
Abstract
Objectives: To compare the impact of appearance versus health-framed messages on engagement in a brief web-based risk screening and alcohol reduction intervention.
Design: Randomised trial delivered via Drinkaware’s website. Visitors were exposed to appearance (n = 51,588) or health-framed messages (n = 52,639) directing them towards an AUDIT-C risk screening questionnaire. Users completing this questionnaire were given feedback on their risk level and extended frame-congruent information.
Outcomes: The primary outcome is completion of the AUDIT-C questionnaire. The secondary outcome is whether the participant accessed any of four further resources.
Results: The appearance-framed message led to a small but significant increase in the number of users completing the AUDIT-C compared to the health-framed message (n = 3,537, 6.86% versus n = 3,355, 6.37%, p < 0.01). Conversely, following subsequent risk feedback, users exposed to extended health-framed information were more likely to access further resources (n = 1,146, 2.17% versus n = 942, 1.83%, p < 0.01).
Conclusions: Physical appearance-framed messages increased the likelihood of engagement with an online alcohol screening and brief intervention tool, whereas health-framed messages increased the likelihood of accessing further resources. This highlights the potential for the use of multi-level approaches in alcohol reduction interventions.
Introduction
Alcohol consumption in the UK
In 2016, 31% of men and 16% of women drank over the low-risk drinking guidelines of no more than 14 units of alcohol per week (NHS Digital, Citation2016). This is despite the UK Chief Medical Officers’ (CMO) recently issued guidelines on alcohol consumption warning that the risk of cancer increases with any level of consumption, and that neither men nor women should regularly consume more than recommended guideline amounts, while also taking care to spread their intake over three or more days per week (rather than binge drink) in order to keep their risk low (Department of Health, Citation2015).
Previously, both anecdotal and peer-reviewed evidence has shown excessive alcohol consumption to be more common in certain sociodemographic groups, such as in adolescents or older males (Britton, Ben-Shlomo, Benzeval, Kuh, & Bell, Citation2015; Healey, Rahman, Faizal, & Kinderman, Citation2014). However, as recent statistics from the UK indicate, a shift in the sociodemographic patterning of alcohol consumption is now underway. Reductions in intake have recently been observed in younger age groups (Institute of Alcohol Studies, Citation2016; Meng, Holmes, Hill-McManus, Brennan, & Meier, Citation2013; NHS Digital, Citation2016), while regular consumption of alcohol, in particular wine, has risen in older age groups and in higher income quintiles (Lewer, Meier, Beard, Boniface, & Kaner, Citation2016). These trends are situated within a wider general context of more frequent drinking in older age groups in the UK, and particularly pronounced increases in older women (Britton et al., Citation2015; Smith, 2009). As such, it is likely that existing interventions to encourage reductions in alcohol consumption now require adaptation to ensure their relevance to these newly emerging ‘high risk’ groups (McCabe et al., Citation2015).
Screening and brief interventions (SBIs) to reduce alcohol consumption
One common approach to reducing alcohol consumption involves screening for alcohol disorders followed by brief intervention (SBI) (Kaner et al., Citation2013). These SBIs are generally delivered in primary care by healthcare professionals, typically last between five to 30 minutes and incorporate screening for alcohol harms, personalised feedback, information provision and strategies to encourage behaviour change (Kaner et al., Citation2018). One tool used to facilitate SBI delivery is the ‘AUDIT-C’ questionnaire, a shortened version of the full ‘Alcohol Use Disorders Identification Test’ (AUDIT). This well-established and pragmatic questionnaire has proven validity in identifying increasing and higher risk drinkers across a range of different population groups (Fujii et al., Citation2016; Larsson & Nehlin, Citation2016; Meneses-Gaya et al., Citation2010).
However, despite promising evidence of effectiveness (O’Donnell et al., Citation2014a; O’Donnell, Wallace, & Kaner, Citation2014b; Scott & Kaner, Citation2014), the potential for SBIs to reach and impact the alcohol consumption of large numbers of recipients has so far been limited by their use predominantly within primary care settings (Khadjesari et al., Citation2015a). This is problematic given research to suggest that the stigma so often associated with excessive alcohol intake can mean patients attending healthcare consultations are reluctant to self-report their true alcohol consumption patterns. This, therefore, precludes identification of appropriate SBI recipients (Haighton et al., Citation2016; Khadjesari, Stevenson, Godfrey, & Murray, Citation2015b). Moreover, there is also evidence that healthcare professionals themselves may be disinclined to deliver SBIs, possibly owing to a lack of organisational support, time, resources and training (Anderson et al., Citation2016, Citation2014; Brown et al., Citation2016; Scott & Kaner, Citation2014).
In response to these barriers, and in recognition of the opportunities for intervention afforded by widespread smart phone and internet access, focus has more recently been directed towards digital platforms as potential alternative routes to SBI delivery (Dulin, Gonzalez, & Campbell, Citation2014; Gonzalez & Dulin, Citation2015; Khadjesari et al., Citation2015a; Sinadinovic, Wennberg, Johansson, & Berman, Citation2014). It is argued that delivering alcohol reduction interventions digitally can offer benefits over and above more traditional approaches such as face-to-face intervention (Johnson, Kypri, & Attia, Citation2013). For example, not only are digital tools comparatively low cost and have potentially broader reach (Andrade et al., Citation2016), two particularly relevant issues for SBIs given that large numbers of people need to be screened in order for brief interventions to elicit measurable impacts on population health (Riper et al., Citation2014), they also afford users anonymity and convenience. These two attributes may help encourage individuals who might wish to reduce their alcohol intake, but who are unlikely to attend primary care for this reason, either due to a lack of time or, as noted, for fear of labelling or stigmatisation (Khadjesari et al., Citation2015b; Murray, Khadjesari, Linke, Hunter, and Freemantle, Citation2013).
A number of self-help digital tools are already publicly available to assist those seeking help and support to reduce their alcohol consumption. One of the widest reaching of these is the website of the Drinkaware Trust, a UK-wide alcohol education charity that aims to reduce alcohol-related harm by helping people to make better choices about their drinking (www.drinkaware.co.uk). As is clear from the number of visitors to Drinkaware’s website (e.g. 8.3-m unique visits in 2014 when this study was designed), digital platforms like this one are extremely well positioned to deliver SBIs at volume to individuals who may already be contemplating making changes to their drinking behaviour and who are in the process of seeking out information and help to support them in this agenda.
SBIs and message framing
The effectiveness of SBIs will depend on the extent to which recipients engage with the content delivered therein, which is, in turn, influenced by the way in which the persuasive messages that they contain are ‘framed’ or presented (Rothman & Salovey, Citation1997).
To date, different message frame variants have been trialled in interventions that aim to reduce alcohol consumption. These include emotion-based message frames invoking shame and guilt (Agrawal & Duhachek, Citation2010), finding participants are particularly resistant to messages that exacerbate negative emotions, and loss versus gain-framed messages (Bernstein, Wood, & Erickson, Citation2016; de Graaf, van den Putte, & de Bruijn, Citation2015; Harrington & Kerr, Citation2017; Hutter, Lawton, Pals, O’Connor, & McEachan, Citation2014; Mckay, Ballantyne, Goudie, Sumnall, & Cole, Citation2012), with research showing frame type tends to exert no main effect, but do interact significantly with other psychological variables of interest such as degree of issue of involvement or perceived severity of health risks.
Other types of message frames that have also been trialled in existing research studies include those that manipulate information presented on the social norms or consequences of drinking (Kingsbury, Gibbons, & Gerrard, Citation2014; Taylor, Vlaev, Maltby, Brown, & Wood, 2015), finding unfavourable peer group comparisons and loss-framed information emphasising the social consequences of being drunk tend to reduce alcohol consumption intentions and behaviour, in addition to messages that vary the temporal context of consumption-related outcomes (Gerend & Cullen, Citation2008). In this latter study by Gerend & Cullen (Citation2008), students who read gain-framed alcohol reduction messages in a laboratory setting reported drinking less compared to those exposed to loss-framed messages, with temporal context acting as a moderator of the framing effect (i.e. gain framed messages elicited behaviour change when only short-term consequences of drinking were highlighted). Conversely, in a study replicating this trial with heavy drinking college students, but delivering the message via email, no main effects of message frame or temporal context (or an interaction between the two) were observed (Bernstein et al., Citation2016).
Framing studies that focus on manipulating the temporal proximity of outcomes are particularly pertinent to alcohol reduction interventions given that the most serious health risks associated with alcohol consumption often take years to accrue, during which time an individual may remain largely asymptomatic (Rehm & Shield, Citation2014). As a result, it has been argued that highlighting these future and probable health outcomes may not prove the most effective means to motivate immediate behaviour change given reliable evidence that individuals tend to engage in temporal discounting (reducing the value ascribed to more distant outcomes compared to immediate ones) (Beenstock, Adams, & White, Citation2011; Mckay et al., Citation2012; Story, Vlaev, Seymour, Darzi, & Dolan, Citation2014).
Trials exploring alternative ways to present messages to encourage reductions in alcohol consumption are therefore needed, with one potentially interesting avenue to explore being the impact of emphasising more proximal outcomes associated with drinking, including those that are not directly health-related (van der Pol, Hennessy, & Manns, Citation2017). This approach may help to overcome temporal discounting effects and enable an intervention message to retain greater motivational potency.
Existing message framing studies that have focussed on more immediate, non-health-related outcomes of alcohol intake have examined the extent to which presenting either emotional or social outcome expectancies prompt behaviour change (Agrawal & Duhachek, Citation2010; Dvorak, Pearson, Neighbors, & Martens, Citation2015; Kingsbury et al., Citation2014). One other more proximal outcome that has yet to be considered within the literature on alcohol consumption, however, is physical appearance. This represents an important omission given widespread recognition that excessive alcohol consumption not only has an immediate effect on mood and cognitive functioning (Eliasen et al., Citation2013; Foulds, Adamson, Boden, Williman, & Mulder, Citation2015; Mukherjee, Citation2013), but also on how one looks. The physical appearance effect of alcohol can result from possible short-term weight gain owing to the extra calories contained in alcohol, or to the fact that alcohol, as an organic solvent, exerts both a direct and indirect harmful influence on a large number of organs (Gr⊘nbaek, Citation2009; Inauen et al., Citation2017). This includes the skin, which can be directly and visibly affected by alcohol (Darvin, Sterry, Lademann, & Patzelt, Citation2013), as well as the impact of alcohol on appearance via its disrupting influence on sleep patterns (Ebrahim, Shapiro, Williams, & Fenwick, Citation2013).
To date, a few message framing studies emphasising physical appearance attributes have been conducted in the context of other health behaviours, with some success. For example, information on physical appearance has been manipulated to promote sun protection (Hevey et al., Citation2010; Thomas et al., Citation2011; Williams, Grogan, Clark-Carter, & Buckley, Citation2012), weight management (Frederick, Saguy, Sandhu, & Mann, Citation2015; Gallagher & Updegraff, Citation2011), and smoking cessation (Flett, Clark-Carter, Grogan, & Davey, Citation2013; Flett, Grogan, Clark-Carter, Gough, & Conner, Citation2015; Grogan et al., Citation2010).
While no evidence as yet exists to suggest that emphasising alcohol’s effect on physical appearance will encourage reductions in intake, recent research points towards appearance-related concerns as relevant in this context (Antin & Paschall, Citation2011; Holzhauer, Zenner, & Wulfert, Citation2016; Milward et al., Citation2016). This supposition is supported by an analysis of usage statistics from a smart phone application designed to support reductions in alcohol consumption, also developed by the Drinkaware Trust, which found that the second most common motivation for downloading and using the application to moderate drinking was related to physical appearance (e.g. to lose weight, cited by 30,924 (25.8%) of 119,713 users) (Attwood, Parke, Larsen, & Morton, Citation2017), and that levels of this motivation varied by gender (e.g. 19,415 female users versus 11,000 male users). This finding stands in support of limited evidence that the relationship between alcohol consumption and physical appearance concerns may differ by gender (Antin & Paschall, Citation2011; Barry & Piazza-Gardner, Citation2012).
Moreover, it can also be hypothesised that the effect of appearance focussed message frame may also be moderated by age, given that the types of outcome commonly highlighted in appearance-framed messages (e.g. wrinkles, weight gain) are likely to be more salient in older age groups who may already be more aware of physical appearance effects wrought by their lifestyle choices over time. Indeed, while we could find no single study that has explored whether age does in fact moderate the effect of appearance-framed messages in the context of alcohol consumption specifically, there is evidence to show age differences in response to other types of framed messages (e.g. gain versus loss) and alternative health behaviours such as physical activity (Mikels et al., Citation2016; Notthoff & Carstensen, Citation2014), suggesting that this is an important potential moderating variable to consider in relation to message framing effects.
One further variable that may also act as another moderator of any appearance-framed message effect on alcohol consumption (compared to a more traditional health-framed alternative) is the amount of alcohol an individual currently consumes. As recent research conducted by the Drinkaware Trust demonstrates, those with higher scores on the AUDIT-C (e.g. those who drink more) tend to also have greater pre-existing awareness of the impact of alcohol on their health (Gunstone, Piggot, Butler, Appleton, & Larsen, 2018) and are more likely than those with lower scores to actively want to reduce drinking for health reasons rather than to support an appearance-related goal such as losing weight (Attwood et al., Citation2017).
Objectives
Taken together, these findings have led us to hypothesise that selectively highlighting the proximal, appearance-related outcomes of alcohol consumption may influence the engagement of visitors to the Drinkaware website in a subsequent SBI. Moreover, we tentatively hypothesise that gender, age, and risk level may moderate the impact of appearance-framed messages on alcohol consumption-related behaviours, with the possibility of larger effects in female, older drinkers, and smaller effects in those at higher risk. The present study intends to explore these hypotheses directly, by answering the question of whether appearance framed versus health-framed web advertisements are more likely to engage visitors to the Drinkaware website to complete an online alcohol reduction SBI and to access further self-help resources to support a change to lower risk consumption behaviour. A second exploratory research question focussed on whether appearance-framed alcohol reduction messages were differentially effective at encouraging further SBI and further self-help resource uptake in men and women, across different age groups and in website visitors with different AUDIT-C risk levels.
Method
Trial design and participants
The study design was a randomised trial comparing two message frame variations. All visitors to the Drinkaware website during the 6-week trial period (November–December 2014) were exposed to a prominently placed banner advertisement emphasising either appearance (n = 51,588) or health-related (n = 52,639) outcomes of excess alcohol consumption and inviting them to complete an online SBI.
If visitors chose to click on this banner advertisement, they were immediately redirected to a cached, linked site; here, participants were exposed to a webpage containing congruently framed risk information and the first question of the AUDIT-C alcohol screening questionnaire.
If the full questionnaire was completed, visitors were then redirected to a linked webpage where they were presented with their AUDIT-C risk score and given further extended frame congruent health or appearance-related information. At the bottom of this webpage, participants were provided with four ‘further resource’ options which they could click on in order to access additional help and support to reduce alcohol consumption (e.g. 1. register for ‘My Drinkaware’ (an online alcohol consumption tracking tool), 2. order a unit measurement cup, 3. receive tips to cut down at home or 4. receive tips to cut down when out). Only the first resource accessed was recorded for each visitor.
Ethical approval and data protection
Ethical approval was obtained from Bristol University School of Economics, Finance and Management Research Ethics Committee in September 2014. The homepage contained a pop-up disclaimer notification to inform visitors that by using the website they consented to Drinkaware’ privacy and cookies policy and stating that their anonymous data may sometimes be used for research purposes (See supplementary file 1 for screen shot). An email address was included for interested individuals to contact the research team. All data were aggregated and no personally identifiable data were used in the analysis presented here. Drinkaware own the data entered by individuals who voluntarily access their website.
Intervention
Appearance and health-framed messages were developed by study authors and reviewed by the Department of Health’s alcohol team and by Drinkaware’s independent Medical Advisory Panel. Both banner advertisements contained the question ‘Are you drinking too much?’ followed either by ‘Is this affecting your health?’ or ‘Is this affecting your appearance?’. The aim of this banner advertisement was to engage and direct website visitors towards the AUDIT-C screening tool. The AUDIT-C is scored out of 12 and reflects both the frequency and amount of alcohol consumed (Public Health England, Citation2009). This tool shows similar accuracy to the full AUDIT questionnaire in detecting risky consumption levels and alcohol use disorders (Bowring, Gouillou, Hellard, & Dietze, Citation2013; Gómez, Conde, Santana, & Jorrín, Citation2005). For the present study, AUDIT-C scores were used to group participants into one of two risk categories (‘low risk’ or ‘increasing risk’) based on a classification system developed by Drinkaware.
Subsequent risk feedback and extended frame congruent messages then signposted visitors to the four further resources. To isolate the specific effect of the appearance versus health-framed content, we matched remaining message attributes as far as possible (e.g. message format, image type, outcome severity, number of outcomes and outcome time frame) (See supplementary file 2 for full intervention text).
Outcomes
The primary outcome was the proportion of website visitors in each trial arm who completed the AUDIT-C risk screening questionnaire. The secondary outcome was the proportion of users who accessed any of the four ‘further resource’ options available (only the first accessed option is recorded).
Exploratory sub-group analyses were also conducted to determine the impact of participant age (<18; 18–24; 25–34; 35–44; 45–64; 65–100 years), gender and risk score on completion of the AUDIT-C and accessing further resources. We could not conduct these analyses for those who clicked through but did not complete the AUDIT-C as it was only possible to gather information on age, gender and risk score of those who provided this information at the point of submitting this questionnaire. Google Analytics was used to track the number of people passing through the SBI. This was recorded in terms of events, rather than user journeys identifiable to a specific user, meaning that individuals could complete the AUDIT-C and access the resources multiple times, but they would have always seen the same version of the intervention each time if using the same web browser.
Sample size
Historical website use data indicated that, before the trial, 2.63% of home page views result in AUDIT-C completion. However, the link to the AUDIT-C from the homepage (where these data are derived) was much smaller and further down the page during the pre-trial period than during the trial period when it was placed in a more visually prominent position in a banner advertisement. As a result, our power calculation was informed by website data on the number of AUDIT-C completions resulting from website users landing from any route, including the Drinkaware homepage, but also directly from google searches and from other Drinkaware pages the user may have visited. This historical data indicated that there is approximately N = 88,000 visits to the Drinkaware homepage per month, and that N = 11,900 of website users started the AUDIT-C questionnaire during the pre-trial period (13.5%), with N = 7,500 (8.5%) of these users following this screening tool through to completion. Therefore, a two-arm randomised trial conducted over a two-month period, assuming 80% power and alpha of 5%, was estimated to be sufficiently powered to detect a mean shift in the primary outcome of 0.5 percentage points. This represents approximately a 450-person difference in the number of homepage visitors who complete the AUDIT-C questionnaire.
Randomisation
A randomisation sequence was generated using a Google algorithm. Allocation concealment was ensured given that generation of the randomisation sequence and intervention assignment was automatic at the time that a user first accessed the Drinkware website. Users were not identifiable by their Internet Protocol (IP) address, although this information was used to ensure that each user was only ever exposed to one message variant in the event of repeated visits (except in cases where users may have accessed the Drinkaware website from different browsers). It was not possible to blind users to intervention content given the nature of this trial. The statistician was not blinded to the allocation during analysis.
Statistical methods
All data were collated through Google Analytics and extracted into Microsoft Excel for processing. Website usage data were provided to study authors in aggregated form by Drinkaware, such that only the number of users in each category (for example, <18-year old/male/completed AUDIT-C/health-framed message, for example, which, if any further resources accessed) was known. These data were then expanded using STATA version 13 to create a dataset of the same scale as the trial, allowing each observation to represent an individual website visit. Categorical variables (such as age) were re-derived to give numerical variables suitable for analysis.
For the primary outcome (proportion of users to complete the AUDIT-C questionnaire), a binary logistic regression was conducted (). A similar analysis was conducted for the secondary outcome comparing the proportion of visitors who chose to access ‘further resources’ in each trial arm (). Finally, for the exploratory subgroup analysis, a series of chi-squared tests were conducted to examine whether the demographic make-up (e.g. gender, age or risk profile) of those who completed the AUDIT-C () or accessed further resources () differed between the two intervention arms.
Table 1. Binary logistic regression for AUDIT-C completion following exposure to health or appearance-framed message.
Table 2. Binary logistic regression for Further Resource accessed following exposure to health or appearance-framed message.
Table 3. Exploratory subgroup analysis of AUDIT-C completions.
Table 4. Exploratory subgroup analysis of accessing further resources.
Results
Participant flow
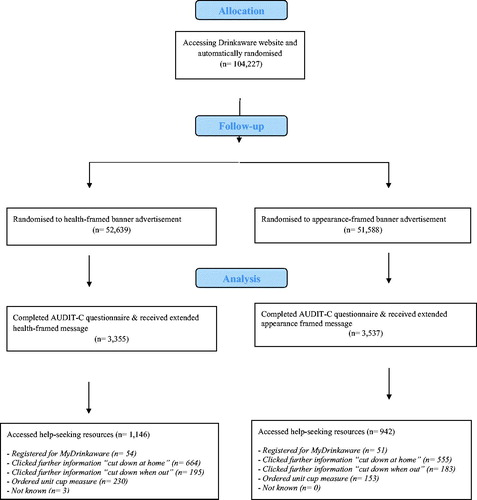
During the trial period, 104,227 visits were made to the Drinkaware homepage. provides details of participant flow through the trial. A total of 6,892 of those visits resulted in completion of the AUDIT-C (6.61%) and 2,088 (2.00%) accessed one or more of the four further resources available. Of those completing the AUDIT-C 30.3% went on to access further resources.
Figure 1. CONSORT flow diagram.
Primary outcome: AUDIT-C completions
shows the proportion of Drinkaware website visits that led to completion of the AUDIT-C questionnaire following exposure to either appearance or health-framed messages. As the results of the binary logistic regression analysis indicate, visits to the website were significantly more likely to lead to AUDIT-C completion if an appearance-framed message was displayed (odds ratio (OR) 1.08, 95% confidence interval (95% CI) 1.03 to 1.14, p = 0.002). This represents a difference of 182 visits resulting in completion of the AUDIT-C between intervention arms.
Secondary outcomes: accessing further resources
Approximately 30% (n = 2,088) of completed AUDIT-C visits resulted in access to further resources (). Appearance-framed messages were significantly less likely to result in access to further resources than health-framed messages (OR 0.70, 95% CI 0.63 to 0.78, p < 0.001) amongst those who completed AUDIT C. This represents 204 fewer occasions that further resource options were accessed between intervention arms.
Although health-framed messages (6.37%) were less likely to lead to AUDIT-C completion than appearance-framed messages (6.86%) see , these messages were more likely to result in access to further resources among website visits overall due to the larger effect size during the second part of the SBI: access to further resources was 2.18% (1,146/52,639) for the health-framed messages and 1.83% (942/51,588) for the appearance-framed messages (OR 1.20, 95% CI 1.10 to 1.31, p < 0.001).
Exploratory subgroup analysis: effects of age, gender and risk level on primary and secondary outcomes
Exploratory subgroup analyses were conducted to determine whether the effect of the message framing intervention on the primary (AUDIT-C completion) and secondary outcomes (accessing further resources) differed by age, gender and risk level. As noted in the methods section, details of age, gender and risk profile were collected on completion of the AUDIT-C (i.e. when visitors submitted their questionnaire responses for calculation), rather than at the point of randomisation into the study. Hence, we cannot determine the extent to which subgroup differences reported here reflect the intervention effect itself (i.e. one type of message frame favours women) as opposed to uneven exposure to intervention arms in the first instance (i.e. more women were originally exposed to one particular frame). Presuming our randomisation was robust, however, participant characteristics should be evenly spread between both intervention arms.
The influence of message frame type on AUDIT-C completions differed significantly by gender, age and risk level (). Our analyses show that more male than female users completed the AUDIT-C overall in both conditions, but a higher relative proportion of females completed the AUDIT-C when exposed to the appearance-framed message (49.9%) than the health-framed message (45.7%) (χ2 = 12.228, p < 0.001). For age, our subgroup analysis was once again significant (χ2 = 15.3852, p = 0.009), indicating an interaction between age and message frame type. For both frame types, more users aged between 45 and 64 years completed the AUDIT-C compared to all other age groups. Our analyses suggests that the appearance-framed message led to a higher relative proportion of users completing the AUDIT-C in those aged over 35 (e.g. ‘older’ users), whereas the health-framed messages led to a higher relative proportion of completions in those aged 34 and under (e.g. ‘younger’ users). The chi-squared test statistic was also significant for the subgroup analysis by risk level (χ2 = 8.553, p = 0.003). Here, those at high risk of alcohol-related harms were far more likely to complete the AUDIT-C than those at lower risk for both frame types, with the appearance frame leading to a marginally greater proportion of completions in higher risk drinkers (89.1%) than the health-framed message (86.9%).
The influence of message frame type on our secondary outcome of numbers accessing further resources also differed significantly by gender and age, but not by AUDIT-C risk level (). For gender, results from our chi-squared tests for this secondary outcome showed a higher proportion of visitors coming from the health-framed condition and accessing further resources were women (52.5% female versus 47.2% male). Conversely, a higher proportion of men who accessed further resources had originally seen the appearance-framed information (46% female versus 54% male) (χ2 = 9.546, p < 0.002). These findings are the converse of our primary outcome subgroup analysis stated above. Additionally, for age, we also find a significant interaction effect between age and frame type (χ2 = 21.58, p < 0.00), with the pattern of effect differing from the primary outcome subgroup analysis given above. This time, appearance-framed messages led to a higher relative proportion of completions in those aged 34 and under, as well as in those aged 65+ (‘younger’ users and the ‘oldest’ age group), while the health-framed message led a high proportion of users accessing further resources in the 35–64 year age groups (e.g. the ‘older’ group). Finally, for risk level, the result of our chi-squared test was not statistically significant, suggesting no differential effect of message frame type by the degree of user risk of alcohol-related harms (χ2 = 0.743, p < 0.38).
Discussion
Main findings
This randomised trial examined whether a novel approach to message framing, namely highlighting short-term appearance-related outcomes of excessive alcohol consumption, would be more effective in engaging website visitors to an online SBI than a more traditional approach emphasising longer term health risks. We observed a small effect of frame type, with visits to the website more likely to result in completion of the screening component of an SBI following exposure to an appearance-framed message.
Once engaged in the intervention, around a third of website visitors went on to complete the SBI. At this stage, we found that exposure to messages highlighting health-related outcomes increased the likelihood that further resource options to help facilitate risk-reducing behaviour change were accessed. Although we acknowledge that examining further resource click rates is not necessarily a valid proxy indicator of either intentions to change drinking behaviour or of change itself, the findings that people do access these resources after receiving their AUDIT C score suggests opportunity for future intervention research specifically designed for individuals wishing to receive immediate support for their drinking at the time of internet access. These ‘just-in-time adaptive interventions’ deliver content based on relevant situational cues and have already proven useful for community support in individuals leaving residential treatment for alcohol use disorder (e.g. Gustafson et al., Citation2014; Nahum-Shani et al., Citation2018). This work may be further informed by existing qualitative research that has identified unique drivers and consequences of drinking patterns within the home specifically (Brierley-Jones et al., Citation2014; Foster, Citation2013).
Results of subgroup analyses, while purely exploratory, imply that appearance-framed messages encouraged more AUDIT C completions in older, female drinkers, supporting our original hypotheses. However, in contrast to our original hypothesis, appearance-framed messages were also found to lead to greater engagement in users with higher AUDIT C risk scores, a group we originally believed would be more responsive to health-framed information. Moreover, further exploratory subgroup analyses with users who accessed further resources (our secondary outcome) following exposure to appearance-framed messaging found that these messages led to greater engagement in male users, those who were either younger (34 years or under) or over 65, and that no differential effects were observed by risk level.
Explanation for the findings
Our main finding is that physical appearance-framed messages increase the likelihood of website users completing an online SBI, whereas health-framed messages increase the likelihood that users will go on to access further behaviour change support resources. This leads us to ask the question – why would appearance-related messages enhance screening uptake, but health messages prompt action? Before the screening test, our messages are rather abstract statements about health (irritable bowel syndrome, cancer and liver disease) and appearance (saggy skin, obesity and premature ageing). Given that people may be more immediately concerned about their image rather than their health (Gerrard, Gibbons, Lane, & Stock, Citation2005; Mahler, Kulik, Gibbons, Gerrard, & Harrell, Citation2003), it is perhaps not surprising that appearance-related messages prove more influential at this earlier stage. However, after the screening test, recipients went on to receive more specific and contextualised information about the likely outcomes of their behvaiour via extended appearance and health-framed messages. Here, the health consequences of alcohol consumption (e.g. bowel cancer, depression and anxiety, osteoporosis) are much more severe, in terms of averseness of experience and levels of threat for the survival of the organism, compared to the consequences for appearance (grey-saggy-dehydrated skin, premature ageing of the skin, poor fitness due to burning less fat and less effective gym sessions). We speculate, therefore, that health messages may be more effective in influencing action at this stage when users may be more engaged in the topic at hand (e.g. imminent pain and death are, and should be, more motivating than physical unattractiveness) (see Jessop, Albery, Rutter, & Garrod, Citation2008 for research on the impact of mortality-related health-risk information and Hayes, Schimel, Arndt, & Faucher, Citation2010 for evidence about the impact of accessibility of thoughts about death).
Although exploratory analysis only, it appears that the main effect of appearance on AUDIT C completions is driven by older, female, drinkers consuming alcohol at levels damaging to their health. This indicates that appearance-framed messages hold some promise for selective engagement of emergent high-risk demographic groups (e.g. older, females). We could speculate that this finding might be attributed to the novelty of those messages, especially for those populations who are likely to already have been exposed to information on health risks. Conversely, we found that visitors accessing further resources were more likely to either fall into younger age groups or the oldest age group, and to be male. It is perhaps the case that the appearance-framed message initially attracted more females, who may be more interested to read and learn about novel appearance-related facts given higher levels of social motivation and enjoyment in seeking out this type of information compared to men (Bidmon & Terlutter, Citation2015), but that those females who access the website because they are explicitly concerned about their health, and want to take action, are more likely to do so when viewing health information which confirms their concerns. Caution is required when interpreting these exploratory subgroup analyses, however, given that information on demographic characteristics was collected after completion of the AUDIT-C. Further research exploring appearance-related message frames across different age groups is therefore warranted to help us determine with greater certainty whether the age, gender and risk subgroup effects outlined here are replicable, and to understand whether tailoring appearance-framed messages to the specific concerns of an age, gender or risk level group enhances their effect.
Strengths and limitations
This study presents a novel finding that emphasising the appearance-related outcomes of alcohol consumption can enhance engagement in a risk-reducing brief intervention. This outcome thus supports evidence garnered in other health behaviour domains, that physical appearance concerns do play an important role in health-related decision-making (Flett et al., Citation2013; Gallagher & Updegraff, Citation2011; Grogan, Fry, Gough, & Conner, Citation2011; Thomas et al., Citation2011).
The fact that this was a web-based intervention employing automatic randomisation and tracking visitors through the Drinkaware website did however limit the extent to which validated, but potentially burdensome, additional behavioural outcome measures were taken. Our analysis of routinely collected data did, however, allow for a very large sample to be studied, thereby enhancing our power to detect significant between-group (as well as subgroup) differences in effect and ensuring ecological validity. However, we do clearly acknowledge that it was not possible to verify the extent to which our outcome measures reflect either intentions to change alcohol consumption or consumption itself. To draw firmer conclusions, experimental replication using validated measures of alcohol intake is required. We also acknowledge that with a small effect size and large sample, the findings of this study could be attributed to Type 1 error, and recommend that others endeavour to conduct future research that attempts to replicate this study.
One further limitation of this work pertains to the fact that demographic details of website visitors were only ascertained on completion of the AUDIT-C questionnaire. We do not therefore know the extent to which our randomisation procedure was effective in evenly distributing demographic characteristics across intervention arms (e.g. more female or high-risk drinkers may have been exposed to appearance-framed messages to start with). That we were unable to explore subgroup differences in the frequency of further resource options accessed between intervention arms also means that no conclusions could be drawn here as to whether one message frame variant is more likely to prompt either men or women, or lower or higher risk drinkers, to risk-reducing action.
Implications
The findings of the present study suggest that others wishing to recruit web-users into online SBIs may engage larger numbers if physical appearance-related outcomes of excessive alcohol consumption are highlighted in advertisements and other communications. We do however caution that this may not be the most effective strategy to ensure behaviour change. In addition, care also needs to be taken to ensure that any possible adverse effects of this message framing approach are avoided. For example, dissatisfaction with the physical attribute of body weight has previously been associated with an increased likelihood of binge drinking (Antin & Paschall, Citation2011; Barry & Piazza-Gardner, Citation2012), implying that physical appearance information may in some cases lead to increases in risky consumption.
Conclusion
This study compared the impact of appearance versus health-framed messages on engagements in a brief web-based risk screening and alcohol reduction intervention developed by UK-based alcohol awareness charity Drinkaware. This study presents a novel finding that framing the outcomes of excessive alcohol consumption in terms of effect the on physical appearance increased engagement with an SBI whereas highlighting the health risks associated with alcohol consumption increased uptake of further resources. This highlights the potential for use of multi-level approaches in alcohol reduction interventions.
Acknowledgements
We would like to thank the Drinkaware team for supporting the research project. Anastasia Terzeon was the person originally coordinating Drinkaware involvement as the project was being set up. Ben Butler was overseeing and technical website design requirements. Ellie Mann and Jessica Miller were communicating and directing the implementation of the website designs which were undertaken by an external website agency.
Disclosure statement
Drinkaware is primarily funded by voluntary and unrestricted donations from UK alcohol producers, retailers and supermarkets, based on an agreement between the UK government and the alcohol industry. The funders of Drinkaware have no involvement in or influence over the activities of the charity which is governed by an independent Board of trustees. Drinkaware works with an independent panel of expert medical advisors who review all medical content for accuracy and ensure that it is based on the most current evidence. The panel is chaired by the Chief Medical Advisor who reports independently to Drinkaware's Board of Trustees.
Data availability
Data is available here https://www.drinkaware.co.uk/research/our-research-and-evaluation-reports/appearance-versus-health-messages-test/.
References
- Agrawal, N., & Duhachek, A. (2010). Emotional compatibility and the effectiveness of antidrinking messages: A defensive processing perspective on shame and guilt. Journal of Marketing Research, 47(2), 263–273. doi:10.1509/jmkr.47.2.263
- Anderson, P., Bendtsen, P., Spak, F., Reynolds, J., Drummond, C., Segura, L., … Gual, T. (2016). Improving the delivery of brief interventions for heavy drinking in primary health care: outcome results of the Optimizing Delivery of Health Care Intervention (ODHIN) five-country cluster randomized factorial trial. Addiction, 111(11), 1935–1945. doi:10.1111/add.13476
- Anderson, P., Wojnar, M., Jakubczyk, A., Gual, A., Reynolds, J., Segura, L., … Kolsek, M. (2014). Managing alcohol problems in general practice in Europe: Results from the European ODHIN survey of general practitioners. Alcohol and Alcoholism, 49(5), 531–539. Retrieved from doi:10.1093/alcalc/agu043
- Andrade, A. L. M., de Lacerda, R. B., Gomide, H. P., Ronzani, T. M., Sartes, L. M. A., Martins, L. F., … Schaub, M. P. (2016). Web-based self-help intervention reduces alcohol consumption in both heavy-drinking and dependent alcohol users: A pilot study. Addictive Behaviors, 63, 63–71. doi:10.1016/j.addbeh.2016.06.027
- Antin, T. M. J., & Paschall, M. J. (2011). Weight perception, weight change intentions, and alcohol use among young adults. Body Image, 8(2), 149–156. doi:10.1016/j.bodyim.2011.01.002
- Attwood, S., Parke, H., Larsen, J., & Morton, K. L. (2017). Using a mobile health application to reduce alcohol consumption: A mixed-methods evaluation of the drinkaware track & calculate units application. BMC Public Health, 17(1), 394. https://doi.org/10.1186/s12889-017-4358-9
- Barry, A. E., & Piazza-Gardner, A. K. (2012). Drunkorexia: Understanding the co-occurrence of alcohol consumption and eating/exercise weight management behaviors. Journal of American College Health, 60(3), 236–243. doi:10.1080/07448481.2011.587487
- Beenstock, J., Adams, J., & White, M. (2011). The association between time perspective and alcohol consumption in university students: Cross-sectional study. European Journal of Public Health, 21(4), 438–443. Retrieved from doi:10.1093/eurpub/ckp225
- Bernstein, M. H., Wood, M. D., & Erickson, L. R. (2016). The effectiveness of message framing and temporal context on college student alcohol use and problems: A selective e-mail intervention. Alcohol and Alcoholism, 51(1), 106–116. Retrieved from doi:10.1093/alcalc/agv091
- Bidmon, S., & Terlutter, R. (2015). Gender differences in searching for health information on the internet and the virtual patient-physician relationship in Germany: Exploratory results on how men and women differ and why. Journal of Medical Internet Research, 17(6), e156. doi:10.2196/jmir.4127
- Bowring, A. L., Gouillou, M., Hellard, M., & Dietze, P. (2013). Comparing short versions of the AUDIT in a community-based survey of young people. BMC Public Health, 13(1), 301. https://doi.org/10.1186/1471-2458-13-301
- Brierley-Jones, L., Ling, J., McCabe, K. E., Wilson, G. B., Crosland, A., Kaner, E. F. S., & Haighton, C. A. (2014). Habitus of home and traditional drinking: A qualitative analysis of reported middle-class alcohol use. Sociology of Health & Illness, 36(7), 1054–1076. doi:10.1111/1467-9566.12145
- Britton, A., Ben-Shlomo, Y., Benzeval, M., Kuh, D., & Bell, S. (2015). Life course trajectories of alcohol consumption in the United Kingdom using longitudinal data from nine cohort studies. BMC Medicine, 13(1), 47. https://doi.org/10.1186/s12916-015-0273-z
- Brown, J., West, R., Angus, C., Beard, E., Brennan, A., Drummond, C., … Michie, S. (2016). Comparison of brief interventions in primary care on smoking and excessive alcohol consumption: a population survey in England. British Journal of General Practice, 66(642), e1 LP–e9. Retrieved from http://bjgp.org/content/66/642/e1.abstract doi:10.3399/bjgp16X683149
- Darvin, M. E., Sterry, W., Lademann, J., & Patzelt, A. (2013). Alcohol consumption decreases the protection efficiency of the antioxidant network and increases the risk of sunburn in human skin. Skin Pharmacology and Physiology, 26(1), 45–51. doi:10.1159/000343908
- de Graaf, A., van den Putte, B., & de Bruijn, G.-J. (2015). Effects of issue involvement and framing of a responsible drinking message on attitudes, intentions, and behavior. Journal of Health Communication, 20(8), 989–994. doi:10.1080/10810730.2015.1018623
- Department of Health. (2015). UK Chief Medical Officers’ Alcohol Guidelines Review. Summary of the Proposed New Guidelines. Retrieved from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/489795/summary.pdf
- Dulin, P. L., Gonzalez, V. M., & Campbell, K. (2014). Results of a pilot test of a self-administered smartphone-based treatment system for alcohol use disorders: Usability and early outcomes. Substance Abuse, 35(2), 168–175. doi:10.1080/08897077.2013.821437
- Dvorak, R. D., Pearson, M. R., Neighbors, C., & Martens, M. P. (2015). Fitting in and standing out: increasing the use of alcohol protective behavioral strategies with a deviance regulation intervention. Journal of Consulting and Clinical Psychology, 83(3), 482–493. doi:10.1037/a0038902
- Ebrahim, I. O., Shapiro, C. M., Williams, A. J., & Fenwick, P. B. (2013). Alcohol and Sleep I: Effects on normal sleep. Alcoholism: Clinical and Experimental Research, 37(4), 539–549. doi:10.1111/acer.12006
- Eliasen, M., Rod, M. H., Flensborg-Madsen, T., Petersen, J. H., Gr⊘nbaek, M., & Tolstrup, J. S. (2013). The association between blood alcohol content and cheerfulness, focus distraction, and sluggishness among young adults attending high school parties. Alcoholism: Clinical and Experimental Research, 38(3), 826–833. doi:10.1111/acer.12268
- Flett, K., Clark-Carter, D., Grogan, S., & Davey, R. (2013). How effective are physical appearance interventions in changing smoking perceptions, attitudes and behaviours? A systematic review. Tobacco Control, 22(2), 74 LP–79. Retrieved from http://tobaccocontrol.bmj.com/content/22/2/74.abstract doi:10.1136/tobaccocontrol-2011-050236
- Flett, K., Grogan, S., Clark-Carter, D., Gough, B., & Conner, M. (2015). Male smokers’ experiences of an appearance-focused facial-ageing intervention. Journal of Health Psychology, 22(4), 422–433. doi:10.1177/1359105315603477
- Foster, J., & Heyman, B. (2013). Drinking alcohol at home and in public places and the time framing of risks. Health Risk & Society, 15(6-07).https://doi.org/10.1080/13698575.2013.839779
- Foulds, J. A., Adamson, S. J., Boden, J. M., Williman, J. A., & Mulder, R. T. (2015). Depression in patients with alcohol use disorders: Systematic review and meta-analysis of outcomes for independent and substance-induced disorders. Journal of Affective Disorders, 185, 47–59. https://doi.org/https://doi.org/10.1016/j.jad.2015.06.024 doi:10.1016/j.jad.2015.06.024
- Frederick, D. A., Saguy, A. C., Sandhu, G., & Mann, T. (2015). Effects of competing news media frames of weight on antifat stigma, beliefs about weight and support for obesity-related public policies. International Journal of Obesity, 40, 543. Retrieved from doi:10.1038/ijo.2015.195
- Fujii, H., Nishimoto, N., Yamaguchi, S., Kurai, O., Miyano, M., Ueda, W., … Okawa, K. (2016). The Alcohol Use Disorders Identification Test for Consumption (AUDIT-C) is more useful than pre-existing laboratory tests for predicting hazardous drinking: a cross-sectional study. BMC Public Health, 16(1), 379. https://doi.org/10.1186/s12889-016-3053-6
- Gallagher, K. M., & Updegraff, J. A. (2011). When ‘fit’ leads to fit, and when ‘fit’ leads to fat: How message framing and intrinsic vs. extrinsic exercise outcomes interact in promoting physical activity. Psychology & Health, 26(7), 819–834. doi:10.1080/08870446.2010.505983
- Gerend, M. A., & Cullen, M. (2008). Effects of message framing and temporal context on college student drinking behavior. Journal of Experimental Social Psychology, 44(4), 1167–1173. https://doi.org/https://doi.org/10.1016/j.jesp.2008.02.007 doi:10.1016/j.jesp.2008.02.007
- Gerrard, M., Gibbons, F. X., Lane, D. J., & Stock, M. L. (2005). Smoking cessation: Social comparison level predicts success for adult smokers. Health Psychology. https://doi.org/10.1037/0278-6133.24.6.623
- Gómez, A., Conde, A., Santana, J. M., & Jorrín, A. (2005). Diagnostic usefulness of brief versions of Alcohol Use Disorders Identification Test (AUDIT) for detecting hazardous drinkers in primary care settings. Journal of Studies on Alcohol, 66(2), 305–308. doi:10.15288/jsa.2005.66.305
- Gonzalez, V. M., & Dulin, P. L. (2015). Comparison of a smartphone app for alcohol use disorders with an Internet-based intervention plus bibliotherapy: A pilot study. Journal of Consulting and Clinical Psychology, 83(2), 335–345. doi:10.1037/a0038620
- Grogan, S., Flett, K., Clark-Carter, D., Gough, B., Davey, R., Richardson, D., & Rajaratnam, G. (2010). Women smokers’ experiences of an age-appearance anti-smoking intervention: A qualitative study. British Journal of Health Psychology, 16(4), 675–689. doi:10.1348/2044-8287.002006
- Grogan, S., Fry, G., Gough, B., & Conner, M. (2011). Smoking to stay thin or giving up to save face? Young men and women talk about appearance concerns and smoking. British Journal of Health Psychology, 14(1), 175–186. doi:10.1348/135910708X327617
- Gr⊘nbaek, M. (2009). The positive and negative health effects of alcohol- and the public health implications. Journal of Internal Medicine, 265(4), 407–420. doi:10.1111/j.1365-2796.2009.02082.x
- Gunstone, B., Piggot, L., Butler, B., Appleton, A., & Larson, J. (2018). Drinkaware Monitor 2018: Drinking behaviour and moderation, 86. Retrieved from https://www.drinkaware.co.uk/research/our-research-and-evaluation-reports/drinkaware-monitor-2018-drinking-behaviour-and-moderation/
- Gustafson, D., McTavish, F., Chih, M., & etal. (2014). A smartphone application to support recovery from alcoholism: A randomized clinical trial. JAMA Psychiatry, 71(5), 566–572. Retrieved from doi:10.1001/jamapsychiatry.2013.4642
- Haighton, C., Wilson, G., Ling, J., McCabe, K., Crosland, A., & Kaner, E. (2016). A qualitative study of service provision for alcohol related health issues in mid to later life. PloS One, 11(2), e0148601. doi:10.1371/journal.pone.0148601
- Harrington, N. G., & Kerr, A. M. (2017). Rethinking risk: Prospect theory application in health message framing research. Health Communication, 32(2), 131–141. doi:10.1080/10410236.2015.1110004
- Hayes, J., Schimel, J., Arndt, J., & Faucher, E. H. (2010). A theoretical and empirical review of the death-thought accessibility concept in terror management research. Psychological Bulletin. https://doi.org/10.1037/a0020524
- Healey, C., Rahman, A., Faizal, M., & Kinderman, P. (2014). Underage drinking in the UK: Changing trends, impact and interventions. A rapid evidence synthesis. International Journal of Drug Policy, 25(1), 124–132. https://doi.org/https://doi.org/10.1016/j.drugpo.2013.07.008 doi:10.1016/j.drugpo.2013.07.008
- Hevey, D., Pertl, M., Thomas, K., Maher, L., Craig, A., & Ni Chuinneagain, S. (2010). Body consciousness moderates the effect of message framing on intentions to use sunscreen. Journal of Health Psychology, 15(4), 553–559. doi:10.1177/1359105309355335
- Holzhauer, C. G., Zenner, A., & Wulfert, E. (2016). Poor body image and alcohol use in women. Psychology of Addictive Behaviors. https://doi.org/10.1037/adb0000115
- Hutter, R. R. C., Lawton, R., Pals, E., O’Connor, D. B., & McEachan, R. R. C. (2014). Tackling student binge drinking: Pairing incongruent messages and measures reduces alcohol consumption. British Journal of Health Psychology, 20(3), 498–513. doi:10.1111/bjhp.12111
- Inauen, J., Bolger, N., Shrout, P. E., Stadler, G., Amrein, M., Rackow, P., & Scholz, U. (2017). Using smartphone-based support groups to promote healthy eating in daily life: A randomised trial. Applied Psychology: Health and Well-Being. https://doi.org/10.1111/aphw.12093
- Institute of Alcohol Studies. (2016). Why are women drinking more? Retrieved from http://www.ias.org.uk/Alcohol-knowledge-centre/Alcohol-and-women/Factsheets/Why-are-women-drinking-more.aspx
- Jessop, D. C., Albery, I. P., Rutter, J., & Garrod, H. (2008). Understanding the impact of mortality-related health-risk information: A terror management theory perspective. Personality and Social Psychology Bulletin, 34(7), 951–964. doi:10.1177/0146167208316790
- Johnson, N. A., Kypri, K., & Attia, J. (2013). Development of an electronic alcohol screening and brief intervention program for hospital outpatients with unhealthy alcohol use. JMIR Research Protocol, 2(2), e36. doi:10.2196/resprot.2697
- Kaner, E., Bland, M., Cassidy, P., Coulton, S., Dale, V., Deluca, P., … Drummond, C. (2013). Effectiveness of screening and brief alcohol intervention in primary care (SIPS trial): Pragmatic cluster randomised controlled trial. BMJ: British Medical Journal, 346. Retrieved from http://www.bmj.com/content/346/bmj.e8501.abstract doi:10.1136/bmj.e8501
- Kaner, E. F., Beyer, F. R., Muirhead, C., Campbell, F., Pienaar, E. D., Bertholet, N., … Burnand, B. (2018). Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database of Systematic Reviews, 2. https://doi.org/10.1002/14651858.CD004148.pub4
- Khadjesari, Z., Newbury-Birch, D., Murray, E., Shenker, D., Marston, L., & Kaner, E. (2015a). Online health check for reducing alcohol intake among employees: A feasibility study in six workplaces across England. PLoS One, 10(3), e0121174. Retrieved from doi:10.1371/journal.pone.0121174
- Khadjesari, Z., Stevenson, F., Godfrey, C., & Murray, E. (2015b). Negotiating the ‘grey area between normal social drinking and being a smelly tramp’: A qualitative study of people searching for help online to reduce their drinking. Health Expectations, 18(6), 2011–2020. doi:10.1111/hex.12351
- Kingsbury, J. H., Gibbons, F. X., & Gerrard, M. (2014). The effects of social and health consequence framing on heavy drinking intentions among college students. British Journal of Health Psychology, 20(1), 212–220. doi:10.1111/bjhp.12100
- Larsson, K., & Nehlin, C. (2016). Screening accuracy of brief alcohol screening instruments in a general hospital setting. Scandinavian Journal of Public Health, 44(6), 599–603. doi:10.1177/1403494816651779
- Lewer, D., Meier, P., Beard, E., Boniface, S., & Kaner, E. (2016). Unravelling the alcohol harm paradox: a population-based study of social gradients across very heavy drinking thresholds. BMC Public Health, 16(1), 599. https://doi.org/10.1186/s12889-016-3265-9
- Mahler, H. I. M., Kulik, J. A., Gibbons, F. X., Gerrard, M., & Harrell, J. (2003). Effects of appearance-based intervention on sun protection intentions and self-reported behaviors. Health Psychology. https://doi.org/10.1037/0278-6133.22.2.199
- McCabe, K. E., Ling, J., Wilson, G. B., Crosland, A., Kaner, E. F. S., & Haighton, C. A. (2015). Alcohol service provision for older people in an area experiencing high alcohol use and health inequalities. Perspectives in Public Health, 136(2), 83–85. doi:10.1177/1757913915597259
- Mckay, M. T., Ballantyne, N., Goudie, A. J., Sumnall, H. R., & Cole, J. C. (2012). “Here for a good time, not a long time”: Decision-making, future consequences and alcohol use among Northern Irish adolescents. Journal of Substance Use, 17(1), 1–18. doi:10.3109/14659891.2011.559566
- Meneses-Gaya, C., Zuardi, A. W., Loureiro, S. R., Hallak, J. E. C., Trzesniak, C., De Azevedo Marques, J. M., … Crippa, J. A. S. (2010). Is the full version of the AUDIT really necessary? Study of the validity and internal construct of its abbreviated versions. Alcoholism: Clinical and Experimental Research, 34(8), 1417–1424. https://doi.org/10.1111/j.1530-0277.2010.01225.x
- Meng, Y., Holmes, J., Hill-McManus, D., Brennan, A., & Meier, P. S. (2013). Trend analysis and modelling of gender-specific age, period and birth cohort effects on alcohol abstention and consumption level for drinkers in Great Britain using the General Lifestyle Survey 1984–2009. Addiction, 109(2), 206–215. doi:10.1111/add.12330
- Mikels, J. A., Shuster, M. M., Thai, S. T., Smith-Ray, R., Waugh, C. E., Roth, K., … Stine-Morrow, E. A. L. (2016). Messages that matter: Age differences in affective responses to framed health messages. Psychology and Aging, 31(4), 409–414. doi:10.1037/pag0000040
- Milward, J., Khadjesari, Z., Fincham-Campbell, S., Deluca, P., Watson, R., & Drummond, C. (2016). User preferences for content, features, and style for an app to reduce harmful drinking in young adults: Analysis of user feedback in app stores and focus group interviews. JMIR MHealth UHealth, 4(2), e47. doi:10.2196/mhealth.5242
- Mukherjee, S. (2013). Alcoholism and its effects on the central nervous system. Current Neurovascular Research. https://doi.org/http://dx.doi.org/10.2174/15672026113109990004
- Murray, E., Khadjesari, Z., Linke, S., Hunter, R., & Freemantle, N. (2013). Health on the web: randomised trial of work-based online screening and brief intervention for hazardous and harmful drinking. BMC Public Health, 13(1), 505. https://doi.org/10.1186/1471-2458-13-505
- Nahum-Shani, I., Smith, S. N., Spring, B. J., Collins, L. M., Witkiewitz, K., Tewari, A., & Murphy, S. A. (2018). Just-in-time adaptive interventions (JITAIs) in mobile health: Key components and design principles for ongoing health behavior support. Annals of Behavioral Medicine, 52(6), 446–462. Retrieved from doi:10.1007/s12160-016-9830-8
- NHS Digital. (2016). Health Survey for England, 2016. Retrieved from https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/health-survey-for-england-2016
- Notthoff, N., & Carstensen, L. L. (2014). Positive messaging promotes walking in older adults. Psychology and Aging, 29(2), 329–341. doi:10.1037/a0036748
- O’Donnell, A., Anderson, P., Newbury-Birch, D., Schulte, B., Schmidt, C., Reimer, J., & Kaner, E. (2014a). The impact of brief alcohol interventions in primary healthcare: A systematic review of reviews. Alcohol and Alcoholism, 49(1), 66–78. Retrieved from doi:10.1093/alcalc/agt170
- O’Donnell, A., Wallace, P., & Kaner, E. (2014b). From efficacy to effectiveness and beyond: what next for brief interventions in primary care? Frontiers in Psychiatry, 5, 113. doi:10.3389/fpsyt.2014.00113
- Public Health England. (2009). Alcohol use screening tests. Retrieved from https://www.gov.uk/government/publications/alcohol-use-screening-tests
- Rehm, J., & Shield, K. D. (2014). Global alcohol-attributable deaths from cancer, liver cirrhosis, and injury in 2010. Alcohol Research: Current Reviews, 35(2), 174–183. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/24881325
- Riper, H., Blankers, M., Hadiwijaya, H., Cunningham, J., Clarke, S., Wiers, R., … Cuijpers, P. (2014). Effectiveness of guided and unguided low-intensity internet interventions for adult alcohol misuse: A meta-analysis. PLoS One, 9(6), e99912. Retrieved from doi:10.1371/journal.pone.0099912
- Rothman, A. J., & Salovey, P. (1997). Shaping perceptions to motivate healthy behavior: The role of message framing. Psychological Bulletin. 121(1), 3–19. doi:10.1037/0033-2909.121.1.3
- Scott, S., & Kaner, E. (2014). Alcohol and public health: Heavy drinking is a heavy price to pay for populations. Journal of Public Health, 36(3), 396–398. Retrieved from doi:10.1093/pubmed/fdu071
- Sinadinovic, K., Wennberg, P., Johansson, M., & Berman, A. H. (2014). Targeting individuals with problematic alcohol use via web-based cognitive-behavioral self-help modules, personalized screening feedback or assessment only: A randomized controlled trial. European Addiction Research, 20(6), 305–318. doi:10.1159/000362406
- Smith, L, F. D. (2009). Drinking in the UK: An exploration of trendstle. Retrieved from https://www.jrf.org.uk/report/drinking-uk-exploration-trends
- Story, G., Vlaev, I., Seymour, B., Darzi, A., & Dolan, R. (2014). Does temporal discounting explain unhealthy behavior? A systematic review and reinforcement learning perspective. Frontiers in Behavioral Neuroscience. Retrieved from https://www.frontiersin.org/article/10.3389/fnbeh.2014.00076
- Taylor, M. J., Vlaev, I., Maltby, J., Brown, G. D. A., & Wood, A. M. (2015). Improving social norms interventions: Rank-framing increases excessive alcohol drinkers’ information-seeking. Health Psychology. https://doi.org/10.1037/hea0000237
- Thomas, K., Hevey, D., Pertl, M., Ní Chuinneagáin, S., Craig, A., & Maher, L. (2011). Appearance matters: The frame and focus of health messages influences beliefs about skin cancer. British Journal of Health Psychology, 16(2), 418–429. doi:10.1348/135910710X520088
- van der Pol, M., Hennessy, D., & Manns, B. (2017). The role of time and risk preferences in adherence to physician advice on health behavior change. The European Journal of Health Economics, 18(3), 373–386. doi:10.1007/s10198-016-0800-7
- Williams, A. L., Grogan, S., Clark-Carter, D., & Buckley, E. (2012). Appearance-based interventions to reduce ultraviolet exposure and/or increase sun protection intentions and behaviours: A systematic review and meta-analyses. British Journal of Health Psychology, 18(1), 182–217. doi:10.1111/j.2044-8287.2012.02089.x