
ABSTRACT
Multiple health behaviour change (MHBC) represents one of the best ways to prevent reoccurrence of cardiovascular events. However, few individuals with cardiovascular diseases engage in this process. The present study examined the role of compensatory health beliefs (CHB; i.e., belief that a healthy behaviour compensates an unhealthy one) as a drag to engagement in this process. Some studies have shown that CHBs predict intention to engage in healthy behaviours, but no study has investigated CHBs in individuals who actually need to change multiple health behaviours. The goal was to better understand the role of CHBs in intentions formation process among individuals with cardiac diseases in an MHBC context. One hundred and four patients completed a questionnaire at the beginning of their cardiac rehabilitation program. Results showed that: (1) CHBs negatively predicted intentions (2) but only for participants with high self-efficacy or low risk perception; (3) CHBs predictions differed depending on the nature of the compensating behaviour, and were more predictive when medication intake was the compensating one. Findings only partially confirmed previous research conducted on healthy individuals who were not in an MHBC process, and emphasized the importance of considering CHBs for individuals in this process.
Introduction
Despite multiple health behaviour change (MHBC) effectiveness (e.g., physical activity, healthy diet, medication, Kotseva et al., Citation2016) on cardiac relapses (Bosworth et al., Citation2011), most individuals with cardiovascular diseases (IWCD) fail in this process. In MHBC, intention to adopt one behaviour may depend on beliefs about other behaviours. The present study adopted a cross-behavioural perspective, by examining the compensatory health beliefs (CHBs, belief that an unhealthy behaviour, such as eating snacks, can be compensated by a healthy one, such as being physically active; Rabiau, Knäuper, & Miquelon, Citation2006) role on intentions.
CHBs may negatively contribute to the intention formation process, independently from behaviour-specific factors (self-efficacy, risk perceptions, outcome expectancies) (Berli, Loretini, Radtke, Hornung, & Scholz, Citation2014; Fleig et al., Citation2015; Radtke, Scholz, Keller, & Hornung, Citation2012), and through the self-efficacy mediating role (Matley & Davies, Citation2017). CHBs may also interact with self-efficacy (they negatively predict intention when self-efficacy is low, Storm et al., Citation2016) and risk perception (they positively predict intention when risk perception is high, Radtke, Kaklamanou, Scholz, Hornung, & Armitage, Citation2014). However, CHBs’ effects have not been examined on IWCD in an MHBC context, but only in healthy populations with low/medium intentions for behaviours change (Radtke et al., Citation2012; Berli et al., Citation2014; Fleig et al., Citation2015; Storm et al., Citation2016). Whether CHBs predict intention in IWCD with high intentions, self-efficacy and perceived risks (e.g., Ghisi, Grace, Thomas, & Oh, Citation2015; Sniehotta et al., Citation2005) remains an open question.
Moreover, previous studies reported low scale homogeneity (e.g., α = .44 Radtke et al., Citation2014). One reason could be that CHBs scales aggregated beliefs about different compensatory behaviours (e.g., unhealthy diet may be compensated by skipping main dish, or by being physically active, Radtke et al., Citation2014), which is problematic because they may differ in several respects (e.g., required effort, perceived efficacy, McEachan, Lawton, & Conner, Citation2010). This raises the question of whether different CHBs similarly predict intentions or not. The present study investigated this question by separating CHBs depending on the nature of the behaviour, as recommended by Kaklamanou, Armitage, and Jones (Citation2013).
The present cross-sectional study investigated whether different CHBs predict intentions in IWCD in an MHBC process. We considered intention toward physical activity and healthy diet, two behaviours that most IWCD have to change (Kotseva et al., Citation2010, Citation2016). We tested in four separated models whether: (1) CHBmedication (i.e., belief that taking pills compensates an unhealthy behaviour), and (2) CHBphysical activity (i.e., belief that physical activity compensates an unhealthy behaviour), interact with self-efficacy and risk perception to predict intentionhealthy diet, and whether (3) CHBmedication and (4) CHBdiet (i.e., belief that healthy diet compensates an unhealthy behaviour) interact with self-efficacy and risk perception to predict intentionphysical activity. We expected CHBs to negatively predict intentions when self-efficacy is low (Storm et al., Citation2016), and to positively predict intentions when risk perception is high (Radtke et al., Citation2014). Control variables included other factors of intention (attitudes and subjective norms).
Method
Participants and procedure
Sample size was determined based on Green’s (Citation1991) recommendation of a minimum of 50 + 8m participants (m= number of predictors) for medium-effect-size studies with a small number of predictors (m ≤ 7), as is the case in the present study (m = 7), with medium-to-large effect sizes estimated (e.g., Gholami, Citation2014; Zhang, Zhang, Schwarzer, & Hagger, Citation2019). One-hundred-and-four IWCD (84 men, Mage = 55, SDage = 9) prescribed to change their diet and physical activity were recruited in a cardiac rehabilitation centre of Grenoble, France. Before the beginning of the program, the experimenter proposed them to participate in a study investigating their attitudes toward different behaviours. Consenting patients (they received no incentive) completed the paper-pencil questionnaire in the centre or at home. Anonymized data were collected from January 2017 to December 2019 (ethical approval n°IRB00010290-2016–07-05–10).
Measures
Three items, based on Knaüper et al.’s (Citation2004) scale were used to assess CHBs. Participants responded on a scale from (1) never to (7) all the time. Kaklamanou et al. (Citation2013) suggested to include a time dimension on CHBs scales, to target the behaviour rather than the belief itself, and that items should be phrased at the first person. Our scale is derived from these recommendations, and from recent measures of CHBs (e.g., Matley & Davies, Citation2017). Rather than focusing on frequency of healthy behaviours, our scale focuses on the unhealthy behaviours adoption frequency, and considers thus the behaviouralsub-dimension of the CHBs more than the belief in the compensatory effect itself.
Intentions were assessed through single-item scales, self-efficacy, subjective norms and risk perceptions through two-item scales, and attitudes with a three-item scale, based on Ajzen (Citation2002) and Schwarzer et al. (Citation2003) (scales in supplementary materials).
Results
Preliminary analyses
Because distributions were skewed, a square root transformation was applied to approximate a normal curve (scale reliability and correlations tables in supplementary materials)Footnote1 .
Main analyses
Both intentions were regressed on intention predictors, CHBs, CHBs x self-efficacy and CHBs x risk perception. Predictors (CHBs) and moderators (self-efficacy and risk perception) were mean-centred.
In intentionphysical activity models, only CHBmedication x self-efficacy was significant (β = −.17, p = .03, η2 = .03).
In intentionhealthy diet models, CHBphysical activity x self-efficacy (β = −.21, p = .01, η2 = .04) and CHBphysical activity x risk perception (β = .22, p= .01, η2 = .04) were significant, as well as CHBmedication x self-efficacy and CHBmedication x risk perception (respectively, β = −.22, p = .00, η2 = .05 and β = .30, p < .001, η2 = .05). Durbin–Watson test (Durbin & Watson, Citation1971) and quantile-quantile plot of all models suggested that residuals were normally distributed and not autocorrelated (i.e., values between 1.5 and 2.5; Field, Citation2013) (see and ).
Table 1. Results of the multiple linear regressions to predict intention toward physical activity.
Table 2. Results of the multiple linear regressions to predict intention toward healthy diet.
Significant interactions were decomposed with interActive (McCabe, Kim, & King, Citation2018). Concerning moderations of CHBs-intentions relationships by self-efficacy, results showed that CHBs negatively predicted intention when self-efficacy was high (). The simple slope of CHBmedication on intentionphysical activity was significant and negative when self-efficacy was 0.35 standard deviations (SD) away from the mean or further. Similarly, the simple slope of CHBmedication on intentionhealthy diet was significant and negative when self-efficacy was 0.55 SD away from the mean or further. The simple slope of CHBphysical activity on intentionhealthy diet was significant and negative when self-efficacy was 0.5 SD away from the mean or further.
Figure 1. Moderation of self-efficacy-intention and risk perception-intention relationships by CHB-medication. Because similar patterns of results were observed for all significant interactions, plots for the other CHBs are in the supplemental materials file. Simple slopes are provided for levels of the moderator 2 SD and 1 SD below and above the mean, and at the mean. Graphs show the computed 95% confidence region (shaded area), the observed data (grey circles), the maximum and minimum values of the outcome (dashed horizontal lines), and the crossover point (diamond). PTCL = percentile.
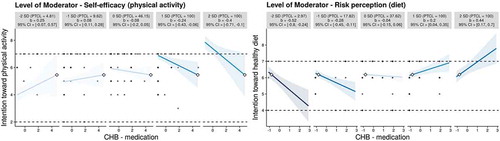
Regarding moderation of CHBs-intentionhealthy diet relationships by risk perception (), simple slopes of CHBphysical activity and CHBmedication were significant and negative, when risk perception was respectively −0.45 SD away from the mean or further, and −0.3 SD away from the mean or further. Finally, the simple slope of CHBmedication was significant and positive when risk perception was 0.75 SD away from the mean or further.
Discussion
This study confirmed that CHBs may negatively contribute to intention formation, but only for IWCD with high self-efficacy, contrary to Storm et al.’s (Citation2016) results. In IWCD, high self-efficacy may act as a self-illusion overestimating patients’ ability to actually change their behaviours. In this case, CHBs could be a strategy to justify and anticipate potential future self-regulation failures.
Interestingly, CHBs positively predicted intentions for IWCD with high-risk perception, corroborating Radtke et al. (Citation2014)’s observations. According to this study, CHBs may act as a motivator at an early stage of the health behaviour change process, where risk perceptions arise as a starting point.
However, our results also showed that CHBs negatively predicted intentions when risk perception was low. This finding adds to the literature by showing that low-risk perception could be more detrimental to intention formation in IWCD than in the general population, especially if it is combined with high CHBs.
Finally, CHBmedication and CHBphysical activity significantly predicted intention but not CHBdiet, confirming the need to distinguish CHBs depending on their nature. Moreover, CHBmedication predicted both intentions. This CHB may be attractive, because it implies that adopting an effortless behaviour (taking pills) may compensate for non-adoption of effortful ones (physical activity and healthy diet, McEachan et al., Citation2010). If this CHB reduces individuals’ adherence to other healthy behaviours, it could in part explain people’s difficulties in MHBC after a cardiac event.
Limitations and futures directions
First, our cross-behavioural approach examined only behaviour-specific intentions. Future studies should test cross-behavioural models (e.g., Compensatory Carry-Over Action Model, Lippke, Citation2014). Secondly, this study focused on intention formation and not on behaviour change. Prospective studies should examine CHBs role during the volitional phase (i.e., behaviour adoption and maintenance). Thirdly, we used single-item scales to avoid overloading participants but, despite its validity (Gogol et al., Citation2014), this method may present psychometric limitations. Future research should use multiple-item measures if study conditions permit it. Finally, exploring CHBs within the same behaviour could be interesting (e.g., belief that unhealthy diet could be compensated by healthy diet the day after).
Conclusion and practical implications
Results suggest the need for cardiac rehabilitation practitioners to alert IWCD about the inaccuracy of CHBs, especially when patients present very high self-efficacy and/or low-risk perception. These persons could need an individualized care, for example, through adapted therapeutic education session. Finally, findings suggest that interventions on CHBs should consider the nature of the compensating and target behaviours.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Supplemental Material
Download Zip (435.8 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for the article can be accessed here.
Additional information
Funding
Notes
1 Data files are available online: https://data.mendeley.com/datasets/5cnsgmpbwn/1
References
- Ajzen, I. (2002). Constructing a TpB Questionnaire : Conceptual and Methodological Considerations. Time. 1–13. doi:10.1002/hep.22759
- Berli, C., Loretini, P., Radtke, T., Hornung, R., & Scholz, U. (2014). Predicting physical activity in adolescents: The role of compensatory health beliefs within the health action process approach. Psychology & Health, 29(4), 458–474.
- Bosworth, H. B., Granger, B. B., Mendys, P., Brindis, R., Burkholder, R., Czajkowski, S. M., … Granger, C. B. (2011). Medication adherence: A call for action. American Heart Journal, 162(3), 412–424.
- Durbin, J., & Watson, G. S. (1971). Testing for serial correlation in least squares regression.III. Biometrika, 58(1), 1–19.
- Field, A. (2013). Discovering statistics using SPSS discovering statistics using SPSS. Area.London: Sage.
- Fleig, L., Ngo, J., Roman, B., Ntzani, E., Satta, P., Warner, L. M., … Brandi, M. L. (2015). Beyond single behaviour theory: Adding cross-behaviour cognitions to the health action process approach. British Journal of Health Psychology, 20(4), 824–841.
- Ghisi, G. L. D. M., Grace, S. L., Thomas, S., & Oh, P. (2015). Behavior determinants among cardiac rehabilitation patients receiving educational interventions: An application of the health action process approach. Patient Education and Counseling, 98(5), 612–621.
- Gholami, M. (2014). Application of the health action process approach to physical activity: A meta-analysis. European Health Psychologist, 16(S), 732. Retrieved from http://www.diss.fu-berlin.de/diss/servlets/MCRFileNodeServlet/FUDISS_derivate_000000015447/Dissertation_Maryam_Gholami_online_submission.pdf#page=47%0Ahttp://edocs.fu-berlin.de/diss/receive/FUDISS_thesis_000000097017
- Gogol, K., Brunner, M., Goetz, T., Martin, R., Ugen, S., Keller, U., … Preckel, F. (2014). “My Questionnaire is Too Long!” The assessments of motivational-affective constructs with three-item and single-item measures. Contemporary Educational Psychology, 39(3), 188–205.
- Green, S. B. (1991). How many subjects does it take to do a regression analysis? Multivariate Behavioral Research, 26(3), 499–510.
- Kaklamanou, D., Armitage, C. J., & Jones, C. R. (2013). A further look into compensatory health beliefs: A think aloud study. British Journal of Health Psychology, 18(1), 139–154.
- Knäuper, B., Rabiau, M., Cohen, O., & Patriciu, N. (2004). Compensatory health beliefs: Scale development and psychometric properties. Psychology and Health,19(5), 607–624. doi:10.1080/0887044042000196737
- Kotseva, K., Wood, D., de Backer, G., de Bacquer, D., Pyörälä, K., Reiner, Z., & Keil, U. (2010). EUROASPIRE III. Management of cardiovascular risk factors in asymptomatic high-risk patients in general practice: Cross-sectional survey in 12 European countries. European Journal of Preventive Cardiology, 17(5), 530–540.
- Kotseva, K., Wood, D., De Bacquer, D., De Backer, G., Rydén, L., Jennings, C., … Vulic, D. (2016). EUROASPIRE IV: A European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. European Journal of Preventive Cardiology, 23(6), 636–648.
- Lippke, S. (2014). Modelling and supporting complex behavior change related to obesity and diabetes prevention and management with the compensatory carry-over action model. Journal of Diabetes and Obesity, 1(2), 1–5.
- Matley, F. A. I., & Davies, E. L. (2017). Resisting temptation: Alcohol specific self-efficacy mediates the impacts of compensatory health beliefs and behaviours on alcohol consumption. Psychology, Health and Medicine, 23(3), 259–269.
- McCabe, C. J., Kim, D. S., & King, K. M. (2018). Improving present practices in the visual display of interactions. Advances in Methods and Practices in Psychological Science, 1(2), 147–165.
- McEachan, R. R. C., Lawton, R. J., & Conner, M. (2010). Classifying health-related behaviours: Exploring similarities and differences amongst behaviours. British Journal of Health Psychology, 15(2), 347–366.
- Rabiau, M., Knäuper, B., & Miquelon, P. (2006). The eternal quest for optimal balance between maximizing pleasure and minimizing harm: The compensatory health beliefs model. British Journal of Health Psychology, 11(1), 139–153.
- Radtke, T., Kaklamanou, D., Scholz, U., Hornung, R., & Armitage, C. J. (2014). Are diet-specific compensatory health beliefs predictive of dieting intentions and behaviour? Appetite, 76, 36–43.
- Radtke, T., Scholz, U., Keller, R., & Hornung, R. (2012). Smoking is ok as long as I eat healthily: Compensatory Health Beliefs and their role for intentions and smoking within the Health Action Process Approach. Psychology and Health, 27(SUPPL. 2), 91–107.
- Schwarzer, R., Sniehotta, F. F., Lippke, S., Luszczynska, A., Scholz, U., Schüz, B., … Ziegelmann, J. (2003). On the assessment and analysis of variables in the health action process approach: Conducting an investigation (pp. 1–18). Berlin: Freie Universität. doi:10.5167/uzh-102499
- Sniehotta, F. F., Scholz, U., Schwarzer, R., Fuhrmann, B., Kiwus, U., & Völler, H. (2005). Long-term effects of two psychological interventions on physical exercise and self-regulation following coronary rehabilitation. International Journal of Behavioral Medicine, 12(4), 244–255.
- Storm, V., Reinwand, D., Wienert, J., Kuhlmann, T., De Vries, H., & Lippke, S. (2016). Brief report: Compensatory health beliefs are negatively associated with intentions for regular fruit and vegetable consumption when self-efficacy is low. Journal of Health Psychology, 22(8), 1094–1100.
- Zhang, C., Zhang, R., Schwarzer, R., & Hagger, M. S. (2019). A meta-analysis of the health action process approach. Health Psychology, 38(7), 623–637.
