
ABSTRACT
Most deaf children have hearing parents who do not know a sign language at birth and are at risk of limited language input during early childhood. Studying these children as they learn a sign language has revealed that timing of first-language exposure critically shapes language outcomes. But the input deaf children receive in their first language is not only delayed, it is much more variable than most first language learners, as many learn their first language from parents who are themselves new sign language learners. Much of the research on deaf children learning a sign language has considered the role of parent input using broad strokes, categorizing hearing parents as non-native, poor signers, and deaf parents as native, strong signers. In this study, we deconstruct these categories and examine how variation in sign language skills among hearing parents might affect children’s vocabulary acquisition. This study included 44 deaf children between 8- and 60-months-old who were learning American Sign Language (ASL) and had hearing parents who were also learning ASL. We observed an interactive effect of parent ASL proficiency and age, such that parent ASL proficiency was a significant predictor of child ASL vocabulary size, but not among the infants and toddlers. The proficiency of language models can affect acquisition above and beyond age of acquisition, particularly as children grow. At the same time, the most skilled parents in this sample were not as fluent as “native” deaf signers, and yet their children reliably had age-expected ASL vocabularies. Data and reproducible analyses are available at https://osf.io/9ya6h/.
1. Introduction
Language input from parents and caregivers is a key determinant of child language acquisition. Among hearing children, variations in the amount of language children are exposed to and in the proficiency of their language models is directly tied to children’s later language outcomes (Huttenlocher et al. Citation1991, Rowe Citation2012, Weisleder & Fernald Citation2013). Among deaf children, the amount of variation in the input from caregivers is orders of magnitude larger. While some deaf children have unfettered access to one or more languages from birth, most deafFootnote1 children do not have complete access to the sounds of speech, and most have parents who are hearing and do not know a sign language at the time of the deaf child’s birth. Thus, many deaf children have limited access to language input, signed or spoken, during early childhood.
Sign language input to deaf children has typically been characterized as either “native,” from deaf, signing parents, or “non-native,” from hearing parents who did not previously know a sign language. In the literature, children with hearing parents are often assumed to have no sign language exposure until school entry. This characterization overlooks the subset of deaf children who have hearing parents who learn and use a naturally-evolved sign languageFootnote2 with their children, as is often recommended by advocates of early sign exposure (Napoli et al. Citation2015). These parents are non-native language models for their deaf children, yet their efficacy as language models is poorly understood. In this paper, we examine how parent sign language skills relate to their deaf children’s vocabulary acquisition. Understanding language acquisition among deaf children with hearing parents learning sign language is important for both practical reasons, like guiding parents and professionals regarding best practices in supporting language acquisition, and theoretical reasons, like clarifying the role of non-native input in first language acquisition during the critical period.
1.1. Variable input to hearing children learning spoken language
Among hearing children, two bodies of literature have focused on the nature of input and its effects on child language. The first concerns variability in the input monolingual children receive, with more input (often quantified as the number of words) and more joint engagement between a caregiver and child associated with better language outcomes (Anderson et al. Citation2021, Hirsh-Pasek et al. Citation2015, Holzinger et al. Citation2020; but cf. Sperry et al. Citation2019). Critical to the current study, this literature highlights the role of input, whether from caregivers, siblings, or others, as a key predictor of language development and later language and academic outcomes.
The second source of evidence considers the variability in input among hearing multilingual children whose parents are new learners of one or more of the child’s languages. Until recently, practical guidance to families whose home language is different from the majority language focused on the importance of using the majority language, rather than the child’s heritage language, in the home setting (see Spelorzi et al. Citation2021 for a review). With solid evidence to the contrary, however, this advice has now shifted to reflect findings demonstrating that bilingual children’s ability to learn the majority language does not depend solely on their parents’ use of that language (Hoff et al. Citation2021). Furthermore, input from native speakers seems to be more helpful for children’s overall language acquisition than input from non-native speakers (Place & Hoff Citation2016). For these reasons, and to promote family communication, parents are now often encouraged to use their primary language with their hearing bilingual children (Spelorzi et al. Citation2021), and educators are encouraged to support that language in a school setting while introducing the majority language.
1.2. Variable input to deaf children learning spoken or signed language
The experience of deaf children is not entirely parallel to hearing monolingual or bilingual language learners. For most deaf children, their home language is a spoken language to which they do not have complete auditory access, even with the use of assistive technology. Thus, their parents’ use of a dominant spoken language is unlikely to lead to age-expected language acquisition during the critical first years of life. This mismatch between a hearing parent’s reliance on one or more spoken languages, and their deaf child’s limited ability to access that language, often means that deaf children acquire a first language later than typically hearing children. Because deaf children vary significantly in when they begin to acquire a first language, researchers have been able to demonstrate that delayed exposure to a first language has robust impacts on many aspects of language, from syntax (Boudreault & Mayberry Citation2006, Henner et al. Citation2016, Mayberry & Lock Citation2003) to phonology (Hall et al. Citation2012, Morford Citation2000). Delayed access to a first language not only has downstream effects on many aspects of language learning, it impacts domains of cognition that depend on language, such as number understanding (see Santos & Cordes Citation2022, for a review) and theory of mind (see Pyers & deVilliers Citation2013, for a review).
While home (spoken) languages are not entirely accessible to deaf children, sign languages are frequently not fully available in the home environment to deaf children with hearing parents. When parents learn a sign language such as American Sign Language (ASL), they are initially novice signers who are learning alongside their deaf child. Their initial proficiency, rate of learning, and ability to use the language during interactions with their deaf child vary widely. Some hearing parents become highly fluent signers while others less so (Lieberman et al. Citation2022, Meyers & Bartee Citation1992). As with hearing bilingual parents (Hoff et al. Citation2021), parents’ proficiency in a sign language may be related to the amount of time they use that sign language with their child: parents who are fluent signers may sign more often, and parents who sign more often may become more fluent.
To what extent does this variation in parent ASL proficiency impact children’s early language acquisition? Our knowledge of the effect of parent sign language skills on deaf children’s language acquisition is coarse and limited. Most empirical studies compare language acquisition of deaf children with deaf parents to that of deaf children with hearing parents, with the assumption that hearing parents are, on average, poor language models (e.g., Hauser et al. Citation2016, Novogrodsky et al. Citation2014, Rosenburg et al. Citation2020). These studies consistently find that deaf children of hearing parents have lower language outcomes than deaf children with deaf parents. Yet the categorical treatment of input based on a parent’s hearing status fails to capture the very real variability in hearing parents’ sign language skills. Researchers were bound to this categorical treatment of input because robust assessments of sign language knowledge are relatively new (e.g., Bochner et al. Citation2011, Hauser et al. Citation2016), and because hearing parents typically learn sign language in informal settings that do not include assessment. Thus, we have been unable to evaluate how a range of sign language skills among hearing parents might relate to the range in language outcomes we see in their deaf children.
Understanding this relationship is critical because practitioners are divided on the efficacy of sign language use among hearing parents with deaf children. Some argue that deaf children’s language development may depend on early exposure to a sign language and on parents becoming fluent signers (e.g., Hall et al. Citation2019, Humphries et al. Citation2019, Napoli et al. Citation2015), while others discourage parents from using a sign language, suggesting that they can never achieve the level of fluency needed to support strong sign language acquisition (Geers et al. Citation2017, Knoors & Marschark Citation2012, Madell Citation2015). Both of these positions are logical, yet neither is based on empirical research that directly speaks to the role of parental input on sign language acquisition because no study to date has measured hearing parents’ sign language skills and assessed the relationship of those skills to their deaf child’s language outcomes.
Deaf children who have hearing parents have highly variable language outcomes (Scott & Dostal Citation2019; see Singleton & Meier Citation2021, for a review). With respect to sign language vocabulary, some work has suggested these children have similar vocabulary acquisition trajectories as deaf children of deaf parents (e.g., Hoiting Citation2005), but other researchers have noted that deaf children with hearing parents have smaller vocabulary sizes on average in comparison to deaf children with deaf parents (e.g., Woll Citation2013). More recently, a large-scale study demonstrated that when deaf children with hearing parents are exposed to sign language during infancy, they consistently develop age-level ASL vocabularies (Caselli et al. Citation2021). While early exposure to sign language can support ASL acquisition, we know a minimal amount about how the characteristics of that sign language exposure, particularly the language proficiency of their caregivers, shapes deaf children’s language growth.
1.3. Current study
In this paper, we ask whether input from caregivers with varying levels of proficiency is related to first language acquisition. While deaf children learning a sign language often have multiple language models outside of their family members such as teachers in early intervention programs and deaf role models who make home visits, many children spend the bulk of their time with their families. As such, we particularly are interested in the effects of input from non-native signing hearing parents. We ask how language input is related to early language development by probing ASL knowledge in a group of hearing parents learning ASL alongside their deaf signing children. If parent language skills are essential for child language acquisition, we would expect parent ASL proficiency to be strongly related to child language acquisition, defined here as ASL vocabulary size. This relationship should hold, independent of other related factors (e.g., age of ASL exposure). Alternatively, if parental ASL skills are just one of many factors that predict a child’s language skills, we may find a weak relationship between parent and child ASL proficiency. Or, there may be no significant relationship between parental ASL skills and children’s ASL vocabularies. We also ask whether the relationship between parent and child ASL skills depends on age, and hypothesize that parent ASL skills may be increasingly important for older children as they acquire more vocabulary.
2. Methods
2.1. Participants
The Boston University Institutional Review Board approved this study. We recruited parents/caregivers of deaf children (n = 55) to participate in the study, using the following inclusion criteria: the parent/caregiver is hearing; the parent/caregiver is learning ASL; the deaf/hard of hearing child is between the ages of 8 and 60 months (though we did include one participant with a 69-month-old child); and the deaf/hard of hearing child is learning ASL, either as their only primary language or alongside spoken English. We used snowball sampling and social media advertisements to recruit participants nationwide; recruitment materials were also sent to ASL parent-infant programs. We confirmed the parent’s eligibility (and removed fraudulent responses) through a three sign ASL vocabulary check where parents saw a slow-motion video of three signs (MOTHER, NAME, and DEAF), and had to type the meaning of at least one of those signs in English.
For the final analyses, we excluded the data from children who had additional diagnoses related to language acquisition (e.g., CHARGE syndrome, Down Syndrome, or Autism Spectrum Disorder), and/or were blind or had low vision to minimize variation in child acquisition (n = 11). When we included these children in the analysis, with diagnosis as an additional predictor, the results were qualitatively the same. The final sample included 44 deaf children (see for demographic information). presents the varied language backgrounds of the participants.
Table 1. Demographic background of participants.
Table 2. Language and hearing background of participants.
2.2. Procedure
Parents were sent a unique link where they provided informed consent, then completed a demographic questionnaire, a vocabulary checklist for their deaf child, and two online assessments of their own ASL skills. Parents could complete the battery of measures across several sittings, but were required to complete all within one week. Families were compensated in increments of $25 up to $75 for three sessions of online testing with a $15 completion bonus.
2.3. Materials
(i) Demographic and Language History Questionnaire
This online questionnaire developed in our lab consisted of questions about the child’s basic demographics (age, race, ethnicity, etc.) and language experience that included questions about hearing loss, use of assistive hearing devices, and use of ASL and spoken English. Parents reported whether their child was currently or had previously been participating in early intervention, however we did not collect detailed information on the type of early intervention nor the exposure to ASL from early intervention or other external sources. The exact wording of the questions reported in can be found in the Appendix.
(ii) American Sign Language Communicative Development Inventory 2.0 (ASL-CDI 2.0; Caselli et al. Citation2020; www.aslcdi.org)
Child ASL vocabulary knowledge was assessed by having parents complete the ASL-CDI 2.0, an authorized ASL adaptation of the MacArthur Bates Communicative Development Inventory (MB-CDI) that measures children’s ASL expressive and receptive vocabulary skills. In the ASL-CDI 2.0, parents view videos of 534 individual ASL signs and report whether their child understands, understands and produces, or does not know, a given sign. While we collected data on both expressive and receptive vocabularies, we report results from only expressive vocabulary measures in this paper in order to be consistent with other adaptations of the MB-CDI, which typically focus on productive vocabulary for older children. Likely due to its length, not all parents completed the entire ASL-CDI (the median number completed was 526, minimum 170), and so child vocabulary scores were computed as a proportion of signs the child knew out of the items for which the parent provided a response. Prior work has demonstrated that scores from subset of as few as 30 items highly correlates with the scores on the whole test (Caselli et al. Citation2020).
The normative sample for the ASL-CDI was a group of 120 deaf children who had deaf, signing parents (ages 9 to 73 months; Caselli et al. Citation2020). From this normative sample, we estimated the range of vocabulary sizes expected for children at each age. These estimates were used as a benchmark in the present study, to determine whether the participants (deaf children who had hearing parents) had age-expected vocabulary sizes (i.e., within about a standard deviation of the mean vocabulary size of children from the normative sample at the same age).
(iii) ASL-Comprehension Test (ASL-CT; Hauser et al. Citation2016)
The ASL-CT is a 30-question multiple-choice ASL test that is administered online to assess sign language comprehension skills including phonology, vocabulary, morphology, syntax, and depiction. It is designed for use with adult signers with a range of proficiencies (from native deaf signers to non-native ASL students).
(iv) ASL-Course Level
Because it was uncertain at the outset whether the ASL-CT would be too difficult for the study population and result in a floor effect, we also evaluated parent expressive ASL skill using an ASL course level assessment, which is an evaluation rubric used at Boston University to place students in one of five ASL course levels. Parents submitted a short video of themselves signing a clip of a non-verbal Pixar movie that is well-suited to elicit depiction and other complex linguistic structures in ASL. A deaf ASL instructor with several years of experience in administering this assessment to hundreds of students determined which ASL course (ranging from 1-5) they would recommend as “placement” for each parent.
3. Results
3.1. Parent ASL proficiency
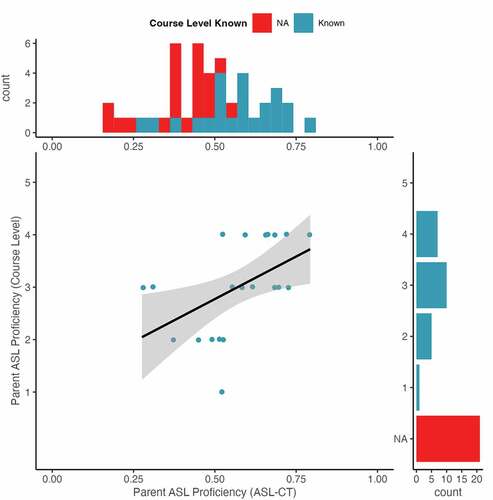
Nearly half of the participants (n = 21) declined to participate in the ASL Course Level assessment, often noting that they felt embarrassed or shy about recording themselves. Generally, the parents who did not participate in the ASL Course Level assessment had lower ASL-CT scores (MWithCourseLevel = 0.39, MWithoutCourseLevel = 0.57; t(41.63) = -4.92, p < 0.01). Among those who participated in the ASL Course Level assessment, we observed a significant positive relationship between parent ASL-CT score and parent ASL Course Level (rho = 0.61, p < 0.01, see ). We did not see a floor effect on the ASL-CT; parents had a range of scores (). This indicates that the ASL-CT is sensitive enough to measure differences among relatively new signers, and that while the ASL-CT is a measure that indexes only comprehension (i.e., receptive ability), it is also an indirect indicator of expressive ability. Because so many caregivers declined to submit a video, we had insufficient ASL Course Level information to include in the subsequent statistical analyses, and we instead used the ASL-CT as the measure of caregiver language skill unless otherwise noted. There was no significant correlation between parent ASL proficiency and child’s age (rho = 0.22, p = 0.15).
Figure 1. The relationship between American Sign Language-Comprehension Test (ASL-CT) scores and ASL Course Level assignments. The margins show histograms illustrating the distribution of ASL Course Levels (side) and ASL-CT scores (top) in the sample. Points jittered slightly to reduce overlap. Plot was created in R using ggplot2 (Wickham Citation2016).
3.2. Parent proficiency as a predictor of child ASL vocabulary
We first asked whether child ASL vocabulary knowledge varied as a function of parent ASL skill, while controlling for factors known to affect vocabulary development (i.e., chronological age and age of exposure to ASL). Using R (version 4.1.2) we ran a linear regression to investigate children’s ASL expressive vocabulary with the following predictors: child’s age, age of child’s first ASL exposure, and parent ASL proficiency (ASL-CT), and an interaction between child age and parent ASL proficiency. There was a significant interaction between child chronological age and parent ASL proficiency (). To interpret this interaction, in we illustrate the estimated effect of parent ASL proficiency for children at three ages (the mean and +/- 1 standard deviation from the mean), and conduct a simple slopes analysis for the effect of parent ASL proficiency at each of these ages with the sim slopes function in the package interactions (Long, Citation2019). The visualization indicates that parents’ ASL proficiency was positively correlated with children’s ASL vocabulary size, and this relationship was stronger for the older and middle age groups than for the younger age group. The simple slopes analysis confirmed this finding, showing that there was significant effect of parent ASL proficiency for the middle (B = 0.74, s.e. = 0.19, t = 3.93, p < 0.01) and older children (B = 1.30, s.e. = 0.32, t = 4.10, p < 0.01), but not for the younger children (B = 0.19, s.e. = 0.27, t = 0.68, p = 0.50). In contrast to previous findings, we observed no effect of age of ASL exposure on children’s expressive vocabulary. The full model accounted for 54.6% of the variance (R2) in children’s expressive vocabulary.
Figure 2. Interaction effect between child age and parent American Sign Language (ASL) proficiency on child ASL vocabulary size. Plot generated with the plot model function in the package sjPlot (Lüdecke Citation2021). The three lines represent the estimated values for children at the mean age (32 months), one standard deviation younger than the mean age (19 months), and one standard deviation older than the mean age (47 months).
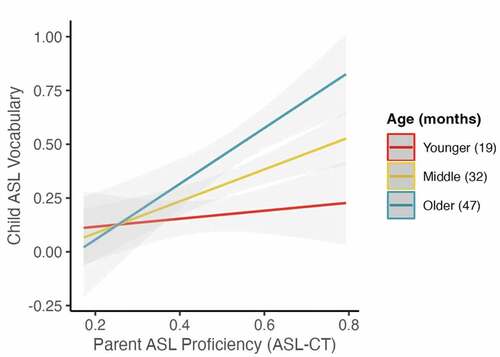
Table 3. Model of child expressive vocabulary as predicted by age, age of ASL exposure, parent ASL proficiency, and an interaction between age and parent ASL proficiency.
3.3. Parent ASL proficiency relative to children’s age-expected ASL vocabulary
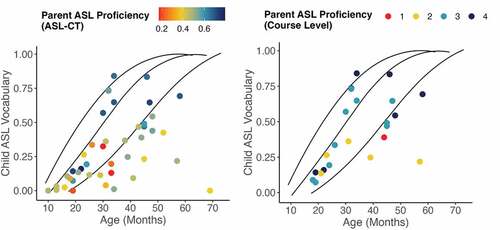
The relationship between parent signing skills and children’s own language skills is stronger for older children than for younger children. Yet, we don’t have a full picture of the nature of this relationship. To explore whether there is a specific level of parent ASL proficiency at which children typically have age-expected vocabularies, we plotted expressive vocabulary size in the current sample of deaf children with hearing parents alongside the normative data from deaf children with fluent signing deaf parents from the ASL-CDI 2.0 norming sample (Caselli et al. Citation2020). We color-coded the child vocabulary data according to their parents’ ASL skills (). If parent ASL skill is the primary determinant of child ASL vocabulary, then only children whose parents are sufficiently proficient would have age-expected vocabulary. Conversely, if parent ASL skill only weakly determines child ASL, then we would expect that children may range in ASL skill regardless of parent ability. Visualization of these data indicates that most children in our sample whose parents had strong ASL skills had ASL vocabulary sizes in the expected range. Notably, some children, particularly younger children, achieved age-expected ASL skills while their parents were still at the early stages of learning ASL.
Figure 3. The relationship between child age and child American Sign Language (ASL) expressive vocabulary size. The y-axis illustrates the child’s vocabulary size, measured as a proportion of signs the child can produce out of the total number of signs for which the parents provided a response. The three black lines show growth curves that are drawn from normed data published in Caselli et al. (Citation2020) and are based on deaf children with deaf parents, indicating the 16th (right-most line), 50th (center line), and 84th percentiles (left-most line). Each dot represents a deaf child with hearing parents in this study. Dots are shaded by parent ASL proficiency, with a gradient from red (least proficient), yellow, teal, to navy (most proficient). On the left, parent proficiency is measured with the ASL-CT, and on the right by ASL Course Level. Plots generated in R using ggplot2 (Wickham Citation2016).
4. Discussion
We investigated the role of parent ASL proficiency on children’s ASL expressive vocabulary. We assessed ASL skill among hearing parents who were learning ASL to communicate with their deaf child, and we assessed those children’s expressive ASL vocabularies. There was an interaction between parent ASL skills and age that revealed that parent ASL skills positively affected vocabulary development among preschool aged children, but did not significantly affect expressive vocabulary size among the youngest children in our sample. Some children demonstrated age-appropriate ASL vocabularies despite the fact that their parent’s ASL skill was still emerging. The interaction between parent ASL proficiency was independent from children’s age of first ASL exposure. Together, these findings bring nuance to our understanding of the role of input variation on children’s language acquisition, and encourage us to think about the importance of early input with respect to not only the timing of language input, but also the kinds of language input children receive during early childhood. We demonstrate that the proficiency of children’s language models can and does play a role in children’s language development.
In this study, we deconstructed the notion of “non-native” input to deaf children, considering hearing parent ASL skills on a continuum rather than simply as categorically unskilled signers. In doing so, we find that hearing parents are not uniformly, categorically, poor signers, and their variation in signing skills positively relates to the variation in their children’s vocabulary acquisition. Thus, children need not only early language input but also exposure to skilled language users.
Importantly, skilled language use does not necessarily mean “native” fluency. Even the most proficient parents in this study did not have ASL skills equivalent to early-exposed, deaf signers, and yet their children reliably had age-expected ASL vocabularies. The most proficient signers in this study were evaluated to be comparable to ASL III or ASL IV students, which reflects three or four semesters or 18 months of coursework. This timing is noteworthy, as our data also show that at 18-months-old, children’s vocabularies are robust to variation in parent ASL skills.
It may be unsurprising that we do not see a strong relationship between parent ASL skills and children’s vocabulary development in the youngest children (i.e., those below 18 months). Most hearing children in this age range (8 to 18 months) have yet to enter a vocabulary spurt and generally have vocabulary sizes of less than 50 words (Bloom Citation1976, Nelson Citation1973), and vocabulary development at this time may more affected by early social pragmatic skills such as gaze following and joint attention (Brooks & Meltzoff Citation2008, Tomasello & Farrar Citation1986) than by a sophisticated understanding of the phonology and morphosyntax of a language. Hearing parents are just beginning their journey of learning a sign language and may not have yet encountered the linguistic features of ASL tapped by the ASL assessment we conducted. Even without being highly proficient signers, their emerging sign language skills and language-related behaviors (e.g., fostering joint attention, showing positive affect, and turn-taking) appear sufficient for parents of young children to engage in rich language experiences with their children. As children begin to string signs together into longer and longer utterances, parents’ more complex sign language abilities may critically support the acquisition of new words, by providing input that includes syntactic and pragmatic cues to meaning (Bloom Citation2000, Gelman & Markman Citation1985, Naigles Citation1990). Stronger ASL skills may allow parents to engage in more complex and extended conversations that introduce new and more varied vocabulary to their children. More work is needed to examine the relationship between parent and child language skills, including higher order language skills, in older children.
Although parent ASL skills positively predicted children’s vocabulary size, we cannot definitively conclude that parent ASL skills drive children’s vocabulary development. It may be the opposite: observing their children’s growing vocabulary size may motivate parents to become more fluent in ASL. In general, parents are highly attuned to their child’s language use and modify their input according to their child’s language skills (Albert et al. Citation2018, Bornstein et al. Citation1999). Some evidence in support of this pattern of development comes from those cases in our data of younger children who have vocabularies comparable to deaf children who have deaf parents, which have emerged despite their parents having weaker ASL skills. Following these children and their parents longitudinally would allow us to see whether children’s growing language skills lead the way for their parents to become more proficient signers, or vice versa. Another possible explanation for the relationship between parent and child ASL skills is that an outside variable like access to ASL learning resources may benefit both parents’ and children’s ASL acquisition, and may at least partially account for the significant relationship we identified here. In particular, older children may participate in early intervention programs that meet more frequently and for longer hours than those in which younger children participate, and early intervention may be an additional source of ASL exposure for some children. Building a more complete picture of the many factors that affect sign language outcomes for deaf children is a critical next step for researchers.
Our findings also point to the fact that children’s vocabulary development is not exclusively dependent on their caregivers’ proficiency in the language. While parent ASL skills account for a significant amount of variation in children’s vocabularies, there are a host of other factors that may also shape vocabulary acquisition. Deaf children and their families in the United States have varying access to early intervention services that support sign language learning in the home (Lieberman et al. Citation2022). Our study did not quantify the types, amount, and quality of language instruction received by children and their families. In studies of hearing children, a significant amount of variation in language skills is also attributable to child-internal processing factors (Kidd & Donnelly Citation2020), and the same is likely true of deaf children learning a sign language.
Young children appear to have the ability to access and learn a perceptually accessible language even when they are receiving input from less proficient signers. This observation is consistent with work showing that children’s language skills can “surpass their models” (Singleton & Newport Citation2004), outperforming their parents on a range of language skills (Flaherty et al. Citation2021). The mechanisms of child learning seem to allow children to exceed their input when that input is inconsistent. The degree to which these mechanisms affect vocabulary development remains to be seen.
Unlike previous studies, age of ASL acquisition did not affect children’s ASL vocabulary. The null effect in this study may be due to a lack of variation on this dimension in this sample; the median age at which children in our sample started learning ASL was two months old, an age of acquisition when age-expected vocabulary development has now been attested (Caselli et al. Citation2021). While some children in this sample began learning ASL as late as 36 months, this age of acquisition is still far younger than most studies of age of first language exposure, which often include children who began learning in adolescence or even adulthood (see Mayberry & Kluender Citation2018, for a review). Also, vocabulary appears to be one domain that is resilient to delayed first language exposure, even among very late learners (Ferjan Ramirez et al. Citation2013). The lack of age of acquisition effects here may also indicate that among very young children, age of exposure is relatively less important than the kinds of language exposure children receive. However, the fact that we did not see evidence for an effect of age of acquisition in this sample does not mean age of ASL exposure does not matter among this age group. For example, exposure to ASL in infancy shapes children’s visual attention to faces during signing (Bosworth et al. Citation2022). It remains to be seen whether and how variations in age of acquisition in the first year of life affects other aspects of sign language acquisition.
Parent sign language proficiency is an important factor in child vocabulary, though it is just one contributor to children’s healthy vocabulary development. Children’s language skills may be shaped by the number of adults and peers they interact with in ASL, the fluency of all of those people, and the amount of time they spend using ASL (See Hoff et al. Citation2021, for a discussion of these factors in spoken language bilinguals). Hearing parents can support their deaf children’s ASL acquisition in many ways beyond learning and using ASL with their child, such as participating in sign-centric parent-infant programs, working with ASL-fluent early intervention specialists, and/or connecting with deaf signing language models. The type and amount of exposure to ASL that deaf children receive varies widely as does the type and amount of access that hearing parents have in obtaining ASL-based services for their families (Lieberman et al. Citation2022, Pichler Citation2021). The current findings serve as a call to the field to build a comprehensive picture of how early language learning environments relate to children’s sign language acquisition. Furthermore, our findings highlight the need for creation of accessible means through which parents can learn ASL.
The current study shows that, on the one hand, parent language skills are important for children to acquire early vocabulary, and, on the other hand, children can acquire an early lexicon with input from novice signing parents, especially in the earliest period of language learning. We do not interpret this pattern to suggest that children do not need language models from birth, but that parents can and do support children as they themselves become more proficient signers. Parents may learn a sign language not only because their children’s language acquisition may depend on their language learning efforts, but also because they want to communicate with their children in ways that are fully accessible for all family members. Communication is important for healthy family relationships and perceived quality of life among deaf children (Kushalnagar et al. Citation2011). And engagement in rich conversations in the family supports stronger social-emotional and psychosocial development (Calderon & Greenberg Citation2011). Parents may also learn ASL because it offers them a way of connecting with deaf communities (e.g., deaf friends, teachers, childcare providers, etc.) in addition to supporting their child’s healthy language development. Lastly, by supporting ASL acquisition in their children, parents may also be indirectly aiding their children’s English acquisition, as English skills are positively related to ASL skills (e.g., Hoffmeister et al. Citation2022, Hrastinski & Wilbur Citation2016, Keck & Wolgemuth Citation2020, Pontecorvo et al. Citation2023).
Together, these results paint a nuanced picture of the importance of language input early in deaf children’s development: parents should learn a sign language in order to facilitate their children’s sign language acquisition, but they do not need to achieve immediate proficiency or native-like fluency for their children to acquire language. Hearing parents can achieve levels of fluency that support their children’s early access to and healthy acquisition of a full and rich natural language.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Notes
1 We use the term “deaf” to refer to this subset of children who have incomplete auditory access to speech. We use the lower case “d” to refer inclusively to children regardless of cultural or linguistic identity.
2 We use the term “naturally-evolved sign language” to refer to sign languages such as American Sign Language that have evolved in the manual-visual modality and, like all languages, are linguistically complete and have their own syntactic, morphological, and phonological systems. We contrast this with manual systems of communication that are designed to make a spoken language visually accessible (e.g., Sign Supported English, Cued Speech, Manually Coded English etc.).
References
- Albert, Rachel R., Jennifer A. Schwade & Michael H. Goldstein. 2018. The social functions of babbling: acoustic and contextual characteristics that facilitate maternal responsiveness. Developmental Science 21(5). 21:e12641.
- Anderson, Nina J., Susan A. Graham, Heather Prime, Jennifer M. Jenkins & Sheri Madigan. 2021. Linking quality and quantity of parental linguistic input to child language skills: A meta analysis. Child Development 92(2). 484–501.
- Bloom, Lois. 1976. One word at a time: The use of single word utterances before syntax. The Hague, the Netherlands: Mouton.
- Bloom, Paul. 2000. How children learn the meanings of words. MIT Press.
- Bochner, Joseph, Karen Christie, Peter Hauser & Matt J. Searls. 2011. When is a difference really different? Learners’ discrimination of linguistic contrasts in American Sign Language. Language Learning 61(4). 1302–1327. doi: 10.1111/j.1467-9922.2011.00671.x.
- Bornstein, Marc H., Catherine S. Tamis-LeMonda & Maurice O. Haynes. 1999. First words in the second year: Continuity, stability, and models of concurrent and predictive correspondence in vocabulary and verbal responsiveness across age and context. Infant Behavior and Development 22(1). 65–85.
- Bosworth, Rain G., So One Hwang & David P. Corina. 2022. Visual attention for linguistic and non-linguistic body actions in non-signing and native signing children. Frontiers in Psychology, 13.
- Boudreault, Patrick & Rachel I. Mayberry. 2006. Grammatical processing in American sign language: Age of first-language acquisition effects in relation to syntactic structure. Language and Cognitive Processes 21(5). 608–635.
- Brooks, Rachel & Andrew N. Meltzoff. 2008. Infant gaze following and pointing predict accelerated vocabulary growth through two years of age: A longitudinal, growth curve modeling study. Journal of Child Language 35(1). 207–220.
- Calderon, Rosemary & Mark Greenberg. 2011. Social and emotional development of deaf children: Family, school, and program effects. In M. Marschark & P. E. Spencer (eds.), The Oxford handbook of deaf studies, language, and education, 188–199. Oxford University Press.
- Caselli, Naomi K., Amy M. Lieberman & Jennie E. Pyers. 2020. The ASL-CDI 2.0: An updated, normed adaptation of the MacArthur bates communicative development inventory for American Sign Language. Behavior Research Methods 52(5). 2071–2084.
- Caselli, Naomi, Jennie E. Pyers & Amy M. Lieberman. 2021. Deaf children of hearing parents have age-level vocabulary growth when exposed to American Sign Language by 6 months of age. The Journal of Pediatrics 232. 229–236.
- Fenson, Larry, Philip S. Dale, J. Steven Reznick, Elizabeth Bates, Donna J. Thal, Stephen J. Pethick, … & Joan Stiles. 1994. Variability in early communicative development. Monographs of the society for research in child development 59(5). i–185.
- Flaherty, Molly, Dea Hunsicker & Susan Goldin-Meadow. 2021. Structural biases that children bring to language learning: A cross-cultural look at gestural input to homesign. Cognition 211. 104608.
- Geers, Ann E., Christine M. Mitchell, Andrea Warner-Czyz, Nae-Yuh Y. Wang, Laurie S. Eisenberg & CDaCI Investigative Team. 2017. Early sign language exposure and cochlear implantation benefits. Pediatrics 140(1).e20163489.
- Gelman, Susan A. & Ellen M. Markman 1985. Implicit contrast in adjectives vs. nouns: Implications for word-learning in preschoolers. Journal of Child Language 12(1). 125–143.
- Hall, Matthew. L., Victor S. Ferreira & Rachel I. Mayberry. 2012. Phonological similarity judgments in ASL. New Methodologies in Sign Language Phonology: Papers from TISLR 10, 15(1). 104–127.
- Hall, Matthew L., Wyatte C. Hall, & Naomi K. Caselli. 2019. Deaf children need language, not (just) speech. First Language 39(4). 367–395.
- Hall, Wyatte C., Scott R. Smith, Erika J. Sutter, Lori A. DeWindt & Timothy Dye. 2018. Considering parental hearing status as a social determinant of deaf population health: Insights from experiences of the “dinner table syndrome.” PloS One 13(9). e0202169.
- Hauser, Peter C., Raylene Paludneviciene, Wanda Riddle, Kim B. Kurz, Karen Emmorey & Jessica Contreras. 2016. American Sign Language Comprehension Test: A tool for sign language researchers. Journal of Deaf Studies and Deaf Education 21(1). 64–69.
- Henner, Jonathan, Catherine L. Caldwell-Harris, Rama Novogrodsky & Robert Hoffmeister. 2016. American sign language syntax and analogical reasoning skills are influenced by early acquisition and age of entry to signing schools for the deaf. Frontiers in Psychology 07.
- Hirsh-Pasek, Kathy, Lauren B. Adamson, Roger Bakeman, Margaret T. Owen, Roberta M. Golinkoff, Amy Pace, … & Katherine Suma. 2015. The contribution of early communication quality to low-income children’s language success. Psychological Science 26(7). 1071–1083.
- Hoffmeister, Robert, Jon Henner, Catherine Caldwell-Harris & Rama Novogrodsky. 2022. Deaf children’s ASL vocabulary and ASL syntax knowledge supports English knowledge. Journal of Deaf Studies and Deaf Education 27(1). 37–47.
- Hoff, Erika, Michelle K. Tulloch & Cynthia Core. 2021. Profiles of minority-majority language proficiency in 5-year-olds. Child Development 92(5). 1801-1816.
- Hoiting, Nini. 2005. Deaf children are verb attenders: Early sign vocabulary development in Dutch toddlers. In Brenda Schick, Marc Marschark & Patricia Elizabeth Spencer (eds), Advances in the Sign-Language Development of Deaf Children, 161–188. New York: Oxford University Press.
- Holzinger, Daniel, Magdelena Dall, Susan Sanduvete-Chaves, David Saldaña, Salvador Chacón-Moscoso & Johannes Fellinger. 2020. The impact of family environment on language development of children with cochlear implants: A systematic review and meta-analysis. Ear and Hearing 41(5). 1077–1091.
- Hrastinski, Iva & Ronnie B. Wilbur. 2016. Academic achievement of deaf and hard-of-hearing students in an ASL/English bilingual program. Journal of Deaf Studies and Deaf Education 21(2). 156–170.
- Humphries, Tom, Poorna Kushalnagar, Gaurav Mathur, Donna J. Napoli, Christian Rathmann & Scott Smith. 2019. Support for parents of deaf children: Common questions and informed, evidence-based answers. International Journal of Pediatric Otorhinolaryngology 118. 134–142.
- Huttenlocher, Janellen, Wendy Haight, Anthony Bryk, Michael Seltzer & Thomas Lyons. 1991. Early vocabulary growth: Relation to language input and gender. Developmental Psychology 27(2). 236–248.
- Keck, Tamara & Keith Wolgemuth. 2020. American Sign Language phonological awareness and English reading abilities. Sign Language Studies 20(2). 334–354.
- Kidd, Evan & Seamus Donnelly. 2020. Individual differences in first language acquisition. Annual Review of Linguistics 6. 319–340.
- Knoors, Harry & Marc Marschark. 2012. Language planning for the 21st century: Revisiting bilingual language policy for deaf children. The Journal of Deaf Studies and Deaf Education 17(3). 291–305.
- Kushalnagar, Poorna, Tari Topolski, Brenda Schick, Todd C. Edwards, Anne M. Skalicky & Donald L. Patrick. 2011. Mode of communication, perceived level of understanding, and perceived quality of life in youth who are deaf or hard of hearing. Journal of Deaf Studies and Deaf Education 16(4). 512–523.
- Lieberman, Amy M., Julie Mitchiner & Elana Pontecorvo. 2022. Hearing parents learning American Sign Language with their deaf children: A mixed-methods survey. Applied Linguistics Review. https://doi.org/10.1515/applirev-2021-0120
- Long, Jacob A. 2019. _interactions: Comprehensive, User-Friendly Toolkit for Probing Interactions_. R package version 1.1.0, https://cran.r-project.org/package=interactions>.
- Lüdecke, Daniel. 2021. sjPlot: Data visualization for statistics in social science (R package version 2. 8.10) [Computer software]. The Comprehensive R Archive Network. https://CRAN.R-project.org/package=sjPlot
- Madell, Jane. 2015. It’s not the same old deafness. Hearing Health Matters. https://hearinghealthmatters.org/hearingandkids/2015/its-not-the-same-old-deafness-2/
- Mayberry, Rachel. I., & Elizabeth Lock. 2003. Age constraints on first versus second language acquisition: evidence for linguistic plasticity and epigenesis. Brain and Language 87(3). 369–384.
- Mayberry, Rachel I. & Robert Kluender. 2018. Rethinking the critical period for language: New insights into an old question from American Sign Language. Bilingualism: Language and Cognition 21(5). 886–905.
- Meyers, John E. & James W. Bartee. 1992. Improvements in the signing skills of hearing parents of deaf children. American Annals of the Deaf 137(3). 257–260.
- Morford, Jill. P. & Rachel I. Mayberry. 2000. A reexamination of “early exposure” and its implications for language acquisition by eye. In C. Chamberlain, J. P. Morford & R. I. Mayberry (eds.), Language acquisition by eye, 111–127 Lawrence Erlbaum Associates Publishers.
- Naigles, Letitia. 1990. Children use syntax to learn verb meanings. Journal of Child Language 17(2). 357–374.
- Napoli, Donna J., Nancy K. Mellon, John K. Niparko, Christian Rathmann, Gaurav Mathur, Tom Humphries, … & John D. Lantos. 2015. Should all deaf children learn sign language? Pediatrics 136(1). 170–176.
- Nelson, Katherine. 1973. Structure and strategy in learning to talk. Monographs of the Society for Research in Child Development 38(1/2). 1.
- Novogrodsky, Rama, Sarah Fish & Robert Hoffmeister. 2014. The acquisition of synonyms in American Sign Language (ASL) toward a further understanding of the components of ASL vocabulary knowledge. Sign Language Studies 14(2). 225–249.
- Pichler, Deborah C. 2021. Constructing a profile of successful L2 signer hearing parents of deaf children. Senri Ethnological Studies 107. 115–131.
- Place, Sylvia & Erica Hoff. 2016. Effects and noneffects of input in bilingual environments on dual language skills in 2 ½-year-olds. Bilingualism: Language and Cognition 19(5). 1023–1041.
- Pontecorvo, Elana, Michael Higgins, Joshua Mora, Amy M. Lieberman, Jennie Pyers & Naomi K. Caselli. 2023. Learning a sign language does not hinder acquisition of a spoken language. Journal of Speech, Language, and Hearing Research, 1–18.
- Pyers, Jennie & Peter A. de Villiers. 2013. Theory of mind in deaf children: Illuminating the relative roles of language and executive functioning in the development of social cognition. In Donald Cohen, Helen Tager-Flusberg, Michael Lombardo & Simon Baron-Cohen (eds.), Understanding other minds: Perspectives from developmental social neuroscience, 345–363. OUP Oxford.
- Ramírez, Naja F., Amy M. Lieberman & Rachel I. Mayberry. 2013. The initial stages of first-language acquisition begun in adolescence: when late looks early. Journal Of Child Language 40(2). 391–414.
- Rich, Benjamin. 2021. table1: Tables of descriptive statistics in html (R package version 1.4.2) [Computer software]. The Comprehensive R Archive Network. https://CRAN.R-project.org/package=table1
- Rosenburg, Patrick, Amy M. Lieberman, Naomi Caselli & Robert Hoffmeister. 2020. The development and evaluation of a new ASL text comprehension task. Frontiers in Communication 25.
- Rowe, Meredith L. 2012. A longitudinal investigation of the role of quantity and quality of child-directed speech in vocabulary development. Child Development 83(5). 1762–1774.
- Santos, Stace & Sara Cordes. 2022. Math abilities in deaf and hard of hearing children: The role of language in developing number concepts. Psychological Review 129(1). 199.
- Scott, Jessica A. & Hannah M. Dostal. 2019. Language development and deaf/hard of hearing children. Education Sciences 9(2). 135.
- Singleton, Jenny L. & Richard P. Meier. 2021. Sign language acquisition in context. In C. Enns, J. Henner, & L. McQuarrie (eds), Discussing bilingualism in deaf children: Essays in honor of Robert Hoffmeister, 17–34. New York: Routledge.
- Singleton, Jenny L. & Elissa L. Newport. 2004. When learners surpass their models: The acquisition of American Sign Language from inconsistent input. Cognitive Psychology 49(4). 370–407.
- Spelorzi, Robert, Eva-Maria Schnelten, Candice Mathers & Antonella Sorace. 2021. More than one language: understanding the educational benefits of bilingualism. In Eurydice Bauer, Lenny Sánchez, Yang Wang and Andrea Vaughan (eds.), A transdisciplinary lens for bilingual education, 55–75. New York: Routledge.
- Sperry, Douglas E., Linda L. Sperry & Peggy J. Miller. 2019. Reexamining the verbal environments of children from different socioeconomic backgrounds. Child Development 90. 1303–1318. https://doi.org/10.1111/cdev.13072
- Strong, Michael & Philip M. Prinz. 1997. A study of the relationship between American Sign Language and English literacy. The Journal of Deaf Studies and Deaf Education 2(1). 37–46.
- Tomasello, Michael & Michael J. Farrar. 1986. Joint attention and early language. Child Development 57(6). 1454–1463.
- Weisleder, Adriana & Anne Fernald. 2013. Talking to children matters: Early language experience strengthens processing and builds vocabulary. Psychological Science 24(11). 2143–2152.
- Wickham, Hadley. 2016. ggplot2: Elegant graphics for data analysis () [Computer software]. The Comprehensive R Archive Network. https://ggplot2.tidyverse.org (December 1, 2022).
- Woll, Bencie. 2013. Sign language and spoken language development in young children: Measuring vocabulary by means of the CDI. In Laurence Meurant, Aurélie Sinte, Mieke Van Herreweghe & Myriam Vermeerbergen (eds.), Sign language research, uses and practices, 15–34. Berlin, Boston: De Gruyter Mouton.