Cassidy J, Clarke S, Diaz-Rubio E, et al. Randomized phase III study of capecitabine plus oxaliplatin compared with fluorouracil/folinic acid plus oxaliplatin as first-line therapy for metastatic colorectal cancer. J Clin Oncol 2008;26:2006-12
- de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol 2000;18:2938-47
- Giantonio BJ, Catalano PJ, O'Dwyer PJ, et al. Impact of bevacizumab dose reduction on clinical outcomes for patients treated on the Eastern Cooperative Oncology Group's Study E3200. J Clin Oncol 2006;ASCO Annual Meeting Proceedings Part I 2006;24:3538
- Pfeiffer P, Nielsen D, Yilmaz M, et al. Cetuximab and irinotecan as third line therapy in patients with advanced colorectal cancer after failure of irinotecan, oxaliplatin and 5-fluorouracil. Acta Oncol 2007;46:697-701
- Pfeiffer P, Nielsen D, Bjerregaard J, et al. Biweekly cetuximab and irinotecan as third-line therapy in patients with advanced colorectal cancer after failure to irinotecan, oxaliplatin and 5-fluorouracil. Ann Oncol 2008;19:1141-5
- Siena S, Cassidy J, Tabernero J, et al. Randomized phase 3 study of Panitumumab with FOLFOX4 compared with FOLFOX4 alone as fist-line treatment in patients with metastatic colorectal cancer: the PRIME Trial. ASCO Annual Meeting 2010.
- Zhao Z, Pelletier E, Barber B, et al. Patterns of treatment with chemotherapy and monoclonal antibodies for metastatic colorectal cancer in Western Europe. Curr Med Res Opin 2012;28:221-9
- Saad ED, Katz A, Hoff PM, et al. Progression-free survival as surrogate and as true end point: insights from the breast and colorectal cancer literature. Ann Oncol 2010;21:7-12
- Fleming TR. Surrogate endpoints and FDA's accelerated approval process. Health Aff (Millwood) 2005;24:67-78
- Schwander B, Ravera S, Giuliani G, et al. Cost comparison of second-line treatment options for late stage non-small-cell lung cancer: cost analysis for Italy. Clinicoecon Outcomes Res 2012;4:237-43
- Escudier B, Goupil MG, Massard C, et al. Sequential therapy in renal cell carcinoma. Cancer 2009;115:2321-6
- Giusti RM, Shastri K, Pilaro AM, et al. U.S. Food and Drug Administration approval: panitumumab for epidermal growth factor receptor-expressing metastatic colorectal carcinoma with progression following fluoropyrimidine-, oxaliplatin-, and irinotecan-containing chemotherapy regimens. Clin Cancer Res 2008;14:1296-302
- Zafar SY, Currow D, Abernethy AP. Defining best supportive care. J Clin Oncol 2008;26:5139-40
- Starling N, Tilden D, White J, et al. Cost-effectiveness analysis of cetuximab/irinotecan vs active/best supportive care for the treatment of metastatic colorectal cancer patients who have failed previous chemotherapy treatment. Br J Cancer 2007;96:206-12