
Background
Behavior change science has developed quickly over the past years. This is partially due to high demand from practice to tackle major societal, complex problems, such as obesity, the keys to which lie in changing behaviors, for example, physical activity and dietary behaviors, via interventions ranging from structural-environmental to individual-level strategies. Advances have been made in theory and methods of intervention research including process evaluation (e.g., Moore et al., Citation2015) and taxonomies of active ingredients of interventions, e.g., behavior change techniques (BCT's) or change methods (e.g., Kok et al., Citation2016; Michie et al., Citation2013).Footnote1
One key advancement has been the taxonomy of BCTs that specifies techniques delivered in interventions. It has helped synthesize evidence (for a review, see Michie et al., Citation2018) and aided in systematic, theory-based intervention development, although important criticisms of the taxonomic approach have been raised (e.g., Ogden, Citation2016).
An acknowledged problem in primary studies and meta-analyses making conclusions based on BCT extraction from intervention protocols is the unknown fidelity (e.g., Hankonen et al., Citation2015; Ogden, Citation2016). Not all techniques are delivered as intended, and thus conclusions of the efficacy of BCTs based on a trial protocol may not be warranted. In addition to delivery, other aspects of fidelity also matter. If the participants do not understand the skills taught to them, nor enact them in their daily life, the intervention may fail to have its effects, however, high the delivery fidelity is. Whereas some BCTs can be delivered to a relatively passive recipient, some BCTs actually require active engagement by the participant, in order to have an effect: BCTs differ in terms of who is responsible for delivering them, or, in other words, the initiative required by the participants themselves. For example, in a dietary counseling intervention where the intervention provider, e.g., a health nurse administers or delivers the BCT provide ‘information on consequences of behavior’, fidelity assessment concerns with whether this BCT was delivered and received only, as it requires no enactment by the participant. In contrast, if in the same intervention, the nurse is expected to prompt the participant to self-monitor, engage in mental rehearsal of behavior’, or self-reward, these need not only to be delivered by the nurse and received by the participant, but necessarily, also enacted by the participant, in order for the BCT to have its effects.Footnote2 This has not always been explicitly considered in the development of interventions, nor assessed in trials.
BCT enactment can be defined as the performance of behavioral and cognitive tasks directed at facilitating behavior change, which resonates with the fidelity-related definition of intervention participants’ use of the learned ‘behavioral skills and cognitive strategies in relevant real-life settings’ (Bellg et al., Citation2004). The concept of BCT enactment is closely related to adoption of or engagement with the intervention. However, enactment should be better conceptualized as referring specifically to participant usage of the active ingredients, for example, BCTs of the intervention. Simply ‘presence in sessions’ or ‘time spent online in digital interventions’ is not sufficient, as this operationalization may mislead researchers from the actual point of interest.
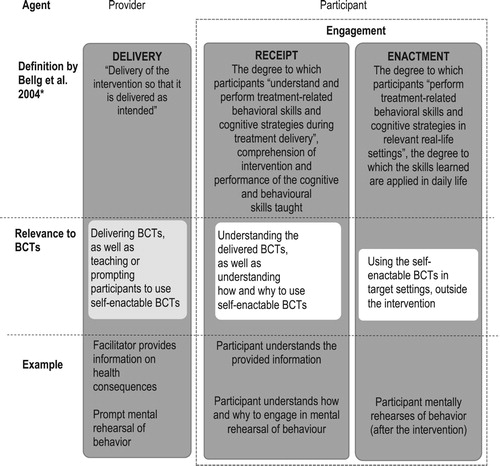
presents the concepts of three fidelity areas, delivery, receipt and enactment, as defined by the NIH Behavior Change Consortium in 2004 (Bellg et al., Citation2004). Engagement has later been used as an umbrella term to refer to participant behaviors (Walton et al., Citation2020), both to what extent a participant understands and can perform the required skills (receipt), and to what extent a participant can put the skills into practice in daily life (enactment) (Bellg et al., Citation2004). This paper focuses on the enactment of BCTs, while acknowledging the importance of receipt as a key aspect of participant engagement in interventions. An increased focus on the participants’ role in using BCTs would enable establishing the degree of participant engagement in interventions – in both protocols and intervention evaluations. The current BCT Taxonomy v1 (Michie et al., Citation2013) coding system does not prompt intervention developers or coders to differentiate the extent to which each BCT requires or enables participant involvement. However, for some BCTs, effectiveness depends on repeated, frequent enactment (e.g., self-monitoring; Harkin et al., Citation2016). More examples of how BCTs differ in terms of the degree of participant enactment assumed, will be presented below.Footnote3
Figure 1. Fidelity of delivery, receipt and enactment. NIH Behavior Change Consortium (Bellg et al., Citation2004); figure adapted from Palsola et al. (Citation2020) (*original terms of the three fidelity areas: delivery of treatment, receipt of treatment, enactment of treatment skills).
Finally, very interestingly, there has been a dearth of attempts to map the variety of ways people may attempt to influence their own motivation, or shield their motivation from external influences. Previous research on self-enactable techniques has mostly focused on the enactment of self-regulation related techniques such as goal setting and planning.
Despite recent, increasing attention paid by behavior change research to increasing rigor in both theory-based development and evaluation of interventions, there has been a lack of systematic integration of individual self-management techniques of motivation and behavior change. In this text, I will argue that behavior change science should systematically theorize and measure strategies and techniques that individuals can and do use ‘to intervene on themselves’. This is useful, because:
there is evidence that a person-centered approach may be more effective than the implicit assumption of a relatively passive participant,
we need tools and conceptual frameworks to define objectives for participant enactment in interventions,
we need tools and conceptual frameworks to assess participant enactment – an important yet under-researched aspect of fidelity in trials,
a focus on how participants manage their own motivation would encompass a larger number of BCTs than BCT Taxonomy v1 (e.g., (Michie et al., Citation2013)) and thus broaden our approach in theorizing about the key mental and other processes involved and also design better interventions to evoke such key processes, and
a clarification of self-enacted BCTs would enable research on how to enhance uptake of these BCTs.
Toward a person-centered approach to motivation and behavior change
A key consideration in behavior change is how we conceptualize the target group of our intervention attempts. Are they active participants or passive recipients of intervention efforts? An explicitly person-centered approach may be more useful and effective than the (implicit) assumption a passive intervention participant. People are active participants of health interventions, and we need to pay attention to how they receive interventions (receipt) and enact skills taught to them (Bellg et al., Citation2004; Rixon et al., Citation2016). Although few interventionists conceptualize participants as passive recipients, we sometimes inadvertently end up doing so in practice, when participants’ receipt and enactment is not given sufficient attention during intervention development, nor evaluated.
Intervention developers should be conscious of who the agent of intervention BCTs are. Interventions can assume a passive recipient or an active participant, or something along a continuum between these extremes, but while either one is not universally superior to the other, for many behaviors the participatory approach may be more efficacious or fruitful. There is evidence that interventions with more engaging components and activating approach are more effective than those assuming a more passive participant. A recent meta-analysis has indeed attempted to take into account whether BCTs such as action planning are collaborative, practitioner-led, or participant led (Knittle et al., Citation2018), but the task is difficult as the precision of previous research reports of the degree of participant autonomy varies considerably – again pointing to the need to enhance the quality of reporting.
Teaching participants about managing their motivation and behavior may prove useful. Teaching them about the underlying mechanisms of behavior change is empowering (e.g., Gillison et al., Citation2015). Actively managing one's own behavior change process rather than being passive target relying on external help can be expected to lead to longer-term, sustainable changes. Motivation and active self-management becomes less important after behaviors automatize over time, but to get there, one needs to enact habit formation techniques. This self-training of habits also requires motivation (Gardner et al., Citation2020).
It should be noted that this call for better conceptualization of self-led parts of interventions does not mean environmental interventions and those focusing on target groups’ automatic non-conscious processes would not also be needed. Compared to environmental interventions (e.g., Marteau et al., Citationn.d.), interventions requiring self-regulation tax individuals’ cognitive and self-regulatory resources. Indeed, interventions that require active agency may be less effective and equitable than population approaches that do not require individuals to use personal resources to benefit (Adams et al., Citation2016). Nevertheless, as a public health strategy, all types of interventions are needed across the spectrum from individual to societal-structural interventions, especially insofar governments are reluctant to heavily regulate environments. Indeed, we should further attempt to improve the effectiveness and usability of self-led behavior change interventions by taking better into account the participant perspective. Could we reduce the participant burden in individual-level interventions by paying more attention to the participant enactment aspects during intervention development and optimization? This is the focus on the next section.
Designing for participant enactment explicitly
In designing interventions, we need to define performance targets or objectives for participant enactment more often than currently is typically being done. The current literature falls short of specifying and distinguishing BCTs that are enactable by the individual, nor have many intervention studies explicitly designed for or assessed BCT enactment. One study has demonstrated their relevance for trial outcomes (e.g., Hankonen et al., Citation2015). Here, intervention counseling had prompted participants to make lifestyle changes. After 12 months, intervention participants were asked whether they had enacted techniques to change their physical activity and diet, for example, using reminders and prompts, self-monitored behavior, made action plans, etc. Those who reported having used all 16 techniques, had achieved significantly larger reductions in BMI over the year, compared to those having used fewer techniques. Several other studies have demonstrated that the use of self-regulation techniques plays a role in predicting intervention outcomes (e.g., planning in the HAPA model, Zhang et al., Citation2018). This growing evidence base shows the value of participant-level enactment.
There have, however, been surprisingly few attempts to conceptually map individual self-enactable behavior change strategies. The attempts have been scattered and located within specific theories (e.g., processes of change in the transtheoretical model, Prochaska & Velicer, Citation1997) and across multiple behavioral domains, challenging our ability to utilize the knowledge effectively.
OxFab taxonomy (Hartmann-Boyce et al., Citation2016) lists 117 behavioral and cognitive strategies used by individuals for weight management, in 23 domains. For example, the domain Motivation includes four strategies that ‘increase the desire to control weight’ and the domain Restraint refers to ‘conscious restriction over the amount that is eaten’ (14, p. 318). However, as a domain-specific taxonomy, its items include a host of weight management-specific strategies and thus cannot serve as a guidance to behavior change theories in general and interventions in other domains.
Explicitly defining self-enactable techniques of an intervention is a key issue in designing especially such interventions where direct contact with and support for the target group is limited, and the main responsibility of the process lies with the target individual. Interventions with small doses of personalized contact may even be cost-effective, and promising in the age of ever diminishing resources for behavioral support. Intervention developers would benefit from a more explicit focus on what the techniques they assume the target group to take up are, and how often, during and after their intervention such techniques are assumed to be used. (For an example of a table outlining optimal use of self-enactable BCTs during an intervention, used in intervention development, see supplementary figure S2 in Hankonen et al., Citationin press.) Considering this explicitly is especially relevant in the development and characterization of digital behavior change interventions that target individuals directly, without face-to-face contact or facilitator-led group activities, for interventions that rely on periods of participants leading themselves, and for post-intervention periods when contact with intervention will be lost.
Assessing participant enactment explicitly
Empirically assessing participant reception and enactment of BCTs would be critical to intervention evaluation and advancement of our understanding of the key processes in changing behavior. Delivery fidelity has been shown essential for intervention effectiveness (e.g., Durlak & DuPre, Citation2008). As many trials may not measure this sufficiently or at all, negative trial outcome evaluations may be due to insufficient implementation rather than ineffectiveness of the delivered techniques. Thus more process evaluations have been increasingly called for (e.g., Moore et al., Citation2015). A further problem is that fidelity investigations have focused mostly on delivery, with far fewer reports of participant receipt and enactment (O’Shea et al., Citation2016; Toomey et al., Citation2020; Walton et al., Citation2017). Evaluations of receipt and enactment would capture cases where despite perfect delivery, the target group may not receive the program as intended, nor enact the taught skills and behaviors as expected. An increased focus on participant enactment fidelity would help overcome this major shortcoming in current intervention evaluation literature.
This would allow interesting avenues for future research. Which BCTs require self-enactment to be effective? Does the degree of self-involvement matter? Such analyses would enable us to identify whether there are BCTs, such as ‘prompts and cues’ or ‘environmental restructuring’ the effectiveness of which may vary depending on whether they are performed by an external intervention provider or the participants themselves.
Furthermore, as mentioned above, evidence from ‘between-trials’ analyses that rely on comparisons based on BCT codings of intervention protocols (Michie et al., Citation2018) may suffer from imprecise estimates due to variable fidelity. This evidence could be corroborated by ‘within-trial’ analyses that would also investigate the link between BCT enactment and outcomes, and potential thresholds needed for optimal outcomes.
Measuring enactment of techniques may present a difficult challenge, due to biases in self-reporting, due to e.g., social desirability, but also due to difficulty in translating each practical operationalisation of a BCT in an intervention to a language that a respondent (not familiar with an abstract technique) may understand. Indeed, intervention engagement has recently increasingly been studied especially in the area of digital health interventions, in which it is easy to reliably assessing participant usage of an mHealth and eHealth/interventions. Digital platforms provide an opportunity to collect data on BCT use, along the process into maintained behavior change (Moller et al., Citation2017). A limitation to this approach is that rather than the use of a particular app, the ‘active ingredient’ in fact is the correct, conscious use of the technique as intended – for example, do the participant actually engage in the creative problem solving efforts required for effective coping planning, or do they in fact mentally visualize the steps they are guided through for mental imagery exercises, thus fulfilling the intended function of the BCT? – This putting forth the BCT's intended mechanism of action may not be fully captured by the intervention-specific usage data only.
The AdditionPlus (Griffin et al., Citation2011; Hankonen et al., Citation2015) was one of the first trials to have measured participant enactment of a wide range of intervention BCTs, particularly in relation to dietary and physical activity changes over the course of a 12-month follow-up period. The shortcomings of that study included the dichotomous measuring of use vs. non-use, and a non-differentiation of an item measuring whether one has ‘motivated oneself to sustain changes’ – this could entail several individual BCTs. Another research project, the Let's Move It cluster-randomized trial that evaluates a school-based multi-level intervention to promote physical activity and decrease sedentary behaviors among older adolescents (Hankonen et al., Citation2016), attempted to take a further step to define and measure what participants actually do in response to intervention prompts. Here, I acknowledged that some BCTs may essentially be sufficient to be enacted only once (e.g., set a physical activity goal), but that the effectiveness of other BCTs requires regular or frequent repetition (e.g., self-monitoring of physical activity).
Distinction between motivational and self-regulation strategies
A significant gap in measurement and theorizing of self-enacted BCTs involves the ones relating to motivation and motivating oneself. Some earlier work has indeed measured goal setting or action planning as a result of the intervention, but not all the techniques or strategies that were theoretically assumed to be enacted by the participants. Furthermore, various strategies how participants sustain their motivation has been an under-investigated area. Although several social cognitive models (e.g., HAPA) may include motivational determinants as precursors of intention formation and motivation, and not directly behavior, such factors continue to be important (at least for some regularly repeated behaviors) also in the post-intentional phase. For instance, we have an understanding factors influencing self-efficacy, but not about the active steps individuals can take to further improve – or sustain – their self-efficacy, during behavior change or goal striving processes. Advancing our theories about the specifics of the key mental and other processes involved in behavior change would help in designing better interventions to induce or support those mental, self-manageable processes.
Sustaining one's motivation may be the key to prolonged behavior change. This aspect has indeed been raised in several behavior change theories (for a review, see Kwasnicka et al., Citation2015). A significant aspect in theorization of self-enactable BCTs involves the distinction between motivational and volitional processes. First, pre-intentional phase of behavior change, becoming motivated or forming an intention has been separated from a volitional phase, where the intention has been formed and goal pursuit takes place. Thus in the volitional post-intentional phase, behavior change progress is not assumed to benefit from further increases targeting motivation or will. However, in real life, this motivation may fluctuate and requires to be kept at a certain level in order for the behavior to be maintained (e.g., Kwasnicka et al., Citation2015). There is surprisingly little research into the role that an individual may play in proactively self-managing levels of motivation, even though there is a host of theories regarding what others (e.g., teachers, managers, coaches) can do to promote a motivational climate. For instance, the self-determination theory (Deci & Ryan, Citation2000) outlines activities and intervention strategies related to fostering autonomous, self-determined motivation (e.g., autonomy supportive facilitation style), but does not propose individual-level strategies for fostering one's own motivation.
Hence, I argue that in addition to self-regulatory techniques, we should attempt to theorize on, synthesize current understanding on, intervene on and measure various ‘self-motivational’ techniques. More precisely, we should also attempt to understand the motivational impact of such self-regulatory (and other) techniques. People may use distinct strategies of self-management of motivation and its daily fluctuation, for example, ‘Managing cognitive salience of various outcomes’, ‘Managing a balance of fear of negative consequences’, ‘Managing correct basic assumptions’, ‘Actively seeking knowledge’, etc. Such motivation self-management strategies could cluster into subgroups such as cognitive, relational, behavioral, and structural/environmental strategies.
Better understanding of intra-individual dynamics of motivation and strategies for ‘self-management of motivation’ could both advance the theory of motivation and enable effective interventions to improve wellbeing. Behavior change research could benefit from acknowledging the key role of individual motivation for the often challenging process of behavior change and, in particular, sustenance of such a change.
Improving promotion of enactment of BCTs
In interventions with null results, it may be that the intervention model and selected behavior change strategies may be valid, but that the lack of overall effect may stem from suboptimal promotion of the use of these strategies (Greaves, Citation2015). If less than a third of intervention participants enacted all of the intervention techniques that they were prompted to (Hankonen et al., Citation2015), a failure to find an effect may not only be a failure of the program content or an inadequate delivery, but also a failure by the target group to take up the intended skills. This points to a weak link in the middle of the causal chain, and prompts us to ask: How to inspire participants to use techniques suggested?
Greaves (Citation2015) notes that we should consider the enactment or use of BCTs as a behavioral target in itself, and investigate a new ‘second order’ question: How to increase the uptake and use of BCTs? ‘What ‘meta behavior change techniques’ (MBCTs) or intervention-delivery techniques (IDTs) are effective in motivating, supporting, and maintaining the use of the BCTs targeted by the intervention?’ For instance, to prompt self-monitoring of physical activity, is it sufficient to simply give people a pedometer and some instructions? Can we use existing techniques, such as ‘prompting practice’ or encouraging social support (e.g., asking partners to remind or encourage the participant to use the pedometer)? Or, do we need novel techniques to promote the uptake and maintenance of BCTs?
Another interesting question relates to the interrelationships between BCTs from this perspective of delivery, receipt and enactment of BCTs. For example, could ‘social support’ entail prompting the use of more self-enacted BCTs? Weekly meetings of peer support groups, or support phone calls, may act as a prompt for the individual to actually self-monitor or resume to goal setting or review activities – and that might actually be the active ingredient of the intervention rather than the social support per se. This hierarchical ordering or ‘nesting’ of BCTs within one another may be another interesting future avenue of inquiry. These calls are not new, of course: various intervention development frameworks and approaches (e.g., Bellg et al., Citation2004; Eldredge et al., Citation2011) have noted that developers have to make sure the receipt of BCTs (or treatment skills) among the participants is optimal, and that participants are motivated and able to enact them (Bellg et al., Citation2004).
In intervention development, adopting the person-centered approach would aid in the feasibility testing and optimization phase. If feasibility studies could identify which of the BCTs are least well met and taken up by the target group, then the intervention program could be better optimized to prompt uptake of the less frequently used BCTs, or consider modifying the intervention theory (for an example, see Hankonen et al., Citation2017). This is likely to make interventions more acceptable, practicable and thereby also effective. Alternatively, attention to this in the development phase may prevent proceeding with interventions with low likelihood of sufficient enactment fidelity in practice.
In addition to promoting uptake, such better focus would enable helping participants’ correct use of the BCTs. Investigation of how the participants interpret and perceive BCTs as they are delivered in interventions may also generate insights to barriers of enactment. Qualitative process evaluation studies on the BCT reception and enactment may reveal important misconceptions that may hinder the optimal uptake of BCTs (e.g., Donnachie et al., Citation2017; Palsola et al., Citation2020) and offer important insights into incorporating new ‘meta-BCTs’ to enhance the intervention.
It should be acknowledged that not all BCTs necessarily need to be taken up by all participants within an intervention. Interventions can be seen as offering toolboxes of several BCTs where participants can pick suitable for them (see also Abraham, Citation2008). Indeed, in the context of a complex behavior change intervention, it may be unrealistic to expect enactment of every BCT or even 80% of them (80–100% integrity often considered high fidelity; Borrelli, Citation2011). Menu-based interventions are not a one-size-fits-all approach, but rather, self-tailored in that participants select components most relevant to them (32). However, in personalized, for example, just-in-time adaptive interventions, where participants are prompted with messages suited to them, based on data (e.g., Hardeman et al., Citation2019), expectations of enactment are likely to be higher, and monitoring whether participants enact the BCTs tailored precisely to them (Hekler et al., Citation2020) should become all the more important. These interventions may also offer exciting opportunities to investigate what factors improve uptake of offered BCTs, and inter-individual variation therein.
Conclusion
This text has argued that we should focus on fidelity beyond delivery – participant receipt and enactment, both in terms of intervention development and evaluation. In the domain of weight loss, there has been a recent development into this direction (Hartmann-Boyce et al., Citation2016), but we need approaches that are applicable across behavioral domains. A useful starting point for this work may be the recently published compendium of self-enactable techniques to change and self-manage motivation and behavior (Knittle et al., Citation2020) that integrates various self-management methods from a variety of sources including existing taxonomies. However, it is only the beginning.
Intervention theories would benefit from more explicit theorizing on what we expect intervention participants to do and how frequently, in terms of BCTs. This is an especially central concern for interventions where direct contact with and support for the target group is limited, and for individually-targeted interventions (e.g., eHealth interventions). A person-centered focus on BCT use would not only help delivering and using the intervention, but also evaluating the process and thus understanding the trial outcomes. Furthermore, it could help us make important advances in understanding possibly individual change pathways and build a more relevant and accurate theory of behavior change via focusing on the real actions of individuals. Goal pursuit and motivation has long traditions within for example social psychology (e.g., Fishbach & Ferguson, Citation2007), integrating such basic research insights with intervention development and evaluation could strengthen both our understanding of behavior change and interventions. In sum, behavior change science would in several ways benefit from focusing more on what participants actually do to intervene on themselves in interventions.
Authors’ contributions
The first and sole author is responsible for writing the entire article.
Acknowledgments
The author wishes to thank Dr. Minna Stenius, Dr. Keegan Knittle, Dr. Elaine Toomey and anonymous reviewers on useful comments to previous versions of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 BCTs are not the only active ingredients, as also other intervention features (e.g. relational techniques or form of delivery components) might also drive intervention effectiveness.
2 It is possible to use ‘information on consequences of behaviour’ in an active, self-enacting way that, e.g. by seeking health relevant information or reminding oneself of health consequences. Also, the BCT self-monitoring can be a largely passive BCT, e.g. when done automatically through devices such as accelerometer (see Harkin et al., Citation2016).
3 BCTs have implicit underlying assumptions, e.g. ‘information on consequences of behaviour’ might have assumptions such as message attention, understanding, memorising, retrieval, integration or self-monitoring has the underlying assumption that the individual has a way to monitor their behavior sufficiently accurately and engages with the monitoring output. For the BCT ‘mental rehearsal of behaviour’, the underlying assumptions might be similar to the assumptions of ‘information on consequences of behaviour’ in that it requires cognitive engagement with the BCT to exert its effects.
References
- Abraham, C. (2008). Beyond stages of change: Multi-determinant continuum models of action readiness and menu-based interventions. Applied Psychology, 57(1), 30–41. https://doi.org/10.1111/j.1464-0597.2007.00320.x
- Adams, J., Mytton, O., White, M., & Monsivais, P. (2016). Why are some population interventions for diet and obesity more equitable and effective than others? The role of individual agency. PLOS Medicine, 13(4), e1001990. https://doi.org/10.1371/journal.pmed.1001990
- Bellg, A. J., Borrelli, B., Resnick, B., Hecht, J., Minicucci, D. S., Ory, M., … Czajkowski, S. (2004). Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH behavior change consortium. Health Psychology, 23(5), 443–451. https://doi.org/10.1037/0278-6133.23.5.443
- Borrelli, B. (2011). The assessment, monitoring, and enhancement of treatment fidelity in public health clinical trials. Journal of Public Health Dentistry, 71(s1), S52–S63. https://doi.org/10.1111/j.1752-7325.2011.00233.x
- Deci, E., & Ryan, R. (2000). The “what” and” why” of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry, 11(4), 227–268. https://doi.org/10.1207/S15327965PLI1104_01
- Donnachie, C., Wyke, S., Mutrie, N., & Hunt, K. (2017). ‘It’s like a personal motivator that you carried around wi’ you’: Utilising self-determination theory to understand men’s experiences of using pedometers to increase physical activity in a weight management programme. International Journal of Behavioral Nutrition and Physical Activity, 14(1), 61. https://doi.org/10.1186/s12966-017-0505-z
- Durlak, J. A., & DuPre, E. P. (2008). Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology, 41(3–4), 327–350. https://doi.org/10.1007/s10464-008-9165-0
- Eldredge, L. K. B., Parcel, G. S., Kok, G., Gottlieb, N. H., & Fernández, M. E. (2011). Planning health promotion programs: An intervention mapping approach. John Wiley & Sons.
- Fishbach, A., & Ferguson, M. J. (2007). The goal construct in social psychology. In A. W. Kruglanski & E. T. Higgins (Eds.), Social psychology: Handbook of basic principles (pp. 490–515). The Guilford Press.
- Gardner, B., Rebar, A. L., & Lally, P. (2020). Habit interventions. In M. S. Hagger, L. Cameron, K. Hamilton, N. Hankonen, & T. Lintunen (Eds.), The handbook of behaviour change (pp. 599–616). Cambridge University Press.
- Gillison, F., Stathi, A., Reddy, P., Perry, R., Taylor, G., Bennett, P., … Greaves, C. (2015). Processes of behavior change and weight loss in a theory-based weight loss intervention program: A test of the process model for lifestyle behavior change. The International Journal of Behavioral Nutrition and Physical Activity, 12(1), https://doi.org/10.1186/s12966-014-0160-6
- Greaves, C. J. (2015). Uptake of behavior change techniques – A key focus for process analysis and for intervention delivery: A comment on Hankonen et al. Annals of Behavioral Medicine, 49(1), 1–2. https://doi.org/10.1007/s12160-014-9630-y
- Griffin, S. J., Simmons, R. K., Williams, K. M., Prevost, A. T., Hardeman, W., Grant, J., … the ADDITION-Plus study team. (2011). Protocol for the ADDITION-Plus study: A randomised controlled trial of an individually-tailored behaviour change intervention among people with recently diagnosed type 2 diabetes under intensive UK general practice care. BMC Public Health, 11(1), 211. https://doi.org/10.1186/1471-2458-11-211
- Hankonen, N., Absetz, P., & Araújo-Soares, V. (in press). Changing activity behaviours in vocational school students: The stepwise development and optimised content of the ‘Let's Move it’ intervention. Health Psychology and Behavioral Medicine. https://doi.org/10.1080/21642850.2020.1813036
- Hankonen, N., Heino, M. T. J., Araujo-Soares, V., Sniehotta, F. F., Sund, R., Vasankari, T., … Haukkala, A. (2016). ‘Let’s Move It’ – a school-based multilevel intervention to increase physical activity and reduce sedentary behaviour among older adolescents in vocational secondary schools: A study protocol for a cluster-randomised trial. BMC Public Health, 16(1), 451. https://doi.org/10.1186/s12889-016-3094-x
- Hankonen, N., Heino, M. T. J., Hynynen, S.-T., Laine, H., Araújo-Soares, V., Sniehotta, F. F., … Haukkala, A. (2017). Randomised controlled feasibility study of a school-based multi-level intervention to increase physical activity and decrease sedentary behaviour among vocational school students. International Journal of Behavioral Nutrition and Physical Activity, 14(1), 37. https://doi.org/10.1186/s12966-017-0484-0
- Hankonen, N., Sutton, S., Prevost, A. T., Simmons, R. K., Griffin, S. J., Kinmonth, A. L., & Hardeman, W. (2015). Which behavior change techniques are associated with changes in physical activity, diet and body mass index in people with recently diagnosed diabetes? Annals of Behavioral Medicine, 49(1), 7–17. https://doi.org/10.1007/s12160-014-9624-9
- Hardeman, W., Houghton, J., Lane, K., Jones, A., & Naughton, F. (2019). A systematic review of just-in-time adaptive interventions (JITAIs) to promote physical activity. International Journal of Behavioral Nutrition and Physical Activity, 16(1), 31. https://doi.org/10.1186/s12966-019-0792-7
- Harkin, B., Webb, T. L., Chang, B. P. I., Prestwich, A., Conner, M., Kellar, I., … Sheeran, P. (2016). Does monitoring goal progress promote goal attainment? A meta-analysis of the experimental evidence. Psychological Bulletin; Washington, 142(2), 198. https://doi.org/10.1037/bul0000025
- Hartmann-Boyce, J., Aveyard, P., Koshiaris, C., & Jebb, S. A. (2016). Development of tools to study personal weight control strategies: OxFAB taxonomy. Obesity, 24(2), 314–320. https://doi.org/10.1002/oby.21341
- Hekler, E., Tiro, J. A., Hunter, C. M., & Nebeker, C. (2020). Precision health: The role of the social and behavioral sciences in advancing the vision. Annals of Behavioral Medicine, kaaa018), https://doi.org/10.1093/abm/kaaa018
- Knittle, K., Heino, M., Marques, M. M., Stenius, M., Beattie, M., Ehbrecht, F., … Hankonen, N. (2020). The compendium of self-enactable techniques to change and self-manage motivation and behaviour v.1.0. Nature Human Behaviour, 1–9. https://doi.org/10.1038/s41562-019-0798-9
- Knittle, K., Nurmi, J., Crutzen, R., Hankonen, N., Beattie, M., & Dombrowski, S. U. (2018). How can interventions increase motivation for physical activity? A systematic review and meta-analysis. Health Psychology Review, 12(3), 211–230. https://doi.org/10.1080/17437199.2018.1435299
- Kok, G., Gottlieb, N. H., Peters, G.-J. Y., Mullen, P. D., Parcel, G. S., Ruiter, R. A. C., … Bartholomew, L. K. (2016). A taxonomy of behaviour change methods: An intervention Mapping approach. Health Psychology Review, 10(3), 297–312. https://doi.org/10.1080/17437199.2015.1077155
- Kwasnicka, D., Dombrowski, S. U., White, M., & Sniehotta, F. F. (2015). Data-prompted interviews: Using individual ecological data to stimulate narratives and explore meanings. Health Psychology, 34(12), 1191–1194. https://doi.org/10.1037/hea0000234
- Marteau, T. M., Fletcher, P. C., Hollands, G. J., & Munafo, M. R. (n.d). Changing behaviour by changing environments. In M. S. Hagger, L. Cameron, K. Hamilton, N. Hankonen, & T. Lintunen (Eds.), The handbook of behaviour change (pp. 193–207). Cambridge University Press.
- Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., … Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. https://doi.org/10.1007/s12160-013-9486-6
- Michie, S., West, R., Sheals, K., & Godinho, C. A. (2018). Evaluating the effectiveness of behavior change techniques in health-related behavior: A scoping review of methods used. Translational Behavioral Medicine, 8(2), 212–224. https://doi.org/10.1093/tbm/ibx019
- Moller, A. C., Merchant, G., Conroy, D. E., West, R., Hekler, E., Kugler, K. C., & Michie, S. (2017). Applying and advancing behavior change theories and techniques in the context of a digital health revolution: Proposals for more effectively realizing untapped potential. Journal of Behavioral Medicine, 40(1), 85–98. https://doi.org/10.1007/s10865-016-9818-7
- Moore, G. F., Audrey, S., Barker, M., Bond, L., Bonell, C., Hardeman, W., … Baird, J. (2015). Process evaluation of complex interventions: Medical Research Council guidance. BMJ, 350(mar19 6), h1258. https://doi.org/10.1136/bmj.h1258
- Ogden, J. (2016). Celebrating variability and a call to limit systematisation: The example of the behaviour change technique taxonomy and the behaviour change wheel. Health Psychology Review, 10(3), 245–250. https://doi.org/10.1080/17437199.2016.1190291
- O’Shea, O., McCormick, R., Bradley, J. M., & O’Neill, B. (2016). Fidelity review: A scoping review of the methods used to evaluate treatment fidelity in behavioural change interventions. Physical Therapy Reviews, 21(3–6), 207–214. https://doi.org/10.1080/10833196.2016.1261237
- Palsola, M., Renko, E., Kostamo, K., Lorencatto, F., & Hankonen, N. (2020). Thematic analysis of acceptability and fidelity of engagement for behaviour change interventions: The let’s Move It intervention interview study. British Journal of Health Psychology, https://doi.org/10.1111/bjhp.12433
- Prochaska, J. O., & Velicer, W. F. (1997). The transtheoretical model of health behavior change. American Journal of Health Promotion, 12(1), 38–48. https://doi.org/10.4278/0890-1171-12.1.38
- Rixon, L., Baron, J., McGale, N., Lorencatto, F., Francis, J., & Davies, A. (2016). Methods used to address fidelity of receipt in health intervention research: A citation analysis and systematic review. BMC Health Services Research, 16(1), 663. https://doi.org/10.1186/s12913-016-1904-6
- Toomey, E., Hardeman, W., Hankonen, N., Byrne, M., McSharry, J., Matvienko-Sikar, K., & Lorencatto, F. (2020). Focusing on fidelity: Narrative review and recommendations for improving intervention fidelity within trials of health behaviour change interventions. Health Psychology and Behavioral Medicine, 8(1), 132–151. https://doi.org/10.1080/21642850.2020.1738935
- Walton, H., Spector, A., Tombor, I., & Michie, S. (2017). Measures of fidelity of delivery of, and engagement with, complex, face-to-face health behaviour change interventions: A systematic review of measure quality. British Journal of Health Psychology, 22(4), 872–903. https://doi.org/10.1111/bjhp.12260
- Walton, H., Spector, A., Williamson, M., Tombor, I., & Michie, S. (2020). Developing quality fidelity and engagement measures for complex health interventions. British Journal of Health Psychology, 25(1), 39–60. https://doi.org/10.1111/bjhp.12394
- Zhang, C.-Q., Zhang, R., Schwarzer, R., & Hagger, M. S. (2018). A meta analysis of the health action process approach. PsyArXiv, https://doi.org/10.31234/osf.io/4pc27