
ABSTRACT
Background
The etiology of POEMS syndrome and its associated polyneuropathy have not been fully elucidated. The clinical picture of POEMS-associated polyneuropathy and nutritional polyneuropathy due to vitamin B6 (VB6) deficiency are strikingly similar, both being typically sensorimotor, symmetrical, stocking and glove distribution, and more severe in the lower extremities.
Case presentation
We report two consecutive POEMS patients with VB6 deficiency who showed unusual rapid and drastic recovery of polyneuropathies within 6–8 weeks after oral VB6 supplementation. Case 1 was supplemented with VB6 from time of autologous stem cell transplantation. Polyneuropathy began to improve within one week, and he became walker-free and could walk unaided with a cane within 6 weeks. Case 2 was supplemented with VB6 from time of stem cell harvest, and he became cane-free and his gait almost normalized within two months. Nerve conduction studies were also confirmatory of neurologic recovery in both cases.
Conclusions
Objective physical improvement of POEMS-associated polyneuropathy has been reported to typically require approximately a year after autologous stem cell transplantation, and together with our observations of VB6 deficiency and supplementations leading to accelerated recoveries of polyneuropathy, VB6 deficiency most probably contributes to POEMS-associated polyneuropathy. VB6 acts as a coenzyme in approximately 150 biochemical reactions. VB6 has been reported to inhibit the hypoxia-inducible factor/vascular endothelial growth factor (VEGF) pathway, and VEGF levels are known to corollate with disease activity of POEMS syndrome. Therefore, VB6 deficiency may contribute not only to POEMS-associated polyneuropathy, but also to the etiology of POEMS syndrome itself.
Introduction
POEMS syndrome is a paraneoplastic syndrome attributed to an underlying plasma cell neoplasm. The acronym POEMS stands for polyneuropathy, organomegaly, endocrinopathy, monoclonal plasma cell disorder, and skin changes. Other characteristic features not included in the acronym are papilledema, extravascular volume overload, sclerotic bone lesions, and thrombocytosis/erythrocytosis. The etiology of POEMS syndrome and its diverse manifestations have not been fully elucidated, but many of the clinical manifestations are thought to be the result of increased vascular permeability and neovascularization secondary to cytokine overproduction of which vascular endothelial growth factor (VEGF) plays a central role. POEMS-associated polyneuropathy is typically sensorimotor, symmetrical, stocking and glove distribution, and more severe in the lower extremities [Citation1,Citation2]. POEMS-associated polyneuropathy is usually slowly progressive, but onset and progression may be acute in certain patients with various contributing factors [Citation3,Citation4]. Anti-plasma cell therapy including autologous stem cell transplantation (ASCT) is often effective for POEMS syndrome, but recovery of polyneuropathy is usually an extremely slow process [Citation2]. We report two consecutive POEMS patients presenting with vitamin B6 (VB6) deficiency who experienced unusual rapid recovery of polyneuropathy after VB6 supplementation. The clinical picture of polyneuropathy seen in POEMS syndrome and VB6 deficiency are strikingly similar, and we speculate that VB6 deficiency plays a major role in POEMS-associated polyneuropathy. The coenzymatic function of VB6 has been reported to inhibit the hypoxia-inducible factor (HIF)/VEGF pathway, and VEGF levels are known to correlate with disease activity of POEMS syndrome [Citation5]. Thus, VB6 deficiency may contribute not only to polyneuropathy, but also to the etiology of POEMS syndrome itself.
Case presentation
Case 1 is a 50-year-old man presenting with polyneuropathy, hyperpigmentation, edema, hypertrichosis, IgA-lambda type M-protein, and an elevated serum VEGF of 9470 pg/mL (normal range: 62–707 pg/mL). CT scans revealed an isolated thoracic spine sclerotic bone lesion (T9) and splenomegaly. POEMS syndrome was diagnosed, and because bone marrow evaluation revealed no clonal plasma cell proliferation, radiation therapy of 40Gy to the T9 bone lesion was carried out. However, no improvements in serum VEGF levels and clinical symptoms (polyneuropathy, hyperpigmentation, edema, hypertrichosis) were observed, and thus thalidomide-dexamethasone therapy was initiated in August 2018. Nearly a year of thalidomide-dexamethasone therapy led to a significant decrease of serum VEGF levels, but again the clinical symptoms did not improve. ASCT with melphalan 200 mg/m2 conditioning was carried out in April 2019. Subsequently, we discovered that serum VB6 levels were undetectably low at <2.0 ng/mL (normal values: 6.0–40.0 ng/mL for males, commercially analyzed by SRL Inc., Tokyo, Japan, as reported previously [Citation6]) (). Supplementation with 60 mg/day of pyridoxal phosphate hydrate (PPH) was initiated, and polyneuropathy began to rapidly improve after 1 week of administration, and within 6 weeks, he became walker-free and could walk unaided with a cane. During these 6 weeks, hyperpigmentation was also almost completely resolved.
Figure 1. Clinical course of two POEMS patients with vitamin B6 deficiency. The dotted lines represent the lower limit of normal for serum vitamin B6. ALT: alanine aminotransferase; ASCT: autologous stem cell transplantation; AST: aspartate aminotransferase; NCS1: nerve conduction study (before VB6 administration); NCS2: nerve conduction study (after VB6 administration); OP: operation; PPH: pyridoxal phosphate hydrate; RT: radiation therapy; THAL + DEX: thalidomide + dexamethasone; VB6: vitamin B6; VEGF: vascular endothelial growth factor; VRD: bortezomib + lenalidomide + dexamethasone
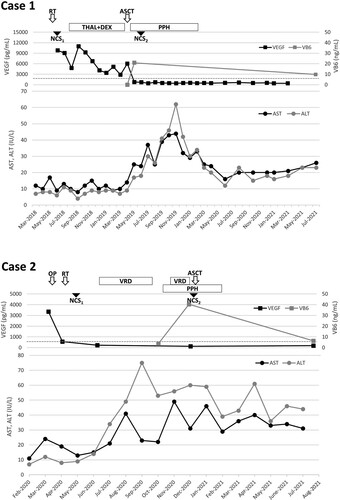
Case 2 is a 51-year-old man presenting with polyneuropathy involving all four limbs, edema, hyperpigmentation, IgG-lambda type M-protein, and an elevated serum VEGF of 3350 pg/mL. CT scans revealed a thoracic spine tumor (T2-4) that was compressing the spinal cord parenchyma, and multiple osteosclerotic and osteolytic lesions in the thoracic spine. The thoracic spine tumor was resected to relieve spinal cord compression, and pathology revealed a plasmacytoma. Thus, multiple myeloma complicated by POEMS syndrome was diagnosed. Postoperative radiation therapy of 24Gy was administered to the original site of plasmacytoma, and three courses of VRD (bortezomib, lenalidomide, dexamethasone) therapy were administered. Although the patient’s gait disturbance improved and was able to walk with a cane after resection of the plasmacytoma, thereafter, his symptoms became fixed for approximately six months and numbness and loss of sensation especially in the lower extremities persisted. In October 2020, VB6 levels were found to be low at 3.8 ng/mL, and supplementation with 60 mg/day of PPH was initiated (). Subsequently, the patient’s lingering symptoms of polyneuropathy suddenly started to improve, and he became cane-free and his gait almost normalized within two months after initiation of VB6 supplementation. The patient underwent two more courses of VRD therapy and proceeded to ASCT with melphalan 200 mg/m2 conditioning in December 2020. The clinical course of case 2 has been previously reported elsewhere [Citation7].
Nerve conduction studies (NCS) also confirmed improvements in polyneuropathy before and after VB6 supplementation in both cases 1 and 2 (), although one limitation is that the pre-evaluation of NCS was not timed exactly before initiation of VB6 administration. Although VB6 supplementations were ceased after ASCT in both cases, no relapses of polyneuropathy have occurred and both cases have maintained normal serum VB6 levels thereafter, and thus VB6 deficiency may be a sign of worse disease status in POEMS syndrome. In line with previous reports, aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were low in both cases due to VB6 deficiency, but elevations to normal levels were observed with VB6 supplementations ().
Table 1. Nerve conduction studies before and after vitamin B6 supplementation.
Discussion
Improvement of polyneuropathy in POEMS patients is a slow process, and in a study of 17 patients, it was reported that more than 12 months after ASCT was necessary for an objective physical improvement to be seen [Citation2]. Compared to this, drastic improvements in polyneuropathy were seen within 6–8 weeks in our two POEMS patients after VB6 supplementation. The clinical picture of POEMS-associated polyneuropathy and nutritional polyneuropathy due to VB6 deficiency are strikingly similar, being typically sensorimotor, symmetrical, stocking and glove distribution, and more severe in the lower extremities. Also common to both polyneuropathies is that a proportion of patients experience painful dysesthesias [Citation1,Citation8]. Together with our observations, it is tempting to speculate that VB6 deficiency is the underlying cause of POEMS-associated polyneuropathy. One argument may be that within the limited data in humans, VB6-deficient polyneuropathy has been reported to be predominantly due to axonopathy, whereas POEMS-associated polyneuropathy involves both demyelination and axonopathy [Citation1,Citation9,Citation10]. However, VB6 is necessary as a coenzyme in sphingolipid synthesis and therefore crucial for myelin formation, and in theory, VB6 deficiency can well contribute to demyelination [Citation11]. Furthermore, in a study of rats fed a VB6-deficient diet, overt polyneuropathy developed, and nerve pathology revealed abnormal thinning of myelin [Citation12]. Therefore, VB6-deficient polyneuropathy may also involve both demyelination and axonopathy as is seen in POEMS-associated polyneuropathy.
VB6 deficiency in POEMS patients has not been previously studied. Besides the two cases presented here, in actual, there was one more POEMS patient recently found to have undetectably low VB6 levels of <2.0 ng/mL at our institution. VB6 supplementation did not have a clinical impact on this patient, but the degree of polyneuropathy was much milder compared to the two presented cases, making it difficult to assess any neurologic improvements. Thus, in total, three consecutive POEMS patients presented with VB6 deficiency at our institution, and VB6 deficiency may be a universal finding among patients with POEMS syndrome. VB6 is abundant in a wide range of food sources, and the synthesis of VB6 by the gut flora also contributes to VB6 intake. Therefore, VB6 deficiency is rare in the general population unless special situations accompany such as malabsorption due to bowel disease and resection, alcoholism, eating disorders, hemodialysis, pregnancy, and certain drugs (e.g. isoniazid, cycloserine, and penicillamine) [Citation6,Citation11,Citation13]. All three patients harbored none of these traits.
VEGF levels have been reported to correlate with POEMS disease activity, and VB6 is known to suppress VEGF mRNA induction through inhibiting the VEGF upstream regulator, HIF [Citation5]. Thus, VB6 deficiency can potentially contribute to the elevation of VEGF levels and therefore may even play a role in the etiology of POEMS syndrome. The main source of VEGF overproduction in patients with POEMS syndrome remains unclear due to reports with conflicting results. Nagao et al reported that VEGF mRNA was not significantly higher in plasma cells of POEMS syndrome compared with other plasma cell dyscrasias, while Wang et al reported that VEGF mRNA levels were significantly higher in plasma cells of POEMS syndrome compared to other plasma cell dyscrasias and are the source of VEGF production. Wang et al also demonstrated that bone marrow plasma cells exhibit higher levels of VEGF mRNA expression compared to CD138-negative cells in patients with POEMS syndrome, and also that both monoclonal and polyclonal plasma cells of patients with POEMS syndrome express equally high levels of intracellular VEGF, which has been one of the unsolved mysteries of POEMS syndrome [Citation14,Citation15]. However, a systemic dysregulation of HIF through VB6 deficiency that equally affects both monoclonal and polyclonal plasma cells would be a rational explanation for this phenomenon [Citation1].
VB6 acts as a coenzyme in approximately 150 biochemical reactions that regulate metabolism of amino acids, lipids, neurotransmitters, DNA, and glucose [Citation16]. Therefore, deficiency can lead to a wide range of clinical manifestations that include, but are not limited to, polyneuropathy, seizures, anemia, diabetes mellitus, dermatitis, stomatitis, and glossitis [Citation11]. Not only polyneuropathy, but also hyperpigmentation rapidly regressed in case 1 after VB6 administration, and we suspect that some of the skin changes found in POEMS syndrome may be due to dermatitis caused by VB6 deficiency. POEMS patients also frequently present with endocrinopathies of which the pathogenesis is unknown [Citation1,Citation17]. Surprisingly, both POEMS syndrome and VB6-deficient states have been associated with identical endocrinopathies or data in parallel including hypogonadism (low testosterone), hyperprolactinemia, hypothyroidism, diabetes mellitus, and adrenal insufficiency. There is substantial evidence for endocrinopathy developing under VB6-deficient states. Rats fed a VB6-free diet have been reported to show significantly decreased testosterone plasma concentrations compared to controls [Citation18]. VB6 deficiency can potentially cause hyperprolactinemia because the conversion of dopa to dopamine is VB6-dependent, and dopamine formation in hypothalamic neurons has an inhibitory effect on prolactin. In line with this, two trials including a total of 349 participants demonstrated that VB6 supplementation was effective in inhibiting post-partum lactation [Citation19]. Dakshinamurti et al reported in VB6-deficient rats low TSH, T3, and T4, and an intact TRH response, and thus demonstrated a hypothalamic type of hypothyroidism [Citation20]. As for diabetes mellitus, VB6 deficiency has been reported to impair insulin secretion in rats, and in vitro experiments of pancreas perfusion have demonstrated equivalent results. Furthermore, Drosophila with genetic mutations involving VB6 metabolism are known to develop diabetes mellitus [Citation16]. In humans, VB6 deficiency increases gestational glucose intolerance, and VB6 supplementation has been reported to improve glucose tolerance during pregnancy [Citation21]. The catabolism of tryptophan to serotonin is VB6-dependent, and decreased serotonin in pancreatic islets has been demonstrated to reduce β-cell proliferation in a serotonin receptor 2B (HTR2B)-dependent manner, and has been implicated as the underlying mechanism. Although VB6 deficiency has not been directly linked to adrenal insufficiency, patients with deprivation of the VB6-dependent enzyme sphingosine phosphate lyase have been shown to develop adrenal insufficiency [Citation22]. Autopsy cases of POEMS patients have found structurally normal and non-characteristic endocrine glands suggestive of a functional rather than a structural gland dysfunction, and this is supportive of the theory that VB6 deficiency contributes to endocrinopathy in POEMS syndrome [Citation17].
Because the clinical manifestations of VB6 deficiency are extremely diverse and none are specific to VB6 deficiency, suspecting deficiency in the right patient can be difficult. However, patients with VB6 deficiency are known to present with abnormally low levels of AST and ALT [Citation23], which is a useful parameter for suspecting VB6 deficiency, and was also the motive for suspecting VB6 deficiency in the three POEMS patients discussed here. Baseline AST and ALT normalized in both cases 1 and 2 following VB6 supplementation and subsequent elevations of serum VB6 levels.
Conclusions
Polyneuropathy is one of the most devastating manifestations for patients with POEMS syndrome, and is irreversible in many cases because symptoms linger for long periods of time and damage accumulates even after treatment initiation. Through our observations, VB6 deficiency may well be a universal finding amongst patients with POEMS syndrome, and early rescue of polyneuropathy with VB6 supplementation as was observed in the presented cases would be most ideal. The types and patterns of polyneuropathy and endocrinopathy in POEMS syndrome and VB6 deficiency are strikingly similar, and VB6 deficiency may be a cause of multiple manifestations of POEMS syndrome. One limitation of this report is that the two patients presented were simultaneously being treated with drugs other than VB6, but the rapid neurological recoveries were only seen directly after VB6 supplementation and therefore were most likely attributed to VB6. Our observations need to be validated in a larger number of patients, and the underlying mechanisms of VB6 deficiency occurring in POEMS patients need to be clarified.
Author contributions
HY, YF, and KN wrote the manuscript, MS, YT, and SS collected and interpreted the data and did the literature research, NH, MA, and NK revised and approved the manuscript.
Data availability statement
Data from this study are available from the corresponding author, Hajime Yasuda.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Dispenzieri A. POEMS syndrome. Update on diagnosis, risk-stratification, and management. Am J Hematol. 2021;96(7):872–888.
- Ohwada C, Sakaida E, Kawajiri-Manako C, et al. Long-term evaluation of physical improvement and survival of autologous stem cell transplantation in POEMS syndrome. Blood. 2018;131(19):2173–2176.
- Isose S, Misawa S, Kanai K, et al. POEMS syndrome with Guillan-Barre syndrome-like acute onset: a case report and review of neurological progression in 30 cases. J Neurol Neurosurg Psychiatry. 2011;82(6):678–680.
- Wang C, Guan YZ, Cai QQ, et al. Rapidly progressive polyneuropathy in a patient with monoclonal gammopathy: a case report of POEMS syndrome and beyond. Medicine (Baltimore). 2016;95(16):e3453.
- Ibuki M, Lee D, Shinojima A, et al. Rice bran and vitamin B6 suppress pathological neovascularization in a murine model of age-related macular degeneration as novel HIF inhibitors. Int J Mol Sci. 2020;21(23):8940.
- Yasuda H, Tsutsui M, Ando J, et al. Vitamin B6 deficiency is prevalent in primary and secondary myelofibrosis patients. Int J Hematol. 2019;110(5):543–549.
- Sano M, Iseki T, Sasaki M, et al. Improvement in the symptoms and VEGF levels after resection of an extrame dullary spinal tumor and additional chemotherapy in a patient with multiple myeloma complicated with POEMS syndrome. Intern Med. 2021;60(22):3625–3630.
- Snider DE, Jr. Pyridoxine supplementation during isoniazid therapy. Tubercle. 1980;61(4):191–196.
- Chelban V, Wilson MP, Warman Chardon J, et al. PDXK mutations cause polyneuropathy responsive to pyridoxal 5'-phosphate supplementation. Ann Neurol. 2019;86(2):225–240.
- Müller T, van Laar T, Cornblath DR, et al. Peripheral neuropathy in Parkinson's disease: levodopa exposure and implications for duodenal delivery. Parkinsonism Relat Disord. 2013;19(5):501–507. discussion.
- Calderon-Ospina CA, Nava-Mesa MO. B vitamins in the nervous system: current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci Ther. 2020;26(1):5–13.
- Dellon AL, Dellon ES, Tassler PL, et al. Experimental model of pyridoxine (B6) deficiency-induced neuropathy. Ann Plast Surg. 2001;47(2):153–160.
- Yasuda H, Fujiwara N, Ishizaki Y, et al. Anemia attributed to vitamin B6 deficiency in post-pancreaticoduodenectomy patients. Pancreatology. 2015;15(1):81–83.
- Nagao Y, Mimura N, Takeda J, et al. Genetic and transcriptional landscape of plasma cells in POEMS syndrome. Leukemia. 2019;33(7):1723–1735.
- Wang C, Huang XF, Cai QQ, et al. Remarkable expression of vascular endothelial growth factor in bone marrow plasma cells of patients with POEMS syndrome. Leuk Res. 2016;50:78–84.
- Mascolo E, Verni F. Vitamin B6 and diabetes: relationship and molecular mechanisms. Int J Mol Sci. 2020;21(10):3669
- Gandhi GY, Basu R, Dispenzieri A, et al. Endocrinopathy in POEMS syndrome: the Mayo clinic experience. Mayo Clin Proc. 2007;82(7):836–842.
- Symes EK, Bender DA, Bowden JF, et al. Increased target tissue uptake of, and sensitivity to, testosterone in the vitamin B6 deficient rat. J Steroid Biochem. 1984;20(5):1089–1093.
- AlSaad D, Awaisu A, Elsalem S, et al. Is pyridoxine effective and safe for post-partum lactation inhibition? A systematic review. J Clin Pharm Ther. 2017;42(4):373–382.
- Dakshinamurti K, Paulose CS, Vriend J. Hypothyroidism of hypothalamic origin in pyridoxine-deficient rats. J Endocrinol. 1986;109(3):345–349.
- Fields AM, Welle K, Ho ES, et al. Vitamin B6 deficiency disrupts serotonin signaling in pancreatic islets and induces gestational diabetes in mice. Commun Biol. 2021;4(1):421.
- Zhao P, Liu ID, Hodgin JB, et al. Responsiveness of sphingosine phosphate lyase insufficiency syndrome to vitamin B6 cofactor supplementation. J Inherit Metab Dis. 2020;43(5):1131–1142.
- Linkswiler H. Biochemical and physiological changes in vitamin B6 deficiency. Am J Clin Nutr. 1967;20(6):547–557.