
Abstract
Context: A comprehensive meta-analysis was carried out to investigate the impact of orthodontics on masticatory muscles.
Methods: A thorough search of various databases, including CNKI, Wan Fang, VIP, CBM, MEDLINE, PubMed, Cochrane Library, EMBASE, Web of Science, and Google Scholar, was performed to identify relevant studies on patients undergoing orthodontics or functional corrections. Six case-control studies were finally included in this analysis, which specifically examined the effect of orthodontic treatment on masticatory muscle function.
Results: The results revealed that the mean masticatory muscle voltage in patients treated with orthodontics was found to be higher after treatment compared to before treatment [odds ratio (OR)=1.57, 95% confidence interval (CI) (0.57, 2.57), p = 0.002], which could potentially have an impact on masticatory muscle function, particularly in individuals with Class II Division 1 malocclusion.
Conclusion: These findings contribute to our understanding of the effects of orthodontic interventions on masticatory muscles, further highlighting the importance of orthodontics in optimising masticatory function.
Introduction
Electromyography (EMG) is a technique used to measure the electrical activity of muscles (Ngo et al. Citation2022). It involves the placement of electrodes on the skin above specific muscles to detect and record the muscle’s electrical signals. The analysis aims to extract meaningful information about muscle activation, coordination, fatigue, and other relevant factors. In the 1940s, Dr. Moyer (Moyers Citation1950) reported the characteristics of electromyography (EMG) of masticatory muscles in patients with misaligned jaws and applied EMG to stomatology for the first time. EMG can objectively and quantitatively reflect the functional state of the neuromuscular system, providing an important means for the study of the relationship between the morphology and function of the oral-maxillofacial system, as well as the clinical diagnosis, treatment, and efficacy evaluation of oral-maxillofacial diseases. With the development of electronic technology and the popularisation of electronic computer application, the study of EMG has gradually evolved from qualitative analysis to quantitative analysis and gradually become the main technology to evaluate the steady-state ability of the human body to adapt to the changes of oral and maxillofacial systems.
Orthodontic treatment helps to fully restore the teeth to their perfect stage, coordinates, balance the tooth-jaw system, achieve the purpose of correcting deformities, and beautify the appearance by using correction technologies. Some published literature also shows that orthodontic treatment can affect patients’ masticatory muscles (Tecco et al. Citation2011; Baldini et al. Citation2015). Its mechanism is to change the position of the upper and lower jaw, enabling the position of the attached muscles to change to a certain extent, and then the masseter muscle changes (Mummolo et al. Citation2020). Neuromuscular function seems to be related to the stability of occlusion (Wang and Yin Citation2012; Baldini et al. Citation2015). The use of orthodontic devices may affect the central nervous system (CNS) during orthodontic treatment. Some previous studies have demonstrated the effect of functional orthodontics and orthodontics on masticatory muscle activity (Ghislanzoni et al. Citation2011; Woźniak et al. 201; Woźniak et al. Citation2015; Lou et al. Citation2021), and recent studies have also shown the effect of wearing transparent orthodontics on masticatory muscle activity (Saccucci et al. Citation2011), so it is reasonable to explain orthodontic treatment by extending the connected muscles through jaw motion (Bishara and Ziaja Citation1989). At present, there have been many relevant studies on the impact of orthodontic treatment on patients’ masticatory muscles domestically and abroad, but no definite conclusions have been made so far. Therefore, this study used the relevant results of EMG of patients’ masticatory muscles as an evaluation index for the systematic analysis, so as to study the impact of orthodontic treatment on patients’ masticatory muscles.
Methods
We performed a meta-analysis based on the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement.
Study criteria
Studies had to meet the following criteria to be included: (1) literature on semi-randomised controlled trials, randomised controlled trials, and clinical case-control trials of orthodontic treatment in both Chinese and English, published at any time; (2) patients requiring orthodontic treatment had not undergone orthodontic or maxillofacial surgery before treatment, had no masticatory muscle diseases before treatment, had complete surgical records and medical records during treatment, and were followed up for at least 1 month after surgery; (3) there were no restrictions on age, sex, nationality, ethnicity, and complications, and they could communicate or participate in research independently; (4) total number of cases included in the study and average masseter voltage measured by EMG before and after treatment.
The exclusion criteria were: (1) animal experiments, case reports, letters, review articles, summaries of personal experience, discussions, meta-analyses, etc.; (2) repeated publication of the same study, or incomplete, chaotic, and unavailable data in the literature; (3) research objects that did not meet the requirements; (4) interventions that did not conform to the study.
Literature sources and retrieval strategies
The results of this study included CNKI, Wan Fang, VIP, CBM, MEDLINE, PubMed, Cochrane Library, EMBASE, Web of Science and Google Scholar which were searched by computer. The search period was dated from January 1956 to September 2021. At the same time, manual retrieval was carried out on the references of the corresponding articles, and related literature was searched as comprehensively as possible. In addition, relevant reviews and systematic evaluations published previously were traced to avoid missing detection. The search keywords adopted were as follows: "Electromyography" AND ("Masseter muscle" OR "Masticatory muscle") AND ("Orthodontics " OR "Orthopaedic therapy "). Their English meanings, synonyms, etc. were also searched.
Document screening
The basic process of data selection was as follows: (1) the initial screening: all documents were imported into EndNote software which could eliminate duplicate documents; two researchers independently read the rest of the document titles and abstracts, eliminating unqualified literature; the third researcher was involved if opinions differed and disagreements were resolved by tripartite consultation and agreement; if consensus still could not be met after negotiation, the fourth researcher was involved; (2) full-text screening: according to the inclusion and exclusion criteria, the researchers read the full text and excluded unqualified literatures again, leaving the remaining literature the finally included literature; the reasons for exclusion were recorded; (3) incomplete information: the corresponding authors of the included studies were contacted to supplement the required information as comprehensively as possible.
Data extraction and quality assessment
The main contents included: (1) basic characteristics: first author, publication year, study type, number of cases, subjects, interventions, and outcome indicators; (2) intervention measures: for various reasons, the need for orthodontic treatment for treatment or aligner, orthodontic surgery; (3) the outcome indicators: the total number of cases, before and after treatment in the study of masseter, and the average voltage value; (4) all indicators of research quality evaluation were included. Different methodological quality evaluation criteria were used according to different types of trials included in the study. The quality of the articles included in this study was determined by the Newcastle-Ottawa Quality Assessment Scale. The above contents were independently extracted and evaluated by three researchers for summary analysis and verification, and differences were resolved through consultation and discussion among three parties.
Statistics
Meta-analysis was performed using RevMan 5.3 software. The researchers input the extracted data and merged the data for analysis. In terms of effect size selection, Standardised Mean Difference (SMD) was used for continuous variables, and 95% CIs were used for each effect size. To assess heterogeneity, I2 and Q statistical tests were performed. For heterogeneity assessment, I2 was classified as none (0-25%), low (26-50%), medium (51-75%), or high (>75%). The difference was statistically significant (p ≤ 0.05), and the test was repeated twice. Random effects model was used if heterogeneity existed, and fixed effects model was used if heterogeneity did not exist to explain differences within and between studies. Publication bias was evaluated using funnel plot, Mr Begg inspection and Egger regression asymmetry evaluation. Data analysis was performed using R version 4.1.1.
Results
Literature retrieval and research traits
The flowchart of literature retrieval is described in . A total of 397 articles were retrieved from the databases. After automatic and manual removal of duplicate literatures, 234 literatures were further excluded by reading titles and abstracts in strict accordance with the inclusion and exclusion criteria. The remaining 59 literatures were further read through in full text and 53 literatures were excluded. Six articles were included in our final meta-analysis. The data of the final included literature are listed in . The six included articles (Aggarwal et al. Citation1999; Akkaya et al. Citation2000; Arat et al. Citation2008; DeRossi et al. Citation2009; Sood et al. Citation2011; Satygo et al. Citation2014) evaluated the effects of orthodontic treatment on masticatory muscles through EMG.
Figure 1. The flowchart of literature retrieval.
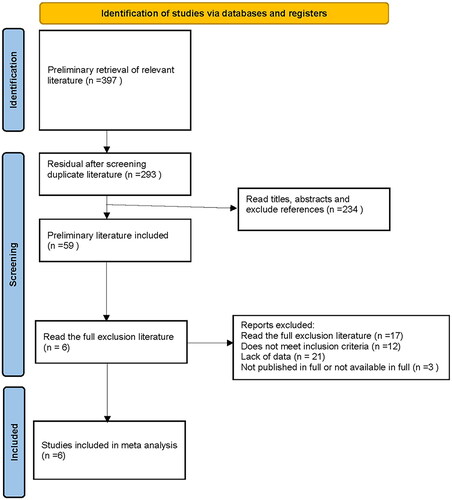
Table 1. Qualitative data of the systematic search (n = 6 studies).
Relationship between orthodontic treatment and masticatory muscle
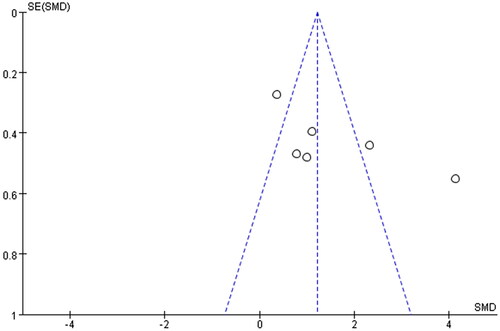
The six studies reported differences in the mean masticatory muscle voltage values before and after orthodontic treatment. shows the effects of orthodontic treatment on masticatory muscles in the included literature, with significant heterogeneity among studies (p = 0.002, I2=89%), combined with a random-effect model. Results obtained from meta-analysis showed that the mean masticatory muscle voltage of patients treated with orthodontics was higher after treatment than before treatment, and the difference was statistically significant (pooled OR = 1.57; 95% CI = 0.57, 2.57; Z value = 3.07, p < 0.00001). Funnel plots for all included studies showed slight asymmetry in , indicating potential publication bias in the included literature.
Figure 2. Forest plot of masseter muscle mean voltage.
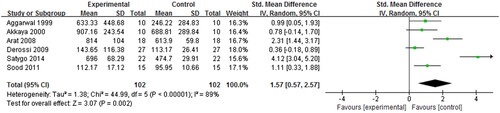
Figure 3. Funnel plot of masseter muscle mean voltage.
Publication bias
R Version 4.1.1 was used to conduct Begg and Egger’s tests to further evaluate publication bias in the literature. The results obtained p = 0.1885 in the Begg test and p = 0.0915 in the Egger test, indicating that there was no significant publication bias in the literature.
Sensitivity analysis
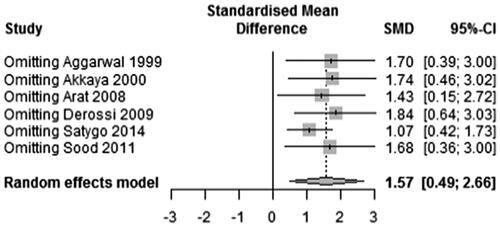
In view of the heterogeneity among the included studies, sensitivity analysis was performed to further explore the source of heterogeneity and to judge the stability of the combined results. The correlation analysis between orthodontic treatment and masticatory muscle was shown in . After removing a single study at each time, I2 was shown to decrease from 89% to 88.9%, and the combined effect size was OR = 1.57; 95% CI = 0.49, 2.66; p = 0.0045, which was generally consistent with the statistical analysis results before exclusion, suggesting that the meta-analysis results were stable.
Figure 4. Risk sensitivity analysis of masseter muscle mean voltage.
Discussion
Orthodontic treatment adjusts the coordination between the facial bones and teeth and maxillofacial soft tissue through adjusting the abnormal relationships between the jaws, the teeth, and the neuromuscular soft tissues that connect them via medical procedures. The ultimate orthodontic goal is to achieve balance, stability, and aesthetics of the oral and maxillofacial system. Nowadays, the incidence of malocclusion has been the most prevalent in oral treatment, leading to a strong demand for orthodontic treatment during oral treatment. Correction of malocclusion can not only improve the occlusal relationship of patients, but also correct the psychological inferiority of patients due to malocclusion.
Malocclusion affects the EMG activity of masticatory muscles of patients (Tosello et al. Citation1999), and the EMG activity of masseter muscles of patients with malocclusion is lower than that of normal people. The decrease of masseter muscle potential was more obvious during the maximum bite at intercuspal position (ICP). Previous studies (Nota et al. Citation2021) have shown that the orthodontic treatment could slightly change the occlusal relationship to some extent, which could lead to a decrease in muscle activity in the short term. However, after three months, the masseter muscle potential could be recovered, and the average voltage value of masseter muscle was higher than before. By looking at a similar study about using orthoses for four weeks, masticatory muscle activity increased in the first two weeks and returned to baseline four weeks later. Long-term observation was not made due to time constraints (Woźniak et al. Citation2013). Satygo et al. (Citation2014) studied the EMG activity of temporalis muscle and masseter muscle in class II and class I malocclusion patients treated with orthodontic trainers. Results showed that the functional appliance could improve EMG muscle activity during treatment to a level similar to that of normal occlusal patients. Ortu et al. (Ortu et al. Citation2019) showed that orthodontic treatment did not affect the activity of masticatory muscles, and after six months of neuromuscular orthodontics, the muscles of patients at rest were more relaxed than those receiving traditional orthodontics, indicating higher effectiveness of neuromuscular orthodontics.
In addition to the impact of orthodontic treatment on masticatory muscle in patients with malocclusion, orthodontic treatment can relieve masticatory muscle pain and related symptoms and signs in patients with myofascial pain syndrome (Tecco et al. Citation2012). In the study of subjects with internal temporomandibular joint (TMJ) disorders, the occlusal device can affect the activation of masseter muscle and anterior temporal muscle (Tecco et al. Citation2008), and after one month of occlusal splint treatment, the degree of fatigue of the masticatory muscles of patients was reduced (Zhang et al. Citation2013). Previous studies (Yagci et al. Citation2010; Uysal et al. Citation2012) have shown that EMG of masticatory muscles was used to evaluate the effect of functional instrument treatment for six months on patients’ masticatory muscles. The results showed that functional appliance reduced the frequency of EMG of masticatory muscles and muscle fatigue. At the same time, the amplitude of EMG was used to represent the force generated during muscle contraction (de Jong et al. Citation2011), which proved that the amplitude of EMG of masticatory muscle could be changed by the appliance. All the above studies indicated that orthodontic treatment has varying degrees of influence on masticatory muscle function of patients.
Although orthopaedic treatment or functional orthopaedics on patients can usually achieve satisfaction, because of the differences in bones, muscles, and dental parameters, there is often a huge variation between individuals, so each patient might require a deep understanding on the treatments and their muscle environment in order to ensure the best treatment effect and the stability of the environment (Patini et al. Citation2017). A study conducted by Winocur et al. (Winocur et al. Citation2007) showed that the oral and maxillofacial system would change after the use of orthodontic or functional orthodontics, and the chewing efficiency of patients was significantly reduced 24 h after initial usage (Ghislanzoni et al. Citation2011; Gameiro et al. Citation2015), which was considered to be due to discomfort, pain or changes in the occlusal relationship between maxillary and mandibular dentition (Miyamoto et al. Citation1996). Masseter and temporalis muscle masticatory efficiency decreased in the short term, but Nishi (Nishi et al. Citation2021) reported that temporalis muscle activity was better during masticatory activity after six months of orthodontic treatment than before.
Orthodontic treatment has a good effect on patients with long-term chewing function, and thus in this meta-analysis, we studied the influence of orthodontic treatment on masticatory muscles. Studies have shown that after orthodontic treatment for at least three months, the average voltage value of patients’ masticatory muscles increased significantly compared with that before treatment. In the electromyogram signal of masticatory muscles, the increase of average voltage value represents the improvement of muscle function, which proves that orthodontic treatment can affect patients’ masticatory muscles to a certain extent. The function of masticatory muscle improved after at least three months of treatment, especially in patients with malocclusion.
Conclusion
Orthodontic treatment can improve the electrical activity of masticatory muscle in patients, especially in individuals with Class II Division 1 dental deformities. These findings highlight the importance of orthodontic treatment in optimising masticatory function.
Author’s contribution
Yuxiang Zhan, Minjie Yang and Shuoqiu Bai carried out study concept & design, literature research, data analysis and statistical analysis; Siqin Zhang, Fansheng Gong, Yunqin Huang and Xiaolin Nong contributed to experimental studies and data acquisition; Yuxiang Zhan is the guarantor of integrity of the entire study and helped to manuscript preparation and editing.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Aggarwal P, Kharbanda OP, Mathur R, Duggal R, Parkash H. 1999. Muscle response to the twin-block appliance: an electromyographic study of the masseter and anterior temporal muscles. Am J Orthod Dentofacial Orthop. 116(4):405–414. doi:10.1016/S0889-5406(99)70225-8.
- Akkaya S, Haydar S, Bilir E. 2000. Effects of spring-loaded posterior bite-block appliance on masticatory muscles. Am J Orthod Dentofacial Orthop. 118(2):179–183. doi:10.1067/mod.2000.104809.
- Arat FE, Arat ZM, Acar M, Beyazova M, Tompson B. 2008. Muscular and condylar response to rapid maxillary expansion. Part 1: electromyographic study of anterior temporal and superficial masseter muscles. Am J Orthod Dentofacial Orthop. 133(6):815–822. doi:10.1016/j.ajodo.2006.07.028.
- Baldini A, Nota A, Cioffi C, Ballanti F, Cozza P. 2015. Infrared thermographic analysis of craniofacial muscles in military pilots affected by bruxism. Aerosp Med Hum Perform. 86(4):374–378. doi:10.3357/AMHP.4115.2015.
- Baldini A, Nota A, Cozza P. 2015. The association between Occlusion Time and Temporomandibular Disorders. J Electromyogr Kinesiol. 25(1):151–154. doi:10.1016/j.jelekin.2014.08.007.
- Bishara SE, Ziaja RR. 1989. Functional appliances: a review. Am J Orthod Dentofacial Orthop. 95(3):250–258. doi:10.1016/0889-5406(89)90055-3.
- de Jong WC, Korfage JAM, Langenbach GEJ. 2011. The role of masticatory muscles in the continuous loading of the mandible. J Anat. 218(6):625–636. doi:10.1111/j.1469-7580.2011.01375.x.
- DeRossi M, DeRossi A, Hallak JE, Vitti M, Regalo SC. 2009. Electromyographic evaluation in children having rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 136(3):355–360. doi:10.1016/j.ajodo.2007.08.027.
- Gameiro GH, Schultz C, Trein MP, Mundstock KS, Weidlich P, Goularte JF. 2015. Association among pain, masticatory performance, and proinflammatory cytokines in crevicular fluid during orthodontic treatment. Am J Orthod Dentofacial Orthop. 148(6):967–973. doi:10.1016/j.ajodo.2015.05.029.
- Ghislanzoni LT, Toll DE, Defraia E, Baccetti T, Franchi L. 2011. Treatment and posttreatment outcomes induced by the mandibular advancement repositioning appliance; a controlled clinical study. Angle Orthod. 81(4):684–691. doi:10.2319/111010-656.1.
- Lou T, Tran J, Castroflorio T, Tassi A, Cioffi I. 2021. Evaluation of masticatory muscle response to clear aligner therapy using ambulatory electromyographic recording. Am J Orthod Dentofacial Orthop. 159(1):e25–e33. doi:10.1016/j.ajodo.2020.08.012.
- Miyamoto K, Ishizuka Y, Tanne K. 1996. Changes in masseter muscle activity during orthodontic treatment evaluated by a 24-hour EMG system. Angle Orthod. 66(3):223–228.
- Moyers RE. 1950. An electromyographic analysis of certain muscles involved in temporomandibular movement. Am J Orthod. 36 (7):481–515. doi:10.1016/0002-9416(50)90063-7.
- Mummolo S, Nota A, Tecco S, Caruso S, Marchetti E, Marzo G, Cutilli T. 2020. Ultra-low-frequency transcutaneous electric nerve stimulation (ULF-TENS) in subjects with craniofacial pain: a retrospective study. Cranio. 38(6):396–401. doi:10.1080/08869634.2018.1526849.
- Ngo C, Munoz C, Lueken M, Hülkenberg A, Bollheimer C, Briko A, Kobelev A, Shchukin S, Leonhardt S. 2022. A wearable, multi-frequency device to measure muscle activity combining simultaneous electromyography and electrical impedance myography. Sensors. 22(5):1941. doi:10.3390/s22051941.
- Nishi SE, Rahman NA, Basri R, Alam MK, Noor NFM, Zainal SA, Husein A. 2021. Surface electromyography (sEMG) activity of masticatory muscle (masseter and temporalis) with three different types of orthodontic bracket. Biomed Res Int. 2021:6642254–6642255. doi:10.1155/2021/6642254.
- Nota A, Caruso S, Ehsani S, Ferrazzano GF, Gatto R, Tecco S. 2021. Short-term effect of orthodontic treatment with clear aligners on pain and sEMG activity of masticatory muscles. Medicina (Kaunas). 57(2):178. doi:10.3390/medicina57020178.
- Ortu E, Pietropaoli D, Adib F, Masci C, Giannoni M, Monaco A. 2019. Electromyographic evaluation in children orthodontically treated for skeletal Class II malocclusion: comparison of two treatment techniques. Cranio. 37(2):129–135. doi:10.1080/08869634.2017.1393916.
- Patini R, Gallenzi P, Spagnuolo G, Cordaro M, Cantiani M, Amalfitano A, Arcovito A, Callà C, Mingrone G, Nocca G. 2017. Correlation between metabolic syndrome, periodontitis and reactive oxygen species production. A pilot study. Open Dent J. 11(1):621–627. doi:10.2174/1874210601711010621.
- Saccucci M, Tecco S, Ierardoa G, Luzzi V, Festa F, Polimeni A. 2011. Effects of interceptive orthodontics on orbicular muscle activity: a surface electromyographic study in children. J Electromyogr Kinesiol. 21(4):665–671. doi:10.1016/j.jelekin.2011.03.005.
- Satygo EA, Silin AV, Ramirez-Yañez GO. 2014. Electromyographic muscular activity improvement in Class II patients treated with the pre-orthodontic trainer. J Clin Pediatr Dent. 38(4):380–384. doi:10.17796/jcpd.38.4.2vh1603n62878673.
- Sood S, Kharbanda OP, Duggal R, Sood M, Gulati S. 2011. Neuromuscular adaptations with flexible fixed functional appliance–a 2-year follow-up study. J Orofac Orthop. 72(6):434–445. doi:10.1007/s00056-011-0048-x.
- Tecco S, Marzo G, Crincoli V, Di Bisceglie B, Tetè S, Festa F. 2012. The prognosis of myofascial pain syndrome (MPS) during a fixed orthodontic treatment. Cranio. 30(1):52–71. doi:10.1179/crn.2012.007.
- Tecco S, Mummolo S, Marchetti E, Tetè S, Campanella V, Gatto R, Gallusi G, Tagliabue A, Marzo G. 2011. sEMG activity of masticatory, neck, and trunk muscles during the treatment of scoliosis with functional braces. A longitudinal controlled study. J Electromyogr Kinesiol. 21(6):885–892. doi:10.1016/j.jelekin.2011.08.004.
- Tecco S, Tetè S, D’Attilio M, Perillo L, Festa F. 2008. Surface electromyographic patterns of masticatory, neck, and trunk muscles in temporomandibular joint dysfunction patients undergoing anterior repositioning splint therapy. Eur J Orthod. 30(6):592–597. doi:10.1093/ejo/cjn052.
- Tosello DO, Vitti M, Berzin F. 1999. EMG activity of the orbicularis oris and mentalis muscles in children with malocclusion, incompetent lips and atypical swallowing–part II. J Oral Rehabil. 26(8):644–649. doi:10.1046/j.1365-2842.1999.00409.x.
- Uysal T, Yagci A, Kara S, Okkesim S. 2012. Influence of pre-orthodontic trainer treatment on the perioral and masticatory muscles in patients with Class II division 1 malocclusion. Eur J Orthod. 34(1):96–101. doi:10.1093/ejo/cjq169.
- Wang C, Yin X. 2012. Occlusal risk factors associated with temporomandibular disorders in young adults with normal occlusions. Oral Surg Oral Med Oral Pathol Oral Radiol. 114(4):419–423. doi:10.1016/j.oooo.2011.10.039.
- Winocur E, Davidov I, Gazit E, Brosh T, Vardimon AD. 2007. Centric slide, bite force and muscle tenderness changes over 6 months following fixed orthodontic treatment. Angle Orthod. 77(2):254–259. doi:10.2319/0003-3219(2007)077[0254:CSBFAM.2.0.CO;2]
- Woźniak K, Piątkowska D, Lipski M, Mehr K. 2013. Surface electromyography in orthodontics - a literature review. Med Sci Monit. 19:416–423. doi:10.12659/MSM.883927.
- Woźniak K, Piątkowska D, Szyszka-Sommerfeld L, Buczkowska-Radlińska J. 2015. Impact of functional appliances on muscle activity: a surface electromyography study in children. Med Sci Monit. 21:246–253. doi:10.12659/MSM.893111.
- Yagci A, Uysal T, Kara S, Okkesim S. 2010. The effects of myofunctional appliance treatment on the perioral and masticatory muscles in Class II, Division 1 patients. World J Orthod. 11(2):117–122.
- Zhang FY, Wang XG, Dong J, Zhang JF, Lü YL. 2013. Effect of occlusal splints for the management of patients with myofascial pain: a randomized, controlled, double-blind study. Chin Med J (Engl). 126(12):2270–2275.