
Abstract
The presented study deals with the relations between the economic life of developed countries and the health of women and men. The primary objective of the presented study was to assess the relations between gender health inequalities and economic productivity in a sample of OECD countries, with a focus on the classification of their health care systems. Analyses included selected causes of mortality as health variables, each in a specification of men and women, and economic productivity represented by Gross Domestic Product (GDP) per person employed (in USD at current prices). The health care systems were represented by multiple insurance model (MI), national health system (NHS) and single payer model (SPM). The analysed data were collected from OECD databases for the period from 2011 to 2016. The analytical processing was carried out by applying descriptive analysis, regression analysis examining the effects of gender inequalities in health on economic productivity, and relationship analysis. Based on the findings, it can be stated that the vast majority of gender inequalities in health is significant. Also, it has been confirmed that gender inequalities in health have an effect on economic productivity. In general (with a few exceptions), it can be concluded that if gender inequalities in health are reduced, economic productivity is expected to increase. From the point of view of the analysed relations, the NHS health care system can be considered the most positive.
1. Introduction
A healthy population is the driving force of every economy; therefore, health is at the heart of public policies around the world (WHO, Citation2002). Many international organizations, such as the OECD or the WHO, make recommendations to individual countries to raise the level of population’s health and reduce health inequalities. This effort focuses on the responsibility of countries that should be proactive in the field of public health, which reflects the maturity of countries. International organizations recommend economies to focus on the effective management of their health care systems that are able to deliver effective health care (OECD, Citation2019; WHO, Citation2013). Subsequently, the effective health care reflects an increased level of population health. Improvement of population’s health in terms of increased life expectancy and reduced mortality is reflected in an increased economic value of health capital, which brings economic gains (Murphy & Topel, Citation2006). These facts highlight the importance of health in the economic dimension, and equally important is the area of health inequalities (Deaton, Citation2003; Woodward & Kawachi, Citation2000), which appear to be a significant economic factor for the prosperity of countries. For this reason, the present study deal with the relations of gender health inequalities and economic productivity in OECD countries.
2. Literature review
The area of health care is a topic that was analysed in many different dimensions, e.g. from the perspective of health care financing (Haseeb et al., Citation2019; Stefko et al., Citation2017), performance of health care systems (Łyszczarz, Citation2016) or health care in the light of the concept of welfare state regimes (Kawiorska, Citation2016). At the current stage of development of the world economy, attention is focused on public health in terms of economic condition. The relation between economy and health was investigated by quite many authors. Population health is a significant factor that affects the economic productivity and income (Sharma, Citation2018), as good health has a positive and statistically significant impact on the aggregate output of economies (Bloom et al., Citation2004). For this reason, it is very important to focus on public health from the economic point of view.
With regard to mortality as a relevant health indicator, it can be emphasized that mortality causes obvious economic losses (Kozlova et al., Citation2017), thus reducing mortality can bring economic benefits, such as the saved years of productive life of the population (Boisclair et al., Citation2018). The longevity of the population is a reflection of mortality in a country, and even in this case it is possible to see a connection with economic life of countries. Boachie (Citation2017) confirmed that good health represented by life expectancy has a significant and positive impact on real GDP. Significant gender inequalities in longevity were identified and confirmed by many authors such as Bai et al. (Citation2018), Belon et al. (Citation2014), Clark and Peck (Citation2012), Sandiford (Citation2009) or Van Oyen et al. (Citation2010). The fact that women show more positive outcomes in life expectancy is well known (Andrade et al., Citation2011; Haeberer et al., Citation2015). The findings revealed that women live longer than men, while men's higher mortality from cancer, circulatory and respiratory diseases appeared to be a major contributor to this gender gap (Le et al., Citation2015). Despite the female advantage in longevity, evidence showed a higher loss in quality-adjusted life years of women. Therefore, men die earlier, but those who live longer are healthier than women (Zhang et al., Citation2016). Jacobs et al. (Citation2014) revealed that the increased longevity of women aged 70 years gradually decreases with advancing age, and disappears after 90 years. On the other hand, gender inequality in longevity has decreased over time and the gender gap is expected to close (Mayor, Citation2015; Megyesiova & Lieskovska, Citation2018). In terms of men's shorter lives, it is possible to point out their higher mortality rates. In general, gender differences in mortality are evident (Liang et al., Citation2003) and women have the advantage of lower mortality (Singh-Manoux et al., Citation2008). Ross et al. (Citation2012) agreed that male mortality is higher than female mortality, and suggested that education may be a factor that lead to close the gender gap in mortality. Gender inequalities in mortality were evidenced not only in the case of all-cause mortality, but also in the case of specific categories of mortality such as cancer (Ellison, Citation2016; Fernandez et al., Citation2000; Kubak et al., Citation2017), asthma, ACOS (asthma-COPD overlap syndrome) and COPD (chronic obstructive pulmonary disease) mortality (Barnes et al., Citation2016). In all cases, the results were more positive for women. The differences in stroke mortality are not clear, women under the age of 75 had a lower risk of stroke, but after that age women lost their advantage (Meirhaeghe et al., Citation2018). Ayala et al. (Citation2002) confirmed the similar findings. In any case, health inequalities are evident in the world and need to be addressed.
At this point, it can be emphasized that health inequalities can be caused by many economic, social, environmental and other factors (Mackenbach et al., Citation2008; Richardson & Mitchell, Citation2010). The financing of the health care system and its efficiency can also be a key factor influencing the health status of the population, the distribution of health care, as well as the inequalities in health (Golinelli et al., Citation2018; Obrizan & Wehby, Citation2018). Ozcan and Khushalani (Citation2017) highlighted the need to improve health care systems, while their evidence reveals the fact that improved health care systems appear to be more efficient, which may be reflected in health outcomes. At the same time, Shuaibu and Oladayo (Citation2016) emphasized that investment in health sector influences the development of human capital in countries. All these aspects represent the level of maturity of countries, which can cause endogenous problems that should not be overlooked when examining health in the economic dimension.
Based on the above-mentioned findings, it is possible to highlight the importance of examining the health inequalities in the economic dimension (Costa-Font & Hernandez-Quevedo, Citation2012; Pacáková & Kopecká, Citation2018). Health inequalities are a much-discussed topic that has been investigated from different views, such as social ecology perspective (Kim & Kim, Citation2018), socioeconomic perspective (Mackenbach et al., Citation2011; Politzer et al., Citation2019) or racial perspective (LaVeist et al., Citation2011). Weil (Citation2007) argued that reducing health inequalities among countries would reduce the variance of economic productivity. Politzer et al. (Citation2019) highlighted the economic impact of socioeconomic health inequalities on economic aspects such as GDP and health care expenditure. Similar evidence was found by Mackenbach et al. (Citation2011), who revealed that the costs of socioeconomic health inequalities are one of the major economic burdens in European countries and reflect the economic losses in labour productivity and GDP. Reducing racial inequalities in health may also have a positive effect on the economic condition in terms of increasing economic savings and decreasing direct and indirect costs (LaVeist et al., Citation2011; Nanney et al., Citation2019).
These facts underline the importance of examining the gender inequalities in health in the economic dimension and also encourage policy makers' efforts to address the effect of gender health inequalities on the economic prosperity. If a country is unable to correctly identify the relationship between the health of the population and the economy, it cannot properly manage its economic development and raise the living standards. At the same time, it is important to take into account the applied health care system when examining public health in different countries, as each system is based on different funding principles, uses different forms of health care coverage and achieves different health care efficiencies (Ahmed et al., Citation2019; Cylus et al., Citation2018; Van der Zee & Kroneman, Citation2007). Therefore, the uniqueness of health care systems represents a significant element and the differentiation of health systems offers more specific and practical implications for individual countries that cope with different conditions.
All the above-mentioned facts were the inspiration for the presented research, which focuses on gender inequalities in health, economic productivity and individual health care systems in an effort to provide a comprehensive picture of the whole issue.
3. Materials and methods
3.1. Research objective
The primary objective of this study was to assess the relations between gender health inequalities and economic productivity in a sample of OECD countries, with a focus on the classification of their health care systems. This objective was achieved through several analytical processes, while a descriptive analysis was performed in the first step in order to understand the variables in more detail. This was followed by the main part of the analytical processing, i.e. regression analysis examining the effects of gender inequalities in health on GDP in the classification of individual health care systems. The last analytical part consisted of a relationship analysis carried out in order to provide a comprehensive picture of the issue under investigation.
3.2. Data and sample
Data from OECD databases entered into analyses, these data were collected from the Health and Productivity sub-databases (OECD, Citation2020a). The analysed data included selected causes of mortality (CM) as health variables specified in the classification of men and women, economic productivity represented by GDP per person employed (in USD at current prices) as an economic variable, followed by variables determining health insurance coverage and health care systems.
The health care system variable classifies the analysed countries into three main categories, namely a multiple insurance system (MI), a national health system (NHS) and a single payer model (SPM) (OECD, Citation2016). The health group of CM consisted of 13 variables (each in male and female specification), namely certain infectious and parasitic diseases (INF), neoplasms (CNC), blood diseases and blood forming organs (BLD), endocrine nutritional and metabolic diseases (END), mental and behavioural disorders (MNT), diseases of the nervous system (NRV), diseases of the circulatory system (CRC), diseases of the respiratory system (RSP), diseases of the digestive system (DGS), skin and subcutaneous tissue diseases (SKN), diseases of the musculoskeletal system and connective tissue (MSC), diseases of the genitourinary system (GNT), certain conditions originating in the perinatal period (PNT). All CM variables were reported in deaths per 100,000 population in standardised rates. These variables can be defined as age-standardised death rates per 100,000 population for selected causes that are calculated by the OECD Secretariat, using the total OECD population for 2011 as the reference population (OECD, Citation2020b).
The analyses covered 35 OECD countriesFootnote1, with the exception of Sweden, as this country has a specific health care system. Due to the large number of missing data, the most recent data were from 2016 and the oldest from 2011.
3.3. Description of analytical processing
The analytical processing to achieve the main objective of this study was divided into several parts. The first part consisted of a descriptive analysis, which includes commonly used statistical indicators. The second part was devoted to determining the effects by a simple regression analysis, using the ordinary least squares (OLS) regression model and the instrumental variables (IV) regression model. The homogeneity of residue variability (homoscedasticity) was verified by the Breusch-Pagan Test. If the assumptions were met, a multiple linear regression model was used. If there was a significant heteroscedasticity, the coefficients were estimated using a robust estimator (White, Citation1980, Citation1982). Subsequently, an analysis of relationships was performed using a non-parametric method of Spearman correlation coefficient ρ.
The analytical data were processed in SPSS v. 23 (IBM, Inc., Armonk, NY, U.S.) and programming language R v. 3.6.1 (nickname: Action of the Toes) in R Studio (Rstudio, Inc., Boston, MA, U.S.).
4. Results
This section of the study deals with the analytical process and includes descriptive analysis, regression analysis and relationship analysis in separate parts.
4.1. Descriptive analysis
The following shows the basic outputs of descriptive analysis of selected health variables. The variables determine the causes of mortality in the individual diagnosis groups. This analysis pointed to selected statistical characteristics of mortality per 100,000 population in categories such as gender specification and gender inequalities in mortality, while these inequalities were described in the classification of health care systems.
Table 1. Gender differences in health – basic statistical characteristics.
The results in can be interpreted as follows. The INF variable provides a value for both women (mean = 11.28) and men (mean = 16.64) with a difference of 5.49, explaining that women die from certain infectious and parasitic diseases by an average of 5.49 (per 100,000 population) less than men. Other variables can also be interpreted in this way. In almost all cases of gender differences, significant inequalities with more positive outcomes for women can be considered. In the variables SKN (mean: male = 1.57; female = 1.64) and MSC (mean: male = 3.42; female = 4.51), women showed a higher (i.e. more negative) value, but no significant difference was found in SKN.
Gender inequalities in the classification of individual health care systems were also assessed. Based on the results, it can be stated that individual countries have specific predispositions for a more frequent incidence of specific types of diseases. These predispositions can be explained from various perspectives, in which sociological, economic, cultural and historical aspects play an important role, while the health care system is also important but not dominant. In terms of individual diagnosis groups of mortality, the highest number of maximum mean values was found in the SPM system (N = 7; MNT, NRV, CRC, RSP, DGS, CNC, PNT), followed by the MI system (N = 4; INF, END, SKN, GNT) and the lowest number of maximum mean values was identified in the NHS system (N = 2; BLD, MSC).
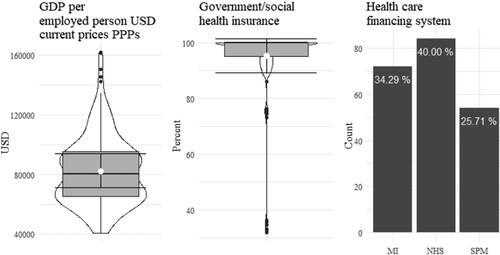
shows the basic statistical characteristics of GDP per person employed as a dependant variable, as well as the characteristics of the variable representing government/social insurance as an instrument variable in a regression model, and the variable determining the ratio of individual health care systems. The white dot symbolizes the mean, the horizontal line inside the boxplot represents the median level, the horizontal lines extending the boxplot (error bar) show the range of standard deviation, and the dark dots represent the outliers. During the analysed period, the average value of GDP in OECD countries was approximately equal to 39451.76 (median = 37330.89; CI 95% = 37396.28-41507.25; SD = 15326.44), and the mean of government/social insurance (%) was 95.29 (median = 100; CI 95% = 93.54-97.05, SD = 12.27). The absolute frequency was 72 for the MI system, 84 for the NHS system, and 54 for the SPM system.
Figure 1. Basic statistical characteristics of selected variables (GDP per person employed, health insurance coverage, health care systems).
Source: own processing
4.2. Analysis of the effects of gender inequalities in selected health indicators on economic productivity in individual health care systems
This part of the analytical process is devoted to assessing the effects of gender inequalities in selected causes of mortality on economic productivity represented by GDP per person employed. The instrumental variables (IV) regression method was used to determine the effects. In the first step, the variability of constant residues was evaluated and then selected diagnostic tests of the regression model of instrumental variables (IV) were used.
provides the output of the heteroscedasticity testing, and if the p-value was less than 0.05, a significant presence of heteroscedasticity could be confirmed and a robust HCl estimator was considered appropriate for estimation.
Table 2. Homoscedasticity test outputs.
shows the basic diagnostic tests of the IV regression method. The null statistical hypothesis of the Weak Instruments (WI) test speaks of weak instruments and it is clear that this hypothesis was rejected and its alternative was accepted in most cases of the MI and NHS systems. In contrast, the p-value of the WI test was higher than 0.05 as well as 0.1 in most cases of the SPM system; therefore, strong instruments cannot be considered in these cases. The null hypothesis of the second diagnostic test, the Wu-Hausman test (WH), speaks of the similarity of the OLS and IV models. Obviously, not all the tests showed optimal values. This result can be considered as a certain limitation of the study, which is especially evident in the SPM system.
Table 3. Diagnostic tests of IV regression model.
provides the results of first stage regression, which is one of the assumptions for the application of IV regression. In most cases, a significant rate of effect was identified, which can be assessed positively in terms of IV assumptions. However, especially in the NHS system, it is possible to see a higher number of observations, in which the effects of the instruments were not significant. This deficiency can be considered as a limitation of the study.
Table 4. First stage regression: effect of health insurance coverage on gender inequalities in selected health variables.
shows the results of the evaluation of the effects of gender inequalities in selected variables that determine the causes of mortality on economic productivity, while all three health care systems were included in the interpretations of this table.
Table 5. Regression analysis outputs.
With a focus on gender inequalities in INF in the MI system, a significant effect was identified by the OLS model. On the other hand, based on the previous diagnostic tests, it is recommended to take into account the IV model, in which no significant effect was found. Regarding the NHS system, both regression models identified a significant and inverse effect (β OLS = −2444.21***; β IV = −2131.50***). In contrast, in the case of the SPM system, none of the models found a significant effect of gender inequalities in INF.
Focusing on gender inequalities in CNC, significant effects were confirmed in all cases, with the exception of the MI system in the OLS regression model. The output of diagnostic tests indicates that in this case, the IV model appears to be more reliable in determining the effect, and thus the significance is evident from the given table (MI β IV = −545.45**). All three health care systems showed significant and negative β coefficients, which can be seen in a positive context, as this indicates that reducing gender inequalities in CNC can lead to an increased economic productivity.
The diagnostic testing of the BLD group was slightly indeterminate, which supports the OLS model as more appropriate for assessing effects, as the diagnostic tests revealed a weak instrument. A significant and inverse effect was found in the MI system (β OLS = −31788.93***), no significant effect was observed in the NHS system, and a significant effect with a positive coefficient was identified in the SPM system using the OLS model (β OLS = 29501.00***), while the IV model showed no significance.
Based on the diagnostic tests, it is recommended to consider the IV regression model in the case of gender inequalities in END. In all three health care systems, the IV model showed significant and positive effects of gender inequalities on economic productivity, indicating that increased gender inequalities in END may lead to an increased productivity.
A significant effect of gender inequalities in MNT was proved by the IV model only in the NHS system (β IV = 10088.16***). Based on the positive coefficient, it can be concluded that an increase in gender inequalities in MNT may lead to an increase in economic productivity.
According to the diagnostic tests, it is recommended to take into account the OLS model in the case of gender inequalities in NRV, as endogeneity does not appear to be a significant problem. It is not possible to confirm a significant effect in the MI system; on the contrary, a significant and inverse effect was found in the NHS system (β OLS = −3204.56***), indicating that economic productivity is expected to increase while reducing gender inequalities, which can be considered positive. Also, a significant effect with a positive coefficient (β OLS = 2610.91*) was identified in the SPM system, but it should be considered with some caution, as significance can be seen only at the α level equal to 0.1.
Based on the diagnostic tests, the effect of gender inequalities in CRC should be considered with some degree of uncertainty in the MI system. On the other hand, significant and inverse effects were clearly confirmed in the NHS and SPM systems, indicating that productivity gains can be expected with reduced gender inequalities in CRC.
According to the diagnostic tests, it is recommended to consider the IV regression model in the case of gender inequalities in RSP, while significant and inverse effects were found in the MI and NHS systems (MI β IV = −1152.11**; NHS β IV = −1258.78***), no significant effect was confirmed in the SPM system.
Also, significant and inverse effects of gender inequalities in DGS were identified in the NHS and SPM systems. The MI system is slightly inconsistent and, based on the diagnostic tests, it is more appropriate to take into account the OLS regression model, which showed a significant effect with a negative coefficient (β OLS = −1242.17***).
In the case of gender inequalities in SKN and GNT, significant and inverse effects were found in the MI and NHS systems. On the other hand, in the SPM system, it is not possible to confirm a significant effect in these diagnosis groups.
Gender inequalities in MSC and PNT were not considered to be dominant in economic productivity changes. Based on the diagnostic tests, a significant and positive effect of gender inequalities in MSC was found in the NHS system. In the countries applying this system, an increase in economic productivity can be expected with an increase in gender inequalities in this diagnosis group. The last diagnosis group, PNT, cannot be considered significant in terms of the effects on economic productivity.
4.3. The relationship between gender health inequalities and economic productivity
The analysis in this part focuses on the assessment of the relationships between economic productivity represented by GDP per person employed and gender inequalities in selected health variables that determine the causes of mortality. The assessment of the relationships was carried out using a non-parametric method of Spearman’s ρ. The previous part of the analytical process presented the analysed issue in a specific perspective, i.e. in the classification of health care systems. A comprehensive view (without the classification) can be considered at least beneficial to the general perspective of the issue.
shows the output of the analysis of relationships. Based on the results, it was possible to confirm a significant relationship between gender inequalities in several health variables and GDP per person employed (in USD at current prices). The p-value higher than 0.05 was identified in six cases (BLD, END, MNT, NRV, SKN, MSC), in which a significant relationship could not be confirmed. The results show both positive and negative coefficients, thus it is necessary to pay attention to this when interpreting. The highest strength of relationships (substantial to very strong) was found in variables such as RSP (ρ = −0.509) and DGS (ρ = −0.636). These variables showed a negative coefficient. Therefore, an increased economic productivity may be associated with a reduction in gender inequalities in these health variables.
Table 6. Relationships (ρ) between economic productivity and gender inequalities in selected health variables.
5. Discussion
The purpose of running public health is to achieve equality in health, which demonstrates the ability of an individual to fulfil a health potential (i.e. the highest level of health) without disadvantages. For this reason, health inequality is a very topical global issue (Costa-Font & Hernandez-Quevedo, Citation2012; Deaton, Citation2003; Pacáková & Kopecká, Citation2018), while identifying and understanding the relations between health inequalities and economic outcomes are considered to be an important aspect in economic decision-making. The presented study offers a very interesting insight into the economic dimension of relations between gender inequalities in health and economic productivity.
The first step of the analytical processing was devoted to the application of descriptive analysis showing the basic characteristics (number, mean, median, standard deviation). This analysis pointed to the average characteristics of mortality per 100,000 population in categories such as gender specification and gender inequalities in mortality, while these inequalities were described in the classification of health care systems. Regarding the causes of mortality, the highest value of the difference was found in the CNC diagnosis group. Based on the results, it can be concluded that women die from neoplasms by an average of 114.24 deaths (per 100,000 persons) less than men. This can be explained by the fact that men have a higher incidence of cancer risk factors, especially smoking. The hectic lifestyles of men, their poor nutrition, overweight, physical inactivity or stress lead to an increased risk of cancer and other critical diseases. Simultaneously, other studies also observed excessive mortality in men (Barnes et al., Citation2016; Haeberer et al., Citation2015; Kubak et al., Citation2017; Ross et al., Citation2012; Singh-Manoux et al., Citation2008).
Differences in the obtained values of gender inequalities can also be observed in the classification of health care systems, while the highest average values in individual diagnosis groups occurred most often in the single payer model (SPM). At this point, it should be noted that each country has specific predispositions to a certain morbidity, as its incidence is influenced by various social, geographical and economic aspects. Another important but not dominant aspect may be the health care system, and as evidence shows, the health care financing system and its efficiency are one of the main factors in improving health status and reducing health inequalities among the population (Golinelli et al., Citation2018; Obrizan & Wehby, Citation2018).
The second part of the analytical processing consisted of regression analysis. The results of the regression analysis showed that gender inequalities in INF have a significant and inverse effect on economic productivity only in the countries that apply the NHS system. Accordingly, an increase in economic productivity can be expected with a reduction in these inequalities. With a focus on gender inequalities in CNC, significant and inverse effects on economic productivity were confirmed in all three analysed health care systems. The diagnostic tests in the BLD group indicated some uncertainty, and the effects of gender inequalities in this diagnosis group should be interpreted with some caution. Thus, a significant inverse effect was identified in the MI system, which can be seen in a positive context as opposed to a positive effect in the SPM system. In the case of gender inequalities in END, significant and positive effects were found in all analysed health care systems, indicating that reduced gender inequalities in this diagnosis group may lead to a decrease in economic productivity, which can be considered negative. At the same time, this can be explained by the fact that the cost of treating endocrine diseases exceeds lost productivity, especially for men. A similar result was found in the MNT diagnosis group in the countries that apply the NHS system. This finding can be explained in the same way as in the previous case, i.e. the loss of productivity does not exceed the costs related to this type of diseases. People suffering from diseases included in the MNT group usually do not work; therefore, they are not productive, but they deplete capital in the form of treatment costs. Focusing on gender inequalities in NRV, a significant and inverse effect was identified in the countries that apply the NHS system. In these countries, a reduction in gender inequalities leads to an increased economic productivity. In the countries applying the SPM system, the positive effect indicates the opposite situation, however, this can be considered significant only at the α level of 0.1. In terms of gender inequalities in CRC, significant and inverse effects were confirmed in the NHS and SPM systems. Also, gender inequalities in RSP showed a significant and inverse effect on economic productivity in the MI and NHS systems. With a focus on gender inequalities in DGS, significant and inverse effects were identified in all health care systems. At the same time, in the case of gender inequalities in the SKN and GNT diagnosis groups, significant and inverse effects on economic productivity were found in the MI and NHS systems. In these cases, it is possible to discuss gender inequality and its inverse effects in a similar positive context as in previous cases with a negative coefficient. Finally, gender inequalities in MSC showed a significant and positive effect on productivity in the NHS system. Based on these results, the NHS system appears to be a system, in which the effects of gender inequalities on economic productivity have been more pronounced and more direct.
With a focus on assessing the relationships between economic productivity and gender inequalities in the variables that determine the causes of mortality, some relations were not significant. On the other hand, strong and significant inverse relationships with GDP per person employed were found in three cases, namely DGS, RSP and CNC. At this hectic time, these diseases are very common in the population groups of productive people, reflecting the reason for the significant relations with economic productivity.
Based on the results of the regression and relationship analyses, it can be concluded that reducing gender inequalities in health may have a significant effect on economic productivity in developed countries that apply individual health care systems. This is supported by several claims that health inequalities between population groups of different socioeconomic, racial or ethnic status may affect the condition of economies (LaVeist et al., Citation2011; Mackenbach et al., Citation2011; Nanney et al., Citation2019; Politzer et al., Citation2019).
At the same time, attention should be focused on cancer mortality, which obtained significant results. In any case, cancer affects various age groups of the population, including young and productive people, who actively contribute to GDP. At the same time, it is clear from the previous results that men are more affected by cancer (Ellison, Citation2016; Fernandez et al., Citation2000), while men are generally more productive in their lives than women. From this point of view, it is logical that gender inequalities in cancer mortality have a significant negative effect on economic productivity. The high mortality of the productive male population contributes these health inequalities, and thus the explanation for this result is obvious.
In general, based on the above-mentioned, it can be concluded that reducing gender inequalities in mortality due to specific causes leads to an increased economic prosperity. To ensure the long-term development of economies, it is important to understand the main factors that affect their prosperity. This study proves that gender inequalities in health are one of these main factors. The public policies of developed countries should focus on reducing health inequalities in order to achieve economic growth. The opportunity can be seen in improving the health care system, as an efficient health system has the potential to better provide health care (Cylus et al., Citation2018). In order to reduce health inequalities, the efforts of policy makers should focus on the effective financing of health care, as well as on creating the conditions to ensure access to health care for all. Last but not least, promoting a healthy lifestyle of people, especially men, seems to be a key factor in reducing gender inequalities in health and increasing economic productivity. Smoking cessation and reduced alcohol consumption could improve health and ultimately bring economic benefits (Li et al., Citation2018; Mackenbach et al., Citation2017; Mehta & Myrskyla, Citation2017). Health policies should also take active steps to reduce the incidence of diseases of civilization. This study emphasizes the need for this effort not only on the part of policy makers, but also on the part of the population and their health-related behaviour. As emphasized, the health care system should also be taken into account in efforts to reduce health inequalities. In the NHS system, the effects of changes in gender inequalities were more pronounced than in other systems. Regarding the transformation of the reduction in gender inequalities into an increase in economic productivity, the NHS system can be considered the most positive and the SPM system can be seen as the least positive. The findings can be compared with those revealed by Van der Zee and Kroneman (Citation2007). In this context, the different efficiency of health care systems is evident and, in any case, improvements in health care systems can lead to an improvement in the health of the population (Ozcan & Khushalani, Citation2017).
6. Conclusion
Based on this research, it can be concluded that public health plays an important role in the economy, especially when the emphasis is on gender inequalities in health. The primary objective of the presented study was to assess the relations between gender health inequalities and economic productivity in a sample of OECD countries, with a focus on the classification of their health care systems. In general, it can be confirmed that there are significant effects of gender inequalities in health on economic productivity in the analysed sample. These findings have shown that economic productivity is associated with gender inequalities in health.
Policy makers should make efforts to reduce gender inequalities in health in order to increase economic prosperity. Prevention and education of healthy lifestyles could be one of the key elements in reducing these inequalities. At the same time, public policies should focus on the equitable distribution of health care.
The main limitation of this study is the fact that the variables included in the analyses were examined in a sample of OECD countries, and therefore the findings can be generalized to developed countries. Another potential limitation may be the fact that economic productivity could affect gender inequalities in health and vice versa. At this point, it should be emphasized that achieving a clear causal relationship is very problematic. Therefore, endogenous effects in individual countries may play an important role and may explain to some extent the health inequalities between men and women. In this study, the potential presence of endogeneity is considered a dominant limitation. In addition to the OLS method, the IV regression method was used to reduce this problem and achieve more reliable results. On the other hand, with a focus on the assumptions for the application of IV regression, the effects in the case of the NHS system can be considered questionable to some extent. These analytical processes allow a relevant estimation of the effects. We consider the selected time period to be representative and with regard to this period, we do not expect any significant impact of other effects.
In the future, research will focus on health in the economic dimension, but it will be more specific and the individual effects will be examined in more detail (e.g. effects on health inequalities). A certain vision of future research is also offered in terms of computational processing and it is possible to replicate research using other tools (modification of tools). This vision is mainly about the application of models with control variables.
Disclosure statement
Authors declare that they do not have any competing financial, professional, or personal interests from other parties.
Data availability statement
All data were provided from the OECD database (https://stats.oecd.org/#). The analysed data included selected causes of mortality (CM) as health variables, economic productivity represented by GDP per person as an economic variable, followed by variables determining health insurance coverage and individual health care systems. The data of causes of mortality were provided from sub-database "Health", folder "Health status" and sub-folder "Causes of mortality". The productivity data were provided from sub-database "Productivity", folder "Productivity and ULC – Annual, Total Economy" and sub-folder "Level of GDP per capita and productivity". The health care systems were provided from "Health Systems Characteristics Survey 2016".
Additional information
Funding
Notes
1 Australia-AUS; Austria-AUT; Belgium-BEL; Canada-CAN; Czech Republic-CZE; Denmark-DNK; Estonia-EST; Finland-FIN; France-FRA; Germany-DEU; Greece-GRC; Hungary-HUN; Chile-CHL; Iceland-ISL; Ireland-IRL; Israel-ISR; Italy-ITA; Japan-JPN; Korea-KOR; Latvia-LVA; Lithuania-LTU; Luxembourg-LUX; Mexico-MEX; Netherlands-NDL; New Zealand-NZL; Norway-NOR; Poland-POL; Portugal-POR; Slovak Republic-SVK; Slovenia-SVN; Spain-ESP; Switzerland-CHE; Turkey-TUR; United Kingdom-GBR; United States-USA.
References
- Ahmed, S., Hasan, M. Z., MacLennan, M., Dorin, F., Ahmed, M. W., Hasan, M. M., Hasan, S. M., Islam, M. T., & Khan, J. A. M. (2019). Measuring the efficiency of health systems in Asia: a data envelopment analysis. BJM Open, 9(3), e022155. https://doi.org/https://doi.org/10.1136/bmjopen-2018-022155
- Andrade, F. C. D., Guevara, P. E., Lebrao, M. L., de Oliveira Duarte, Y. A., & Santos, J. L. F. (2011). Gender differences in life expectancy and disability-free life expectancy among older adults in Sao Paulo, Brazil. Womens Health Issues, 21(1), 64–70. https://doi.org/https://doi.org/10.1016/j.whi.2010.08.007
- Ayala, C., Croft, J. B., Greenlund, K. J., Keenan, N. L., Donehoo, R. S., Malarcher, A. M., & Mensah, G. A. (2002). Sex differences in US mortality rates for stroke and stroke subtypes by race/ethnicity and age, 1995-1998. Stroke, 33(5), 1197–1201. https://doi.org/https://doi.org/10.1161/01.STR.0000015028.52771.D
- Bai, R., Wei, J., An, R., Li, Y., Collett, L., Dang, S., Dong, W., Wang, D., Fang, Z., Zhao, Y., & Wang, Y. (2018). Trends in life expectancy and its association with economic factors in the belt and road countries evidence from 2000-2014. International Journal of Environmental Research and Public Health, 15(12), 2890. https://doi.org/https://doi.org/10.3390/ijerph15122890
- Barnes, C., Andersen, Z. J., Overvad, K., Tjonneland, A., & Ulrik, C. S. (2016). Mortality rates in individuals with asthma, COPD and ACOS in a large population-based cohort: Is gender important? European Respiratory Journal, 48 (suppl 60), PA1136. https://doi.org/https://doi.org/10.1183/13993003.congress-2016.PA1136
- Belon, A. P., Lima, M. G., & Barros, M. B. A. (2014). Gender differences in healthy life expectancy among Brazilian elderly. Health and Quality of Life Outcomes, 12, 88 https://doi.org/https://doi.org/10.1186/1477-7525-12-88
- Bloom, D. E., Canning, D., & Sevilla, J. (2004). The effect of health on economic growth: A production function approach. World Development, 32(1), 1–13. https://doi.org/https://doi.org/10.1016/j.worlddev.2003.07.002
- Boachie, M. K. (2017). Health and economic growth in Ghana: an empirical investigation. Fudan Journal of the Humanities and Social Sciences, 10(2), 253–265. https://doi.org/https://doi.org/10.1007/s40647-016-0159-2
- Boisclair, D., Decarie, Y., Laliberte-Auger, F., Michaud, P. C., & Vincent, C. (2018). The economic benefits of reducing cardiovascular disease mortality in Quebec, Canada. Plos One, 13(1), e0190538 https://doi.org/https://doi.org/10.1371/journal.pone.0190538
- Clark, R., & Peck, B. M. (2012). Examining the gender gap in life expectancy: A cross-national analysis, 1980-2005. Social Science Quarterly, 93(3), 820–837. https://doi.org/https://doi.org/10.1111/j.1540-6237.2012.00881.x
- Costa-Font, J., & Hernandez-Quevedo, C. (2012). Measuring inequalities in health: What do we know? What do we need to know? Health Policy (Amsterdam, Netherlands), 106(2), 195–206. https://doi.org/https://doi.org/10.1016/j.healthpol.2012.04.007
- Cylus, J., Permanand, G., & Smith, P. C. (2018). Making the economic case for investing in health systems: What is the evidence that health systems advance economic and fiscal objectives?. WHO Regional Office for Europe. Retrieved October 3, 2020, from https://www.euro.who.int/__data/assets/pdf_file/0010/380728/pb-tallinn-01-eng.pdf?ua=1
- Deaton, A. (2003). Health, inequality, and economic development. Journal of Economic Literature, 41(1), 113–158. https://doi.org/http://doi.org/10.1257/002205103321544710 https://doi.org/https://doi.org/10.1257/jel.41.1.113
- Ellison, L. F. (2016). Differences in cancer survival in Canada by sex. Health Reports, 27(4), 19–27.
- Fernandez, E., Bosetti, C., La Vecchia, C., Levi, F., Fioretti, F., & Negri, E. (2000). Sex differences in colorectal cancer mortality in Europe, 1955-1996. European Journal of Cancer Prevention: The Official Journal of the European Cancer Prevention Organisation (Ecp), 9(2), 99–104. https://doi.org/https://doi.org/10.1097/00008469-200004000-00005
- Golinelli, D., Bucci, A., Toscano, F., Filicori, F., & Fantini, M. P. (2018). Real and predicted mortality under health spending constraints in Italy: a time trend analysis through artificial neural networks. BMC Health Services Research, 18(1), 671. https://doi.org/https://doi.org/10.1186/s12913-018-3473-3
- Haeberer, M., Noguer, I., & Mujica, O. J. (2015). Educational inequalities in mortality and survival of women and men in the Americas, 1990-2010. Revista Panamericana de Salud Publica = Pan American Journal of Public Health, 38(2), 89–95.
- Haseeb, M., Kot, S., Hussain, H. I., & Jermsittiparsert, K. (2019). Impact of economic growth, environmental pollution, and energy consumption on health expenditure and R&D expenditure of ASEAN countries. Energies, 12(19), 3598. https://doi.org/https://doi.org/10.3390/en12193598
- Jacobs, J. M., Cohen, A., Ein-Mor, E., & Stessman, J. (2014). Gender differences in survival in old age. Rejuvenation Research, 17(6), 499–506. https://doi.org/https://doi.org/10.1089/rej.2014.1587
- Kawiorska, D. (2016). Healthcare in the light of the concept of welfare state regimes – comparative analysis of EU member states. Oeconomia Copernicana, 7(2), 187–206. https://doi.org/https://doi.org/10.12775/OeC.2016.012
- Kim, J. I., & Kim, G. (2018). Effects on inequality in life expectancy from a social ecology perspective. BMC Public Health, 18(1), 243. https://doi.org/https://doi.org/10.1186/s12889-018-5134-1
- Kozlova, O. A., Nifantova, R. V., & Makarova, M. N. (2017). Methods of the assessment of economic losses caused by the mortality of the population employed in regional economy. Ekonomika Regiona-Economy of Region, 13(2), 511–523. https://doi.org/https://doi.org/10.17059/2017-2-16
- Kubak, M., Stefko, R., Bartak, M., Majernik, J., Vagasova, T., & Fedelesova, M. (2017). Risk of dying from cancer by socio-demographic indicators in the Slovak republic. Central European Journal of Public Health, 25, S37–S43. https://doi.org/https://doi.org/10.21101/cejph.a5050
- LaVeist, T. A., Gaskin, D., & Richard, P. (2011). Estimating the economic burden of racial health inequalities in the United States. International Journal of Health Services : Planning, Administration, Evaluation, 41(2), 231–238. https://doi.org/https://doi.org/10.2190/HS.41.2.c
- Le, Y., Ren, J., Shen, J., Li, T., & Zhang, C. (2015). The changing gender differences in life expectancy in Chinese cities 2005-2010. Plos One, 10(4), e0123320. https://doi.org/https://doi.org/10.1371/journal.pone.0123320
- Li, Y., Pan, A., Wang, D. D., Liu, X., Dhana, K., Franco, O. H., Kaptoge, S., Di Angelantonio, E., Stampfer, M., Willett, W. C., & Hu, F. B. (2018). Impact of healthy lifestyle factors on life expectancies in the US population. Circulation, 138(4), 345–355. https://doi.org/https://doi.org/10.1161/CIRCULATIONAHA.117.032047
- Liang, J., Bennett, J. M., Sugisawa, H., Kobayashi, E., & Fukaya, T. (2003). Gender differences in old age mortality: roles of health behavior and baseline health status. Journal of Clinical Epidemiology, 56(6), 572–582. https://doi.org/https://doi.org/10.1016/s0895-4356(03)00060-x
- Łyszczarz, B. (2016). Public-private mix and performance of health care systems in CEE and CIS countries. Oeconomia Copernicana, 7(2), 169–185. https://doi.org/https://doi.org/10.12775/OeC.2016.011
- Mackenbach, J. P., Bopp, M., Deboosere, P., Kovacs, K., Leinsalu, M., Martikainen, P., Menvielle, G., Regidor, E., & de Gelder, R. (2017). Determinants of the magnitude of socioeconomic inequalities in mortality: a study of 17 European countries. Health & Place, 47, 44–53. https://doi.org/https://doi.org/10.1016/j.healthplace.2017.07.005
- Mackenbach, J. P., Meerding, W. J., & Kunst, A. E. (2011). Economic costs of health inequalities in the European Union. Journal of Epidemiology and Community Health, 65(5), 412–419. https://doi.org/https://doi.org/10.1136/jech.2010.112680
- Mackenbach, J. P., Stirbu, I., Roskam, A. J. R., Schaap, M. M., Menvielle, G., Leinsalu, M., & Kunst, A. E. (2008). Socioeconomic inequalities in health in 22 European countries. The New England Journal of Medicine, 358(23), 2468–2481. https://doi.org/https://doi.org/10.1056/NEJMsa0707519
- Mayor, S. (2015). Life expectancy gender gap will close in England and Wales, study predicts. BMJ, 350(apr29 13), h2322–h2322. https://doi.org/https://doi.org/10.1136/bmj.h2322
- Megyesiova, S., & Lieskovska, V. (2018). Analysis of the sustainable development indicators in the OECD countries. Sustainability, 10(12), 4554. https://doi.org/https://doi.org/10.3390/su10124554
- Mehta, N., & Myrskyla, M. (2017). The population health benefits of a healthy lifestyle: life expectancy increased and onset of disability delayed. Health Affairs, 36(8), 1495–1502. https://doi.org/https://doi.org/10.1377/hlthaff.2016.1569
- Meirhaeghe, A., Cottel, D., Cousin, B., Dumont, M. P., Marecaux, N., Amouyel, P., & Dallongeville, J. (2018). Sex differences in stroke attack, incidence, and mortality rates in Northern France. Journal of Stroke and Cerebrovascular Diseases : The Official Journal of National Stroke Association, 27(5), 1368–1374. https://doi.org/https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.12.023
- Murphy, K. M., & Topel, R. H. (2006). The value of health and longevity. Journal of Political Economy, 114(5), 871–904. https://doi.org/https://doi.org/10.1086/508033
- Nanney, M. S., Myers, S. L., Xu, M., Kent, K., Durfee, T., & Allen, M. L. (2019). The economic benefits of reducing racial disparities in health: the case of Minnesota. International Journal of Environmental Research and Public Health, 16(5), 742. https://doi.org/https://doi.org/10.3390/ijerph16050742
- Obrizan, M., & Wehby, G. L. (2018). Health expenditures and global inequalities in longevity. World Development, 101, 28–36. https://doi.org/https://doi.org/10.1016/j.worlddev.2017.08.003
- OECD (2016). Health systems characteristics survey 2016. Retrieved August 12, 2020, from http://www.oecd.org/els/health-systems/OECD-HSC-Survey-2016-Project-outline.pdf
- OECD (2019). Health at a Glance 2019: OECD indicators. OECD Publishing. https://doi.org/https://doi.org/10.1787/4dd50c09-en
- OECD (2020a). OECD.stat. Retrieved August 12, 2020, from https://stats.oecd.org/
- OECD (2020b). Causes of mortality. Retrieved August 12, 2020, from https://stats.oecd.org/wbos/fileview2.aspx?IDFile=638c2ac2-5f0f-41ef-b2d9-2cfa1fd56429
- Ozcan, Y. A., & Khushalani, J. (2017). Assessing efficiency of public health and medical care provision in OECD countries after a decade of reform. Central European Journal of Operations Research, 25(2), 325–343. https://doi.org/https://doi.org/10.1007/s10100-016-0440-0
- Pacáková, V., & Kopecká, L. (2018). Comparing inequalities in health outcomes in European countries. Journal of International Studies, 11(4), 215–227. https://doi.org/https://doi.org/10.14254/2071-8330.2018/11-4/15
- Politzer, E., Shmueli, A., & Avni, S. (2019). The economic burden of health disparities related to socioeconomic status in Israel. Israel Journal of Health Policy Research, 8(1), 46 https://doi.org/https://doi.org/10.1186/s13584-019-0306-8
- Richardson, E. A., & Mitchell, R. (2010). Gender differences in relationships between urban green space and health in the United Kingdom. Soc Sci Med), 71(3), 568–575. https://doi.org/https://doi.org/10.1016/j.socscimed.2010.04.015
- Ross, C. E., Masters, R. K., & Hummer, R. A. (2012). Education and the gender gaps in health and mortality. Demography, 49(4), 1157–1183. https://doi.org/https://doi.org/10.1007/s13524-012-0130-z
- Sandiford, P. (2009). Gender inequality in New Zealand life expectancy: decomposition by age and cause. The New Zealand Medical Journal, 122(1307), 10–17.
- Sharma, R. (2018). Health and economic growth: evidence from dynamic panel data of 143 years. Plos One, 13(10), e0204940. https://doi.org/https://doi.org/10.1371/journal.pone.0204940
- Shuaibu, M., & Oladayo, P. T. (2016). Determinants of human capital development in Africa: a panel data analysis. Oeconomia Copernicana, 7(4), 523–549. https://doi.org/https://doi.org/10.12775/OeC.2016.030
- Singh-Manoux, A., Gueguen, A., Ferrie, J., Shipley, M., Martikainen, P., Bonenfant, S., Goldberg, M., & Marmot, M. (2008). Gender differences in the association between morbidity and mortality among middle-aged men and women. American Journal of Public Health, 98(12), 2251–2257. https://doi.org/https://doi.org/10.2105/AJPH.2006.107912
- Stefko, R., Jencova, S., Litavcova, E., & Vasanicova, P. (2017). Management and funding of the healthcare system. Polish Journal of Management Studies, 16(2), 266–277. https://doi.org/https://doi.org/10.17512/pjms.2017.16.2.23
- Van der Zee, J., & Kroneman, M. W. (2007). Bismarck or Beveridge: a beauty contest between dinosaurs. BMC Health Services Research, 7(1), 94. https://doi.org/10.1186/1472-6963-7-94
- Van Oyen, H., Cox, B., Jagger, C., Cambois, E., Nusselder, W., Gilles, C., & Robine, J. M. (2010). Gender gaps in life expectancy and expected years with activity limitations at age 50 in the European Union: associations with macro-level structural indicators. European Journal of Ageing, 7(4), 229–237. https://doi.org/https://doi.org/10.1007/s10433-010-0172-2
- Weil, D. N. (2007). Accounting for the effect of health on economic growth. The Quarterly Journal of Economics, 122(3), 1265–1306. https://doi.org/https://doi.org/10.1162/qjec.122.3.1265
- White, H. (1980). A heteroskedasticity-consistent covariance-matrix estimator and a direct test for heteroskedasticity. Econometrica, 48(4), 817–838. https://doi.org/https://doi.org/10.2307/1912934
- White, H. (1982). Instrumental variables regression with independent observations. Econometrica, 50(2), 483–499. https://doi.org/https://doi.org/10.2307/1912639
- WHO (2013). Health 2020: a European policy framework supporting action across government and society for health and well-being. WHO Regional Office for Europe. Retrieved August 12, 2020, from http://www.euro.who.int/__data/assets/pdf_file/0006/199536/Health2020-Short.pdf?ua=1
- WHO. (2002). Health, economic growth, and poverty reduction. The report of working group 1 of the Commission on macroeconomics and health. World Health Organization. Retrieved August 12, 2020, from https://apps.who.int/iris/bitstream/handle/10665/42492/9241590092.pdf;jsessionid=19B0494A7B879D7BE2F98CC714DFCFC5?sequence=1
- Woodward, A., & Kawachi, I. (2000). Why reduce health inequalities? Journal of Epidemiology and Community Health, 54(12), 923–929. https://doi.org/https://doi.org/10.1136/jech.54.12.923
- Zhang, T., Shi, W., Huang, Z., Gao, D., Guo, Z., & Chongsuvivatwong, V. (2016). Gender and ethnic health disparities among the elderly in rural Guangxi, China: estimating quality-adjusted life expectancy. Global Health Action, 9, 32261 https://doi.org/http://doi.org/10.3402/gha.v9.3</seurld> https://doi.org/https://doi.org/10.3402/gha.v9.32261