
Abstract
This study aimed to quantify correlations between theory of planned behaviour (TPB) variables and (i) intentions to consume alcohol and (ii) alcohol consumption. Systematic literature searches identified 40 eligible studies that were meta-analysed. Three moderator analyses were conducted: pattern of consumption, gender of participants and age of participants. Across studies, intentions had the strongest relationship with attitudes (r+ = .62), followed by subjective norms (r+ = .47) and perceived behavioural control (PBC; r+ = .31). Self-efficacy (SE) had a stronger relationship with intentions (r+ = .48) compared with perceived control (PC; r+ = −.10). Intention had the strongest relationship with alcohol consumption (r+ = .54), followed by SE (r+ = .41). In contrast, PBC and PC had negative relationships with alcohol consumption (r+ = −.05 and −.13, respectively). All moderators affected TPB relationships. Patterns of consumption with clear definitions had stronger TPB relations, females reported stronger attitude–intention relations than males, and adults reported stronger attitude–intention and SE–intention relations than adolescents. Recommendations for future research include targeting attitudes and intentions in interventions to reduce alcohol consumption, using clear definitions of alcohol consumption in TPB items to improve prediction and assessing SE when investigating risk behaviours.
Alcohol consumption is the third biggest risk to health in developed countries (WHO, Citation2002). It leads to harm from both chronic intake (i.e., long-term, regular, consumption) and acute intake (i.e., consuming a large number of alcoholic units in a single session or episode; Babor et al., Citation2010). Liver disease is a harm associated with chronic intake and is the fifth largest cause of death in the UK, killing more than 15,000 people a year (British Liver Trust, Citation2009). With regard to acute harms, episodes of excessive consumption have been linked to health and social problems such as crime, injuries and sexually transmitted infections (Centers for Disease Control and Prevention, Citation2011). The British Crime Survey (Home Office, Citation2009) found that 76,000 facial injuries each year were linked to drunken violence, while Jones, Bellis, Dedman, Sumnall, and Tocque (Citation2008) noted that 26% of all deaths in 16- to 24-years olds in the UK are due to alcohol, resulting from accidents and acute poisoning. Thus, it is important to understand the psychological determinants of alcohol consumption.
A model of human behaviour that has been extensively utilised to predict health-related behaviours such as alcohol consumption is the theory of planned behaviour (TPB; Ajzen, Citation1991). This model proposes that the most important determinant of behaviour is a person's intention to perform the behaviour. In turn, three variables are identified as determinants of intention: attitude, subjective norm and perceived behavioural control (PBC). Attitudes are an individual's positive or negative evaluation of performing the behaviour. Subjective norms reflect an individual's perceptions of social approval or disapproval for performing the behaviour. PBC represents an individual's perceptions of control over behavioural performance in the face of internal and external barriers. Ajzen (Citation2002) views PBC as a combination of perceived control (PC; i.e., perceptions of external barriers to behavioural performance) and self-efficacy (SE; i.e., confidence that one has the ability to perform behaviour). The TPB also proposes that PBC can act as a predictor of behaviour if it accurately reflects actual control over behavioural performance.
Meta-analytic reviews support the capacity of the TPB to explain variance in intentions and behaviour for many health-related behaviours (Armitage & Conner, Citation2001; Conner & Sparks, Citation2005; McEachan, Conner, Taylor, & Lawton, Citation2011). McEachan et al. (Citation2011) reviewed over 200 studies that used the TPB to prospectively predict health-related behaviours. The review found that intention and PBC accounted for 19% of the variance in behaviour and that attitude, subjective norms and PBC accounted for 44% of the variance in intention.
Reviews also exist for individual health-related behaviours. Meta-analyses of studies applying the TPB to physical activity (Hagger, Chatzisarantis, & Biddle, Citation2002) and screening (Cooke & French, Citation2008) have found strong positive relationships. In contrast, a meta-analysis of studies applying the TPB to smoking (Topa & Moriano, Citation2010) found weak relationships, with negative PBC–intention and PBC–behaviour relationships. These results suggest the possibility that TPB studies of behaviours that are harmful to health, such as alcohol consumption, may yield different relationships when compared with results for behaviours that are beneficial to health, particularly in relation to PBC. Specifically, individuals may wish to emphasise a lack of control over health risk behaviours, because these behaviours are not seen as socially desirable and may need to be explained away by reference to external causes such as peer pressure (de Visser & McDonnell, Citation2013).
Although previous reviews of health-related behaviours have included data from studies applying the TPB to alcohol consumption, these reviews have several limitations. First, these reviews do not report results for alcohol consumption studies separately; for example, McEachan et al. (Citation2011) combined results from studies of alcohol consumption with studies examining other substance-use behaviours (e.g., drug use, smoking). Second, existing reviews identified few studies applying the TPB to alcohol consumption; McEachan et al. (Citation2011) found only five studies on this topic. However, there has been a recent increase in studies applying the TPB to alcohol use since the endpoint of the review done by McEachan et al. Finally, previous reviews have combined studies of abstinence, episodic drinking and getting drunk, which may obscure differences in the prediction for these different patterns of alcohol consumption.
The present systematic review is needed for three reasons. First, to identify those constructs that are most strongly associated with alcohol consumption intentions and behaviour to inform the development of interventions based on the TPB to reduce alcohol consumption and associated harms. Second, to clarify the impact of PBC on alcohol consumption. Previous research has found PBC to be a poor predictor of alcohol consumption (e.g., Norman, Citation2011). One explanation for this finding is that researchers applying the TPB to predict alcohol consumption vary in how they have measured PBC. PBC has been measured as (i) PC only (e.g., ‘Whether or not I engage in binge drinking in the next week is under my control’, Glassman et al., Citation2010), (ii) SE only (e.g., ‘If I wanted to, I am confident that I could engage in binge drinking in the next week’, Johnston & White, Citation2003) or (iii) a combination of PC and SE (e.g., Cooke, Sniehotta, & Schuez, Citation2007). Third, to identify potential moderators of TPB relationships. Miller, Plant, and Plant (Citation2005) found that pattern of consumption affected the likelihood of individuals experiencing alcohol problems; individuals who consumed all of their alcohol on a few occasions reported more alcohol problems (e.g., accidents, fights) compared with individuals who spread their alcohol consumption over more occasions. Given this, pattern of consumption will be considered as the first potential moderator variable in the meta-analysis. Second, it is likely that males and females experience different pressures to drink, which could affect TPB relationships. For example, de Visser and McDonnell (Citation2013) noted that male students rated alcohol consumption as a masculine behaviour. This may result in great social pressure to drink. In contrast, qualitative research with female students has noted that they focus on the positive behavioural effects of excessive alcohol use (Guise & Gill, Citation2007). As a result, gender differences may be expected in the strength of different TPB relationships for alcohol-use intentions and behaviour. Finally, some researchers (Gibbons & Gerrard, Citation1995; Kuther, Citation2002) claim the TPB has less utility with younger populations because adolescents have less access to alcohol and are less likely to plan alcohol consumption compared to adults. Thus, in the present review, results for TPB relationships were compared between adolescents and adults.
The main aim of the present study is to provide a comprehensive and up-to-date systematic review and meta-analysis of applications of the TPB in the domain of alcohol consumption. Specifically, the present study examines the size of nine relationships within the TPB in the context of alcohol consumption: attitude–intention, subjective norm–intention, PBC–intention, SE–intention, PC–intention, intention–behaviour, PBC–behaviour, SE–behaviour, PC–behaviour. The second aim is to assess the extent to which several moderator variables affect the size of TPB relationships: (i) pattern of consumption, (ii) gender of participants and (iii) age of participants.
Method
Search strategy and inclusion/exclusion criteria
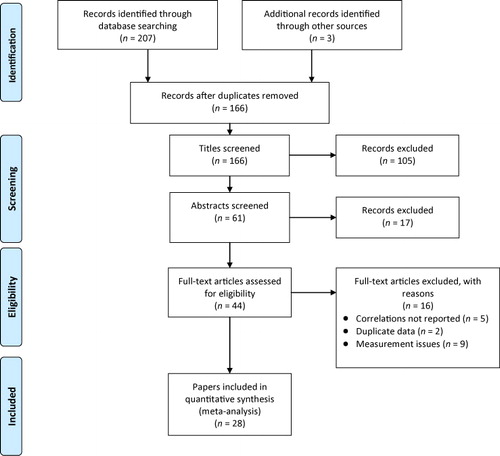
Relevant studies were identified using the following methods: (i) Electronic databases (PubMed and Web of Knowledge) were searched to 7 November 2013, (ii) reference lists of included articles were manually searched and (iii) authors of published articles were contacted to request in press results. The following keywords were used in the electronic searches: ‘theory of planned behavio*’, ‘alcohol’, or ‘binge-drink*’, or ‘harmful drinking’ or ‘heavy drinking’ or ‘intoxication’. The searches generated 166 independent papers, after duplicates were removed, which were then screened according to the following inclusion criteria:
Studies had to report results in English
Studies had to measure intentions to consume alcohol, drink within certain limits or abstinence. We excluded studies reporting interventions to reduce alcohol consumption (Murgraff, Abraham, & McDermott, Citation2007) or investigating drink driving (Rivis, Abraham, & Snook, Citation2011).
Studies had to include direct measures of attitudes, subjective norms and PBC (or PC or SE). This lead to the exclusion of review papers (e.g., Kuther, Citation2002).
A bivariate statistical relationship between TPB constructs and intention had to be retrievable, either from the paper or upon request from the authors.
Selection of studies
The first two authors independently reviewed the titles of the 166 papers for potential relevance to the research question and excluded 105 papers at this stage. The abstracts of the remaining 61 papers were then screened and a further 17 papers were excluded. Full text of potentially eligible papers (n = 44) was then assessed, and 16 papers were excluded for one of three reasons: Five papers were excluded because no correlations were reported, and data could not be retrieved from paper authors, two papers reported data already duplicated in the systematic review, and nine papers were excluded due to measurement issues, such as not measuring intentions (e.g., Kuther & Higgins-D'Alessandro, Citation2003) or using atypical measures (McMillan & Conner, Citation2003). provides a flow chart outlining the screening and eligibility processes. Full details of the excluded papers are provided in Supplementary Table 1.
Data management, extraction and coding
Data were extracted from included papers by the first two authors. Differences in data extraction were resolved following discussion. Where necessary, we contacted the authors of the primary studies to obtain additional information about correlation coefficients and measures used. As noted above, some studies assessed PBC using items assessing PC and SE, whereas other studies included separate measures of PC and SE. As a result, items used to measure PBC in each study were coded independently by the first and third authors. Differences in coding were resolved following discussion. Items were coded as assessing PC (e.g., ‘Whether or not I engage in binge drinking in the next week is under my control’, ‘It is up to me whether or not I engage in binge drinking in the next week’) or SE (e.g., ‘If I wanted to, I am confident that I could engage in binge drinking in the next week’, ‘For me, to engage in binge drinking in the next week would be easy’). On the basis of these codings, measures were categorised as a ‘pure’ measure of PC (i.e., only containing PC items), a ‘pure’ measure of SE (i.e., only containing SE items) or a ‘mixed’ measure of PBC (i.e., containing PC and SE items).
Data extraction identified 20 different definitions of alcohol consumption (see Supplementary Table 2) including, definitions based on governmental guidelines, as well as quantity of drinks consumed, abstinence and ‘getting drunk’. Many definitions focused on consumption of more than multiples of standardised ‘drinks’ or units of alcohol in a single session. For example, in several UK studies, ‘binge-drinking’ was defined in terms of females drinking more than 7 units in a single session, and males drinking more than 10.5 units of alcohol, where a unit is defined as 8 g of pure ethanol. As definitions of consumption varied between countries, consumption levels were converted into total grams of ethanol. After performing these calculations, a bimodal distribution was apparent on either side of 56 g of ethanol, which was therefore chosen as the cut-off point between ‘heavy’ and ‘light’ episodic drinking. The criterion of 56 g of ethanol reflects definitions used by the National Institute of Alcohol Abuse and Alcoholism (Citation2004) to identify problematic drinking for women, as well as early UK definitions of ‘binge-drinking’ in women (i.e., drinking more than 7 units of alcohol in a single session, Health Education Authority, Citation1996). As a result, episodic drinking definitions outlined below focus on women's drinking, which seemed appropriate given that most samples included in the review were predominantly female (see Supplementary Table 3).
Using these calculations, studies were coded by the first and final author into one of five categories: ‘Getting drunk’ = drinking to get drunk (e.g., Wall, Hinson, & McKee, Citation1998), ‘Heavy episodic drinking’ = women drinking more than 56 g of ethanol during a single drinking episode/session (e.g., Norman & Conner, Citation2006), ‘Light episodic drinking’ = women drinking less than 56 g of ethanol during a single drinking episode/session (e.g., Johnston & White, Citation2003), ‘Quantity of drinks consumed’ = participants’ ratings of how likely they were to drink a certain quantity of drinks during a single episode/session (e.g., Jamison & Myers, Citation2008) or ‘Not drinking’ = avoiding alcohol consumption (e.g., Rise & Wilhelmsen, Citation1998). Several studies did not fit these categories (Ajzen & Sheikh, Citation2013; Conner, Warren, Close, & Sparks, Citation1999; Kim & Hong, Citation2013; O'Callaghan, Chant, Callan, & Baglioni, Citation1997; Spijkerman, van den Eijnden, Vitale, & Engels, Citation2004; see Supplementary Table 2 for the definitions used in these studies) and were excluded from moderator analyses examining pattern of consumption.
All studies were coded for gender of participants and mean age of participants. If a study recruited both males and females, it was coded as ‘males and females’, studies that recruited males only were coded ‘males’ and studies that only recruited females were coded ‘females’. To code the age of participants, studies where the sample mean age was 18 or above were coded as ‘adult’, whereas studies where the sample mean age was less than 18 were coded as ‘adolescent’.
Meta-analysis procedure
This meta-analysis is reported in accordance with the PRISMA statement (Liberati et al., Citation2009). Comprehensive Meta-Analysis Version 2.0 (2005, Biostat Inc.) was used to calculate sample-weighted average correlations (r+) based on a random effects model. All analyses are described in line with Cohen's (Citation1992) recommendations where a correlation of r = .10 represents a small effect size, r = .30 represents a medium effect size and r = .50 represents a large effect size. Forest plots are included to provide a graphical representation of the relative strength of correlations included for each TPB relationship. Homogeneity analyses were conducted using the chi-square statistic (Hedges & Olkin, Citation1985) to determine whether variation in the correlations between studies was greater than chance. If the overall χ2 statistic was significant, pairwise Z tests were conducted between all pairs of tests to determine where differences existed in effect size estimates. Publication bias was subjectively assessed using funnel plots and quantitatively assessed using the trim and fill method of Duval and Tweedie.
Multiple samples and multiple measures
Where studies reported separate statistical tests for more than one sample, the correlation coefficient from each sample was used as the unit of analysis (e.g., Rise & Wilhelmsen, Citation1998). Where studies had reported correlations for multiple measures of a single TPB construct, as opposed to a composite variable (e.g., Cooke & French, Citation2011), we used the mean of the reported correlation coefficients. Hagger, Lonsdale, Hein, et al. (Citation2012) reported results from the same sample on two occasions. Because data were collected on separate occasions, it was treated as independent and both sets of correlations were included. Ajzen and Sheikh (Citation2013) reported results for the TPB applied to drinking alcohol and avoiding alcohol, collected from the same sample. Because both behaviours are relevant for inclusion in the present review, the correlations between TPB variables for both behaviours were treated as independent and both sets of correlations were included.
Results
Study characteristics
Based on the above criteria, 28 papers reporting 40 studies were included. Full details of included studies are provided in Supplementary Table 3. The oldest paper included was published in 1997, while most of the research identified has been published since 2006. The majority of studies included were conducted in the UK (k = 20). Research has also been conducted in the USA (k = 4), Norway (k = 4), Australia (k = 3), Canada (k = 3), Germany (k = 2), Estonia (k = 1), the Netherlands (k =1), South Korea (k =1) and Sweden (k = 1). Samples were frequently recruited from universities (k = 33), with female participants, aged 18–25, over-represented. Study sample sizes ranged from 49 to 2814, with most studies reporting sample sizes between 100 and 150.
TPB relationships across studies
summarises the results for TPB relationships across studies. Forest plots for all relationships can be found in Supplementary Figures 1–9. Attitudes had the strongest relationship with intentions (r+ = .62). Subjective norms (r+ = .47) had a stronger relationship with intentions than PBC (r+ = .31). Results for studies using ‘pure’ measures showed that SE (r+ = .48) had a stronger relationship with intentions than the non-significant PC–intention association (r+ = −.10). Four of the six PC studies had negative relationships indicating that a lack of control was associated with higher intentions to drink alcohol. Intention had a large-sized relationship with alcohol consumption (r+ = .54) while SE had a medium-sized relationship (r+ = .41). In contrast, PBC and PC had negative relationships with alcohol consumption (r+ = −.05 and r+ = −.13, respectively), with the PC–behaviour relationship also not being statistically significant. Five of 11 PBC–behaviour relationships and all 6 PC–behaviour relationships were negative.
Table 1. Summary of TPB relationships estimated by random effects meta-analysis.
Funnel plots were generated for each TPB relationship (see Supplementary Figures 10–18). Quantitative assessment of these plots estimated that the review was missing four studies measuring the PBC–intention relationship and seven studies that measured the SE–intention relationship. After accounting for these studies, the random effect sizes would be r+ = .22 for the PBC–intention relationship and r+ = .32 for the SE–intention relationship. We have reason to doubt the existence of missing studies for the SE–intention relationship based on examination of the funnel plot for the SE–intention relationship (see Supplementary Figure 13). A single study (Spijkerman et al., Citation2004) reported a negative correlation (r = −.49), in contrast to all other studies, and was removed from the analyses, to perform a sensitivity analysis. The results indicate no missing studies. Spijkerman et al. differed from most other studies assessing the SE–intention relationship in that it recruited participants aged between 12 and 16 years. At this age, individuals may have limited experience of alcohol consumption, which may have affected their ability to accurately report their SE regarding alcohol consumption.
Tests for heterogeneity for each of the TPB relationships were significant for every relationship apart from the PC–behaviour relationship. Heterogeneity indicates greater variability in effect size estimates between studies than expected on the basis of random sampling error alone, suggesting a need to identify moderators. Results for moderator analyses are reported in and .
Table 2. Effect sizes by pattern of consumption for TPB relationships.
Table 3. Effect sizes by gender of participants and age of participants for attitude–intention, subjective norm–intention, PBC–intention, SE–intention, and intention–behaviour Relationships.
Moderator analyses: pattern of consumption
Most studies investigated either heavy episodic drinking (k = 11) or light episodic drinking (k = 11), with fewer studies investigating not drinking (k = 5), quantity of drinks (k = 3) or getting drunk (k = 3). Pattern of consumption moderated the attitude–intention relationship (χ2(4) = 102.65, p < .001). Studies investigating episodic drinking had statistically significantly larger attitude–intention relationships (r+ = .74 and r+ = .72, for heavy and light patterns, respectively) than all other patterns of consumption. Results from studies of getting drunk (r+ = .57) statistically significantly differed from studies on quantity of drinks and not drinking (r+ = .38 and r+ = .35, respectively). No other differences were found.
Pattern of consumption also moderated subjective norm–intention relationships (χ2(4) = 33.73, p < .001). Relations for light episodic drinking (r+ = .57) were statistically significantly larger than for all other patterns of consumption. Results for heavy episodic drinking (r+ = .48) and not drinking (r+ = .46) statistically significantly differed from quantity of drinking (r+ = .28) and getting drunk (r+ = .21). There were no other differences.
The PBC–intention relationship was moderated by pattern of consumption (χ2(2) = 223.21, p < .001). Studies examining getting drunk reported a negative PBC–intention relationship (r+ = −.46) compared to positive PBC–intention relationships for heavy episodic drinking (r+ = .44) and light episodic drinking (r+ = .55). All values statistically significantly differed from each other. Pattern of consumption also moderated the SE–intention relationship (χ2(3) = 9.91, p = .019). Results for light episodic drinking (r+ = .65) were statistically significantly larger than heavy episodic drinking (r+ = .50), quantity of drinks (r+ = .49) and not drinking (r+ = .40), while results for not drinking were statistically significantly smaller than all other patterns of consumption. No other differences were found. Pattern of consumption did not moderate the PC–intention relationship.
Pattern of consumption moderated the intention–behaviour relationship (χ2(3) = 15.29, p = .002). Light episodic drinking had a statistically significantly larger relationship (r+ = .67) than all other patterns of consumption, with no other differences found. PBC–behaviour relationships for getting drunk (r+ = −.39) were statistically significantly different from relationships for heavy episodic drinking (r+ = .31; Z = 11.11, p < .001). Pattern of consumption did not moderate the SE–behaviour (χ2(2) = 4.60, p = .100) relationship.
Moderator analyses: gender of participants
Studies applying the TPB to predict alcohol consumption typically recruit majority female samples. Whilst the vast majority of studies collected data from female and male participants (k = 30), only seven of the 40 samples reviewed had approximately equal numbers of male and female participants or more males than females in their samples. There were five studies with females only and five studies with males only.
Gender of participants was a statistically significant moderator of attitude–intention relations (χ2(2) = 50.39, p < .001). The attitude–intention relationship for samples with both males and females (r+ = .68) was statistically significantly stronger than equivalent relationships for female-only samples (r+ = .46), which in turn had statistically significantly stronger relationship than for male-only samples (r+ = .36). Gender of participants did not moderate subjective norm–intention, PBC–intention, SE–intention and intention–behaviour relationships. A lack of studies prevented tests of moderation by gender of sample for PC–intention, SE–behaviour, PBC–behaviour or PC–behaviour relationships.
Moderator analyses: age of participants
Although most studies (k = 35) reported data from adult samples, two studies collected data from adults who were not university students (Hagger, Lonsdale, Hein, et al., Citation2012; Kim & Hong, Citation2013). Five adolescent samples were also identified. Adults’ attitudes had a larger association with their intentions (r+ = .65) compared with adolescents’ attitudes (r+ = .40; Z = 18.70, p < .001). The SE–intention relationship was statistically significantly larger for adults (r+ = .57) compared to adolescents (r+ = .22; Z = 17.59, p < .001). Age of participants did not moderate subjective norm–intention relations. A lack of studies prevented tests of moderation by age of sample for PBC–intention, PC–intention, intention–behaviour, SE–behaviour, PBC–behaviour or PC–behaviour relationships. As none of the studies with adolescent samples collected behavioural data, it was not possible to test moderation of TPB relationships with behaviour by age of participants.
Discussion
Overall, the current meta-analysis supports the utility of the TPB when applied to alcohol consumption intentions and behaviour; medium-to-large effect sizes were found for many, but not all, of the TPB relationships. Considering alcohol consumption intentions, strong correlations were found for attitude and subjective norm, and a medium correlation was found for PBC. In addition, SE also had a strong correlation with intention, whereas PC had a small, negative and non-significant correlation. Considering alcohol consumption behaviour, intention had a strong correlation with behaviour, whereas the correlation for PBC was small, negative and non-significant. In addition, SE had a medium-to-strong correlation with behaviour, whereas PC had a small negative correlation.
The results presented in the current systematic review and meta-analysis are broadly similar to those presented in previous reviews of the TPB applied to health behaviours (McEachan et al., Citation2011; Topa & Moriano, Citation2010). Similar to the review of health behaviours done by McEachan et al., we found that attitudes had the strongest relationship with intentions and that intentions had the strongest relationship with behaviour. The subjective norm–intention relationship reported in the current review was larger than is typically reported and may reflect the social nature of alcohol consumption. Results for PBC were similar to the review of studies applying the TPB to smoking by Topa and Moriano (Citation2010), with medium and small correlations being identified. These effects are smaller than those reported by McEachan et al. (Citation2011), and given that their results were based mainly on health promotion behaviours, this implies that correlations between PBC and intention and PBC and behaviour are smaller for health risk behaviours than health promotion behaviours.
Pattern of consumption and age and gender of sample moderated some relationships. Specifically, studies that used precise definitions of alcohol consumption (e.g., where participants were asked to respond in relation to drinking more than a specified number of units of alcohol on a single occasion) reported stronger TPB relationships than studies that used vague definitions (e.g., getting drunk). Females had larger attitude–intention relationships than males, and adults had stronger attitude–intention and SE–intention relationships than adolescents.
Pattern of consumption
Pattern of consumption moderated the size of TPB relationships; large or medium correlations were found in studies focusing on episodic drinking, whereas studies on ‘getting drunk’ typically reported small correlations. These findings are in accordance with the principle of compatibility, the idea that items measuring TPB constructs should be specified at the same level of generality as items measuring behaviour (Ajzen & Fishbein, Citation1980). The definitions given for episodic drinking were precise, indicating consumption of more than the specified multiples of precisely defined quantities of alcohol. Thus, when the action and measures are less ambiguous, associations between TPB variables are increased, whereas when participants are less clear about the exact behaviours they are being asked about, associations between TPB variables are decreased, i.e., ‘getting drunk’ is open to interpretation by participants. Researchers need to precisely define the behaviours they are examining when constructing TPB items for use in studies on alcohol consumption. In addition, analyses by pattern of consumption also showed that certain patterns of consumption have not been addressed by researchers using the TPB, including frequent consumption spread over the week and problematic or dependent drinking.
Gender of participants
Analysis by gender indicated that the attitude–intention relationship was the only relationship moderated by gender; females reported stronger attitude–intention correlations than men. Previous qualitative work has highlighted that females may focus on the expected positive outcomes of drinking alcohol (which underlie attitudes; Guise & Gill, Citation2007), whereas men may be more influenced by masculinity concerns and consequent social pressures to drink (de Visser & McDonnell, Citation2013). Further research is needed to explore the motivations, or reasons, underlying the drinking behaviour of males and females. However, it should be noted that this comparison is based on five female-only and five male-only samples, so caution is required when drawing conclusions. The results could also be confounded by other moderators, such as patterns of consumption and age groups.
Age of participants
Previous research (Gibbons & Gerrard, Citation1995; Kuther, Citation2002) has argued that the TPB is not suitable for use with younger populations because adolescents are less likely to plan alcohol consumption compared to adults, not least because alcohol consumption is harder for adolescents because it is usually illegal for them to purchase it. The present review found some support for the idea that the TPB has greater utility when applied to adults’ alcohol intentions than adolescents’ alcohol intentions. For example, adults’ attitudes and SE had large correlations with their intentions, whereas adolescents’ attitudes and SE had medium and small, respectively, correlations with intentions. One potential confound in this analysis is that four of the five adolescent samples focused on not drinking (e.g., Rise & Wilhelmsen, Citation1998), whereas only one of the adult samples focused on not drinking (i.e., Ajzen & Sheikh, Citation2013). Therefore, it may be that results for the two groups differ due to the pattern of consumption. As there were only five adolescent data sets, these results should be interpreted with caution. Future research is needed that focuses on both drinking and not drinking in adults and adolescents.
Nature of the PBC construct
A key finding from this review is the variation between studies in how PBC is operationalised. Ajzen (Citation2002) views PBC as a combination of perceived control (PC) and SE. Studies included in this review were found to employ ‘pure’ measures of PC and SE as well as ‘mixed’ measures of PBC that included both PC and SE items. These different measures were found to have different relationships with intentions and behaviour. PBC had a medium correlation with intention, but a small, negative correlation with behaviour. SE had a strong correlation with intentions and a medium-to-strong correlation with behaviour, whereas PC had small negative correlations with intention and behaviour. Thus, higher confidence (i.e., SE) in one's ability to consume alcohol is associated with stronger intentions to consume and higher consumption. In contrast, stronger perceptions of control over alcohol consumption are not always associated with stronger intentions to consume alcohol. Instead, weaker perceptions of control over alcohol consumption were associated with higher levels of alcohol consumption. Three possible explanations for these effects are considered below.
First, it is likely that people are more accurate in their perceptions of SE relative to their perceptions of PC. Individuals may overestimate the extent to which alcohol consumption is volitional and underestimate the impact of external factors (e.g., peer pressure, celebrations) on their alcohol consumption. Greater accuracy for SE relative to PC could account for the stronger relationships.
Second, participants may misinterpret what PBC items refer to. French, Cooke, McLean, Williams, and Sutton (Citation2007) found that when asked to ‘think aloud’ while completing a TPB questionnaire measuring ‘binge-drinking’ several participants misinterpreted what the PBC items referred to. Participants interpreted PBC items as asking about control over behaviour performed when drunk, i.e., acting irresponsibly, rather than control over their drinking behaviour. Such misinterpretations are likely to weaken relationships between measures of PBC that assess perceptions of control and alcohol intentions and behaviour. Equally, it has been argued (e.g., Skinner, Citation1996) there has been a shift in the definition of SE over time, with Bandura moving from SE defined in terms of control over behaviour (e.g., alcohol consumption, Bandura, Citation1977) to SE defined in terms of control over ends (e.g., avoiding hangovers by limiting alcohol consumption, Bandura, Citation1997). A consequence of this change is that measures of SE are typically contaminated by outcome expectancies (Williams, Citation2010), so correlations with SE may be an artefact due to also assessing aspects of attitude with these items. This may account for the greater correlation between SE and intentions and behaviour relative to PBC.
Third, participants may want to attribute a lack of control over their alcohol consumption, depending on the pattern of consumption they are asked about.
Pattern of consumption moderated the PBC–intention relationship showing a medium-sized negative relationship for ‘getting drunk’ and a large-sized positive relationship for light episodic drinking. Thus, individuals may want to emphasise control over light episodic drinking, because they view this pattern of consumption as socially desirable, but deny control over getting drunk, because this is seen as socially undesirable. As a whole, these findings indicate the importance of conceptual and operational clarity over constructs.
Gaps in the literature
The most notable gap identified in the present review is the dearth of studies looking at other patterns of alcohol consumption, notably long-term heavy drinking, which is a key behaviour to understand to reduce disease burden. For example, in their longitudinal study of untreated heavy drinkers, Rolfe, Orford, and Martin (Citation2009) noted that this population use hospital services at a higher rate than the general population. Schlegel, D'Avernas, Zanna, DeCourtville, and Manske (Citation1992) noted that among problem drinkers (i.e., individuals who drank at levels associated with alcohol-related problems), PBC, but not intention, predicted alcohol consumption. Conversely, among non-problem drinkers, intentions, but not PBC, predicted consumption. Thus, prediction of alcohol consumption by the TPB may be dependent on whether individuals have been engaged in long-term, heavy, alcohol consumption. Furthermore, researchers should consider measuring TPB constructs regarding both abstaining and consuming in the same population. For example, Richetin, Conner, and Perugini (Citation2011) found that intentions to abstain from performing behaviour are not the opposite of intentions to engage in behaviour. They also found that both types of intentions could have predictive utility in relation to future behaviour.
Future research applying the TPB to alcohol intentions and behaviour should collect more data from male-only or majority male samples. Given that men consume more alcohol than women (Lader & Goddard, Citation2006), it is important to know if results reported in this review paper represent men as well as women. Similarly, more data from younger and older samples would be welcome. Only two studies (Rise & Wilhelmsen, Citation1998; Spijkerman et al., Citation2004) recruited adolescent samples and only two studies (Hagger, Lonsdale, Hein, et al., Citation2012; Kim & Hong, Citation2013) recruited non-undergraduate, adult, samples. Therefore, future work is needed to confirm the suitability of the TPB for use with non-undergraduate samples.
The reasons why PC, PBC and SE have different patterns of association with intentions and behaviour warrants further investigation. In particular, it is essential that future research uses clearly distinct measures of PC and SE. Johnston et al. (Citation2014) used discriminant content validity to examine whether common PBC and SE items assessed were distinct. Experts were asked to code items as either PBC, SE, both or neither based on construct definitions. PBC items were coded inconsistently (i.e., two items were coded as PBC, one as SE and two as neither), whereas experts consistently coded SE items as SE. Applying this method to alcohol consumption behaviours would help to ensure the content validity of measures used in future tests of the predictive validity of PC and SE. Researchers looking to develop measures are advised to use manuals that have been created to help standardise measures used in TPB research (see Ajzen, Citation2006; Francis et al., Citation2004).
Future research applying the TPB to alcohol consumption should make greater use of the TACT (Target, Action, Context, Time; Ajzen & Fishbein, Citation1980) principle when designing items. This principle aims to improve the quality of TPB items tapping constructs by ensuring that participants know (i) who is the target of the item (e.g., them), (ii) what action is being considered (e.g., heavy episodic drinking), (iii) the context where the action is located (e.g., bar) and (iv) what is the timeframe for the action (e.g., 1 week). Applying this principle to the items reviewed shows that authors always clarify the target, rarely consider context (cf. Cooke & French, Citation2011) and vary in the action and timeframe they reference. Although variation between studies is to be expected, identifying 20 definitions of alcohol consumption across 28 included papers suggests that researchers need to collaborate more on how to define alcohol consumption (e.g., Rehm et al. Citation2013). This is important because the specificity of the action moderated the size of TPB relationships.
The current results provide good evidence for the utility of the TPB in relation to alcohol consumption. Nonetheless, the TPB is not without its limitations as highlighted in a recent critique by Sniehotta, Presseau, and Araújo-Soares (Citation2014) (and discussed in subsequent commentaries, e.g., Ajzen, Citation2014; Armitage, Citation2014). First, the TPB does not fully account for the influence of other variables on health-related intentions and behaviour. For example, many TPB studies have found a direct (i.e., unmediated) effect of past behaviour on future behaviour, including studies on alcohol consumption (e.g., Cooke et al., Citation2007; Norman & Conner, Citation2006; Norman, Armitage, & Quigley, Citation2007). Such findings call into question the sufficiency of the TPB and suggest the influence of automatic as well as intentional processes on alcohol-related behaviour (Norman, Citation2011). Second, the TPB provides a better explanation of intention than behaviour. In particular, Schwarzer (Citation2014) makes the distinction between goal setting (motivation, intention formation) and goal pursuit (volition, action) and argues that the TPB is primarily a theory of intention formation. As a result, to fully explain alcohol-related behaviour, the TPB may need to incorporate addition, post-intentional, variables. Third, there are few experimental tests of the TPB and none on alcohol-related behaviour. Such experimental tests provide the ultimate test of theory.
Interventions to reduce alcohol consumption
Based on the overall analysis, it is recommended that interventions aimed at reducing alcohol consumption intentions should target attitudes, subjective norms and SE. While considerable research has focused on interventions targeting norms (e.g., Campo et al., Citation2003), less work has targeted attitudes and/or SE to reduce alcohol intentions. The lack of interventions targeting control constructs may be due to the inconsistency in associations between intention and PBC identified in these studies. The effects for SE may offer a promising avenue for intervention research, particularly as SE is also associated with alcohol consumption. Rather than decrease an individual's confidence to drink (which might be difficult), interventions could seek to increase SE about the avoidance of certain types of alcohol consumption behaviours. For example, Murgraff et al. (Citation2007) found that a brief intervention that included messages and strategies to strengthen SE to reduce alcohol consumption had a positive effect on SE levels and subsequent drinking behaviour.
Strengths and weaknesses
The present meta-analysis has a number of strengths. First, the paper captures the recent surge in research testing the TPB as a model of alcohol consumption intentions and behaviour. Second, past reviews of the TPB have combined studies on alcohol consumption with other substance-use behaviours, making for imprecise estimates of the effects for the TPB applied to alcohol. Third, the paper complements meta-analysis of the TPB applied to smoking done by Topa and Moriano (Citation2010), by finding a negative PBC–behaviour relationship in studies on alcohol consumption, implying that individuals have a lack of control over performing risky behaviours. Health risk behaviours are usually viewed as enjoyable, but socially undesirable (French & Cooke, Citation2012), so individuals may overestimate their capacity to resist engaging in such behaviours, especially when performing these behaviours only once over a typical period of 2 weeks counts as a ‘binge’ or ‘relapse’ in these studies and hence failure of control.
The present systematic review and meta-analysis also has some limitations. First, we had to create a coding system to examine the pattern of consumption moderator analysis. Analyses by pattern of consumption helped to highlight differences in results; however, we note that this system may need further refinement. Furthermore, because none of the studies investigated determinants of drinking on multiple occasions, we were not able to consider this pattern of consumption in the review. Researchers are encouraged to apply the TPB to predict determinants of drinking on multiple occasions, because this pattern of consumption seems particularly hazardous (Miller et al., Citation2005). Second, some of the moderator analyses can be criticised for having few studies available for some comparisons and meta-analysis results. For example, only five studies collected data from adolescent samples. Moreover, due to a lack of studies, it was not possible to fully explore the possibility that there were confounding variables that might account for some of the moderator effects. Nevertheless, we feel that these analyses are useful to generate hypotheses for future research and the number of samples analysed are comparable to previous meta-analyses. A recent systematic review of Cochrane reviews (Davey, Turner, Clarke & Higgins, Citation2011) noted that the median number of studies included in meta-analyses was three. Thus, analyses presented in this review are comparable with those reported elsewhere. Third, behaviour was always assessed by self-report, which is problematic as previous TPB meta-analyses have reported stronger effect sizes for TPB studies using self-report measures compared to objective measures (Armitage & Conner, Citation2001; McEachan et al., Citation2011). Future studies need to apply the TPB to predict objective measures of alcohol consumption, including indirect measures such as blood alcohol content measured by a breathalyser, alcohol test strips or hair analysis.
Conclusion
The present systematic review and meta-analysis provides support for the utility of the TPB applied to alcohol consumption and intentions. In particular, attitudes, subjective norms and SE had large-sized relationships with intentions which, in turn had a large-sized relationship with behaviour. Thus, interventions to reduce alcohol consumption should target attitudes, subjective norms and SE as a means to alter intentions, and ultimately, reduce alcohol consumption. Additionally, researchers are urged to use the TACT principle when designing measures to use in future research and to apply the TPB to predict long-term, heavy, alcohol consumption.
Supplemental data
Supplemental data (Supplementary Tables 1–3 and Supplementary Figures 1–18) for this article can be accessed here: http://dx.doi.org/10.1080/17437199.2014.947547.
Supplementary_Table1.pdf
Download PDF (209 KB)PRISMA_2009_Checklist.pdf
Download PDF (83.7 KB)Supplemental_Figures_1_18.pdf
Download PDF (83.2 KB)References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. doi:10.1016/0749-5978(91)90020-T
- Ajzen, I. (2002). Perceived behavioral control, self-efficacy, locus of control and the theory of planned behavior. Journal of Applied Social Psychology, 32, 665–683. doi:10.1111/j.1559-1816.2002.tb00236.x
- Ajzen, I. (2006). Constructing a theory of planned behavior questionnaire: Conceptual and methodological considerations. Retrieved from http://people.umass.edu/∼aizen/pdf/tpb.measurement.pdf
- Ajzen, I. (2014). The theory of planned behaviour is alive and well, and not ready to retire: A commentary on Sniehotta, Presseau and Araújo-Soares. Health Psychology Review. doi:10.1080/17437199.2014.883474
- Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice Hall.
- Ajzen, I., & Sheikh, S. (2013). Action versus inaction: Anticipated affect in the theory of planned behavior. Journal of Applied Social Psychology, 43, 155–162. doi:10.1111/j.1559-1816.2012.00989.x
- Armitage, C. (2014). Time to retire the theory of planned behaviour? Health Psychology Review. doi:10.1080/17437199.2014.892148
- Armitage, C. J., & Conner, M. (2001). Efficacy of the theory of planned behaviour: A meta-analytic review. British Journal of Social Psychology, 40, 471–499. doi:10.1348/014466601164939
- Armitage, C. J., Norman, P., & Conner, M. (2002). Can the theory of planned behaviour mediate the effects of age, gender and multidimensional health locus of control? British Journal of Health Psychology, 7, 299–316. doi:10.1348/135910702760213698
- Babor, T., Caetano, R., Casswell, S., Edwards, G., Giesbrecht, N., Graham, K., & Rossow, I. (2010). Alcohol: no ordinary commodity (2nd ed.). Oxford: OUP.
- Bandura, A. (1977). Social learning theory. Englewood Cliffs, NJ: Prentice Hall.
- Bandura, A. (1997). Self-efficacy: The exercise of control. New York: WH Freeman.
- British Liver Trust. (2009, January). British Liver Trust analysis of ONS mortality statistics covering all deaths related to liver dysfunction covering ICD K70-76 and other codes including C22-24 (liver cancer), and B15-B19 (viral hepatitis). Retrieved from http://www.britishlivertrust.org.uk/about-us/media-centre/facts-about-liver-disease/
- Campo, S., Brossard, D., Frazer, M. S., Marchell, T., Lewis, D., & Talbot, J. (2003). Are social norms campaigns really magic bullets? Assessing the effects of students’ misperceptions on drinking behavior. Health Communication, 15, 481–497. doi:10.1207/S15327027HC1504_06
- Centers for Disease Control and Prevention (2011). Fact sheets: Binge drinking. Retrieved from http://www.cdc.gov/alcohol/fact-sheets/bingedrinking.htm
- Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159. doi:10.1037/0033-2909.112.1.155
- Conner, M., & Sparks, P. (2005). Theory of planned behaviour and health behaviour. In M. Conner & P. Norman (Eds.), Predicting health behaviour (2nd ed., pp. 170–222). Maidenhead: OUP.
- Conner, M., Warren, R., Close, S., & Sparks, P. (1999). Alcohol consumption and the theory of planned behavior: An examination of the cognitive mediation of past behavior. Journal of Applied Social Psychology, 29, 1676–1704. doi:10.1111/j.1559-1816.1999.tb02046.x
- Cooke, R., & French, D. P. (2008). How well do the theory of reasoned action and theory of planned behaviour predict intentions and attendance at screening programmes? A meta-analysis. Psychology & Health, 23, 745–765. doi:10.1080/08870440701544437
- Cooke, R., & French, D. P. (2011). The role of context and timeframe in moderating relationships within the theory of planned behaviour? Psychology & Health, 26, 1225–1240. doi:10.1080/08870446.2011.572260
- Cooke, R., Sniehotta, F., & Schuez, B. (2007). Predicting binge-drinking behaviour using an extended TPB: Examining the impact of anticipated regret and descriptive norms. Alcohol & Alcoholism, 42, 84–91. doi:10.1093/alcalc/agl115
- Davey, J., Turner, R. M., Clarke, M. J., & Higgins, J. P. (2011). Characteristics of meta-analyses and their component studies in the Cochrane database of systematic reviews: A cross-sectional, descriptive analysis. BMC Medical Research Methodology, 11(1), 160. doi:10.1136/bmj.327.7414.557
- de Visser, R. O., & McDonnell, E. J. (2013). “Man points”: Masculine capital and young men's health. Health Psychology, 32(1), 5–14. doi:10.1037/a0029045
- Elliot, M. A., & Ainsworth, K. (2012). Predicting university undergraduates’ binge-drinking behavior: A comparative test of the one- and two-component theories of planned behavior. Addictive Behaviors, 37(1), 92–101. doi:10.1016/j.addbeh.2011.09.005
- Francis, J. J., Eccles, M. P., Johnston, M., Walker, A., Grimshaw, J., Foy, R., … Bonetti, D. (2004). Constructing questionnaires based on the theory of planned behaviour: A manual for health service researchers. Retrieved from http://www.bangor.ac.uk/∼pes004/exercise_psych/downloads/tpb_manual.pdf
- French, D. P., & Cooke, R. (2012). Using the theory of planned behaviour to understand binge drinking: The importance of beliefs for developing interventions. British Journal of Health Psychology, 17, 1–17. doi:10.1111/j.2044-8287.2010.02010.x
- French, D. P., Cooke, R., McLean, N., Williams, M., & Sutton, S. (2007). What do people think about when they answer theory of planned behaviour questionnaires? A ‘Think Aloud’ study. Journal of Health Psychology, 12, 672–687. doi:10.1177/1359105307078174
- Gagnon, H., Tessier, S., Cote, J., April, N., & Julien, A.-S. (2012). Psychosocial factors and beliefs related to intention to not binge drink among young adults. Alcohol & Alcoholism, 47, 525–532. doi:10.1093/alcalc/ags049
- Gardner, B., de Bruijn, G.-J., & Lally, P. (2012). Habit, identity, and repetitive action: A prospective study of binge-drinking in UK students. British Journal of Health Psychology, 17, 565–581. doi:10.1111/j.2044-8287.2011.02056.x
- Gibbons, F. X., & Gerrard, M. (1995). Predicting young-adults health risk behavior. Journal of Personality and Social Psychology, 69, 505–517. doi:10.1037/0022-3514.69.3.505
- Glassman, T., Braun, R. E., Dodd, V., Miller, J. M., & Miller, E. M. (2010). Using the theory of planned behavior to explain the drinking motivations of social, high-risk, and extreme drinkers on game day. Journal of Community Health, 35(2), 172–181. doi:10.1007/s10900-009-9205-1
- Guise, J. M. F., & Gill, J. S. (2007). “Binge drinking? It's good, it's harmless fun”: A discourse analysis of accounts of female undergraduate drinking in Scotland. Health Education Research, 22, 895–906. doi:10.1093/her/cym034
- Hagger, M. S., Anderson, M., Kyriakaki, M., & Darkings, S. (2007). Aspects of identity and their influence on intentional behavior: Comparing effects for three health behaviors. Personality & Individual Differences, 42, 355–367. doi:10.1016/j.paid.2006.07.017
- Hagger, M. S., Chatzisarantis, N. L. D, & Biddle, S. J. H. (2002). A meta-analytic review of the theories of reasoned action and planned behavior in physical activity: Predictive validity and the contribution of additional variables. Journal of Sports & Exercise Psychology, 24, 3–32.
- Hagger, M. S., Lonsdale, A. J., Hein, V., Koka, A., Lintunen, T., Pasi, H., … Chatzisarantis, N. L. D. (2012). Predicting alcohol consumption and binge drinking in company employees: An application of planned behaviour and self-determination theories. British Journal of Health Psychology, 17, 379–407. doi:10.1111/j.2044-8287.2011.02043.x
- Hagger, M. S., Lonsdale, A., Koka, A., Hein, V., Pasi, H., Lintunen, T., & Chatzisarantis, N. L. D. (2012). An intervention to reduce alcohol consumption in undergraduate students using implementation intentions and mental simulations: A cross-national study. International Journal of Behavioral Medicine, 19, 82–96. doi:10.1007/s12529-011-9163-8
- Health Education Authority (1996). Think about a drink: There's more to drink than you think. London: Author.
- Hedges, L., & Olkin, I. (1985). Statistical methods for meta-analysis. New York: Academic Press.
- Home Office. (2009). British crime survey, 2007–2008. Colchester: Essex.
- Jamison, J., & Myers, L. B. (2008). Peer-group and price influence students drinking along with planned behaviour. Alcohol & Alcoholism, 43, 492–497. doi:10.1093/alcalc/agn033
- Johnston, K. L., & White, K. M. (2003). Binge-drinking: A test of the role of group norms in the theory of planned behaviour. Psychology & Health, 18, 63–77. doi:10.1080/0887044021000037835
- Johnston, M., Dixon, D., Hart, J., Glidewell, L., Schröder, C., & Pollard, B. (2014). Discriminant content validity: A quantitative methodology for assessing content of theory-based measures, with illustrative applications. British Journal of Health Psychology, 19, 240–257. doi:10.1111/bjhp.12095
- Jones, L., Bellis, M. A., Dedman, D., Sumnall, H., & Tocque, K. (2008). Alcohol attributable fractions for England: Alcohol attributable mortality and hospital admissions. North-West Public Health Observatory and Department of Health. Retrieved from http://www.nwph.net/nwpho/publications/alcoholattributablefractions.pdf
- Kim, Y., & Hong, O. (2013). Understanding controlled drinking behaviour among Korean male workers. American Journal of Health Behavior, 37, 181–189. doi:10.5993/AJHB.37.2.5
- Kuther, T. L. (2002). Rational decision perspectives on alcohol consumption by youth. Addictive Behaviors, 27(1), 35–47. doi:10.1016/S0306-4603(00)00161-1
- Kuther, T. L., & Higgins-D'Alessandro, A. (2003). Attitudinal and normative predictors of alcohol use by older adults. Journal of Drug Education, 33(1), 71–90. doi:10.2190/G0PR-XVHT-JL92-HE8T
- Lader, D., & Goddard, E. (2006). Drinking: Adults behaviour and knowledge in 2006: November 2006, Omnibus Survey Report number 31. London: ONS.
- Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., … Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Medicine, 6(7), e1000100. doi:10.1371/journal.pmed.1000100.s002
- McEachan, R. R. C., Conner, M., Taylor, N. J., & Lawton, R. J. (2011). Prospective prediction of health-related behaviours with the theory of planned behaviour: A meta-analysis. Health Psychology Review, 5(2), 97–144. doi:10.1080/17437199.2010.521684
- McMillan, B., & Conner, M. (2003). Using the theory of planned behaviour to understand alcohol and tobacco use in students. Psychology, Health & Medicine, 8, 317–328.
- Miller, P., Plant, M., & Plant, M. (2005). Spreading out or concentrating weekly consumption: Alcohol problems and other consequences within a UK population sample. Alcohol & Alcoholism, 40, 461–468. doi:10.1093/alcalc/agh169
- Murgraff, V., Abraham, C., McDermott, M. R. (2007). Reducing Friday alcohol consumption among moderate women drinkers. Alcohol & Alcoholism, 42(1), 37–41. doi:10.1093/alcalc/agl083
- National Institute of Alcohol Abuse and Alcoholism. (2004). NIAAA council approves definition of binge drinking. NIAAA Newsletter, 3, p. 3. Retrieved from http://pubs.niaaa.nih.gov/publications/Newsletter/winter2004/Newsletter_Number3.pdf.
- Norman, P. (2011). The theory of planned behavior and binge drinking among undergraduate students: Assessing the impact of habit strength. Addictive Behaviors, 36, 502–507. doi:10.1016/j.addbeh.2011.01.025
- Norman, P., Armitage, C. J., & Quigley, C. (2007). The theory of planned behavior and binge drinking: Assessing the impact of binge drinker prototypes. Addictive Behaviors, 32, 1753–1768. doi:10.1016/j.addbeh.2006.12.009
- Norman, P., & Conner, M. (2006). The theory of planned behaviour and binge drinking: Assessing the moderating role of past behaviour within the theory of planned behaviour. British Journal of Health Psychology, 11, 55–70. doi:10.1348/135910705X43741
- Norman, P., Conner, M. T., & Stride, C. B. (2012). Reasons for binge drinking among undergraduate students: An application of behavioural reasoning theory. British Journal of Health Psychology, 17, 682–698. doi:10.1111/j.2044-8287.2012.02065.x
- O'Callaghan, F. V., Chant, D. C., Callan, V. J., & Baglioni, A. (1997). Models of alcohol use by young adults: An examination of various attitude-behavior theories. Journal of Studies on Alcohol, 58, 502–507.
- Park, H. S., Klein, K. A., Smith, S., & Martell, D. (2009). Separating subjective norms, university descriptive and injunctive norms, and U.S. descriptive and injunctive norms for drinking behavior intentions. Health Communication, 24, 746–751. doi:10.1080/10410230903265912
- Rehm, J., Marmet, S., Anderson, P., Gual, A., Nutt, D., Room, R., … Gmel, G. (2013). Defining substance use disorders: Do we really need more than heavy use? Alcohol & Alcoholism, 48, 633–640. doi:10.1093/alcalc/agt127
- Richetin, J., Conner, M., & Perugini, M. (2011). Not doing is not the opposite of doing: Implications for attitudinal models of behavioral prediction. Personality & Social Psychology Bulletin, 37, 40–54. doi:10.1177/0146167210390522
- Rise, J., & Wilhelmsen, B. U. (1998). Prediction of adolescents’ intention not to drink alcohol: Theory of planned behaviour. American Journal of Health Behavior, 22, 206–217.
- Rivis, A., Abraham, C., Snook, S. (2011). Understanding young and older male drivers’ willingness to drive while intoxicated: The predictive utility of constructs specified by the theory of planned behaviour and the prototype willingness model. British Journal of Health Psychology, 16, 445–456. doi:10.1348/135910710X522662
- Rolfe, A., Orford, J., & Martin, O. (2009). Birmingham untreated heavy drinkers project final report. London: Department of Health. Retrieved from https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/215795/dh_123886.pdf
- Schlegel, R. P., D'Avernas, J. R., Zanna, M. P., DeCourville, N. H., & Manske, S. R. (1992). Problem drinking: A problem for the theory of reasoned action?. Journal of Applied Social Psychology, 22, 358–385. doi:10.1111/j.1559-1816.1992.tb01545.x
- Schwarzer, R. (2014). Life and death of health behaviour theories. Health Psychology Review, 8(1), 53–56. doi:10.1080/17437199.2013.810959
- Skinner, E. A. (1996). A guide to constructs of control. Journal of Personality and Social Psychology, 71, 549–570. doi:10.1037/0022-3514.71.3.549
- Sniehotta, F. F., Presseau, J., & Araújo-Soares, V. (2014). Time to retire the theory of planned behaviour. Health Psychology Review, 8, 1–7. doi:10.1080/17437199.2013.869710
- Spijkerman, R., van den Eijnden, R. J. J. M., Vitale, S., & Engels, R. C. M. E. (2004). Explaining adolescents’ smoking and drinking behavior: The concept of smoker and drinker prototypes in relation to variables of the theory of planned behavior. Addictive Behaviors, 29, 1615–1622. doi:10.1016/j.addbeh.2004.02.030
- Todd, J., & Mullan, B. (2011). Using the theory of planned behaviour and prototype willingness model to target binge drinking in female undergraduate university students. Addictive Behaviors, 36, 980–986. doi:10.1016/j.addbeh.2011.05.010
- Topa, G., & Moriano, J. A. (2010). Theory of planned behaviour and smoking: meta-analysis and SEM model. Substance Abuse and Rehabilitation, 1, 23–33. doi:10.2147/SAR.S15168
- Wall, A. M., Hinson, R. E., & McKee, S. A. (1998). Alcohol outcome expectancies, attitudes toward drinking and the theory of planned behaviour. Journal of Studies on Alcohol, 59, 409–414.
- Williams, D. M. (2010). Outcome expectancy and self-efficacy: Theoretical implications of an unresolved contradiction. Personality and Social Psychology Review, 14, 417–425. doi:10.1177/1088868310368802
- WHO. (2002). The World Health Report: Reducing risks to health, promoting health life. Retrieved from http://www.who.int/wht/2002/en
- Woolfsen, L. M., & Maguire, L. (2010). Binge drinking in a sample of Scottish undergraduate students. Journal of Youth Studies, 13, 647–659. doi:10.1080/13676261003801804
- Zimmerman, F., & Sieverding, M. (2010). Young adults’ social drinking as explained by an augmented theory of planned behaviour: The roles of prototypes, willingness, and gender. British Journal of Health Psychology, 15, 561–581. doi:10.1348/135910709X476558