
Abstract
Background
Involvement in research and shared priorities among occupational therapists (OTs) can enhance the quality of occupational therapy practice.
Aims
To explore the research involvement and research priorities of OTs in Norway.
Materials and methods
An online survey comprising 14 open-ended and closed questions was made available to participants at the Seventh Norwegian Congress in Occupational Therapy to fill out.
Results
Out of 633 congress participants, 307 (49%) OTs completed the survey. Among the respondents, ∼40% were involved in research. The most commonly reported area of research was rehabilitation. Research involvement was associated with employment in education or specialist healthcare services and with greater work experience and post-bachelor’s degree education. The most frequently prioritized research question addressed the effect of occupational therapy. Unmet needs and factors conducive to increasing OT’s involvement in research were identified.
Conclusions and significance
The survey revealed that a considerable, but uneven, distribution of OTs were involved in research. To encourage greater participation in research, researchers, decision-makers, and employee associations should take steps to make research more appealing to OTs. The research priorities highlighted by Norwegian OTs align with those stated by OTs in other countries.
Introduction
Evidence-based practice (EBP) involves synthesizing critically appraised research results, a practitioner’s clinical experience, and the client’s preferences [Citation1,Citation2]. Assuming access to high-quality and up-to-date research, EBP enables occupational therapists (OTs) to choose the most effective treatment techniques, apply clinical skills, and collaborate with patients in making informed decisions regarding their treatment options [Citation1,Citation2]. Results from a qualitative systematic review shows that health care professionals’ involvement in research improve both access to evidence based health care and the quality of their clinical performance [Citation3]. Consequently, there has been a call for OTs to increase their research involvement [Citation4].
Evidence regarding the effects of occupational therapy has increased markedly since the beginning of the 2000s [Citation5,Citation6]. Many OTs are also involved, or eager to become involved, in research [Citation7]. That said, few OTs have formal research expertise [Citation8]. Furthermore, a search in PubMed on occupational therapy and its effects shows that the number of published articles within occupational therapy is limited compared to other healthcare disciplines, such as nursing and physiotherapy. When considering a future scenario where healthcare services have fewer employees per patient, it is imperative that OTs offer evidence-based, sustainable, and effective interventions [Citation9].
With limited access to research resources, it is also important for researchers, clinicians, and healthcare users to work together and agree on researching areas of the highest priority [Citation10]. Within the field of occupational therapy, attempts have been made to comply with this recommendation. The World Federation of Occupational Therapists has agreed upon an international research priority statement that highlights a need to investigate the effectiveness of occupational therapy interventions [Citation11]. In a recent paper, Watson et al. explored unanswered questions about occupational therapy from a shared perspective of users and providers of healthcare services in the United Kingdom [Citation12]. The top three reported research priorities were related to the core competence of occupational therapy and how to make a difference in people’s everyday lives. These priorities aim to ensure a person-centred practice, increase efficacy, and to streamline access to services for patients, family, and carers [Citation12].
To ensure that research holds high quality, Chalmers and Glasziou [Citation13] recommend asking research questions relevant to those concerned, apply high-quality study designs and appropriate methods, and ensure that results are accessible to all interested parties. There is thus an emphasis on collaboration across different stakeholders, national borders, and research groups [Citation11,Citation14,Citation15], and on better anchoring research in established teams led by investigators with a good track record in obtaining funding and performing high-quality research [Citation16].
Even if collaboration between clinicians and researchers is recommended and a prerequisite for quality in research, collaboration can also be complex and challenging to navigate [Citation17]. OTs who are motivated to get involved in research may experience barriers, such as a lack of established practice for research involvement, or that patient treatment takes priority over research [Citation18]. Such barriers may be surmountable if OTs who are involved in research have sufficient support from colleagues and leaders, and have time specifically allocated to focus solely on their research activity [Citation4]. However, more knowledge is needed regarding factors that may contribute to promoting OTs’ involvement in research.
The aim of this study was to explore research involvement and research priorities among OTs in Norway.
Materials and methods
To ensure transparent reporting, we used the Consensus-Based Checklist for Reporting of Survey Studies [Citation19].
Study design
To obtain a national perspective regarding OTs’ priorities and involvement in research, a cross-sectional study design using an online survey was carried out with OTs filling out the answers themselves. The survey method gave the researchers access to a broad range of OTs and facilitated rapid completion of the survey and data collection.
Setting
The survey was conducted during the Seventh Norwegian Congress in Occupational Therapy, which was organized by the Norwegian Association of Occupational Therapists. The congress took place in Stavanger between the 19th and 21st of September 2022 and was open to both members and non-members, although there was a discount for members. With a population of ∼5.5 million, Norway has about 5200 practicing OTs in hospitals, institutions, and local municipalities, as well as in education and the private sector [Citation8]. In 2022, 3911 were members of the Norwegian Association of Occupational Therapists, of which 171 were specialists within the following seven areas: somatic health (physical diseases and injuries) (n = 101); children’s health (n = 20); mental health (n = 20); general health (n = 12); geriatric health (n = 11); occupational health (n = 6) or public health (n = 1). Since 2020, a general (not related to the specialty area) master’s degree has been a requirement for specialist approval [Citation20]. This means that all OT specialists approved after 2020 have completed a master’s degree, while this will vary among specialists approved before 2020. The Association’s member survey from 2022 shows that 90% of OTs are females [Citation21].
Participants
The target group for the congress was Norwegian OTs, meaning that a diversity of OTs working in clinical practice, education institutions, or research participated. All registered participants at the congress were invited to complete the survey. Surveys submitted within the predefined deadline of a week past the end of the congress were included. Questionnaires completed by people who were not OTs, or from respondents of an uncertain occupation were excluded.
Questionnaire
A survey was developed as there was no existing questionnaire regarding occupational therapy and involvement in research. The survey was modelled according to the Guidelines for visual design of questionnaires (version 1.1), published by Statistics Norway [Citation22]. A first draft was developed by two of the authors (LEH and MH). Thereafter, the draft was discussed by the authors, which are a mix of clinicians, researchers, and OTs working in education. The draft was thereafter adjusted before the questions were tested out among four authors of the study, all OTs. The testing did not prompt any amendments to the questionnaire.
The survey (see Supplement Citation1) contained 14 questions organized in three sections. First, there was a background section, which contained nine questions where respondents reported their gender (female/male); profession (occupational therapist, yes/no); year of completed bachelor’s degree in occupational therapy; place of bachelor education (listing the six occupational therapy educations in Norway and a seventh option ‘abroad’ with a space for describing where); education after completed bachelor’s degree (higher level education after a completed bachelor’s degree, master’s degree or PhD); specialisation (yes/no, and if yes, tick-off one of the seven specialist areas); occupational therapy work experience (in years), service area of practice (primary care/specialist care/education/welfare services/private sector/other); and main patient group or focus (tick-off one of the seven specialist areas).
The next section addressed research involvement and priorities, and contained the following two questions: ‘are you or have you been involved in research’ (yes/no, with a space for description of their research topic); and ‘tick-off your top two prioritized questions for future occupational therapy research from the following list: why do people develop occupational problems (etiology); how many people have occupational problems (prevalence); how can we assess occupational performance (diagnosis); how can we enhance occupational performance (effect of occupational therapy); what is the likely course or outcome(s) of occupational problems (prognosis); how do people experience living with occupational problems (lived experience); and what do we know from previous research about occupational problems and the effect of occupational therapy (reviews), with open space for additional text’.
There then followed a question where respondents were asked to tick-off which of the three following factors would enhance their future participation in research: time; interest; research knowledge and experience; collaboration partners; supervisors; access to updated literature; opportunity for further education; supervision in how to read and understand academic literature in English; support from my leaders; and financial support. In the final open question, respondents were asked to describe what the Norwegian Association of Occupational Therapists should do to promote occupational therapy research.
Data collection
The survey was promoted using a banner stand in the congress area, on flyers, and orally in conference sessions. Participants were given access to the survey by scanning a QR code. Data were collected by using Nettskjema [Citation23], which is a flexible tool designed for the digital collection of data. The website was closed after 1 week.
Data analysis
Descriptive statistics were used to summarise demographic characteristics. Logistic regression models were used to explore associations between being involved with research (dependent variable), site of education, workplace location, number of years with occupational therapy experience, education level, and being a certified OT specialist (independent variables). All models are unadjusted multivariate models. The level of significance was set as 0.05. Statistical analyses were performed using Microsoft Excel 2016 for Windows [Citation24] and Stata 16.1 (STATA Corp., College Station, TX, USA).
The qualitative data concerning involvement in research, research priorities, and the role of the Norwegian Association of Occupational Therapists were analyzed in three steps. Respondents’ statements were copied into three separate documents (one for each open question). A preliminary analysis was carried out separately by two of the authors (LEH and IK), by reading through the comments to identify and code statements concerning involvement, priorities, and the role of the Norwegian Association of Occupational Therapists, respectively. If a comment contained more than one topic or role, each of these were coded separately. Following this, the codes were combined into different categories. Thereafter, the analyses were compared and discussed until an agreement was reached [Citation25].
Ethics
The study adheres to the principles of the Declaration of Helsinki [Citation26] and was approved by the Norwegian Agency for Shared Services in Education and Research (reference number 450236). Participants provided consent by answering the questionnaire. Encrypted data were sent to and safely stored at Services for Sensitive Data (TSD) at the University of Oslo. TSD is an integrated solution for collecting sensitive data and provides a platform where researchers can collect, store, and analyze sensitive research data in a secure environment [Citation27]. After the data is analyzed and published, they will be deleted.
Results
From a total of 633 registered congress participants, 307 (49%) completed the survey. Out of these, four were excluded due to the respondent not being an OT, and one because their professional affiliation was unclear.
Characteristics of the participants
Most participants were female and had a post-bachelor’s degree level of education (see ). The distribution of occupational therapy specialists (n = 56) was as follows; somatic health (n = 36), children’s health (n = 5), geriatric health (n = 4), mental health (n = 4), general health (n = 3), occupational health (n = 3) and public health (n = 1). The participants were educated between 1980 and 2022, with a median of 15 years of working experience (minimum 1.5 months, maximum 42 years).
Table 1. Characteristics of the participating OTs.
Research involvement
Of the 307 respondents, 120 participants (40%) reported having been involved in research, with many reporting having been involved in more than one research project (see ).
Table 2. Involvement in research and factors for enhancing future participation in research reported by participating OTs.
The most frequently reported area of research involvement was rehabilitation (n = 17), including reablement and habilitation. Many also reported being involved in educational research, or with testing psychometric properties and the feasibility of assessment instruments. shows research areas reported by ≥7 respondents.
Figure 1. Research involvement by area of research as reported by respondents. The figure shows areas reported by seven or more respondents. Horizontal numbers refer to responses. Multiple categories were allowed.
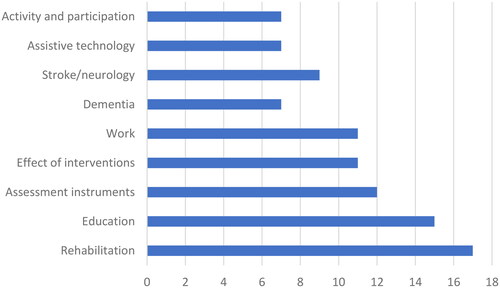
However, many of the responses were difficult to categorize (n = 23). These included research on the involvement of relatives and next of kin, on roles within inter-professional teams, and on knowledge translation and implementation.
Factors associated with involvement in research
presents factors associated with involvement in research. Results show that having completed a bachelor’s degree in occupational therapy in Bergen, Oslo, Trondheim, or abroad, and working in specialist healthcare services, at an education institution or at ‘other’ workplaces were significantly and positively associated with increased involvement in research. Having completed a bachelor’s degree abroad or in Trondheim and working within an educational institution or other sectors showed the strongest associations with involvement in research. Furthermore, years of work experience and education level above a bachelor’s degree were positively associated with increased involvement in research.
Table 3. Logistic regression analysis between predictor variables and the outcome variable (n = 290).
Research priorities
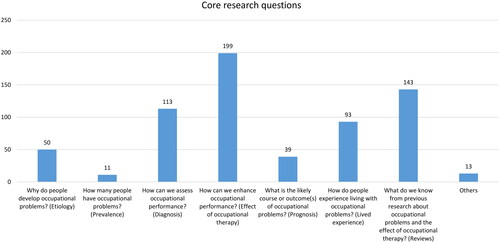
The three most frequently prioritized core research questions were ‘how can we enhance occupational performance (effect of occupational therapy)’; ‘what do we know from previous research about occupational problems and the effect of occupational therapy (literature reviews)’ and ‘how can we assess occupational performance (diagnosis)’ (see ).
Figure 2. Prioritized core research questions reported by respondents. Respondents were encouraged to provide two priorities. Vertical numbers refer to responses given.
A total of 262 (87%) participants commented on priorities for research (see ).
Figure 3. Categories of research priorities (written statements). Multiple categories were allowed. Horizontal numbers refer to responses given.
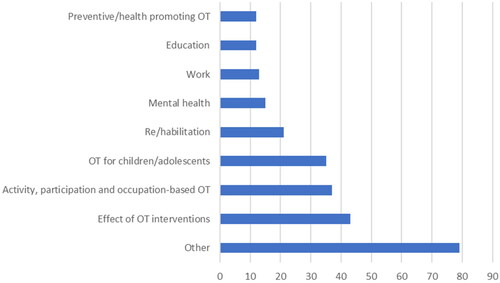
Comments from participants were mostly related to research into the effect of specific occupational therapy interventions; into activity, participation, and occupation-based occupational therapy; and into occupational therapy for children and adolescents. However, the largest category was ‘other’ with 79 written statements or comments. The priorities in this category included the development and organization of (sustainable) occupational therapy services within specialist and primary care (including coordination and cooperation between levels of care); the role of the occupational therapist within different services and settings; occupational therapy for specific patient or diagnostic groups; and content and delivery of specific interventions.
Factors enhancing future participation in research and the role of the Norwegian Association of Occupational Therapists
Time, interest, and collaboration partners were the most frequently cited important factors for enhancing future participation in research (see ).
A total of 166 (55%) participants described one or more roles or tasks that the Norwegian Association of Occupational Therapists could take on to support and/or increase occupational therapy research. Financial support and incentives were by far the most frequently cited role (n = 60), covering both direct financial support or scholarships, supervising members in writing applications for external funding, and supporting members in negotiating full or part-time paid time-off for research or engagement in development projects. Other common suggestions (n = 25) regarded building networks between researchers and clinicians, between different research areas and across levels of care, as well as arranging conferences and digital meetings. Several participants also suggested arranging courses and lectures on research methods (n = 16), and that the Association should help to identify knowledge gaps and point to prioritized areas of research within occupational therapy (n = 13). Among other suggestions were negotiating for higher salaries after completion of additional education, such as a master’s or doctoral degree, and publishing peer-reviewed articles in the Norwegian occupational therapy journal. One respondent suggested establishing a position dedicated to research within the Association itself. Many participants underlined the important role of the Association in supporting research in general and in promoting occupational therapy to politicians and other decision-makers.
Discussion
This survey explored research involvement among Norwegian OTs, factors associated with such involvement, their research priorities, and factors that may enhance their future participation in research.
Research involvement among Norwegian OTs
Evidence-based practice is the gold standard in all healthcare services, including occupational therapy [Citation1,Citation2]. This standard may be easier to comply with for those who already have knowledge of and experience from participating in research [Citation3]. The finding that 40% of the participants in this study were involved in research is therefore uplifting, as previous research shows that such involvement is likely to improve health care performance [Citation3]. Rehabilitation was the most frequently reported area of research. This may reflect the fact that rehabilitation is a statutory task where OTs are given an important role, whether they work in a primary or specialized healthcare setting, or in the Norwegian Labour and Welfare Organisation (NAV). Rehabilitation aims to help people become as independent as possible in everyday activities and enables participation in meaningful life roles [Citation28]. This is in line with the core competence in occupational therapy [Citation29] and is therefore probably easily adopted by OTs. Furthermore, the high proportion of OTs involved in rehabilitation research may also be explained by the recent implementation of reablement in Norway [Citation30]. Here, OTs are an integral part of the inter-professional team, and many have also been involved in research undertaken to evaluate the programme [Citation30]. These findings show that national initiatives provide opportunities for OTs who would like to participate in research.
Factors associated with research involvement
High research involvement in our study was positively associated with working within an educational institution or specialist healthcare setting, whereas working in primary care was negatively associated with such involvement. This may be explained by the fact that conducting research is a statutory task for universities [Citation31] and hospitals [Citation32], whereas this is not the case for primary healthcare services [Citation33]. Consequently, employees in the former institutions have easier access to financial incentives and a greater acceptance of prioritizing research activities, whereas this may not be the case for OTs working in primary care. Still, it is stated in The Health&Care21 strategy [Citation34], that healthcare research efforts directed towards primary healthcare services are not proportionate to the challenges and significant amounts of public resources used in primary health care services. Furthermore, it is pointed out that an increased and long-term investment in primary care research is needed, and that future studies should be conducted in collaboration with other research actors, especially higher education institutions [Citation35]. In line with this, OTs in primary care are often important partners in research initiated at universities and hospitals, and such collaboration is frequently recommended [Citation11,Citation14,Citation15]. Hopefully, future research projects will be initiated to a greater extent by OTs in primary healthcare services.
As expected, involvement in research was positively associated with more work experience and further education after completing a bachelor’s degree. In line with previous research, it can be assumed that more work experience and a higher level of education both increase individual competence and the self-confidence needed to participate in research [Citation36,Citation37]. In addition, a larger network can lead to more opportunities for research involvement [Citation37]. This should act as an incentive for decision-makers to facilitate further education, especially among OTs in primary healthcare services.
An unexpected finding of this survey was the lack of association between being a specialist OT and involvement in research. However, we may be at a turning point regarding this as this study found that higher education was associated with being involved in research, and a master’s degree is now a prerequisite to becoming a specialist OT. Furthermore, higher levels of education may also promote curiosity and reflection and enhance clinicians’ ability to comply with evidence-based practice [Citation3].
Priorities in research
In line with international research priorities, participants in our study highlight the need to investigate the effectiveness of occupational therapy interventions [Citation11,Citation12]. Being able to demonstrate the effect of occupational therapy interventions is not only important for engaging with informed patients and their next of kin, but also for negotiations with decision-makers and when cutbacks need to be made, where showing significant results can be perceived as a weighty argument. Considering the likely scenario of a healthcare service with fewer employees per patient [Citation9], it seems vital for OTs to be able to demonstrate the effect of their interventions. The participants in our study expressed a strong preference for researchers to prioritize systematic reviews. Given the competing demands between patient care and professional development, there is a perceived need for time-efficient access to summarised knowledge. Reviews offer valuable contributions by providing a comprehensive overview that incorporates multiple perspectives and offers clear recommendations for both clinical practice and future research [Citation35]. Participants who commented on research priorities also highlighted research on activity, participation, and occupation-based occupational therapy as being important. These themes may reflect the fact that the participants are familiar with and concerned about the current activity paradigm in our profession [Citation38].
Factors enhancing OTs involvement in research
Participants in our study reported that having time, interest, collaboration partners, financial support, support from leaders, and access to supervisors or supervision were factors that would help to increase their involvement in research (see ). Similar findings have been reported by other researchers. Di Bona et al. [Citation4] argued that OTs’ involvement in research was enabled by having specifically allocated time for research, positive attitudes, and support. Based on a qualitative study conducted by Dwyer et al. in Ireland [Citation18], the authors observed that OTs involvement in research depended on their interest in the topic under investigation and their desire to enhance their skills in that area.
Moreover, a number of the participants in our study also stated that having the opportunity to pursue further education, and to gain further research knowledge and experience, having access to up-to-date literature, and supervision in how to read and understand academic literature in English language were factors that would enable or enhance future involvement in research activities. The responses in our study align with the research engagement strategies recently proposed by Yoong et al. [Citation37] aimed at increasing healthcare providers and healthcare organizations’ engagement in research activities. They provided the following list of research engagement strategies in their scoping review: (i) dual skilled team/staff, (ii) resources or physical infrastructure, (iii) incentives, (iv) leadership support of research, (v) education/training, (vi) networks, (vii) forming partnerships or collaborations, and (viii) overall leadership structure of entity.
Many respondents in our study requested support from the Norwegian Association of Occupational Therapists. This indicates that there are unmet needs when it comes to different forms of support for Norwegian OTs. Considering that the primary task of the Association of Occupational Therapists is aimed at improving OTs’ profession and working conditions, it is not surprising that many of the respondents expressed the need for financial support for research and development. Such opportunities are in accordance with services offered by similar Norwegian professional associations, for example, for nurses or physiotherapists.
Besides financial support, the results indicate that a greater commitment by the Association to facilitate occupational therapy research through various incentives may enhance OTs’ participation in future research projects. This could, for instance, be achieved by establishing various networks or fronting research on different occasions. As a further commitment, one of the respondents suggested establishing a position within the Association of Occupational Therapists dedicated to research activities. As far as we know, this is not common practice in this type of organization. However, due to the increasing need to prioritize the most effective interventions [Citation9], it may be crucial to front both professional development and research. Even though we asked the respondents what the Norwegian Association of Occupational Therapists could do to promote opportunities for research, the responses also reflected unmet needs that may be met by other bodies, such as healthcare or educational institutions.
Methodological considerations
Our study has several strengths and limitations. One strength is that the results reflect opinions from a wide spectrum of OTs, ranging from the newly graduated to the retired. Although the gender composition aligns with the membership base of the Norwegian Association of Occupational Therapists, it would be desirable to have more male respondents as they may bring different research priorities and experiences to the table.
Furthermore, by asking congress participants who have prioritized finances and the time for professional replenishment, we may get answers from a selection of OTs who are particularly concerned with research and professional development. This bias may have contributed to the high proportion of participants with research involvement in our study. For those involved in research, we have no information on what proportion of their working time was used for research. Compared with the general membership of the Norwegian Association of Occupational Therapists, where the largest proportion of OTs are employed in primary healthcare services [Citation21], a relatively high proportion of the participants in our study were from specialist healthcare services (30%). This may have camouflaged important priorities of a significant group of OTs within primary healthcare. These biases limit the generalization of the findings to a broader population of OTs.
Another limitation is the questionnaire itself, which was developed specifically for this study, meaning it was neither standardized nor validated for its purpose. It was, however, designed in accordance with current guidelines for designing questionnaires [Citation22] and was also tested by OTs (n = 4). The questions and response options were considered relevant and easy to understand, meaning no amendments were needed before initiating the main study. However, essential terms, such as research and research involvement were not pre-defined or explained to the respondent. Instead, we left it up to each individual respondent to define their own understanding of the questions asked. This means that we cannot be sure that respondents had a common understanding of these terms. The results of the study must be interpreted with care. The relatively high response rate of 49% may be explained by the use of a QR code, which provided easy access to the survey, as well as the fact that we did not collect any data that could be used to identify the participants.
Conclusions
The survey revealed that a considerable, yet uneven, distribution of OTs is involved in research, with rehabilitation being reported as the most common area of research. Factors positively associated with research involvement were working within education or specialist healthcare, more work experience, and further higher education beyond a bachelor’s degree. Factors that enhanced involvement were time, interest, collaboration partners, financial support, support from leaders, and access to supervisors. The number one research priority was research on the effects of occupational therapy, followed by systematic reviews and assessment instruments. There are several measures that researchers, decision-makers, and employee associations can take to encourage increased participation in research, such as providing financial support, time off from clinical practice, and financial rewards for research experience.
Implications to practice
This study draws attention to the skewed distribution of research involvement within the field of occupational therapy. We suggest closer cooperation between OTs across professional areas and sectors, and a cooperation in which researchers are encouraged to take responsibility. We also encourage decision-makers, especially in primary healthcare services to facilitate further education beyond a bachelors’ degree. Decision-makers should also pay more attention to and prioritize improving factors that will enhance OTs’ participation in research.
Supplemental Material
Download MS Word (23.8 KB)Acknowledgements
We thank the OTs who responded to the survey and shared their opinions with us. We would also like to thank researcher Anne Therese Tveter for setting up the technical solution for data collection.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Rappolt S. The role of professional expertise in evidence-based occupational therapy. Am J Occup Ther. 2003;57(5):1–11. doi: 10.5014/ajot.57.5.589.
- Sackett DL, Rosenberg WMC, Gray JAM, et al. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71–72. doi: 10.1136/bmj.312.7023.71.
- Newington L, Wells M, Adonis A, et al. A qualitative systematic review and thematic synthesis exploring the impacts of clinical academic activity by healthcare professionals outside medicine. BMC Health Serv Res. 2021;21(1):400. doi: 10.1186/s12913-021-06354-y.
- Di Bona L, Wenborn J, Field B, et al. Enablers and challenges to occupational therapists’ research engagement: a qualitative study. Br J Occup Ther. 2017;80(11):642–650. doi: 10.1177/0308022617719218.
- Bennett S, McKenna K, McCluskey A, et al. Evidence for occupational therapy interventions: effectiveness research indexed in the OTseeker database. Br J Occup Ther. 2007;70(10):426–430. doi: 10.1177/030802260707001003.
- Steultjens EM, Dekker J, Bouter LM, et al. Evidence of the efficacy of occupational therapy in different conditions: an overview of systematic reviews. Clin Rehabil. 2005;19(3):247–254. doi: 10.1191/0269215505cr870oa.
- Bonsaksen T, Dolva AS, Hagby C, et al. Involvement in research and development projects among community-working occupational therapists in Norway. Occup Ther Health Care. 2019;33(1):22–36. doi: 10.1080/07380577.2018.1526434.
- Ness NE, Horghagen S. Ergoterapi i hundre år. Ergoterapeuten. 2017;5:36–42.
- NOU. 4 Tid for handling. Personellet i en bærekraftig helse- og omsorgstjeneste. Oslo: Helse- og omsorgsdepartementet; 2023.
- Watson J. Research priorities for occupational therapy in the UK. Br J Occup Ther. 2021;84(1):3–5. doi: 10.1177/0308022620976834.
- Mackenzie L, Coppola S, Alvarez L, et al. International occupational therapy research priorities. OTJR. 2017;37(2):72–81.
- Watson J, Cowan K, Spring H, et al. Identifying research priorities for occupational therapy in the UK: a james lind alliance priority setting partnership. Br J Occup Ther. 2021;84(12):735–744. doi: 10.1177/03080226211026557.
- Chalmers I, Glasziou P. Avoidable waste in the production and reporting of research evidence. Obstet Gynecol. 2009;114(6):1341–1345. doi: 10.1097/AOG.0b013e3181c3020d.
- Meld. St. 18 (2012–2013). Long-term perspectives-knowledge provides opportunity. Oslo: Ministry of Education and Research; 2013.
- Meld. St. 16 (2020–2021). Utdanning for omstilling-Økt arbeidslivsrelevans i høyere utdanning. Oslo: Kunnskapsdepartementet; 2021.
- Mayers CA, Nilsson ÅL, Stamm T, et al. Survey of occupational therapy/occupational science research being undertaken within the european community. Br J Occup Ther. 2008;71(1):17–22. doi: 10.1177/030802260807100104.
- Laustsen CE, Petersson P, Westergren A, et al. Involvement of professionals in research: knowledge integration, development of practice, and challenges: a group concept mapping study. Health Res Policy Syst. 2021;19(1):115. doi: 10.1186/s12961-021-00763-5.
- Dwyer CP, Keane A, Casey D, et al. A qualitative investigation of influences on occupational therapists’ research involvement in Ireland. Br J Occup Ther. 2023;86(4):320–330. doi: 10.1177/03080226221136812.
- Sharma A, Minh Duc NT, Luu Lam Thang T, et al. A consensus-based checklist for reporting of survey studies (CROSS). J Gen Intern Med. 2021;36(10):3179–3187. doi: 10.1007/s11606-021-06737-1.
- Ergoterapeutene. Ergoterapeutenes spesialistordning [Internett]. [updated 2021 Apr; cited 2023 Jun 6]. Available from: https://ergoterapeutene.org/spesialist/
- Ergoterapeutene. Lønnsundersøkelsen. 2022. Oversikt over medlemmenes lønns- og arbeidsforhold 2022 [updated 2023 Jun 2; cited 2023 Jun 6]. Available from: https://ergoterapeutene.sharepoint.com/:b:/g/ER3i-x9PQnhKiOeUYljItc4BAdnbBgV2TUeaGRsR1lPpIA?e=bKsPO1
- Statistics Norway. Retningslinjer for visuell utforming av spørreskjema [Guidelines for visual design of questionnaire]. Oslo; Kongsvinger: Statistisk sentralbyrå; Statistics Norway; 2007 [cited 2023 Jun 6]. Available from: https://www.ssb.no/a/histstat/ssh/ssh_88.pdf
- University of Oslo. Nettskjema [Internet]. [updated 2023 Mar 10; cited 2022 May 12]. Available from: https://www.uio.no/english/services/it/adm-services/nettskjema/
- Microsoft Cooperation. Microsoft Excel; 2016.
- Kvale S, Brinkmann S. Det kvalitative forskningsintervju [The qualitative research interview]. 3rd ed. Oslo: Gyldendal Akademisk; 2015.
- World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
- University of Oslo. Services for Sensitivve Data (TSD) [Internet]. [updated 2023 Jun 6; cited 2023 Jun 6]. Available from: https://i.ntnu.no/wiki/-/wiki/English/TSD+-+Services+for+Sensitive+Data#:∼:text=TSD%20is%20a%20secure%2C%20private%20cloud%20with%20a,researchers%20at%20several%20national%20research%20institutions%2C%20including%20NTNU
- World Health Organization. Rehabilitation 2023 [Internet]. [updated 2023 Jan 30; cited 2023 Jun 6]. Available from: https://www.who.int/news-room/fact-sheets/detail/rehabilitation
- Townsend E, Polatajko H. Enabling occupation II: advancing an occupational therapy vision for health, well-being. 2nd ed. Ottawa: CAOT; 2013.
- Langeland E, Førland O, Aas E, et al. Modeller for hverdagsrehabilitering- en følgeevaluering i norske kommuner. Bergen: Senter for omsorgsforskning; 2016.
- Univerity- and University Colleges Acts. Act relating to universities and university colleges of 2019-06-21 nr 61; 2005.
- Spesialisthelsetjenesteloven. Lov om spesialisthelsetjenesten m.m. 1999. av 1999-07-02 nr 61.
- Helse- og omsorgstjenesteloven. Lov om kommunale helse- og omsorgstjenester m.m. 2011. av 2011-06-24 nr 30.
- Helse- og omsorgsdepartementet. HelseOmsorg21. Et kunnskapssystem for bedre folkehelse. Nasjonal forsknings- og innovasjonsstrategi for helse og omsorg. Oslo: Helse- og omsorgsdepartementet; 2014 [cited 2023 Jun 6]. Available from: https://www.helseomsorg21.no/Om-HelseOmsorg21/strategien/
- Aromataris E, Pearson A. The systematic review: an overview. Am J Nurs. 2014;114(3):53–58. doi: 10.1097/01.NAJ.0000444496.24228.2c.
- Pighills AC, Plummer D, Harvey D, et al. Positioning occupational therapy as a discipline on the research continuum: results of a cross-sectional survey of research experience. Aust Occup Ther J. 2013;60(4):241–251. doi: 10.1111/1440-1630.12057.
- Yoong SL, Bolsewicz K, Reilly K, et al. Describing the evidence-base for research engagement by health care providers and health care organisations: a scoping review. BMC Health Serv Res. 2023;23(1):75. doi: 10.1186/s12913-022-08887-2.
- Hammel KRW. Engagement in living. Critical perspectives on occupation, rights, and wellbeing. Ottawa: Candian Association of Occupational Therapists; 2020.