Abstract
Chronobiological disorders and syndromes include seasonal affective disorder (SAD), total blindness, advanced and delayed sleep phase syndrome, jet lag, and shift work maladaptation. These disorders are treated by adjusting circadian phase, using appropriately timed bright light exposure and melatonin administration (at doses of 0.5 mg or less). In some cases, it may be necessary to measure internal circadían phase, using the time when endogenous melatonin levels rise.
Los síndromes y trastornos cronobiológicos incluyen el trastorno afectivo estacional (TAE), la ceguera total, los síndromes de avance y retraso de fases del sueño, el jet lag y la mala adaptación a los turnos laborales. Estos trastornos se tratan ajustando las fases circadianas, mediante la utilización de un tiempo apropiado de exposición a la luz brillante y la administración de melatonina (en dosis de 0,5 mg o menos). En algunos casos puede ser necesario medir las fases circadianas internas utilizando el período en que se elevan los niveles de melatonina endógena.
Les syndromes et troubles chronobiologiques regroupent le trouble affectif saisonnier (TAS), les desordres entraînés par la cécité totale, les syndromes type retard ou avance de phase, les symptômes liés aux changements de fuseaux horaires (jet lag), et les perturbations dues au travail posté. Ces troubles sont traités en réajustant le rythme circadien, grâce à l'utilisation judicieuse et minutée de l'exposition à la lumière brillante et à l'administration de mélatonine (0,5 mg ou moins). Parfois, il semble nécessaire de mesurer le rythme circadien interne, au moment de l'élévation des concentrations de mélatonine endogène.
Melatonin appears to be useful in two ways to the field of human chronobiology. One role is as a marker for biological rhythms. The other role is as a circadian phaseshifting agent. Both roles appear to be important.
In virtually all organisms, melatonin is produced mainly during nighttime darkness.Citation1,Citation2 In most vertebrates, circulating melatonin levels are derived exclusively from the pineal gland.Citation3,Citation4 In most mammals, the changing duration of melatonin production throughout the year is the cue for seasonal rhythms.Citation5 In some mammals, such as humans, a feedback loop exists between melatonin and the endogenous circadian pacemaker.Citation6-Citation13
An approximately 24-h (hence, circadian) rhythm in melatonin is generated by 12 h of (usually daytime) inhibition of an otherwise constantly “on” signal from the paraventricular nucleus of the hypothalamus.Citation14 This inhibition comes from the endogenous circadian pacemaker, located in the suprachiasmatic nucleus (SCN).Citation15-Citation17 The pineal gland is then stimulated to produce melatonin for about 12 h via a neural pathway that traverses through the intermedullary column and thoracic sympathetic outflow ().Citation18 Preganglionic neurons synapse in the superior cervical ganglion with postganglionic neurons that enter the cranium and innervate pincalocytes.Citation19 The latter release the sympathetic neurotransmitter, norepinephrine, which stimulates β1-adrenergic receptors and results in the synthesis and secretion of melatonin, which is then released into blood and cerebrospinal fluid (CSF).Citation20 Receptors for melatonin have been identified in a number of sites, including the SCN.Citation21,Citation22
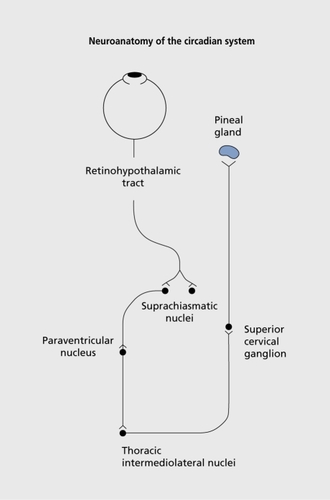
The approximately 24-h rhythm generated by the SCN becomes precisely 24 h via photic input from ganglion cells in the retina.Citation23,Citation24 At least one novel photoreceptor has been identified that mediates circadian en train ment.Citation25 The pathway from the retina, to the hypothalamus, the retinohypothalamic tract, is different from that which mediates vision.Citation26
The light/dark cycle synchronizes the SCN, and therefore its many driven circadian rhythms, to the 24-h day.Citation27,Citation28 Unique to melatonin, light acutely suppresses its production.Citation29 Thus, if the SCN has not turned off melatonin production in the morning, exposure to light will. Also, light exposure at the end of the day will suppress the evening rise in melatonin production.Citation30
These effects of light shape the melatonin profile. As mentioned above, annual rhythms common to many mammals receive their seasonal time cue from the changing duration of melatonin production, thought to define the “biological night.” Whether or not humans have important seasonal rhythms is a matter of some controversy.Citation31,Citation32 If humans have important seasonal rhythms, it is thought that the duration of melatonin production would regulate them. Not controversial is the fact that similar to other animals, humans have circadian rhythms that are primarily regulated by the light/dark cycle.Citation30,Citation33-Citation38
The endogenous melatonin profile as a marker for circadian phase position
In humans, the melatonin profile is the most reliable marker for circadian phase ().Citation39-Citation41 The time that melatonin levels rise appears to be a useful phase maker. The melatonin onset (MO) is a clearly demarcated event. It can be operationally defined in a number of ways, some of which use a threshold (2 pg/mL, 10 pg/mL, etc), which appears as a subscript in the acronym.Citation42 In order to minimize the acute suppressant effect of light, plasma samples are collected under dim light (optimally, less than 30 lux). Therefore, in sighted people this marker is called the dim light melatonin onset (DLMO).Citation43 The plasma DLMO10 occurs on average about 14 h after waketime in entrained, sighted people, and the DLMO2 occurs about 1 h earlier.Citation13,Citation44,Citation45
The light zeitgeber (German for time-giver, or time cue) first occurs each day at waketime.Citation46 In the circadian literature, this is called zeitgeber time 0 (ZT 0). (Sometimes the term circadian time [CT] is used under certain circumstances; although they are technically different, ZT and CT will be used interchangeably in this monograph, in order to minimize confusion on the part of readers who are not experts in chronobiology.) As mentioned above, the average CT or ZT of the plasma DLMO10 is 14 h in entrained, sighted people. The DLMO ZT also describes the relationship between the circadian rhythms that are tightly coupled to the SCN (such as melatonin) and those that are more loosely coupled (such as the sleep/wake cycle, for example, waketime). Therefore, any mismatch in circadian rhythms will be reflected in a ZT that differs from the 14-h standard.
The light PRC
Light's phase-shifting effects on circadian rhythms can be explained by a phase response curve (PRC). Its essential features are that light exposure in the morning causes a phase advance (shift to an earlier time) and that light exposure in the evening causes a phase delay (shift to a later time).Citation33,Citation36,Citation47 In addition, maximal phase shifts occur in the middle of the night, and minimal phase shifts occur during the middle of the day.Citation48-Citation51 PRCs are usually plotted according to CT. The break points that separate advance and delay responses for the light. PRC are 12 h apart: they occur at CT 6 and CT 18. Converting to clock time for an individual who habitually awakens at 7.00 am, these are 1.00 pm and 1.00 am, respectively. With regard to the light. PRC, there are several investigators who think that these break points occur a few hours later.Citation52 The jury is out on this question.
As mentioned above, light is the most potent circadian zeitgeber in virtually all organisms. However, this was not fully appreciated in humans until it was shown that humans require brighter light for this effect than other animals, which was dramatically demonstrated with respect to acute suppression of melatonin production.Citation53 The phase-shifting and suppressant effects of light are thought to be closely associated. Since sunlight (10 000-100 000 lux) is usually brighter than indoor light humans might be responding to the natural light/dark cycle, relatively unaffected by ordinary-intensity indoor light (200-500 lux). A second implication is that bright artificial light could be substituted for sunlight, in order to experimentally (and perhaps therapeutically) manipulate biological rhythms in humans.
Winter depression (SAD)
One of the first therapeutic uses of bright light was to treat winter depression, or seasonal affective disorder (SAD).Citation54,Citation55 Bright light has also been used to treat nonseasonal depression,Citation56 which is reviewed elsewhere (see Parry's and Wirz-Justice 's contributions to this volumeCitation57,Citation58), as well as many of the hypotheses for SAD (see Parry's, Wirz -Justice's and Praschak-Rieder's contributions to this volumeCitation57,Citation59) and so these will not be covered here. This monograph will concentrate on diagnosing circadian phase disorders using the endogenous melatonin profile and on the basic principles for treating them.
The leading hypothesis for SAD is the phase shift hypothesis (PSH).Citation33 According to the PSH, the typical SAD patient becomes depressed in the winter, at least in part because of a phase delay of circadian rhythms (marked by the DLMO) with respect to sleep,Citation33,Citation60,Citation61 having a mismatch in circadian rhythms (similar to jet lag), which persists for several months. Therefore, bright light exposure should be most antidepressant when it is scheduled in the morning, when it would be expected to cause a corrective phase advance. Bright light exposure in the morning should certainly be more antidepressant than evening bright light, which would be expected to cause a phase delay.
The first major test of the PSH was a crossover study of eight patients and seven control subjects.Citation36 There was a small, but statistically significant, delay of the DLMO in patients compared to controls at prebaseline and at the end of the initial week of baseline conditions (sleep permitted only between 10.00 pm and 6.00 am). Two hours of morning bright light (2500 lux) caused advances in the DLMO; evening bright light caused delays. The combination of morning plus evening light (which was the last treatment week) moved the DLMO towards its baseline time. Morning light produced a significant antidepressant effect compared with baseline and with evening light. The combination was again intermediate between that of morning light alone and evening light alone. This study was by and large replicated a few years later.Citation62,Citation63 Since then, not much has changed in the recommended light treatment regimen, except that light intensity can be as great as 10 000 lux,Citation64 and perhaps 1 h per day is sufficient, as long as it is scheduled immediately upon awakening. Once treatment is satisfactory, the duration of light exposure can almost always be reduced.Citation65
Several other studies have supported these findings, but some have notCitation66,Citation67: these studies were usually parallel-designed, so that patients themselves did not have the opportunity to compare light exposure at different times (which would have minimized the placebo component). In 1998, three independent research groups published large-N studies in which morning light was shown to be more antidepressant than evening light thereby moving the field towards consensus about the superiority of morning light.Citation45,Citation68,Citation69 However, superior efficacy of morning light does not necessarily prove the PSH, because it could be more antidepressant at this time for some reason other than causing a phase advance. However, it has been shown that the antidepressant response to morning light does, in some circumstances, correlate with the amount of phase advance in the DLMO. This was first reported with respect to treatment group means,Citation61 followed by an analysisCitation70 of individual DLMOs and depression scores collected independently.Citation36,Citation63 More recently, this latter finding was essentially replicated using another data set.Citation71 Further support of the PSH along these lines will be discussed below. It should also be noted that a very small subgroup of SAD patients appear to be cueing to dusk and should be treated with evening bright light; clinically, these patients can be identified by a history of early morning awakening year round, going to bed much earlier in the winter.Citation65
In any event, the earliest and most common use of the DLMO has been to assess the phase-shifting effects of light. Bright light has also been used to treat a number of other circadian phase disorders, such as advanced sleep phase syndrome (ASPS), delayed sleep phase syndrome (DSPS), jet lag, and shift work maladaptation (see below).
The melatonin PRC
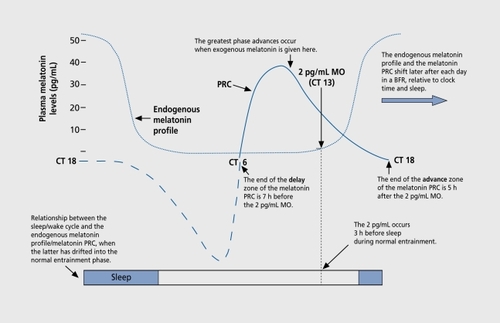
The phase-shifting effects of melatonin are also described by a PRC. The melatonin PRC is about 12 h out of phase with the light. PRC.Citation13,Citation44 Both PRCs are phase-locked to each other, as well as to the melatonin profile (Figure 2). As mentioned above, waketime is usually designated ZT 0. Sleep time is therefore usually ZT 16. In the melatonin PRC studies of sighted people, the baseline plasma DLMO10 was designated CT 14. It is also designated CT 14 in free-running blind people. We call this phase marker the MO in blind people. Saliva can also be used (at this time of the night, salivary melatonin levels are about one -third those of plasma).Citation72 Measuring the MO in blind people provides a reference point to determine the phase of the endogenous circadian pacemaker and the melatonin PRC. Unless stated otherwise, in the following the MO refers to the plasma 10 pg/mL threshold or its salivary equivalent (3 pg/mL).The melatonin PRC was first described using four daily doses of 0.5 mg melatonin in sighted people. It has been by and large replicated by two other research groups.Citation73,Citation74
In sighted people who habitually awaken at 7.00 am, the break points that divide the two intervals of the melatonin PRC occur at 1.00 pm (CT 6) and 1.00 am (CT 18), just as with the light PRC. The phase-advance zone is between 1.00 am and 1.00 pm; the phase-delay zone is between 1.00 am and 1.00 pm. Once again, the phaseadvance zone of the melatonin PRC extends from CT 6 to CT 18, and the phase-delay zone extends from CT 18 to CT 6. Therefore, once the time of the MO is known, the advance zone extends from 8 h before the MO until 4 h after the MO. The delay zone extends from 4 h after the MO until 8 h before the MO.
Treating SAD patients with melatonin: the importance of creating “owerfap”
Creating “overlap” may be an important principle in optimizing melatonin's phase-shifting effects. 'Phis was demonstrated in a pilot study treating SAD patients with melatonin.Citation75 In order to avoid the soporific side effect of sleepiness that occurs in some people, the dose of melatonin is kept to a minimum, so as to reduce the initial spike in melatonin levels following an oral, immediaterelease formulation. However, according to the melatonin PRC, the earlier melatonin is given in the afternoon (at least for the second half of the advance zone), the greater the magnitude of the phase-advance shift. If a low dose is given too early, however, there will be a melatonin-frec interval between the end of the exogenous pulse and the beginning of the endogenous melatonin profile that occurs about 14 h after waketime in entrained, sighted people. Therefore, a second (or even a third or possibly fourth) small dose of melatonin is given to create overlap between elevated melatonin levels arising from exogenous and endogenous sources, so that the SCN is exposed to one continuous melatonin signal.
Recently, a more definitive test of the PSH for SAD was completed, using three to four small doses of melatonin (0.075-0.1 mg) given every 2 h in the morning or in the afternoon/evening. One hundred patients were studied over four winters. One-third of them did not receive melatonin in any capsule, although all subjects took the same number of capsules per day. Subjects were held to consistent bedtimes and waketimes of their choosing.
The results supported the PSH. In the most phase-delayed group of patients (those with a DLMO ZT >14.6), there was a significant correlation between the amount of phase delay at baseline and the severity of depression ratings. After 3 weeks of treatment, this correlation remained significant, but only if depression severity was analyzed with regard to the absolute difference from the hypothesized “normal.” ZT of 14. Change scores analyzed in this way were also statistically significant: as DLMO ZT normalized, depression ratings improved. This may be one of the first examples of a physiological marker that correlates with psychopathology at baseline and posttreatment.
These data are consistent with the clinical observation that too much of a phase advance can result in a return of symptoms. In any event, morning light appears to be more antidepressant than evening light in typical SAD patients, because, at least in part, it is correcting a phase delay that occurs in SAD patients when they become depressed in the winter. Using SAD as a model chronobiological psychiatric (affective) disorder, it would now seem timely to investigate other disorders, in order to assess the contribution of a mismatch between circadian rhythms to the pathology.
Treating free-running totally blind people with melatonin: the importance of avoiding “spillover”
About 15% of blind people completely lack light perception. Most, if not all of them, have abnormal circadian rhythms, and many of them “free-run,” whereby their MOs drift a little later each day. When they are out of phase, they find it difficult to sleep at night and are tired during the day - a burden described by some as second only to lack of vision. A daily drift in sleep times is not usually observed. However, assessment of physiological rhythms clearly indicates this daily drift in the phase of the endogenous circadian pacemaker. Any of several circadian rhythms can be measured, including Cortisol and temperature.Citation76-Citation79 However, these are masked by changes in activity.Citation80 Melatonin production is masked only by light,Citation53 which is not an issue in blind people.
A number of studies now document circadian abnormalities in the totally blind population.Citation81-Citation83 The MO has proved to be a useful phase marker in blind people, whether it is extracted from 1-h samples over 24 h or from sampling every 30 to 60 min within a narrower window when it is expected to occur. However, as will be explained below, assessing MOs is not absolutely necessary in diagnosing and treating most cases.
Following the discovery that light can suppress melatonin production in humans,Citation53 the obvious next step was to assess the melatonin profiles of blind people. One-day assessments indicated that melatonin levels were continuously elevated for about 12 h out of every 24 h, similar to sighted people.Citation84 However, it was not always confined to night. Two bilaterally enucleated people were studied longitudinallyCitation85: one of them appeared to be stably entrained, but 180° out of phase (that is, melatonin levels peaked in the middle of the day, week after week); the other was freerunning with an intrinsic circadian period (tau, or τ) of 24.7 h (that is, the endogenous melatonin profile shifted later at a rate of about 0.7 h per day or about 5 h per week). Several studies have since confirmed that the circadian rhythms of blind people are of three types: normally entrained, abnormally entrained, and free-running.Citation85 When out of phase, these individuals have difficulty sleeping at night and take more naps during the day. The melatonin rhythm reflects the phase of all other endogenous circadian rhythms, including those of Cortisol, temperature, and sleep propensity (see above).
As mentioned earlier, another use of melatonin is to give it exogenously in order to cause phase shifts.Citation13 Inspired by animal studies,Citation86 these effects were most conclusively demonstrated by entraining free-running blind people (blind free-runners [BFRs]) with a daily dose of melatonin.Citation87 Although an early subject showed apparent entrainment to a dose of about 7 mg,Citation88-Citation90 entrainment of BFRs was conclusively demonstrated using a dose of 10 mg.Citation87,Citation91 Only one of seven BFRs failed to entrain to the 1.0-mg dose; this BFR had the longest tau (24.9 h).
Although the melatonin PRC was experimentally determined in sighted people, it appears to apply to blind people as well. Currently, more is known about the phaseadvance zone of the melatonin PRC: for at least the second half of the advance zone, the earlier melatonin is given, the greater the magnitude of the phase-advance shift. When melatonin is given daily to a free-running blind person, the melatonin PRC will continue to drift later and later until exogenous melatonin is hitting the point on the melatonin PRC that will produce a phase advance equal to the daily drift (this is called the entrainment point on the melatonin PRC and will vary between individuals, depending in part on the intrinsic tau). Then, the endogenous pacemaker will lock on to the daily melatonin dose. For example, if a BFR's intrinsic circadian period, or tau, is 24.4 h, the melatonin dose will stop the pacemaker from drifting later when it is stimulating that part of the melatonin PRC when it produces a phase advance of 0.4 h. Thus, entrainment occurs and the pacemaker now functionally has a tau of 24.0 h.
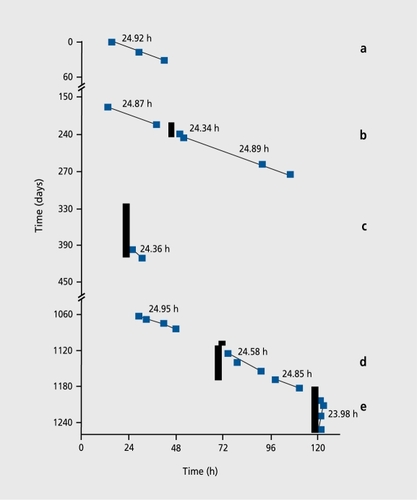
The finding that low doses of melatonin may be more effective than high doses, leading to the idea of avoiding spillover, is illustrated in the treatment of the one BFR who failed to entrain to the 10-mg dose (recall that he had the longest tau, 24.9 h, in that study). Despite repeat treatment with 9 to 10 mg melatonin for 83 days and 20 mg melatonin for 60 days (),Citation92 he failed to entrain, although his tau did shorten to 24.36 and 24.58 h, respectively He was finally entrained with 0.5 mg melatonin.Citation92
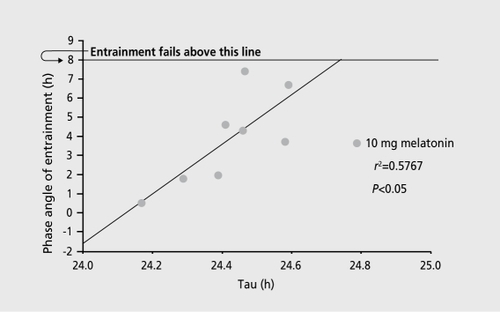
The melatonin PRC might explain why a lower dose of melatonin is more effective than higher doses (). While administering melatonin earlier in the advance zone causes a greater phase advance and while higher melatonin levels probably cause more of a phase advance (perhaps by stimulating more of the phase-advance zone), it appears that if the dose is too high, it will stimulate more of the delay zone and therefore reduce the magnitude of the phase advance. In other words, a lower dose will have less “spillover” and might thus be more effective than a higher dose.
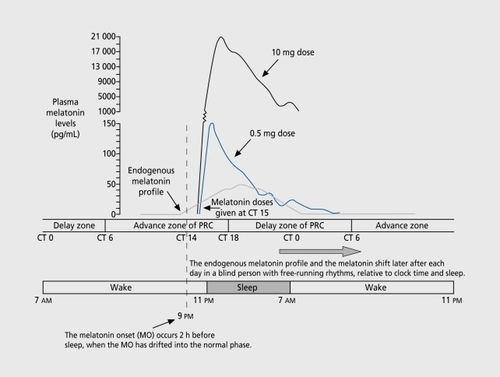
The efficacy of low doses means that melatonin can be administered well before sleep without causing daytime or evening sleepiness. This is important because the treatment goal is not only entrainment, but also entrainment at the optimal phase. Indeed, in the original study of 10 mg,Citation87 successfully entrained BFRs had MOs occurring after sleep onset, often much later ().Citation93 In other words, the MO occurred at the same time each night, but later than normal. As in animal studies, the greater the pretreatment free-running tau, the later entrainment occurs relative to the time of the entraining stimulus. In our entrained BFRs, their sleep disorders had improved with treatment, but our subjects still had trouble falling asleep and getting up in the morning. About 30% of people become sleepy on melatonin, and this side effect appears to be dose-related and is troublesome at doses greater than 1 mg, certainly at 10 mg. Now that 0.5 mg has been shown to be an effective dose with minimal soporific side effects, it can be administered earlier than bedtime (which is when the 10 mg was originally given, in order to make use of this side effect). Melatonin can be given earlier in the evening, so that the MO occurs 2 h before desired sleep time, thus resulting in optimal sleep quality.
When shifting the clock time of exogenous melatonin administration, the endogenous MO can be reset to any time. Shifting the clock time of administration earlier should be done gradually, so as not to cross over the break point on the melatonin PRC. The clock time of administration can also be shifted later, which can be done in 1 day without loss of entrainment. In either case, the pacemaker will shift with the time of the melatonin dose. In blind people who appear to be entrained (or at least have a tau virtually indistinguishable from 24.0 h) to a behaviorally related zeitgeber or to ambient light (perhaps in some blind people who are not bilaterally enucleated), MOs can be reset earlier or later with a daily dose of melatonin, so that the MO occurs 14 h after waketime.
Several years ago, we also proposed that the abscissa and ordinate of Figure 5 could be reversed.Citation94 Accordingly, the phase angle of entrainment could be used to predict tau. While the taus of BFRs are probably the most accurate estimate of the genetically programmed intrinsic tau (which might be of use in studying clock genes in humansCitation95-Citation97), we also suggested that the DLMO ZT in sighted people might be a useful way to estimate at least the functional tau in people entrained to the light/dark cycle.
Melatonin treatment can be initiated at any time in BFRs
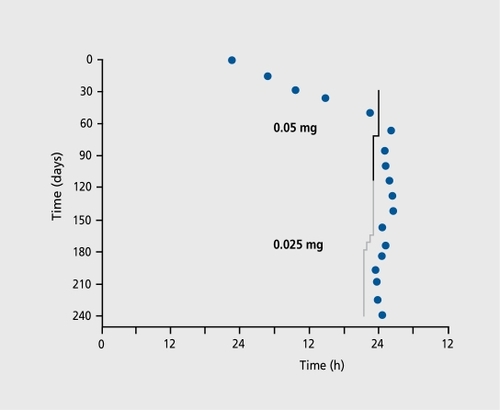
What would have happened if melatonin treatment were initiated in BFRs on the “wrong” zone of the melatonin PRC? In animal studies, it does not matter when the entraining stimulus is given: eventually, the pacemaker is stably entrained at a steady-state phase position, once the entraining stimulus comes into contact with the entrainment point of the PRC.Citation98 However, in a study published a few years ago, the University of Surrey research group found that they were able to entrain only about half of their group of seven BRFs to a 5-mg dose of melatonin.Citation99 They noted that entrainment was successful only when melatonin treatment was started on the advance zone of the PRC, but not when treatment was started on the delay zone, even if daily melatonin doses were continued through a complete circadian beat cycle, so that eventually melatonin stimulated all of the advance zone. They further noted that this finding contradicted those of animal studies, in which starting a zeitgeber on the delay zone did not affect its capability to eventually cause entrainment (it just took longer before the entrainment point was reached as the pacemaker, and the PRC, drifted into phase). If the Surrey group is correct, this would mean that all BFRs should have frequent. MO assessments to determine on what day melatonin treatment should be initiated. Fortunately, this docs not appear to be true. We found in seven out of seven BFRs that when low-dose melatonin is initiated on the delay zone, entrainment eventually occurs when melatonin is given at the entrainment point in the advance zone.Citation100 The following case () using 0.05 mg is an example; in the other cases, a dose of 0.5 mg was used. Recently, the Surrey group found that some BFRs entrained when 0.5 mg was initiated on the delay zone; however, they continue to recommend initiating melatonin treatment on the advance zone.
Very low doses of melatonin are effective in entraining BFRs
In this case (Figure 6), a very low dose (0.05 mg) of melatonin was initiated in a BFR with a tau of 24.35 h on the delay zone (CT 4.95). Initially, a clear increase in tau occurred, consistent with a greater daily phase delay. Within a few days, melatonin was stimulating the advance zone and once the entrainment point was reached, the pacemaker locked on. As mentioned above, low doses of melatonin can usually entrain BFRs, no matter when treatment is initiated. Therefore, at least for most blind people, one does not need to start melatonin treatment on the advance zone, although it may take longer to reach the entrainment point when treatment begins on the delay zone. The clinical implications of this finding are very important: clinically, most blind people can be treated without having to measure their endogenous circadian phase. Work is on-going to entrain BFRs to doses of melatonin even lower than 0.05 mg. These doses produce peak melatonin levels that are less than what is maximally produced endogenously. Melatonin can also reset the phase of abnormally entrained blind people, even under circumstances when they may be entraining to a poorly perceived ambient light/dark cycle.Citation101
Guidelines for treating CSDs in blind people
The above database provides a preliminary set of treatment guidelines that should be effective in most blind people with circadian sleep disorders (CSDs). However, more studies need to be done, and there will clearly be some blind people who will have to be assessed using the MO for optimal treatment.
Not every blind person has a CSD. Most, if not all, blind people completely lacking in light perception have CSDs, or at least merit treatment to prevent an eventual occurrence; however, the more light perception, the more likely stable entrainment at a normal phase will be the case. In any event, the first step is to take a sleep history to determine whether the patient has DSPS or ASPS, or sometimes has both that regularly recur, which would suggest free-running circadian rhythms. If possible, keeping a sleep diary - noting daily sleep times, naps, nighttime sleep quality, and daytime alertness - is advised; depressive symptoms may also occur when there is a mismatch between circadian rhythms and the sleep/wake cycle.
Melatonin treatment should then be started. A dose of 0.5 mg at about 8.00 pm should result in entrainment of BFRs and to optimal phase resetting in most blind people. Stable steady-state entrainment at the normal phase will take shorter or longer, depending on the tau and on what day treatment was initiated. Although repeated assessments of MOs can determine these parameters with precision, they should not be necessary in most people: eventually this treatment should be successful. If 3 months have passed without marked improvement, referral to sleep a disorder center or some other facility in which MOs can be assessed is advised.
In a few individuals, the 0.5 mg dose may cause some acute sleepiness. If unpleasant, the dose can be gradually tapered every 2 weeks in increments of 0.1 mg to as low as 0.1 mg, and then in increments of 0.025 mg to 0.05 mg, if desired. However, for individuals who have longer taus, the dose should not be reduced below 0.3 mg. Individuals who report bouts of symptoms as often as every 4 to 6 weeks are likely to have longer taus (>24.6 h).
After finding a suitable maintenance dose, the clock time of administration can then be adjusted if the patient still complains of symptoms of ASPS or DSPS. When shifting the administration time earlier, advancing it no more than 30 min every 2 weeks should be sufficiently conservative, so that the entrainment point will not be crossed. Delaying a person with symptoms of ASPS need not be done incrementally. However, in either case shifting the clock time should be stopped when sleep symptoms abate.
These patients should probably remain on melatonin treatment for the rest of their lives. Some minor shifts in clock time of administration may be required. If not taken daily, escape from steady-state entrainment at the normal phase will likely occur. However, after the pacemaker drifts through a complete cycle, the melatonin dose should again capture the pacemaker at the optimal phase.
Although long-term studies of melatonin need to be done, it is likely that doses of 0.5 mg or less (which result in levels within the same order of magnitude as those produced by the pineal) should be safe. To date, no serious, irreversible side effects have been unequivocally linked to melatonin even at doses greater than 0.5 mg. Nevertheless, we recommend that continuous melatonin treatment be monitored by a physician or other responsible caregiver, who is familiar with the most recent scientific and medical literature.
Other circadian phase disorders
Research in SAD patients and blind people has helped us understand how to treat circadian phase disorders and syndromes in the general sighted population. These disorders include ASPS and DSPS, jet lag, and shift work maladaptation. All of these disorders and syndromes are to a greater or lesser extent related to the circadian timing system and can be phase typed, according to whether they are phase delayed or phase advanced (Table I).
Table I Phase typing for circadian rhythm disorders.
Treatment of these disorders is based on the light and melatonin PRCs.Citation44 To provide a corrective phase advance, bright light should be scheduled immediately upon awakening in the morning and melatonin should be taken in the afternoon/evening. To provide a corrective phase delay, bright light should be scheduled in the evening and melatonin should be taken in the morning.
Delayed sleep phase syndrome
Melatonin and light are both effective in treating DSPS.Citation102,Citation103 The first published report of treating DSPS with light was in 1983.Citation33 This topic is reviewed elsewhere.Citation104 Most people with DSPS are younger and prefer to sleep late in the morning, having difficulty falling asleep until as late as 4.00 am. These individuals can be treated by scheduling their waketimes to occur gradually earlier (perhaps 15 min every other day) until the desired waketime is reached. Going outdoors immediately upon awakening for about 30 min will help advance the circadian rhythm of sleep propensity, as will taking 0.5 mg of melatonin about 8 h after waketime. One or both of these treatments may be necessary to hold the sleep/wake cycle to the desired time. If outdoor sunlight is not available or inconvenient, a portable fixture may be used for 30 to 60 min; the fixture should be at a distance from the eyes so that the intensity is about 10 000 lux. Research on the most potent wavelengths for phase shifting and melatonin suppression may eventually result in some modification of light sources. In the US, melatonin is widely available. If the dose of 0.5 mg happens to cause sleepiness in an individual who is unusually sensitive to this side effect, it should be decreased and a repeat dose should be given a few hours later. For individuals who become sleepy on (usually higher doses of) melatonin, 1 to 3 mg at bedtime may be usefully taken to induce sleep.
Advanced sleep phase syndrome
ASPS generally occurs in older individuals, who tire early in the evening and wake up as early as 4.00 am. The first reference to treating ASPS with light was published in 1985.Citation105 This subject is reviewed elsewhere.Citation104 Treatment recommendations include 1 to 2 h of 10 000 lux exposure in the evening, ending at least 1 h before desired bedtime. Melatonin (0.5 mg) should be taken at each awakening and upon final arising in the morning. Whenever melatonin is taken during waketime, people should not drive if they feel sleepy and lowering the dose should be considered.
Jet lag
Although sleep deprivation resulting from flying at night contributes to the malaise following air travel, there is little doubt that jet lag is caused by a mismatch between circadian rhythms that are tightly coupled to the endogenous circadian pacemaker and destination sleep/wake time. A good rule of thumb is that it takes 1 day to recover from every time zone crossed, with the caveat that jet lag is usually worse when traveling east than when traveling west.
There have been numerous studies of light and melatonin in the amelioration of jet lag. These have been recently reviewed.Citation106,Citation107 The first study to test the effect of light on jet lag was published in 1984.Citation108 The first study to test the effect of melatonin on jet lag was published in 1986.Citation109 On the whole, both have been shown to be somewhat efficacious. However, optimal testing of melatonin in the treatment of jet lag has not yet occurred. For example, no peerreviewed report has included taking 0.5 mg melatonin in the afternoon before traveling east or in the morning before traveling west, which is what we recommend should be done for up to 2 days before travel, as well as on the day of travel. Taking melatonin at destination is more complicated. After traveling across more than five time zones, melatonin can be taken at bedtime. However, as the endogenous circadian pacemaker adjusts to local time, bedtime may not be the best time - and may even be the wrong time - to take melatonin (see below).
Bright light exposure is not convenient to schedule before travel. At destination, obtaining sunlight exposure at the correct time can greatly facilitate circadian realignment. Even more important, particularly after crossing more than five time zones, is avoiding sunlight exposure at the wrong time, which will shift circadian rhythms in the direction opposite to that traveled. When flying from Los Angeles to Madrid, for example, it would take several more days to delay the body clock 15 h than to advance it 9 h. (However, extreme night owls might prefer to delay their clocks no matter which direction of travel.)
Precise recommendations for obtaining and avoiding sunlight at destination depend on what are thought to be the light PRC's break points. The following recommendations are based on a light PRC with the break points at CT 6 and CT 18, using the beginning of the light pulse as its phase reference. Using the middle of a relatively long bout of bright light exposure as the phase reference, which is done in most human (but not animal) studies, would put these break points a few hours later; however, this requires people to schedule long periods of (preferably bright) light exposure. Furthermore, a recent study indicates that the beginning of the light pulse is its most powerful part, at least with respect to causing phase advances.
After traveling across five or fewer time zones, start sunlight exposure as early as possible in the morning after going east or as late as possible in the afternoon after going west. After traveling across six or more time zones, obtain sunlight exposure in the middle of the day and avoid it in the morning after going east or at the end of the day after going west. On subsequent days, these times can be shifted, as if one had traveled through fewer time zones (see below).
Using both light and melatonin at the optimal times, it is reasonable to assume a rate of phase shifting of 3 h per day. For example, after traveling nine time zones to the east, a person who habitually arises at 7.00 am should avoid sunlight exposure before 10.00 am and obtain at least 30 min of it shortly after this time. The next day sunlight exposure should occur shortly after 7.00 am. Melatonin should be taken at 2.00 pm before travel and at 11.00 pm upon reaching the destination. It should then be taken 3 h earlier each day until it is again taken at 2.00 pm for a couple of days. After traveling nine time zones to the west, take melatonin at 10.00 pm the first night, but on subsequent nights it should be taken only if awake after 1.00 am and then again upon final awakening in the morning.
After traveling six or more time zones to the west, bright light should be avoided at the end of the day and sunlight should be obtained in the middle of the day. After 1 or 2 days, bright light should be obtained at the end of the day. Melatonin can be taken at bedtime the first night at destination, but should not be taken before 1.00 am on subsequent days, except under special circumstances. Optimal scheduling of light and melatonin depends on the habitual waketime of an individual, the direction of travel, the number of time zones crossed, and the presumed rate of phase shifting. A complete table of instructions would be helpful and will hopefully be available soon. We recommend taking the lowest dose of melatonin currently available or using a pill cutter. In a few people, even the 0.5 mg dose may cause sleepiness immediately after taking it during the day. Lowering the dose further will reduce the soporific side effect, but then a second dose should be taken a few hours later, particularly when a phase advance is desired, in order to create overlap between the exogenous melatonin pulse and the endogenous melatonin profile, as described above.
Shift work maladaptation
Although it is quite clear that very few shift workers adapt their circadian rhythms to conform to their work schedules, there is no consensus as to how best to help them. This topic has been reviewed elsewhere. The first use of light to treat shift workers was published in 1987.Citation110 The first use of melatonin to treat shift workers was published in the early 1990s.Citation111,Citation112 When trying to sleep at odd hours, shift workers have a type of jet lag. Night workers have the same problems as someone who has traveled through 12 time zones, in fact, worse, since air travelers usually adjust at a rate of at least 1 h per day, as mentioned above. Night workers rarely adjust their circadian rhythms, probably because of the morning sunlight exposure that occurs on the way home from work. Evening workers have it somewhat easier. Chronobiologists uniformly recommend staying on the same schedule every day, week after week. Neither light nor melatonin would then be necessary. However, workers (certainly those who do so at night) are uniformly against sleeping during the day on their weekends. Because their circadian rhythms do not usually adapt to their work schedules, shift workers feel good only on their days off. After working each night, they force themselves to sleep during the day when their body clocks would have them stay up, and of course their work suffers as they soldier through the wee hours of the night when their body clock would have them sleep. A number of medical complaints often accompany shift work, and the older one gets, the harder it is to adapt.
Experts do not agree on how to help shift workers. As mentioned above, part of the problem lies in the fact that some workers would rather feel better on their days off than on their workdays, while managers understandably want workers to be most rested and alert during their hours of employment. Even if this issue is resolved, the next conundrum is that one cannot shift more than 3 to 4 h per day.
Compromise schedules that rely on the use of appropriately timed bright light and/or melatonin administration have been proposed that stabilize circadian phase midway between work and off-work schedules. For example, Eastman and associates have proposed such a compromise schedule.Citation113 We are in the process of developing our own version of a compromise schedule, but its implementation may depend on the development of delayed-relcase melatonin formulations that are not yet available.
Selected abbreviations and acronyms
| ASPS | = | advanced sleep phase syndrome |
| BFR | = | blind free-runner |
| CSI | = | circadian sleep disorder |
| CT | = | circadian time |
| DLMO | = | dim light melatonin onset |
| DSPS | = | delayed sleep phase syndrome |
| MO | = | melatonin onset |
| PRC | = | phase response curve |
| PSH | = | phase shift hypothesis |
| SAD | = | seasonal affective disorder |
| SCN | = | suprachiasmatic nucleus |
| ZT | = | zeitgeber time |
Supported by grants from the Public Health Service (R01 MH56874 to Drs Lewy and Sack; R01 MH55703, R01 AG21826 and R01 HD42125 to Dr Lewy; and MO1 RR00334 to the General Clinical Research Center of OHSU) and the National Alliance for Research on Schizophrenia and Depression (2000 NARSAD Distinguished Investigator Award to Dr Lewy). We are indebted to the nursing staff of the General Clinical Research Center, to Dr Robert Sack, Dr Jonathan Emens, Dr Paul Giger, Dr Kyle Johnson, Rick Boney, Nancy Stahl, Neil Cutler, Bryan Lefler, Krista Yuhas, and Angie Koenig for their valuable assistance, and to Keith Parrott, PharmD, for the formulation of the melatonin capsules.
REFERENCES
- LernerAB.CaseJD.TakahashiY.LeeTH.MoriN.Isolation of melatonin, the pineal gland factor that lightens melanocytes.J Am Chem Soc.1958802587
- ArendtJ.Melatonin and the Mammalian Pineal Gland. London, UK: Chapman & Hall;1995
- LewyAJ.TetsuoM.MarkeySP.GoodwinFK.KopinIJ.Pinealectomy abolishes plasma melatonin in the rat.J Clin Endocr Metab.1980502042057350183
- NeuweltEA.LewyAJ.Disappearance of plasma melatonin after removal of a neoplastic pineal gland.N Engl J Med.1983308113211356835337
- GoldmanBD.DarrowJM.The pineal gland and mammalian photoperiodism.Neuroendocrínology.198337386396
- UnderwoodH.Circadian rhythms in lizards: phase response curve for melatonin.J Pineal Res.198631871963723331
- ArmstrongSM.ThomasEMV.ChesworthMJ.Melatonin-induced phaseshifts of rat circadian rhythms. In: Reiter RJ, Pang SF, eds.Advances in Pineal Research. London, UK: John Libbey;1989265290
- LewyAJ.SackRL.LathamJM.Exogenous melatonin administration shifts circadian rhythms according to a phase response curve. Presented at The Vth Colloquium of the European Pineal Study Group. Guildford, UK; Abstract 021. 1990
- LewyAJ.SackRL.LathamJM.Circadian phase shifting of blind and sighted people with exogenous melatonin administration: evidence for a phase response curve.Soc Light Treatment Biol Rhythms Abst.1990222
- LewyAJ.SackRL.LathamJ.A phase response curve for melatonin administration in humans.Sleep Res.199120461
- LewyAJ.SackRL.LathamJM.Melatonin and the acute suppressant effect of light may help regulate circadian rhythms in humans. In: Arendt J, Pevét P, eds.Advances in Pineal Research. London, UK: John Libbey;1991285293
- LewyAJ.The pineal gland. In: Wyngaarden JB, Smith LH, Bennett JC, eds.Cecil Textbook of Medicine. Philadephia, Pa: WB Saunders;199112461248
- LewyAJ.AhmedS.JacksonJML.SackRL.Melatonin shifts circadian rhythms according to a phase-response curve.Chronobiol Int.199293803921394610
- PickardGE.TurekFW.The hypothalamic paraventricular nucleus mediates the photoperiodic control of reproduction but not the effects of light on the circadian rhythm of activity.Neurosci Lett.19834367726199696
- HendricksonAE.WaggonerN.CowanWM.An autoradiographic and electron microscopic study of retino-hypothalamic connections.Z Zellforsch.19721351264629413
- StephanFK.ZuckerI.Circadian rhythms in drinking behavior and locomotor activity of rats are eliminated by hypothalamic lesions.Proc Natl Acad Sci USA.197269158315864556464
- MooreRY.EichlerVB.Loss of circadian adrenal corticosterone rhythm following suprachiasmatic lesions in the rat.Brain Res.1972422012065047187
- VesselyLH.LewyAJ.Melatonin as a hormone and as a marker for circadian phase position in humans. In: Pfaff D, Arnold A, Etgen A, Fahrbach S, Rubin R, eds.Hormones, Brain and Behavior, Vol 5. San Diego, Calif: Elsevier Science;2002121141
- Ariëns-KappersJ.The development, topographical relations and innervation of the epiphysis cerebri in the albino rat.Z Zellforsch Mikrosk Anat.19605216321513751359
- AxelrodJ.ZatzM.The β-adrenergic receptor and the regulation of circadian rhythms in the pineal gland. In: Litwack G, ed.Biochemical Actions of Hormones. New York, NY: Academic Press;1977249268
- ReppertSM.WeaverDR.RivkeesSA.StopaEG.Putative melatonin receptors are located in a human biological clock.Science.198824278812845576
- DubocovichML.BenloucifS.MasanaMl.Melatonin receptors in the mammalian suprachiasmatic nucleus.Behav Brain Res.1996731411478788492
- GekakisN.StaknisD.NguyenHB.et al.Role of the CLOCK protein in the mammalian circadian mechanism.Science.1998280156415699616112
- BersonDM.DunnFA.TakaoM.Phototransduction by retinal ganglion cells that set circadian clock.Science.20022951070107311834835
- ProvencioI.RodriguezIR.JiangG.HayesWP.MoreiraEF.RollagMD.A novel human opsin in the inner retina.J Neurosci.20002060060510632589
- MooreRY.LennNJ.A retinohypothalamic projection in the rat.J Comp Neurol.19721461144116104
- SchwartzWJ.DavidsenLC.SmithCB.In vivo metabolic activity of a putative circadian oscillator, the rat suprachiasmatic nucleus.J Comp Neurol.19801891571677351445
- SchwartzWJ.GainerH.Localization of the “biological clock” in the brain.JAMA.19812466817253124
- IllnerováH.Melatonin in rat pineal gland and serum; rapid parallel decline after light exposure at night.Neurosci Lett.197818919319605216
- LewyAJ.SackRL.SingerCM.Immediate and delayed effects of bright light on human melatonin production: shifting “dawn” and “dusk” shifts the dim light melatonin onset (DLMO).Ann N Y Acad Sci.19854532532593865585
- AschoffJ.Annual rhythms in man. In: Aschoff J, ed.Handbook of Behavioral Neurobiology. New York, NY: Plenum Press;1981475487
- WehrTA.AeschbachD.DuncanWC.Evidence for a biological dawn and dusk in the human circadian timing system.J Physiol.200193795111559786
- LewyAJ.SackRL.FredricksonRH.ReavesM.DenneyD.ZielskeDR.The use of bright light in the treatment of chronobiologic sleep and mood disorders: the phase-response curve.Psychopharmacol Bull.1983195235256635127
- WeverR.PolasekJ.WildgruberC.Bright light affects human circadian rhythms.Eur J Physiol.19833968587
- LewyAJ.SackRL.SingerCM.Assessment and treatment of chronobiologic disorders using plasma melatonin levels and bright light exposure: the clock-gate model and the phase response curve.Psychopharmacol Bull.1984205615656473662
- LewyAJ.SackRL.MillerS.HobanTM.Antidepressant and circadian phase-shifting effects of light.Science.19872353523543798117
- CzeislerCA.AllanJS.StrogatzSH.et al.Bright light resets the human circadian pacemaker independent of the timing of the sleep-wake cycle.Science.19862336676713726555
- EastmanCI.MiesckeKJ.Bright light improves the entrainment of the circadian body temperature rhythm to a 26-h sleep-wake schedule in humans.Sleep Res.198615271
- LewyAJ.Melatonin secretion as a neurobiological “marker” and effects of light in humans.Psychopharmacol Bull.1982181271297156273
- LewyAJ.Human melatonin secretion (II): a marker for the circadian system and the effects of light. In: Post RM, Ballenger JC, ed.Neurobiology of Mood Disorders. Baltimore, Md: Williams and Wilkins;1984215226
- LewyAJ.BauerVK.HaslerBP.KendallAR.PiresMLN.SackRL.Capturing the circadian rhythms of free-running blind people with 0.5 mg melatonin.Brain Res.20019189610011684046
- LewyAJ.CutlerNL.SackRL.The endogenous melatonin profile as a marker for circadian phase position.J Biol Rhythms.19991422723610452335
- LewyAJ.SackRL.The dim light melatonin onset (DLMO) as a marker for circadian phase position.Chronobiol Int.19896931022706705
- LewyAJ.BauerVK.AhmedS.et al.The human phase response curve (PRC) to melatonin is about 1 2 hours out of phase with the PRC to light.Chronobiol Int .19981571839493716
- LewyAJ.BauerVK.CutlerNL.et al.Morning versus evening light treatment of patients with winter depression.Arch Gen Psychiatry.1998558908969783559
- AschoffJ.HoffmannK.PohlH.WeverR.Re-entrainment of circadian rhythms after phase shifts of the zeitgeber.Chronobiologia.1975223781192905
- LewyAJ.Regulation of melatonin production in humans by bright artificial light: evidence for a clock-gate model and a phase response curve. In: Brown GM, Wainwright SD, ed.The Pineal Gland: Endocrine Aspects. Advances in the Biosciences. Oxford, UK: Pergamon Press;1985203208
- HonmaK.HonmaS.A human phase response curve for bright light pulses.Jpn J Psychiatry.198842167168
- CzeislerCA.KronauerRE.AllanJS.et al.Bright light induction of strong (type O) resetting of the human circadian pacemaker.Science.1989244132813332734611
- WeverRA.Light effects on human circadian rhythms. A review of recent Andechs experiments.J Biol Rhythms.198941611862519587
- MinorsDS.WaterhouseJM.Wirz-JusticeA.A human phase-response curve to light.Neurosci Lett.199113336401791996
- EastmanCI.Bright light on the night shift: circadian rhythms can advance or delay.Sleep Res.199120453
- LewyAJ.WehrTA.GoodwinFK.NewsomeDA.MarkeySP.Light suppresses melatonin secretion in humans.Science.1980210126712697434030
- LewyAJ.KernHA.RosenthalNE.WehrTA.Bright artificial light treatment of a manic-depressive patient with a seasonal mood cycle.Am J Psychiatry.1982139149614987137404
- RosenthalNE.SackDA.GillinJC.et al.Seasonal affective disorder: a description of the syndrome and preliminary findings with light therapy.Arch Gen Psychiatry.19844172806581756
- KripkeDF.RischSC.JanowskyD.Effect on depression of early awakening and bright light.Sleep Res.198211123
- ParryBL.MaurerE.Light treatment of mood disorders.Dialogues Clin Neurosci.2003535336522033495
- Wirz-JusticeA.Chronobiology and mood disorders.Dialogues Clin Neurosci.2003531532522033593
- Praschak-RiederN.WilleitM.Treatment of seasonal affective disorders.Dialogues Clin Neurosci.20035391400
- LewyAJ.SackRL.Minireview: light therapy and psychiatry.Proc Soc Exp Biol Med.198618311183529100
- LewyAJ.SackRL.SingerCM.WhiteDM.HobanTM.Winter depression and the phase shift hypothesis for bright light's therapeutic effects: history, theory and experimental evidence.J Biol Rhythms.198831211342979635
- AveryDH.KhanA.DagerSR.CoxGB.DunnerDL.Bright light treatment of winter depression: morning versus evening light.Acta Psychiatr Scand.1990823353382281802
- SackRL.LewyAJ.WhiteDM.SingerCM.FiremanMJ.VandiverR.Morning versus evening light treatment for winter depression: evidence that the therapeutic effects of light are mediated by circadian phase shifts.Arch Gen Psychiatry.1990473433512322085
- TermanM.TermanJS.QuitkinFM.et al.Dosing dimensions of light therapy: duration and time of day. In: Thompson C, Silverstone T, ed.Seasonal Affective Disorder. London, UK: CNS (Clinical Neuroscience) Publishers;1989187204
- LewyAJ.Treating chronobiologic sleep and mood disorders with bright light.Psychiatry Ann.198717664669
- ThalénB-E.KjellmanBF.MorkridL.WibomR.WetterbergL.Light treatment in seasonal and nonseasonal depression.Acta Psychiatr Scand.1995913523607639093
- Wirz-JusticeA.GrawP.KrauchiK.et al.Light therapy in seasonal affective disorder is independent of time of day or circadian phase.Arch Gen Psychiatry.1993509299378250678
- EastmanCI.YoungMA.FoggLF.LiuL.MeadenPM.Bright light treatment of winter depression: a placebo-controlled trial.Arch Gen Psychiatry.1998558838899783558
- TermanM.TermanJS.RossDC.A controlled trial of timed bright light and negative air ionization for treatment of winter depression.Arch Gen Psychiatry.1998558758829783557
- TermanM.Problems and prospects for use of bright light as a therapeutic intervention. In: Wetterberg L, ed.Light and Biological Rhythms in Man. Stockholm, Sweden: Pergamon Press;1993421436
- TermanJS.TermanM.LoES.CooperTB.Circadian time of morning light administration and therapeutic response in winter depression.Arch Gen Psychiatry.200158697511146760
- VoultsiosA.KennawayDJ.DawsonD.Salivary melatonin as a circadian phase marker: validation and comparison to plasma melatonin.J Biol Rhythms.1997124574669376644
- ZaidanR.GeoffriauM.BrunJ.et al.Melatonin is able to influence its secretion in humans: description of a phase-response curve.Neuroendocrinology.1994601051128090277
- MiddletonB.ArendtJ.StoneBM.Complex effects of melatonin on human circadian rhythms in constant dim light.J Biol Rhythms.1997124674779376645
- LewyAJ.BauerVK.CutlerNL.SackRL.Melatonin treatment of winter depression: a pilot study.Psychiatry Res.199877576110710176
- SackRL.LewyAJ.HobanTM.Free-running melatonin rhythms in blind people: phase shifts with melatonin and triazolam administration. In: Rensing L, an der Heiden U, Mackey MC, ed.Temporal Disorder in Human Oscillatory Systems. Heidelberg, Germany: Springer-Verlag;1987219224
- SackRL.KeithD.LewyAJ.Cortisol and melatonin rhythms in free-running blind people have identical periods.Sleep Res.198918441
- NakagawaH.SackRL.LewyAJ.Sleep propensity free-running in parallel with the melatonin rhythm in a totally blind person.Sleep Res.199120467
- NakagawaH.SackRL.LewyAJ.Sleep propensity free-runs with the temperature, Cortisol and melatonin rhythms in a totally blind person.Sleep.1992153303361519008
- WaterhouseJM.MinorsDS.Masking and entrainment. In: Hekkens WTJM, Kerkhof GA, Rietveld WJ, ed.Trends in Chronobiology. Oxford, UK: Pergamon;1988163171
- SackRL.LewyAJ.BloodML.KeithLD.NakagawaH.Circadian rhythm abnormalities in totally blind people: incidence and clinical significance.J Clin Endocr Metab.1992751271341619000
- LockleySW.SkeneDJ.ArendtJ.Changes in sleep in relation to circadian phase in the blind. In: Touitou Y, ed.Biological Clocks. Mechanisms and Applications. Amsterdam, The Netherlands: Elsevier;1998247252
- SkeneDJ.LockleySW.ArendtJ.Melatonin in circadian sleep disorders in the blind.Biol Signals Receptors.199989095
- LewyAJ.Human plasma melatonin studies: effects of light and implications for biological rhythm research. In: Birau N, Scholoot W, ed.Melatonin: Current Status and Perspectives. Advances in the Biosciences. Oxford, UK: Pergamon Press;1981397400
- LewyAJ.NewsomeDA.Different types of melatonin circadian secretory rhythms in some blind subjects.J Clin Endocrinol Metab.198356110311076841552
- RedmanJ.ArmstrongS.NgKT.Free-running activity rhythms in the rat: entrainment by melatonin.Science.1983219108910916823571
- SackRL.BrandesRW.KendallAR.LewyAJ.Entrainment of free-running circadian rhythms by melatonin in blind people.N Engl J Med.20003431070107711027741
- SackRL.StevensonJ.LewyAJ.Entrainment of a previously free-running blind human with melatonin administration.Sleep Res.199019404
- SackRL.LewyAJ.Melatonin administration phase advances endogenous rhythms in humans.Sleep Res.198817396
- SackRL.LewyAJ.BloodML.StevensonJ.KeithLD.Melatonin administration to blind people: phase advances and entrainment.J Biol Rhythms.199162492611773095
- SackRL.BrandesRL.DeJonghEA.PenS.NordstromS.LewyAJ.Melatonin entrains free-running circadian rhythms in a totally blind person.Sleep.199922(suppl)S138
- LewyAJ.EmensJS.SackRL.HaslerBP.BernertRA.Low, but not high, doses of melatonin entrained a free-running blind person with a long circadian period.Chronobiol Int.20021964965812069043
- LewyAJ.HaslerBP.EmensJS.SackRL.Pretreatment circadian period in free-running blind people may predict the phase angle of entrainment to melatonin.Neurosci Lett.200131315816011682151
- LewyAJ.BauerBK.SingerCW.MinkunasDV.SackRL.Later circadian phase of plasma melatonin relative to usual waketime in older subjects.Sleep.200023(suppl 2)A188
- GekakisN.SaezL.Delahaye-BrownA.et al.Isolation of timeless by PER protein interaction: defective interaction between timeless protein and long-period mutant PER.Science.19952708118157481773
- YoungMW.The tick-tock of the biological clock.Sci Am.2000647110736840
- BersonDM.DunnFA.TakaoM.Phototransduction by retinal ganglion cells that set circadian clock.Science.20022951070107311834835
- PittendrighCS.DaanS.A functional analysis of circadian pacemakers in nocturnal rodents: IV. Entrainment: pacemaker as a clock.J Comp Physiol.1976106291331
- LockleySW.SkeneDJ.JamesK.ThapanK.WrightJ.ArendtJ.Melatonin administration can entrain the free-running circadian system of blind subjects.J Endocrinol.2000164R1R610607943
- LewyAJ.EmensJS.BernertRA.LeflerBJ.Eventual entrainment of the human circadian pacemaker by melatonin is independent of the circadian phase of treatment initiation: clinical implications.J Biol Rhythms. In press.
- LewyAJ.EmensJS.SackRL.HaslerBP.BernertRA.Zeitgeber heirarchy in humans: resetting the circadian phase positions of blind people using melatonin.Chronobiol Int.20032083785214535357
- DahlitzM.AlvarezB.VignauJ.EnglishJ.ArendtJ.ParkesJD.Delayed sleep phase syndrome response to melatonin.Lancet.1991337112111231674014
- RosenthalNE.Joseph-VanderpoolJR.Levendosky AA, et al. Phototherapy for delayed sleep phase syndrome.Biol Psychiatry.19912940S
- SchenckCH.MahowaldMW.SackRL.Assessment and management of insomnia.JAMA.20032892475247912759306
- LewyAJ.SackRL.SingerCM.Melatonin, light and chronobiological disorders. In: Evered D, Clark S, ed.Photoperiodism, Melatonin and the Pineal. London, UK: Pitman;1985231252
- HerxheimerA.PétrieKJ.Melatonin for the prevention and treatment of jet lag.Cochrane Library.2002Disk issue 4CD001520
- SackRL.Shift work and jet lag. In: Lee-Chiong TL, Sateia MJ, Carskadon MA, ed.Sleep Medicine. Philadelphia, Pa: Hanley and Belfus;2002
- DaanS.LewyAJ.Scheduled exposure to daylight: a potential strategy to reduce “jet lag” following transmeridian flight.Psychopharmacol Bull.1984205665686473663
- ArendtJ.AldhousM.MarksV.Alleviation of “jet lag” by melatonin: preliminary results of controlled double-blind trial.BMJ.198629211703085768
- EastmanCI.Bright light in work-sleep schedules for shift workers: application of circadian rhythm principles. In: Rensing L, an der Heiden U, Mackey MC, ed.Temporal Disorder in Human Oscillatory Systems. New York, NY: Springer-Verlag;1987176185
- SackRL.BloodML.LewyAJ.Melatonin rhythms in night shift workers.Sleep.1992154344411455127
- SackRL.BloodML.LewyAJ.Melatonin administration promotes circadian adaptation to night-shift work.Sleep Res.199423509
- EastmanCI.MartinSK.How to use light and dark to produce circadian adaptation to night shift work.Ann Med.199931879810344580