
ABSTRACT
Many people self-weigh and many interventions addressing weight-related problems such as obesity promote self-weighing. However, while self-weighing has been associated with weight loss, there is mixed evidence regarding the psychological impact of this behaviour. The present review aimed to quantify the relationship between self-weighing and: (i) affect (e.g., anxiety, depression); (ii) psychological functioning (e.g., self-esteem); (iii) body-related attitudes and (iv) disordered eating. A computerized search of scientific databases in September 2014 and subsequent ancestry and citation searches identified 29 independent tests of the relationship between self-weighing on psychological outcomes. Meta-analysis was used to quantify the size of the association across the tests. Results indicated that there was no association between self-weighing and affect, body-related attitudes or disordered eating. There was, however, a small-sized negative association between self-weighing and psychological functioning. The age of participants, obesity status, the extent of weight loss, duration of self-weighing and study design (RCT versus correlational) were found to influence at least some of the psychological outcomes of self-weighing. The findings suggest that, for the most part, self-weighing is not associated with adverse psychological outcomes. However, in some cases the association between self-weighing and psychological outcomes may be more negative than in others.
Faced with a growing obesity problem, interventions have been – and are being – designed to help individuals to lose weight or avoid weight gain. These interventions include regular exercise, self-monitoring of dietary intake, and regular self-weighing. Of the three, self-weighing is perhaps the simplest method, and has been repeatedly shown to help people to lose or maintain weight (e.g., Klem, Wing, McGuire, Seagle, & Hill, Citation1997; McGuire, Wing, Klem, & Hill, Citation1999; Qi & Dennis, Citation2000; Wing & Phelan, Citation2005; for a recent review, see Zheng et al., Citation2015). Self-weighing is believed to be effective because it allows people to monitor their progress, detect changes in their weight, and apply corrective action if needed (Chambers & Swanson, Citation2012). This is perhaps also why many people weigh themselves on a regular basis, even if they are not taking part in a specific intervention designed to promote weight loss (Mercurio & Rima, Citation2011; Quick, Loth, MacLehose, Linde, & Neumark-Sztainer, Citation2013). The process of monitoring progress is considered central to several models of goal directed behaviour such as Control Theory (Carver & Scheier, Citation1982; Powers, Citation1973). Progress monitoring involves comparing the current state (in this case, current weight) to a desired state or goal (e.g., to lose 2 lb), in order to decide whether corrective action is required, and has been found to promote goal attainment across a range of domains (e.g., Harkin et al., Citation2016; Michie, Abraham, Whittington, McAteer, & Gupta, Citation2009).
However, self-weighing as a means of monitoring progress towards weight-related goals may be a ‘double-edged sword’ (Dionne &Yeudall, Citation2005), as evidence suggests that it can be associated with psychological distress (Ogden & Whyman, Citation1997; Quick et al., Citation2013), lower levels of body satisfaction (Mercurio & Rima, Citation2011) and problematic dietary behaviour such as binge eating and skipping meals (Neumark-Sztainer, van den Berg, Hannan, & Story, Citation2006). For example, Ogden and Whyman (Citation1997) asked a group of female volunteers to weigh themselves daily for two weeks, while those in the control group were weighed only at the beginning and at the end of the study. Daily self-weighing was found to result in poorer mood and lower levels of self-esteem; something that may lead people to avoid monitoring their weight (i.e., lead to ‘the ostrich problem’, Webb, Chang, & Benn, Citation2013). In contrast, however, other research has reported no negative psychological outcomes following self-weighing. For example, Wing et al. (Citation2007) randomly assigned participants who had already successfully lost weight to either a face-to-face or online intervention designed to help them to maintain their weight loss, or to a control condition. The intervention encouraged participants to weigh themselves daily. Both the intervention groups reported more frequent self-weighing than the control group, but this was not accompanied by any adverse psychological effects. Instead, self-weighing was associated with increased dietary restraint and decreases in disinhibition (loss of control over eating), depressive symptoms and binge eating episodes.
Two recent reviews have sought to characterise the relation between self-weighing and psychological outcomes (Pacanowski, Linde, & Neumark-Sztainer, Citation2015; Zheng et al., Citation2015). Both reviews agreed that self-weighing is largely a useful tool for losing weight; however, their conclusions regarding the psychological impact of self-weighing differed. Zheng and colleagues reviewed five longitudinal studies and concluded that there was no evidence to suggest that self-weighing was associated with negative psychological outcomes. Rather, self-weighing was associated with an increase in dietary restraint and body satisfaction, a decrease in disinhibition, depressive symptoms and weight and shape concerns. In apparent contrast, Pacanowski and colleagues’ review of 20 studies concluded that self-weighing was associated with negative psychological outcomes, but that this relationship may be moderated by individual differences (e.g., those who are more sensitive to their body image – such as females or teenagers – may be more affected by self-weighing). Unfortunately, neither review quantified the size of the relationship between self-weighing and psychological outcomes. Given the mixed findings in the literature to date, it may be that the effects are relatively small and therefore could be interpreted as evidence that self-weighing does not have a substantive effect on psychological outcomes.Footnote1 Meta-analysis is therefore needed to identify and quantify the direction and size of the relationship between self-weighing and psychological outcomes. It would also seem to be important to identify factors that may explain the (likely) variation in findings across the extant studies.
What factors influence the psychological impact of self-weighing?
A number of factors may influence the psychological impact of self-weighing. Given that self-weighing likely draws attention to the body (Mercurio & Rima, Citation2011) and can highlight discrepancies between current and desired shape or weight (Dionne & Yeudall, Citation2005), self-weighing may result in worse psychological outcomes among those who are sensitive or concerned about their bodies. It is likely that this includes teenagers and young adults (Friend, Bauer, Madden, & Neumark-Sztainer, Citation2012; Pacanowski, Loth, Hannan, Linde, & Neumark-Sztainer, Citation2015; Quick et al., Citation2012, Citation2013) and females (Geier & Rozin, Citation2008; Pingitore, Spring, & Garfieldt, Citation1997). It will therefore be important to examine whether and how the nature of the sample influences the association between self-weighing and psychological outcomes.
The duration with which participants engage in self-weighing may also influence its psychological impact. For example, although both Ogden and Whyman (Citation1997) and Wing et al.(Citation2007) asked participants to weigh themselves daily, the former asked participants to weigh themselves for two weeks (and found negative psychological outcomes), whereas the latter had participants weigh themselves for 18 months (and found positive psychological outcomes). One reason why self-weighing may have a negative effect on psychological outcomes is that it draws attention to the discrepancy between desired and current weight (Dionne & Yeudall, Citation2005). However, the psychological impact of such information may diminish over time as it becomes less surprising (see Webb, Benn, & Chang, Citation2014, for a similar argument with respect to self-monitoring of household energy consumption). Therefore, we might expect to observe a smaller relation between self-weighing and psychological outcomes in studies where participants self-weigh for a long relative to a short period of time.
The extent to which self-weighing is accompanied by weight loss is also likely to influence the psychological impact of this behaviour. Evidence suggests that improvements in body image during weight loss interventions are closely related to changes in weight (Lasikiewicz, Myrissa, Hoyland, & Lawton, Citation2014). One explanation for this finding is that self-weighing draws attention to weight loss (or lack thereof). The extent of weight loss is, therefore, likely to moderate the effect of self-weighing on psychological outcomes, such that more positive effects of self-weighing could occur when self-weighing is accompanied by weight loss.
A recent meta-analysis of interventions designed to promote progress monitoring found that the effects of monitoring on goal attainment were larger when monitoring took place publicly (e.g., participants reported the amount of physical activity that they do in front of other people) or when monitoring was done in private, but the outcomes were reported to someone afterwards (e.g., participants recorded their level of physical activity in private, but had to subsequently report this to a researcher) than when monitoring took place in private and was not reported (Harkin et al., Citation2016). Monitoring in public may also have a different psychological impact to monitoring in private, with empirical research suggesting that public weighing can, in some cases, be uncomfortable (Geier & Rozin, Citation2008). It would therefore seem important to examine whether the psychological impact of self-weighing is influenced by (i) the context in which self-weighing takes place (e.g., in public or private) and (ii) how the outcomes of self-weighing are reported.
Finally, obesity and being overweight have been associated with poor psychological states, including relatively high levels of depression (Luppino et al., Citation2010), anxiety (Gariepy, Nitka, & Schmitz, Citation2010), poor body image (Schwartz & Brownell, Citation2004) and disordered eating (Stunkard & Allison, Citation2003). As such, it is possible that being obese or overweight may amplify the psychological impact of self-weighing, as self-weighing may highlight the degree to which the current state is different from a desired, or a healthy state. It would therefore seem important to compare the psychological impact of self-weighing among people who are obese or overweight with those who are of normal weight.
The present research
The present meta-analysis sought to quantify the effect of self-weighing on four psychological outcomes: (i) affect (e.g., levels of depression and anxiety), (ii) psychological functioning (e.g., levels of stress and self-esteem), (iii) body-related attitudes (e.g., body image and body dissatisfaction) and (iv) disordered eating (e.g., binge eating, restraint). These outcomes are similar to those considered by Pacanowski, Linde et al. (Citation2015), but we considered self-esteem and stress separately from body-related attitudes, as it has been shown that these are not always related (e.g., Furnham, Badmin, & Sneade, Citation2002; Quick et al., Citation2012; Silberstein, Striegel-Moore, Timko, & Rodin, Citation1988). Based on the literature, we hypothesized that self-weighing would not be associated with negative psychological outcomes. However, we expected to observe an association in particular circumstances and among particular samples. For example, we expected that self-weighing would be associated with (negative) psychological outcomes (i) among younger samples, females and obese and over-weight individuals, (ii) when people are required to weigh themselves for short, rather than long, periods of time and (iii) when self-weighing is not accompanied by weight loss. In addition, we expected that weighing in public, or being asked to report weight to someone else, would be associated with larger effects on psychological outcomes than self-weighing in private.
Studies investigating the effects of self-weighing on psychological outcomes typically involve either randomised controlled trials (RCTs), in which participants are typically randomly allocated to receive instructions to self-weigh or not (e.g., Steinberg et al., Citation2014) or correlational designs that measure the frequency of self-weighing (e.g., Klos, Esser, & Kessler, Citation2012). While it is well established that RCTs are the gold standard to be used in meta-analytic reviews (Barton, Citation2000) and can provide a causal test of the impact of self-weighing on psychological outcomes, focusing only on RCTs limits the evidence base and assumes (rather than tests the idea) that study design will influence effect sizes (something that is not necessarily the case, see Benson & Hartz, Citation2000). As such, the current review adopts an inclusive approach, but we compare the effects between the two types of studies. We also sought to compare effects between published and unpublished reports and between studies with relatively small and relatively large samples.
Methods
Selection of studies
The sample of studies was generated via a computerized search of Web of ScienceFootnote2 and UMI Dissertation Abstracts in September 2014. Two search filters were used: one for identifying studies involving self-weighing (self-weigh* OR regular weigh*) and the other for psychological outcomes (body* OR affect* OR emotion* OR mood* OR motiv* OR depress* OR anxi*).Footnote3 To be included in the review, studies had to include at least one term from each of the filters in the title, abstract or keywords and include a measure of the frequency of self-weighing, as well as a measure of psychological outcomes. Psychological outcomes were defined as measures of well-being, mood, affect or emotion, psychological functioning such as social functioning or self-esteem, measures of body- and/or weight-related attitudes, beliefs or perceptions, or measures of disordered eating. Studies of clinical populations such as those who were diagnosed with eating disorders were excluded.Footnote4
shows the flow of information through the review. Of the 15,102 articles initially identified, 4972 duplicates were removed. We then screened the remaining 10,130 articles, of which 103 were identified as potentially eligible for inclusion. The majority of the other articles were rejected because they failed to include relevant measures (e.g., they focused on self-monitoring of diet, rather than weight). The remaining 103 articles were then evaluated in detail. At this stage, articles were rejected if they did not report the frequency of self-weighing (e.g., Ogden & Evans, Citation1996), did not include any psychological measures (e.g., VanWormer, Linde, Harnack, Stovitz, & Jeffery, Citation2012) or if psychological outcomes were only measured prior to self-weighing (e.g., Strimas & Dionne, Citation2010).
Figure 1. Flow of information through the review.
We then examined the 447 articles that were cited by each of the 24 articles identified by the database search that met our inclusion criteria (i.e., we used an ancestry approach; Johnson, Citation1993). Of these, 172 papers had already been identified by the database search (i.e., were duplicates) and so were removed. We also identified articles that cited each of those that met our inclusion criteria. This resulted in an additional 251 articles of which 96 duplicates were removed and 5 were deemed suitable for inclusion in the review.
Of the 29 articles that were initially identified for inclusion, 3 were later removed (Kong et al., Citation2012; Neumark-Sztainer, van der Berg et al., Citation2006; Welsh, Sherwood, Van Wormer, Hotop, & Jeffery, Citation2008) as they were found to use the same data as articles already included in the review (Kong et al., Citation2012; Quick et al., Citation2012; Welsh, Sherwood, Van Wormer, Hotop, & Jeffery, Citation2009). One study was removed as it provided insufficient data for us to be able to calculate an effect size (Van Wormer, Martinez, Cosentino, & Pronk, Citation2010) and a further two articles (Boutelle, Libbey, Neumark-Sztainer, & Story, Citation2009; McGuire, Wing, Klem, Lang, & Hill, Citation1999) were removed as they compared a group of overweight individuals who lost weight to those who did not lose weight. As such, the groups differed on a dimension that we hypothesized might influence the effect of self-weighing on psychological outcomes (namely, weight loss), and so could not provide a clear test of the relation between self-weighing and psychological outcomes. Thus, the present review is based on the data from 23 articles (a list of citations is provided in Appendix A in the Supplemental material). In an effort to identify unpublished studies, at least one author from each of these 23 publications was contacted and asked if they had any unpublished material that could be suitable for this meta-analysis. Most authors replied, but none offered additional data.
Where articles reported the relationship between self-weighing and psychological outcomes separately for different groups of participants (e.g., Quick et al., Citation2012, reported effects separately for males and females), the subgroups were treated as separate studies to enable us to examine factors that influenced the reported relations (e.g., gender). As a result, 29 independent tests of the relationship between self-weighing and psychological outcomes, involving 10,775 participants, were included in the meta-analysis. presents the number of participants and effect size in each test.
Table 1. Effect sizes (r) for the relationship between self-weighing and psychological outcomes for studies included in the meta-analysis.
Data extraction
Computing effect sizes
Both studies with correlational designs (where the frequency of self-weighing was measured) and RCTs (where the frequency of self-weighing was manipulated) were included in the review. In each case, we used effect size r to represent the relationship between self-weighing and the different psychological outcomes. For correlational studies, we computed an effect size representing the strength of the relationship between measures of the frequency of self-weighing and psychological outcomes. For the RCTs, we compared psychological outcomes between conditions that differed in the frequency of self-weighing (typically using effect size d, which was then converted to r). If studies did not report the relevant effect size, then it was derived from other statistics using conversion formulas (Johnson, Citation1993). When effect sizes could not be computed on the basis of information in the report, the authors were contacted to request this information.Footnote5 Where psychological outcomes were measured at multiple points, we used the measure that most closely followed self-weighing. In addition, the effect of self-weighing on weight loss was recorded where available. Positive effect sizes indicate that self-weighing had a positive effect on psychological outcomes (i.e., reduced depression or anxiety, increased self-esteem, improved body satisfaction or reduced disordered eating). When studies compared more than two groups (e.g., Linde et al., Citation2007, compared participants who weigh daily, weekly, monthly and less than monthly), we compared the two groups of participants that differed the most in the frequency of self-weighing (i.e., those reporting daily self-weighing versus those reporting less than monthly self-weighing). One study (Gow, Trace, & Mazzeo, Citation2010) used two different interventions (self-weighing alone, or self-weighing with internet support) and two corresponding control conditions. In this case, an effect size was calculated comparing each intervention separately with respect to the corresponding control condition.
Coding of study characteristics
For all studies, we recorded sample characteristics, including age, gender (operationalized as the percentage of females in the study), weight status (overweight/obese or normal weight) and, where relevant, the extent of weight loss during the study period, and the time period during which participants were asked to self-weigh. We also identified the study design (RCT or correlational) and recorded whether self-weighing took place in a public or private context, whether the weight was reported, and whether the effect size came from a published or an unpublished report. The characteristics of the primary studies were coded by the first and third authors. There was a high level of agreement (for categorical characteristics, median kappa = 0.97, range = 0.89 to 1.00; for continuous characteristics, median r = .96, range = .92 to 1.00) and disagreements were resolved jointly by discussion.
Meta-analytic strategy
Effect sizes were computed using SPSS version 20 and the macros developed by Wilson (Citation2005). This provided effect sizes weighted by sample size, with a 95% confidence interval, and an estimate of heterogeneity. A random effects model was employed to account for the idea that differences in effects between studies likely includes random error from unidentifiable sources (Lipsey & Wilson, Citation2001). Following Cohen's (Citation1992) recommendations, r = .10 was taken to represent a ‘small’ effect size, r = .30 a ‘medium’ effect size and r = .50 a ‘large’ effect size.
The moderating effect of continuous variables (e.g., age of participants, the extent of weight loss) was tested using a series of weighted linear regression models regressing the effect size for the association between self-weighing and the psychological outcome on the moderator, weighted by the inverse variance of each effect size (Hedges & Olkin, Citation1985), which was estimated following established procedures (Steel & Kammeyer-Mueller, Citation2002). To test the moderating effects of categorical variables (e.g., whether weight status had an effect on the psychological outcomes as a result of self-weighing), the studies were split based on levels of the categorical moderator and a separate meta-analysis was conducted on each subgroup. We did not compare subgroups that were represented by only a single study, but report the effect sizes for information.
Results
Relationship between self-weighing and psychological outcomes
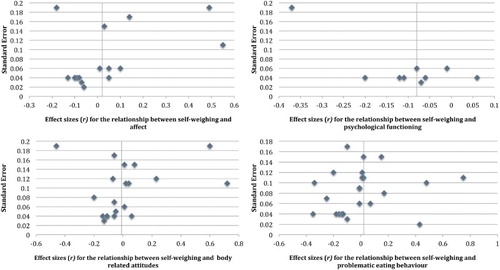
provides a visual representation of the relationship between self-weighing and psychological outcomes as derived from the primary studies. There was no association between self-weighing and affect (r+ = .02; k = 15, N = 7352, 95% CI: −0.06 to 0.06), body-related attitudes (r+ = −.01, k = 20, N = 5879, 95% CI: −0.07 to 0.06) or disordered eating (r+ = .02, k = 23, N = 8650, 95% CI: −0.12 to 0.13). There was, however, a small-sized, but statistically significant, negative association between self-weighing and psychological functioning (r+ = −.08, k = 9, N = 4849, 95% CI: −0.14 to −0.03), such that self-weighing was associated with poorer psychological functioning (i.e., lower levels of self-esteem and/or higher levels of stress).
Figure 2. Funnel plots showing the effect sizes (r) for the relationship between self-weighing and psychological outcomes.
Examination of publication bias
Despite our efforts to identify the unpublished data, only one unpublished study was identified as suitable for inclusion in the review (Katterman, Citation2010), and hence, it was not possible to directly compare effect sizes between published and unpublished reports. We therefore conducted a series of Egger's regressions (Egger, Davey-Smith, Schneider, & Minder, Citation1997) to examine potential asymmetry in the effect sizes derived from the primary studies and, thus, the possibility that additional (likely, unpublished) studies may exist that were not identified by our searches. These analyses suggested no bias in the estimate of the relationship between self-weighing and psychological functioning (p = .64), body-related attitudes (p = .06) or disordered eating (p = .65). There did, however, appear to be a significant bias in the estimate of the relationship between self-weighing and affect (p = .03). Using STATA version 11 (StataCorp, Citation2009) to conduct a trim and fill analysis (Duval & Tweedie, Citation2000) in order to estimate the missing effect sizes. This analysis inputted four additional studies, but did not substantially change the sample-weighted effect size, which remained non-significant (r+ = −.05, k = 19, 95% CI: −0.12 to 0.01).
Examination of small study bias
Estimates of population effect sizes in meta-analysis can be adversely influenced by effect sizes from studies with relatively small samples that are relatively underpowered (Kraemer, Gardner, Brooks, & Yesavage, Citation1998). We therefore sought to compare effect sizes between studies with relatively small versus relatively large samples as suggested by Coyne, Thombs, and Hagedoorn (Citation2010). We compared effect sizes between studies with relatively small samples and relatively large samples separately for correlational and experimental studies because correlational studies typically had larger samples and tended to report negative effects of self-weighing on psychological outcomes (see the section on study design below). Thus, comparison between studies with relatively small versus relatively large samples would likely be confounded by the design of the study. Therefore, the median sample size was calculated separately for experimental and correlational studies for each psychological outcome. Studies with a sample size smaller than the median were classified as having a relatively small sample; studies with sample sizes larger than the median were classified as having relatively large samples. The results suggested that studies with relatively small samples did not significantly bias the estimates of the relationship between self-weighing and any of the psychological outcomes (see ).
Table 2. The relationship between self-weighing and psychological outcomes as a function of sample size and study design.
Moderators of the relationship between self-weighing and psychological outcomes
Effect sizes derived from the primary studies were relatively heterogeneous (for the relationship between self-weighing and affect: Q(14) = 65.21, p < .001, psychological functioning: Q(8) = 25.85, p < .001, body-related attitudes: Q(19) = 100.89, p < .001, disordered eating: Q(22) = 587.44, p < .001). We therefore examined factors that might explain the variation in effect sizes.
Age
The average age of participants in the primary studies was 28.98 (SD = 14.04, range 14–52). Age did not significantly influence the relationship between self-weighing and affect, psychological functioning or body-related attitudes. However, age was significantly associated with the relationship between self-weighing and disordered eating, with the association between self-weighing and disordered eating being more negative among younger samples (see ).
Table 3. Continuous moderators of the relationship between self-weighing and psychological outcomes.
Gender
On average, the samples in the primary studies contained 69.37% female participants (SD = 35.15, range 0%–100%). The percentage of females in the sample was not significantly associated with the relationship between self-weighing and affect, psychological functioning, body-related attitudes or disordered eating (see ).
Weight status
Participants’ weight status (i.e., obese/overweight or normal weight) did not moderate the relationship between self-weighing and affect, psychological functioning or disordered eating; although it should be noted that there were relatively few studies of the effects of self-weighing among normal weight participants (see ). Participants’ weight status did, however, moderate the relationship between self-weighing and body-related attitudes, such that self-weighing had a significant, positive relationship with body-related attitudes among studies that recruited obese and overweight participants, but a non-significant relationship among studies that recruited normal weight participants.
Table 4. Categorical moderators of the relationship between self-weighing and psychological outcomes.
Weight-loss
Self-weighing had a medium-sized effect on weight loss among the 10 studies that reported this effect (d+ = 0.68, 95% CI: 0.20 to 1.16, p < 0.01). The extent of weight loss did not significantly influence the relationship between self-weighing and psychological functioning, body-related attitudes or disordered eating. However, weight loss did moderate the association between self-weighing and affect, such that self-weighing was more likely to be associated with positive affect and/or less likely to be associated with negative affect in studies where participants lost more weight (see ).
Duration of self-weighing
Twelve studies provided information about the number of days over which participants self-weighed. The mean duration was157 days (SD = 119.13, range = 14 to 365). The duration over which participants self-weighed had no impact on the relationship between self-weighing and affect, psychological functioning or disordered eating. However, duration significantly moderated the relationship between self-weighing and body-related attitudes, such that self-weighing over longer (relative to shorter) durations was associated with more positive and/or less negative body-related attitudes (see ).
Study design
Study design moderated the effect of self-weighing on three of the four psychological outcomes – RCTs typically reported a positive relationship between self-weighing and affect and body-related attitudes, while correlational studies typically reported a negative relationship between self-weighing and affect and psychological functioning (see ). One possible explanation for the difference between RCTs and correlational studies is that RCTs often examine the effect of self-weighing as part of a larger intervention designed to promote weight loss, whereas correlational studies typically examine the effects of (unprompted) self-weighing. It may therefore be that additional intervention components (e.g., social support) reduce any negative effect of self-weighing on psychological outcomes in studies with an RCT design.
In order to explore this idea, we identified whether self-weighing took place as part of an intervention and compared the effect of so doing on psychological outcomes to studies that did not include an intervention. Whether the study involved an intervention moderated the relationship between self-weighing and affect, body related attitudes and disordered eating (see ). Self-weighing tended to have a more positive association with affect, body-related attitudes and reduced disordered eating in studies where self-weighing occurred as part of an intervention than in studies that did not involve an intervention. The presence of an intervention did not moderate the effect of self-weighing on psychological functioning.Footnote6
Public versus private weighing
Eleven studies reported the psychological outcomes associated with asking participants to weigh themselves privately, but unfortunately none reported the effects of self-weighing in public and so the effects of public versus private self-weighing on psychological outcomes could not be compared (see ).
Reported versus not-reported weighing
Only one study did not require participants to report their weight in some form or another (either through a website, or directly to the researcher or a health professional). Therefore, we were unable to reliably compare the effect of reporting versus not-reporting weight (see ).
Discussion
The present review used meta-analysis to investigate the relationship between self-weighing and psychological outcomes including affect, psychological functioning, body-related attitudes and disordered eating. For the most part, self-weighing was not associated with adverse psychological outcomes. There was, however, a small-sized, negative association between self-weighing and psychological functioning, suggesting that self-weighing can reduce self-esteem and/or increase stress. Correction for publication or small study bias did not alter the findings. These findings support the conclusions of a recent narrative review of five studies (Zheng et al., Citation2015) and, importantly, quantify the magnitude of the relationships. For three of the four psychological outcomes (affect, body-related attitudes and disordered eating) the effect sizes were virtually zero (r+ = −.01), and for the fourth outcome (psychological functioning) the effect size was small (r+ = −.08). These findings should not, however, be taken as evidence that self-weighing is psychologically neutral. We found a small-sized, negative relationship between self-weighing and psychological functioning and a number of studies have found negative effects of self-weighing on this and other psychological outcomes (e.g., Mercurio & Rima, Citation2011; Neumark-Sztainer, van der Berg et al., Citation2006; Ogden & Whyman, Citation1997; Quick et al., Citation2013). In addition, a number of factors moderated the psychological impact of self-weighing. Therefore, although self-weighing is, for the most part, not psychologically aversive, it is possible that in some circumstances and among some individuals self-weighing can be problematic – something that we expand on below.
What factors influence the psychological impact of self-weighing?
We examined the effect of several moderators on the relationship between self-weighing and psychological outcomes. While age had no impact on the relationship between self-weighing and body-related attitudes, psychological functioning or affect, studies that involved younger participants reported a stronger association between self-weighing and disordered eating. This is consistent with the findings of several studies focusing on the effects of self-weighing among adolescents (e.g., Friend et al., Citation2012; Quick et al., Citation2012, Citation2013), and supports the idea that self-weighing should be used with care (e.g., accompanied by psychological and/or social support) or avoided altogether within this age group (Neumark-Sztainer, van der Berg et al., Citation2006). The percentage of females in the study did not influence the relationship between self-weighing and any of the psychological outcomes that we examined. This finding is consistent with studies showing that the psychological outcomes of self-weighing (or lack thereof) apply to both males and females (Neumark-Sztainer, van der Berg et al., Citation2006; Quick et al., Citation2012, Citation2013).
Although we hypothesised that self-weighing would have a more negative psychological impact among obese and overweight individuals (on the basis that it likely draws attention to discrepancies between desired and actual weight), weight status did not influence the impact of self-weighing on affect, psychological functioning or disordered eating. Furthermore, self-weighing was actually associated with more positive body-related attitudes among obese and overweight individuals. Given that self-weighing has been shown to be an effective method to encourage weight-loss in obese people (Van Wormer et al., Citation2009), it is encouraging that self-weighing in this population does not have negative psychological outcomes.
We found that weight loss influenced the relationship between self-weighing and affect (but not other psychological outcomes), such that self-weighing was more likely to be associated with positive affect (or less likely to be associated with negative affect) in studies where participants lost more weight, relative to studies in which they lost less weight. Weight loss has previously been shown to reduce depressive symptoms (Dixon, Dixon, & O'Brien, Citation2003). It therefore seems likely that self-weighing draws attention to weight loss, the knowledge of which then serves to improve affect.
The length of time that participants engaged in self-weighing had no impact on its relationship with affect, psychological functioning or disordered eating. However, it did influence the association between self-weighing and body-related attitudes, such that the longer the participants engaged in self-weighing, the more positive was the association between self-weighing and body-related attitudes. One possible explanation for this finding is that there is a bidirectional relationship between self-weighing and body-related attitudes such that improvements in body-related attitudes motivate continued self-weighing. In support of this idea, evidence suggests that, although body dissatisfaction can motivate the desire to lose weight (Heinberg, Thompson, & Matzon, Citation2001), continued low levels of body satisfaction can lead people to drop out of weight loss programs (Carels, Cacciapaglia, Douglass, Rydin, & O'Brien, Citation2003; Kiernan, King, Kraemer, Stefanick, & Killen, Citation1998).
Study design moderated the effect of self-weighing on affect, body-related attitudes and disordered eating. While RCTs tended to report a positive relationship between self-weighing and psychological outcomes, correlational studies tended to report more negative relationships. There are a number of possible explanations for this effect. It may be that taking part in an intervention increases participants’ motivation to lose weight, or that simply being pro-active and taking steps to control weight improves psychological outcomes. Alternatively (or in addition) RCTs may provide a more valid test of the effect of self-weighing on psychological outcomes because self-weighing is typically manipulated (e.g., participants in the intervention condition are asked to weigh themselves, whereas participants in the control condition are not) rather than measured as in correlational studies. However, we suspect that the difference might be explained by the inclusion of additional intervention components in RCTs. In support of this idea, we found that self-weighing that occurred as part of an intervention was more likely to be associated with positive psychological outcomes than unprompted self-weighing that occurred naturally. This relationship held even when we examined studies with the same design (namely, those with correlational designs) that included versus did not include an intervention. As such, future research might usefully investigate which intervention components (e.g., motivation, social support, strategies to promote self-acceptance or self-efficacy) influence the relationship between self-weighing and psychological outcomes.
Limitations
The current meta-analysis identified several shortcomings in the available data. For example, it was not possible to examine the effect of self-weighing in public versus in private, or when weight was reported versus not reported, because almost all studies asked participants to weigh themselves privately and to report their weight. Given that public self-weighing is a key component of commercially available weight loss programs (e.g., Slimmer's World, Weight Watchers) and that previous reviews suggest larger effects (on goal attainment) of public (relative to private) self-monitoring (Harkin et al., Citation2015), studies of the psychological impact of so doing would seem to be a priority for future research.
Conclusion
The present research used meta-analysis to quantify the relationship between self-weighing and four different psychological outcomes. For the most part, self-weighing was not associated with adverse psychological outcomes, but there was a small-sized, negative association between self-weighing and psychological functioning. The findings also support previous reviews in showing that self-weighing has a different effect on psychological outcomes among some individuals and in some situations. In particular, our findings suggest that self-weighing is more likely to be associated with negative psychological outcomes among younger samples, normal weight participants, those who have lost less weight, are self-weighing for a short, relative to a long, period of time and when self-weighing is not delivered as part of an intervention. Future research might usefully explore the mechanisms underlying these moderating effects, as well as addressing gaps in the literature – for example, the psychological impact of self-weighing in public contexts.
References_supplemental material
Download PDF (215 KB)Supplemental material
Download (8.5 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Notes
1. Note that statistically small effects may not necessarily be trivial, given that self-weighing forms a key part of many interventions designed to promote weight loss, commercial weight loss programs (e.g., CitationWeight Watchers UK) and day-to-day life (e.g., Mercurio & Rima, Citation2011; Quick et al., Citation2013) (for a similar argument with respect to ‘small’ effects of smoking cessation treatments, see West, Citation2007).
2. Databases include the Science Citation Index Expanded (1900–present), Social Sciences Citation Index (1956–present), Arts & Humanities Citation Index (1975–present), Conference Proceedings Citation Index – for Science and for Social Science & Humanities (1990–present), Book Citation Index – for Science and for Social Science & Humanities (2005–present), Current Chemical Reactions (1985–present), Index Chemicus (1993–present), BIOSIS Citation Index (1926–present), BIOSIS Previews (1969–present), Current Contents Connect (1998–present), Data Citation Index (1900–present), Derwent Innovations Index (1963–present), MEDLINE (1950–present), SciELO Citation Index (1997–present) and the Zoological Record (1864–present).
3. In order to examine whether our search terms were sufficient to identify all articles investigating the relationship between self-weighing and psychological outcomes, we tested whether the inclusion of additional search terms would have identified any additional articles. To do so, we entered the abstracts of the articles that met our inclusion criteria into Wordle (http://www.wordle.net) to identify the most commonly used words. This prompted us to try an additional term in the first filter: frequent weigh*, and an additional term in the second filter: satisf*. Searching the databases again using these new filters resulted in an additional 12,509 articles, from which 2648 duplicates were removed. We screened 1000 articles from the remaining 9861 articles, but as none of these met our inclusion criteria, our original search terms were deemed to have been sufficient for identifying all studies investigating the relationship between self-weighing and psychological outcomes.
4. This decision did not have a substantive bearing on the evidence base available for the review as only one study with a clinical sample met the other inclusion criteria (Shafran, Fairburn, Robinson, & Lask, Citation2004).
5. Three authors were contacted, of whom all replied, but only two could address our request.
6. Because the presence of an intervention was confounded with study design (i.e., RCTs were more likely to include an intervention than correlational studies), we also compared the effects of self-weighing between correlational studies that included versus did not include an intervention. Although relatively few correlational studies involved an intervention, the magnitude of the effects reported by these studies are consistent with the idea that self-weighing that occurs as part of an intervention tends to be associated with more positive psychological outcomes than self-weighing outside an intervention. Specifically, correlational studies that included an intervention tended to report a positive effect on body-related attitudes (r+ = .08, k = 1, 95% CI: -0.23 to 0.35) affect (r+ = .10, k = 1, 95% CI: -0.04 to 0.24) and disordered eating (r+ = .07, k = 4, 95% CI: -0.23 to 0.36). No correlational studies examined the effect of self-weighing as part of an intervention on psychological functioning. In contrast, correlational studies with no intervention tended to report negative effects of self-weighing on psychological outcomes: Affect: (r+ = -.06, k = 8, 95% CI: -0.09 to -0.04), psychological functioning: (r+ = -.08, k = 7, 95% CI: -0.11 to -0.05), body-related attitudes (r+ = -.07, k = 12, 95% CI: -0.11 to -0.02) and disordered eating (r+ = -.12, k = 12, 95% CI: -0.28 to 0.05).
References
- Barton, S. (2000). Which clinical studies provide the best evidence? The best RCT still trumps the best observational study. British Medical Journal, 321(7256), 255–256. doi: 10.1136/bmj.321.7256.255
- Benson, K., & Hartz, A. J. (2000). A comparison of observational studies and randomized, controlled trials. New England Journal of Medicine, 342(25), 1878–1886. doi:10.1056/NEJM200006223422506
- Boutelle, K. N., Libbey, H., Neumark-Sztainer, D., & Story, M. (2009). Weight control strategies of overweight adolescents who successfully lost weight. Journal of the American Dietetic Association, 109(12), 2029–2035. doi:10.1016/j.jada.2009.09.012
- Carels, R. A., Cacciapaglia, H. M., Douglass, O. M., Rydin, S., & O'Brien, W. H. (2003). The early identification of poor treatment outcome in a women's weight loss program. Eating Behaviour, 4(3), 265–282. doi:10.1016/S14710153(03)00029-1
- Carver, C. S., & Scheier, M. F. (1982). Control theory: A useful conceptual framework for personality, social, clinical and health psychology. Psychological Bulletin, 92(1), 111–135. doi:10.1037//0033-2909.92.1.111
- Chambers, J. A., & Swanson, V. (2012). Stories of weight management: Factors associated with successful and unsuccessful weight maintenance. British Journal of Health Psychology, 17(2), 223–243. doi:10.1111/j.2044-8287.2011.02030.x
- Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159. doi: 10.1037/0033-2909.112.1.155
- Coyne, J. C., Thombs, B. D., & Hagedoorn, M. (2010). Ain't necessarily so: Review and critique of recent meta-analyses of behavioral medicine interventions in health psychology. Health Psychology, 29(2), 107. doi:10.1037/a0017633
- Dionne, M. M., & Yeudall, F. (2005). Monitoring of weight in weight loss programs: A double-edged sword? Journal of Nutrition Education and Behavior, 37(6), 315–318. doi:10.1016/S1499-4046(06)60162-0
- Dixon, J. B., Dixon, M. E., & O'Brien, P. E. (2003). Depression in association with severe obesity: Changes with weight loss. Archives of Internal Medicine, 163(17), 2058–2065. doi:10.1001/archinte.163.17.2058
- Duval, S., & Tweedie, R. (2000). A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association, 95, 89–99.
- Egger, M., Davey-Smith, G., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple graphical test. British Medical Journal, 315, 629–634. doi: 10.1136/bmj.315.7109.629
- Friend, S., Bauer, K. W., Madden, T. C., & Neumark-Sztainer, D. (2012). Self-weighing among adolescents: Associations with body mass index, body satisfaction, weight control behaviors, and binge eating. Journal of the Academy of Nutrition and Dietetics, 112(1), 99–103. doi:10.1016/j.jada.2011.08.036
- Furnham, A., Badmin, N., & Sneade, I. (2002). Body image dissatisfaction: Gender differences in eating attitudes, self-esteem, and reasons for exercise. The Journal of Psychology, 136(6), 581–596. doi:10.1080/00223980209604820
- Gariepy, G., Nitka, D., & Schmitz, N. (2010). The association between obesity and anxiety disorders in the population: A systematic review and meta-analysis. International Journal of Obesity, 34(3), 407–419. doi:10.1038/ijo.2009.252
- Geier, A. B., & Rozin, P. (2008). Weighing discomfort in college age American females: Incidence and causes. Appetite, 51(1), 173–177. doi:10.1016/j.appet.2008.02.002
- Gow, R. W., Trace, S. E., & Mazzeo, S. E. (2010). Preventing weight gain in first year college students: An online intervention to prevent the “freshman fifteen”. Eating Behaviors, 11(1), 33–39. doi:10.1016/j.eatbeh.2009.08.005
- Harkin, B., Webb, T. L., Chang, B. P., Prestwich, A., Conner, M., Kellar, I., … Sheeran, P. (2016). Does monitoring goal progress promote goal attainment? A meta-analysis of the experimental evidence. Psychological Bulletin, 142(2), 198–229. doi: 10.1037/bul0000025
- Hedges, L. V., & Olkin, I. (1985). Statistical methods for meta-analysis. Orlando, FL: Academic Press.
- Heinberg, L. J., Thompson, J. K., & Matzon, J. L. (2001). Body image dissatisfaction as a motivator for healthy lifestyle change: Is some distress beneficial? In R. H. Striegel-Moore & L. Smolak (Eds.), Eating disorders: Innovative directions in research and practice (pp. 215–232). Washington, DC: American Psychological Association. doi:10.1037/10403-011
- Johnson, B. T. (1993). DSTAT. Software for the meta-analytic review of research literatures (rev. ed.). [Computer software]. Hillsdale, NJ: Erlbaum.
- Katterman, S. N. (2010). An evaluation of daily weight monitoring as a method of weight gain prevention (Doctoral dissertation). Philadelphia, PA: Drexel University.
- Kiernan, M., King, A. C., Kraemer, H. C., Stefanick, M. L., & Killen, J. D. (1998). Characteristics of successful and unsuccessful dieters: An application of signal detection methodology. Annals of Behavioral Medicine, 20(1), 1–6. doi:10.1007/BF02893802
- Klem, M. L., Wing, R. R., McGuire, M. T., Seagle, H. M., & Hill, J. O. (1997). A descriptive study of individuals successful at long-term maintenance of substantial weight loss. American Journal of Clinical Nutrition, 66(2), 239–246.
- Klos, L. A., Esser, V. E., & Kessler, M. M. (2012). To weigh or not to weigh: The relationship between self-weighing behavior and body image among adults. Body Image, 9(4), 551–554. doi:10.1016/j.bodyim.2012.07.004
- Kong, A., Beresford, S. A., Alfano, C. M., Foster-Schubert, K. E., Neuhouser, M. L., Johnson, D. B., … McTiernan, A. (2012). Self-monitoring and eating-related behaviors are associated with 12-month weight loss in postmenopausal overweight-to-obese women. Journal of the Academy of Nutrition and Dietetics, 112(9), 1428–1435. doi:10.1016/j.jand.2012.05.014
- Kong, A., Beresford, S. A., Imayama, I., Duggan, C., Alfano, C. M., Foster-Schubert, K. E., … McTiernan, A. (2012). Adoption of diet-related self-monitoring behaviors varies by race/ethnicity, education, and baseline binge eating score among overweight-to-obese postmenopausal women in a 12-month dietary weight loss intervention. Nutrition Research, 32(4), 260–265. doi:10.1016/j.nutres.2012.03.001
- Kraemer, H. C., Gardner, C., Brooks III, J. O., & Yesavage, J. A. (1998). Advantages of excluding underpowered studies in meta-analysis: Inclusionist versus exclusionist viewpoints. Psychological Methods, 3(1), 23. doi:10.1037/1082-989X.3.1.23
- Lasikiewicz, N., Myrissa, K., Hoyland, A., & Lawton, C. L. (2014). Psychological benefits of weight loss following behavioural and/or dietary weight loss interventions. A systematic research review. Appetite, 72, 123–137. doi:10.1016/j.appet.2013.09.017
- Linde, J. A., Jeffery, R. W., Finch, E. A., Simon, G. E., Ludman, E. J., Operskalski, B. H., … Rohde, P. (2007). Relation of body mass index to depression and weighing frequency in overweight women. Preventive Medicine, 45(1), 75–79. doi:10.1016/j.ypmed.2007.03.008
- Lipsey, M. W., & Wilson, D. B. (2001) Practical meta-analysis. Thousand Oaks, CA: Sage.
- Luppino, F. S., de Wit, L. M., Bouvy, P. F., Stijnen, T., Cuijpers, P., Penninx, B. W., & Zitman, F. G. (2010). Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Archives of General Psychiatry, 67(3), 220–229. doi:10.1001/archgenpsychiatry.2010.2
- McGuire, M. T., Wing, R. R., Klem, M. L., & Hill, J. O. (1999). Behavioral strategies of individuals who have maintained long-term weight losses. Obesity Research, 7(4), 334–341. doi: 10.1002/j.1550-8528.1999.tb00416.x
- McGuire, M. T., Wing, R. R., Klem, M. L., Lang, W., & Hill, J. O. (1999). What predicts weight regain in a group of successful weight losers? Journal of Consulting and Clinical Psychology, 67(2), 177–185. doi:10.1037//0022-006x.67.2.177
- Mercurio, A., & Rima, B. (2011). Watching my weight: Self-weighing, body surveillance, and body dissatisfaction. Sex Roles, 65(1–2), 47–55. doi:10.1007/s11199-011-9980-x
- Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychology, 28(6), 690–701. doi:10.1037/a0016136
- Neumark-Sztainer, D., van den Berg, P., Hannan, P. J., & Story, M. (2006). Self-weighing in adolescents: Helpful or harmful? Longitudinal associations with body weight changes and disordered eating. Journal of Adolescent Health, 39(6), 811–818. doi:10.1016/j.jadohealth.2006.07.002
- Neumark-Sztainer, D., Paxton, S. J., Hannan, P. J., Haines, J., & Story, M. (2006). Does body satisfaction matter? Five-year longitudinal associations between body satisfaction and health behaviors in adolescent females and males. Journal of Adolescent Health, 39(2), 244–251. doi:10.1016/j.jadohealth.2005.12.001
- Ogden, J., & Evans, C. (1996). The problem with weighing: Effects on mood, self-esteem and body image. Journal of the International Association for the Study of Obesity, 20(3), 272–277.
- Ogden, J. E., & Whyman, C. (1997). The effects of repeated weighing on psychological state. European Eating Disorders Review, 5(2), 121–130. doi:10.1002/(SICI)1099-0968(199706)5:2<121::AID-ERV167>3.0.CO;2-N
- Pacanowski, C. R., Linde, J. A., & Neumark-Sztainer, D. (2015). Self-weighing: Helpful or harmful for psychological well-being? A review of the literature. Current Obesity Reports, 4(1), 65–72. doi:10.1007/s13679-015-0142-2
- Pacanowski, C. R., Loth, K. A., Hannan, P. J., Linde, J. A., & Neumark-Sztainer, D. R. (2015). Self-weighing throughout adolescence and young adulthood: Implications for well-being. Journal of Nutrition Education and Behavior, 47(6), 506–515. doi:10.1016/j.jneb.2015.08.008
- Pingitore, R., Spring, B., & Garfieldt, D. (1997). Gender differences in body satisfaction. Obesity Research, 5(5), 402–409. doi:10.1002/j.1550-8528.1997.tb00662.x
- Powers, W. T. (1973). Behavior: The control of perception. Chicago, IL: Aldine.
- Qi, B. B., & Dennis, K. E. (2000). The adoption of eating behaviors conducive to weight loss. Eating Behaviour, 1(1), 23–31. doi:10.1016/S1471-0153(00)00003-9
- Quick, V., Larson, N., Eisenberg, M. E., Hannan, P. J., Stat, M., & Neumark-Sztainer, D. (2012). Self-weighing behaviors in young adults: Tipping the scale toward unhealthy eating behaviors? Journal of Adolescent Health, 51(5), 468–474. doi:10.1016/j.jadohealth.2012.02.008
- Quick, V., Loth, K., MacLehose, R., Linde, J. A., & Neumark-Sztainer, D. (2013). Prevalence of adolescents’ self-weighing behaviors and associations with weight-related behaviors and psychological well-being. Journal of Adolescent Health, 52(6), 738–744. doi:10.1016/j.jadohealth.2012.11.016
- Schwartz, M. B., & Brownell, K. D. (2004). Obesity and body image. Body Image, 1(1), 43–56. doi:10.1016/S1740-1445(03)00007-X
- Shafran, R., Fairburn, C. G., Robinson, P., & Lask, B. (2004). Body checking and its avoidance in eating disorders. International Journal of Eating Disorders, 35(1), 93–101. doi:10.1002/eat.10228
- Silberstein, L. R., Striegel-Moore, R. H., Timko, C., & Rodin, J. (1988). Behavioral and psychological implications of body dissatisfaction: Do men and women differ? Sex Roles, 19(3), 219–232. doi:10.1007/BF00290156
- StataCorp. (2009). Stata statistical software (11th edition). Dallas, TX: College Station.
- Steel, P. D., & Kammeyer-Mueller, J. D. (2002). Comparing meta-analytic moderator estimation techniques under realistic conditions. Journal of Applied Psychology, 87(1), 96–111. doi:10.1037/0021-9010.87.1.96
- Steinberg, D. M., Tate, D. F., Bennett, G. G., Ennett, S., Samuel-Hodge, C., & Ward, D. S. (2014). Daily self-weighing and adverse psychological outcomes. A randomized controlled trial. American Journal of Preventative Medicine, 46(1), 24–29. doi:10.1016/j.amepre.2013.08.006
- Strimas, R., & Dionne, M. M. (2010). Differential effects of self-weighing in restrained and unrestrained eaters. Personality and Individual Differences, 49(8), 1011–1014. doi:10.1016/j.paid.2010.07.035
- Stunkard, A. J., & Allison, K. C. (2003). Two forms of disordered eating in obesity: Binge eating and night eating. International Journal of Obesity, 27(1), 1–12. doi:10.1038/sj.ijo.0802186
- VanWormer, J. J., Linde, J. A., Harnack, L. J., Stovitz, S. D., & Jeffery, R. W. (2012). Self-weighing frequency is associated with weight gain prevention over 2 years among working adults. International Journal of Behavioral Medicine, 19(3), 351–358. doi:10.1007/s12529-011-9178-1
- VanWormer, J. J., Martinez, A. M., Cosentino, D., & Pronk, N. P. (2010). Satisfaction with a weight loss program: What matters? American Journal of Health Promotion, 24(4), 238–245. doi:10.4278/ajhp.080613-QUAN-92
- Van Wormer, J. J., Martinez, A. M., Martinson, B. C., Crain, A. L., Benson, G. A., Cosentino, D. L., & Pronk, N. P. (2009). Self-weighing promotes weight loss for obese adults. American Journal of Preventive Medicine, 36(1), 70–73. doi:10.1016/j.amepre.2008.09.022
- Webb, T. L., Benn, Y., & Chang, B. P. (2014). Antecedents and consequences of monitoring domestic electricity consumption. Journal of Environmental Psychology, 40, 228–238. doi:10.1016/j.jenvp.2014.07.001
- Webb, T. L., Chang, B. P. I., & Benn, Y. (2013). ‘The Ostrich Problem’: Motivated avoidance or rejection of information about goal progress. Social and Personality Psychology Compass, 7, 794–807. doi:10.1111/spc3.12071
- Weight Watchers UK. Retrieved from http://www.weightwatchers.co.uk/templates/marketing/Landing_1col_nonav.aspx?skipmap=1&Pageid=1211262
- Welsh, E., Sherwood, N., Van Wormer, J., Hotop, A. M., & Jeffery, R. (2008). The effects of self-weighing on weight change and body shape satisfaction in a telephone-based weight loss trial. Obesity, 16, S213–S213.
- Welsh, E. M., Sherwood, N. E., Van Wormer, J. J., Hotop, A. M., & Jeffery, R. W. (2009). Is frequent self-weighing associated with poorer body satisfaction? Findings from a phone-based weight loss trial. Journal of Nutrition Education and Behavior, 41(6), 425–428. doi:10.1016/j.jneb.2009.04.006
- West, R. (2007). The clinical significance of ‘small’ effects of smoking cessation treatments. Addiction, 102(4), 506–509. doi:10.1111/j.1360-0443.2007.01750.x
- Wilson, D. B. (2005). SPSS macros for meta-analytic data. Retrieved January 15, 2015, from http://mason.gmu.edu/~dwilsonb/ma.html
- Wing, R. R., Gorin, A. A., Raynor, H. A., Tate, D. F., Fava, J. L., & Machan, J. (2007). “STOP regain": Are there negative effects of daily weighing? Journal of Consulting and Clinical Psychology, 75(4), 652–656. doi:10.1037/0022-006x.75.4.652
- Wing, R. R., & Phelan, S. (2005). Long-term weight loss maintenance. American Journal of Clinical Nutrition, 82(1), 222S–225S.
- Zheng, Y., Klem, M. L., Sereika, S. M., Danford, C. A., Ewing, L. J., & Burke, L. E. (2015). Self-weighing in weight management: A systematic literature review. Obesity, 23, 256–265. doi:10.1002/oby.20946