
ABSTRACT
Stress leads to detrimental health outcomes through direct biological and indirect behavioural changes. Stress can lead to disruption to normal eating behaviours, although the strength of these associations is unknown. This is the first meta-analysis to determine the strength of the stress-eating relationship in healthy adults and to explore the impact of potential moderators. Studies included had a clearly defined measure of stress (i.e., any noxious event or episode in one’s environment with the exclusion of emotional distress) that was linked to non-disordered eating. Key terms were searched in Medline, PsycInfo and Ovid databases (23,104 studies identified). 54 studies (combined N = 119,820) were retained in the meta-analysis. A small, positive effect size was found for the stress-overall food intake relationship (Hedges’ g = 0.114). Stress was associated with increased consumption of unhealthy foods (Hedges’ g = 0.116) but decreased consumption of healthy foods (Hedges’ g = −0.111). Only one significant moderator (restraint on stress-unhealthy eating) was identified. This meta-analysis identified the magnitude of the effect of stress on eating behaviour outcomes. Significant heterogeneity was observed that was not explained by the moderators examined. Further research on moderators of the stress-eating relationship is required and should distinguish effects for healthy versus unhealthy eating.
Introduction
Understanding the influence of stress on health presents an ongoing challenge due to the complex nature of stress and the behavioural, endocrine and neural systems involved (Finch et al., Citation2019; O’Connor et al., Citation2021). Previous research has shown that high levels of stress have been directly linked with greater risk of a range of diseases and health conditions such as cardiovascular disease, hypertension, stroke, obesity, immune function, and accelerated rates of disease progression (Cohen et al., Citation2007, Citation2012; Morera et al., Citation2019; O’Connor et al., Citation2021; Steptoe & Kivimäki, Citation2012; Tomiyama, Citation2019). Stress is thought to influence health via two distinct but interacting pathways: a direct, biological pathway (e.g., by influencing neuroendocrine and autonomic processes) and an indirect, behavioural pathway (e.g., by influencing habitual and non-habitual health behaviours) (O’Connor et al., Citation2021). These pathways are likely to operate in a bi-directional fashion, with changes in behaviour impacting biology, and changes in biology influencing behavioural changes which affect health.
Over the past twenty-five years, a considerable amount of research has investigated the relationship between stress and eating behaviour and a large number of studies have shown that stress is associated with changes in food intake in adults and children (Araiza & Lobel, Citation2018; Dallman et al., Citation2003; Greeno & Wing, Citation1994; Hill et al., Citation2018; O’Connor & Conner, Citation2011; Wardle et al., Citation2000). In fact, it has been estimated that 35–40% of people increase their food intake when experiencing stress, whilst the remaining proportion either decrease or do not change their food intake in response to stress (Oliver & Wardle, Citation1999; Pool et al., Citation2015; Sproesser et al., Citation2014). Moreover, where changes are observed in eating habits under conditions of stress, these have been shown to manifest in two contrasting ways (Greeno & Wing, Citation1994; Hill et al., Citation2018; O’Connor & Conner, Citation2011; Wardle et al., Citation2000). For example, where stress is experienced chronically, an individual may increase their food intake in response to stress, which can in turn lead to weight gain through chronic, positive energy balance (Newman et al., Citation2007; Torres & Nowson, Citation2007). In contrast, an individual may decrease their food intake, subsequently leading to weight loss through chronic, negative energy balance. However, the dysregulation of bio-behavioural responses to food consumption, in particular, increased high fat, energy dense foods under conditions of stress has received the most research attention, given the longer-term implications for physical disease risk (O’Connor & Conner, Citation2011; Ulrich-Lai et al., Citation2010). Nevertheless, surprisingly, there has been no meta-analytical synthesis of the stress-eating evidence base and the magnitude of this relationship remains unknown.
The concept of stress has had a long and productive history, but it also has its critics who have highlighted the simplistic, inconsistent and imprecise use of the term (see Segerstrom & O’Connor, Citation2012). Stress can be conceptualised as a stimulus, a response, or as a transaction between the person and their environment (O’Connor & Ferguson, Citation2016). In the latter case, stress is defined as ‘a particular relationship between the person and the environment that is appraised by the person as taxing or exceeding his or her resources and endangering his or her well-being’ (Lazarus & Folkman, Citation1984, p. 19). The notion of stress appraisal is central to Lazarus and Folkman’s (Citation1984) transactional model of stress. Stress appraisals are the interpretations of events in terms of their benefit or harm for the individual and are posited to have two dimensions: primary and secondary appraisals (Lazarus & Folkman, Citation1984). Primary appraisal involves the evaluation of the risks, demands, or challenges of a situation, while secondary appraisal evaluates the availability of perceived resources and whether anything can be done to alter the outcome of the situation. Therefore, in this meta-analysis, informed by the transactional model, stress was considered to be any noxious event or episode which has the potential to be perceived as threatening, harmful or loss provoking to an individual (Lazarus, Citation1999). Moreover, given the conceptualisation issues mentioned above, in the current meta-analysis, we included only studies that incorporated: (i) a measure of stress (i.e., any noxious event or episode in one’s environment that could be appraised as threatening, risky or harmful) which was clearly defined (in the description and/or study design employed) within the paper and, (ii) a measure of eating behaviour linked to that stress measure. More specifically, included studies were required to have a discrete measure of stress that captured the participants’ appraisal of a recent, current or on-going stressor, or included a validated technique or paradigm developed through research that reliably induces stress (e.g., the Trier Social Stress Test). Studies which exclusively focused on emotions and/or emotional distress were excluded as these constructs were considered to be responses to stressors, opposed to a specified measure of stress itself. This exclusion was added in order to refine the scope of the review.
Moderators of stress and eating
The present review also aimed to investigate a range of potential moderating variables of the stress and eating relationship. The rationale for including specific moderating variables was informed by previous literature reviews (see below) and by the extent to which the relevant data was available in the identified studies for inclusion (outlined in the Method).
As noted above, one key moderator may be the nature of the food consumed in response to stress, with some foods such as unhealthy high fat foods more likely to be consumed and some foods such as healthy low fat and low sugar foods less likely to be consumed. Given the potential importance of food type we structured our examination of other moderators by food type (i.e., exploring moderating effects across all foods and within healthy and unhealthy foods). Moreover, the individual differences model of stress and eating suggests that differences in learning history, attitudes towards eating, or biology produce variations in vulnerability to the effects of stress (Araiza & Lobel, Citation2018; Gibson, Citation2012; Greeno & Wing, Citation1994; O’Connor & Conner, Citation2011; Tomiyama, Citation2019). Those exhibiting vulnerability are assumed to respond to stress with an environmental, psychological or physiological change that has an effect on eating behaviour. Previous research has shown that stress influences the type of foods chosen as well as the amount of food consumed (Araiza & Lobel, Citation2018; Hill et al., Citation2018; O’Connor & Conner, Citation2011). In some individuals, the intake of unhealthy foods (i.e., high energy low nutrient foods) appears to increase as a function of stress (for a literature review see Lyzwinski et al., Citation2018). Studies have found that stress is associated with increased consumption of unhealthy foods, particularly those high in fat and sugar (Newman et al., Citation2007; Roberts et al., Citation2014). In contrast, stress has been negatively associated with the consumption of low energy high nutrient foods (i.e., healthy foods), particularly fruit and vegetables, where intake of these foods decreases as stress increases (Mikolajczyk et al., Citation2009; O'Connor et al., Citation2008; Wallis & Hetherington, Citation2009).
Reward theories posit that, under conditions of stress, changes in glucocorticoids (including cortisol) and corticotropin-releasing factor sensitise areas of the brain associated with reward (e.g., nucleus accumbens), increasing the drive to eat high energy, low nutrient and highly palatable foods (Cottone et al., Citation2009; Sinha & Jastreboff, Citation2013). Consequently, eating habits are maintained through a positive feedback loop where highly palatable foods are perceived as being rewarding under conditions of stress which in turn enhances the salience of these foods (Nieuwenhuizen & Rutters, Citation2008; Sominsky & Spencer, Citation2014). Given these differential effects of stress on types of food intake, previous reviews have explored the impact of stress on unhealthy and healthy eating behaviour, together with overall food intake (e.g., Adam & Epel, Citation2007; Araiza & Lobel, Citation2018; Hill et al., Citation2018; Lyzwinski et al., Citation2018; Torres & Nowson, Citation2007).
Several groups have been identified who likely differ in their responses to stress and these include: women versus men; normal weight versus overweight/obese; restrained (i.e., those attempting to control their food intake or dieters) versus unrestrained eaters. Age is another potential moderating variable that has received less research attention but that is considered in the current meta-analysis. Alongside individual differences variables, it is likely that additional heterogeneity in the stress-eating effect size will be accounted for by study specific characteristics, such as study quality, the type of stress measure included in the study, and the sample size. Therefore, these study specific characteristics were also included as potential moderating variables. The rationale for including each of these moderating variables is presented briefly below.
The effect of stress on eating behaviour is thought to influence women and men differently. Research has indicated that females are more likely to change their normal eating behaviours when experiencing stress compared to males (Mikolajczyk et al., Citation2009; Sims et al., Citation2008; Stone & Brownell, Citation1994; Weinstein et al., Citation1997); however this difference between genders has not been consistently found in previous research (Barrington et al., Citation2014; Conner et al., Citation1999; El Ansari & Berg-Beckhoff, Citation2015; Reichenberger et al., Citation2018). Furthermore, some studies have used exclusively female samples (e.g., Habhab et al., Citation2009; Wallis & Hetherington, Citation2009), making it difficult to interpret the strength of stress-related eating in males and females separately.
Body weight has been found to influence stress-related food consumption. Previous studies have found that weight is positively associated with stress-related eating behaviours, where heavier individuals are more susceptible to increased food consumption when stressed compared to those lower in weight (Cotter & Kelly, Citation2018; Greeno & Wing, Citation1994; Sinha, Citation2018; Tomiyama, Citation2019; Yau & Potenza, Citation2013). However, the findings from some earlier reviews have been inconsistent (e.g., Greeno & Wing, Citation1994), therefore, it would be useful to establish in the broader, cumulative literature whether body weight (e.g., normal weight versus overweight/obese) moderates the stress-eating relationship.
Eating styles are thought to moderate food consumption when experiencing stress (e.g., restraint, emotional, and external eating; Adam & Epel, Citation2007; Greeno & Wing, Citation1994; Wardle et al., Citation2000). In particular, research has found that individuals higher in dietary restraint and emotional eating are more likely to engage in stress-related eating behaviours compared to those lower in these styles (Adriaanse et al., Citation2011; O'Connor et al., Citation2008; Torres & Nowson, Citation2007; Wallis & Hetherington, Citation2004). Nevertheless, the extent to which these variables are robust and consistent moderators of the stress-eating relationship is unclear.
The final individual differences variable considered as a potential moderator of the stress-eating relationship is age. The effects of stress on eating outcomes have been investigated across a range of ages, with findings from studies in children and adolescents (Hill et al., Citation2018; O’Connor, Citation2018) and adults (Araiza & Lobel, Citation2018; Lyzwinski et al., Citation2018). However, evidence is beginning to emerge to suggest that there may be differences in the triggers of food intake between children and adults. For example, Moss et al. (Citation2021), have recently shown that unhealthy snack responses to negative emotion are greater in young adults compared to children and that healthy snack responses to positive emotion are greater in children compared to adults. These findings notwithstanding, it is important to establish whether the effects of stress on eating behaviour are similar or different across samples of adults with different ages.
As outlined above, it is also important to establish the extent to which study specific characteristics may also account for the heterogeneity in stress-eating findings. In particular, we were interested in exploring the influence of study quality, sample size and type of stress measure. Study quality has been identified as a longstanding issue in stress research (e.g., Kasl & Cooper, Citation1987) and has been found to be a key moderator in related reviews and meta-analyses (e.g., Wardle et al., Citation2011). Moreover, study quality is a useful approximation to compare studies against differing criteria, including sampling methods, consideration of potential covariates and validity and reliability of measures used. Using three categories of study quality (weak, moderate and strong), the present meta-analysis aimed to determine whether these study factors would influence the strength of potential effects between stress and food consumption (both overall food consumption, and intake of healthy and unhealthy foods). Sample size was included as a moderator in the present meta-analysis to determine whether the strength of associations between stress and food consumption was influenced by the reported sample sizes of studies included in this review.
We were also interested in exploring whether the type of stress measure moderated the strength of the relationship between stress and eating. Previous research has found associations between stress and eating habits using different types of study design, including stress induction paradigms (e.g., Oliver et al., Citation2000), daily diary studies (e.g., Conner et al., Citation1999; O'Connor et al., Citation2008) and questionnaire-based surveys of perceived stress at different time points (e.g., Vidal et al., Citation2018). Therefore, we wanted to determine whether the type of stress measure (either perceived or induced stress) moderated associations between stress and food consumption.
Aims
To summarise, this review aimed to synthesise previous research on stress-eating relationships in healthy adults and to determine the strength of the association. Furthermore, the review aimed to investigate the effects of stress on the amount of overall food consumed, as well as separately for unhealthy and healthy foods along with an examination of moderating variables of the stress and food intake relationship (i.e., gender, weight status, eating styles, age, study quality, stress measure and sample size). Given the hypothesised differences between unhealthy and healthy eating, the moderator analyses were performed across the full sample and then separately within studies measuring unhealthy or healthy eating as outcomes.
Method
Search terms
The systematic review and meta-analysis was registered on PROSPERO on the 12th December 2017 (record number CRD42017082646). Online databases were searched on the 17th of October 2019 using key terms which were combined using Boolean operators. Key terms were searched in PsycINFO (1806 to Present) and Ovid databases (Ovid MEDLINE and Epub Ahead of Print, In-Process and other Non-Indexed Citations, Daily and Versions, 1946 to October 7th 2019). The database search was limited to human studies, English language, journal articles and restricted by age (≥18 years old). Search terms were based on those used in a previous meta-analysis (Hill et al., Citation2018) and based on key terms used in relevant studies. The search terms were informed by the conceptualisation of stress outlined for the purposes of this meta-analysis (see supplementary materials for full list of search terms in an example search strategy). Additionally, reference lists of papers included at full text level were hand searched to include relevant studies which were not initially identified via the online database search.
Inclusion and exclusion criteria
Papers were screened for their inclusion in the meta-analysis based on the study population, stress measurement used and type of eating behaviour. Papers were included in the review if participants were aged 18 years or older. Studies that were partially within the age range (for example 16–25 years old) were retained in the screening process to determine whether data were available on the adult participants within the study. Studies that reported a mean age of at least 18 years old were retained in the meta-analysis. The review included any healthy populations of adults, which was defined as individuals without any pre-existing physical or psychological illnesses. Only healthy adults were included due to the comorbidities between psychological wellbeing and poorer health generally (Scott et al., Citation2016). Similarly, studies that focused exclusively on clinical patients or individuals with disordered eating behaviours (e.g., bulimia) were excluded from the review.
In addition, studies were retained in the review if they included a measurement of stress and a clear eating outcome that was linked to the stress measure. More specifically, included studies were required to have a discrete measure of stress that captured the participants’ appraisal of recent, current or on-going stressors (that have the potential to be perceived as threatening, harmful or loss provoking) or included a validated technique or paradigm developed through research that reliably induces stress. This could include perceptions and appraisals of stress (measured via standardised questionnaires, daily diaries and other self-report measures of acute, on-going or chronic stress) and laboratory-based inductions to stimulate the experience of stress (e.g., Trier Social Stress Task; Kirschbaum et al., Citation1993). Studies which measured constructs other than stress, such as emotional distress (e.g., the Patient Health Questionnaire, Spitzer et al., Citation1999), anxiety (e.g., State-Trait Anxiety Inventory, Spielberger et al., Citation1970) or negative affect (e.g., Positive and Negative Affect Schedule, Crawford & Henry, Citation2004) were not included in the current review. Similarly, studies which did not use a validated measure of stress or did not include a manipulation check for the measurement of stress (such as Sproesser et al., Citation2014) were excluded. We considered emotional distress and negative affect to be responses to stressors (and outwith the specific conceptualisation of stress outlined earlier).
Finally, as indicated above, studies were retained in the review if they included some form of food intake as an eating behaviour that was clearly linked to a stress measure. Eating behaviours included dietary habits, snack consumption, food frequency measures and/or macronutrient intake. Studies were excluded from the review if they focused on body weight as an outcome measure (such as BMI or adiposity). Similarly, studies which measured behaviours around eating without the inclusion of any food intake (such as dietary restraint) were also excluded from the review.
Data and variable coding
Studies were coded based on the type of stress measure and the type of eating outcome as previously outlined in Hill et al. (Citation2018). Stress measures were categorised into perceived stress (which included daily diary studies) or induced stress (such as a stress induction paradigm or stress vs no stress periods). Eating outcomes were categorised into three types of food intake: healthy, unhealthy and other foods. The categorisation of foods was based on nutritional quality of foods (Poon et al., Citation2018). For example, healthy foods were identified as those which are health promoting, such as intake of low energy, high nutrient foods like fruit and vegetables. Unhealthy foods were identified as high energy, low nutrient foods which may be health limiting. Foods that did not fall into either healthy or unhealthy categories, such as macronutrients (like protein, carbohydrates), total energy intake, number of snacks consumed, or non-specific food groups where the nutrient profile could not be accurately determined (e.g., cereals, meat products and fish/seafood products) were categorised as being 'other foods'. Note that this eating outcome was not used in moderation analyses due to the ambiguity of foods included in this categorisation. Study specific details on the categorisation of food outcomes are included as footnotes in the supplementary materials.
Studies with more than one type of food intake were included within each eating outcome (i.e., appearing either once, twice or three times depending on the types of food consumption included within a study). However, to ensure studies were not ‘double counted’ the sample sizes were reduced appropriately. For example, where a study had reported two eating outcomes, sample sizes were halved, while a study reporting three eating outcomes the sample size was divided by three. This correction was only used to allow a meaningful subgroup analysis across the three eating types. This method of accounting for within-study dependencies was compared with an aggregation method (Hoyt & Del Re, Citation2015) which found minimal differences to calculated effect sizes (variations between 0.007 to 0.013 in Hedge’s g), with the reduction in sample sizes producing more conservative estimates of effects sizes than an aggregation method. All data included in the current meta-analysis has been shared and is freely available on the Open Science Framework (see https://osf.io/jk7m9/).
Quality assessment
A quality assessment tool was developed based on the Effective Public Health Practice Project (EPHPP) assessment tool for quantitative studies (Thomas et al., Citation2004). The EPHPP was developed for assessing the quality of randomised controlled trials (RCTs) and includes six component scoring sections; Selection Bias, Study Design, Confounders, Blinding, Data Collection Methods and Withdrawals / Drop-outs. One section (Blinding) was specific to RCTs and was removed from the EPHPP for use in this review. Studies were assessed on the remaining 5 sections (See supplementary materials for the full assessment tool and with scoring instructions). Two component scoring sections (Study Design and Data Collection Methods) were adapted to better reflect the type of studies retained in this review. In the Study Design component section, a rating of strong was given to studies which had used an objective measure of food intake, either across multiple time points or at a single time point. A moderate quality rating was given to studies which had adopted a daily diary methodology or had investigated stress at more than one time point (including longitudinal studies). Finally, a weak Study Design rating was given to studies which had used stress and subjective eating measures at only one time point. Similarly, if the study design could not be determined, it was coded as weak in this component section.
The Data Collection Methods component section was adapted to assess the reliability and validity of stress and eating measures independently to one another. A study was rated as strong in quality when both the stress and eating measures were valid and reliable. A moderate rating was given to studies where both measures are shown to be valid, and one or both measures were either not reliable, or reliability for the measure was not reported. Similarly, if one measure was both valid and reliable, a moderate rating was given. Finally, a weak study quality rating was given in this component section where both the stress and eating measures were neither valid nor reliable, or where validity and reliability could not be determined.
After completion of component sections, studies were assigned a global quality rating following the method outlined by Thomas et al. (Citation2004). Where no weak ratings were given on any of the component scales (i.e., all sections were either strong or moderate), studies were identified as being strong in study quality overall. A moderate global rating was given for studies which included one weak rating out of the 5 component rating sections. Finally, studies were coded as being weak in quality where they scored weak on two or more of the component scales.
Data synthesis
All studies retrieved from the initial database search were screened at title, abstract and full text levels by a reviewer. A minimum of 10% of studies were independently coded by a second reviewer (RM/SW) at title (n = 2,319), abstract (n = 39) and at full text levels (n = 9). Cohen’s kappa (Cohen, Citation1960) value was found to be good overall for the screening process (κ = 0.84), with high agreement levels across title (κ = 0.72) and abstract levels (κ = 0.72), and perfect agreement at full text screening (κ = 1.00).
Study quality was assessed on all papers included in the review using the modified EPHPP tool. At least 10% of studies included in the review (κ = 8) were assessed by an independent reviewer (RM/SW) and agreement levels were calculated. Agreement levels across the five component scales ranged from some disagreements (62%) to agreement accepted in most situations at 80% (Neuendorf, Citation2016). Disagreements were discussed and resolved, resulting in perfect agreement (κ = 1.00) on study quality ratings for the studies.
Method of analysis
Prior to analysis all extracted data were checked by an independent reviewer (FC/SW). Data were synthesised using Comprehensive Meta-Analysis version 3 (Borenstein et al., Citation2005) and effect sizes were calculated using Hedges’ g to account for any small sample sizes included in the review (Orwin, Citation1983). Effect sizes up to 0.49 were considered to be small, between 0.50 and <0.80 medium effect sizes and ≥0.80 were considered large (Cohen, Citation1988). Publication bias was assessed across all studies using a funnel plot of observed and imputed effect sizes, with additional analyses used to determine the severity of potential publication bias in this review.
Standardised residuals were used to assess potential outliers in computed effect sizes. Any studies with a standardised residual > +/− 3 were further investigated using sensitivity analyses. Two studies (Boggiano et al., Citation2015; Conner et al., Citation1999) were identified as potential outliers, with standardised residual values of 6.36 and 3.07 respectively. To determine the impact of potential outliers in the analysis, each study was systematically removed from the overall analysis to determine its individual contribution. Removal of each study in turn resulted in a change to the overall effect size by −0.019 and −0.013 for each of the two studies respectively. Due to the minimal impact overall to the findings, these studies were retained in analyses.
A random effects meta-analysis was used to investigate assumed heterogeneity across studies (Riley et al., Citation2011). Analyses aimed to investigate the association between stress and food consumption overall, across all studies, and determine the effect of moderating variables on this relationship. This same method was employed to investigate the effect of stress on the type of eating outcome (i.e., unhealthy and healthy foods) as well as the other moderation analyses.
The relationship between stress and overall food intake was assessed, with moderation analyses used to determine the effect of stress on type of eating behaviour (unhealthy and healthy) independently. Heterogeneity was assessed for main analyses and moderating variables using Cochran Q tests and I2 (Higgins et al., Citation2003; Lipsey & Wilson, Citation2001), where I2 (reported as a percentage) indicates the degree of heterogeneity across studies, opposed to variance occurring due to chance (Higgins & Thompson, Citation2002).
Pearson’s correlations were used to determine the interdependence between the moderating variables used in analyses. Gender (where data was available for females and males separately), mean BMI, proportion healthy/overweight individuals, mean dietary restraint, mean age, study quality, stress measurement and sample size were each included as moderating variables. Where reported, mean values for dietary restraint were standardised into z-scores to control for the use of different questionnaires.
The moderating effect of categorical variables (i.e., gender, study quality and stress measure) were examined using subgroup analyses where at least four studies were present in each subgrouping. The moderating effect of continuous variables (i.e., mean BMI, proportion of healthy and overweight individuals, eating styles, mean age and sample size) was investigated using meta-regressions (maximum likelihood).
Results
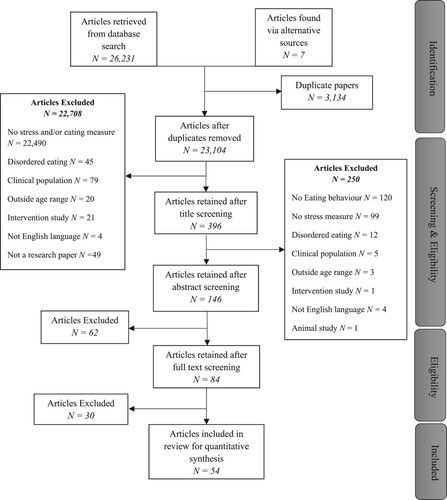
A total of 23,104 unique articles were retrieved from searching electronic databases and hand searching of reference lists (see for a PRISMA flow diagram; Moher et al., Citation2009). The main reason for exclusion from the review at title level was due to articles having no measure of stress or eating behaviours (k = 22,490). Of the 396 studies screened at abstract level, 146 were retained for full text screening. The main reason for exclusion at abstract level was studies not including a measure of food consumption (k = 120). From full text screening, 84 studies were identified for inclusion in the review. During quantitative synthesis, two studies were excluded due to using the same data set as another included paper (O'Connor et al., Citation2009; van Strien et al., Citation2012). A further 28 studies were excluded from the review due to insufficient data, leaving 54 studies included in this review.
Figure 1. PRISMA flow diagram indicating articles retained and excluded at each stage of the screening process (Moher et al., Citation2009).
Study characteristics
The combined sample size from the 54 included studies was 119,820 (range 9 to 65,235 in individual studies), of which 64,775 were female (54.06%) and 54,742 were male (45.69%). Of the 54 studies, 23 used exclusively female participants (comprising of 3,301 participants) and two studies used exclusively male participants (total of 56 participants). Gender was not reported for 303 participants (<1%). Mean age for the total sample was 27.49 years (range 18 to >80 years were reported). Mean age was not reported in five studies. The mean BMI was 24.82 kg/m2 with a range of 20.2 kg/m2 to 36.5 kg/m2. Where reported, studies were categorised by weight status; 13 studies reported the proportion of participants who were a healthy weight (defined as a BMI from 18.5 to 24.9 kg/m2) and the proportion of participants who were overweight/obese (with a BMI over 25 kg/m2). BMI was not reported in 24 studies.
Studies were categorised based on the type of stress measurement and type of eating outcome (for details on coding, see method section). Studies which included multiple stress measures and/or eating outcomes were included within each relevant category. Most studies used a measure of perceived stress (k = 32). Twenty-two studies used a stress induction methodology. Similarly, studies were categorised based on the type of eating outcome. Of the 54 studies included in the review, 35 included a measure of unhealthy food consumption, 17 used healthy food consumption and 31 used a measure of other food intake.
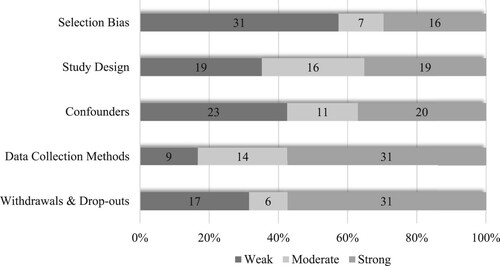
Finally, studies were categorised based on overall study quality. The majority of the studies included in the review were identified as being weak in study quality (k = 30), with fewer being categorised as moderate in study quality (k = 19) and only 5 identified as being strong in study quality. A breakdown of study quality across the five component ratings is presented in . Over half of the studies included in the review were identified as at risk of selection bias where the sample may not provide an accurate reflection of the wider population (for example undergraduate university students enrolled on a Psychology course). However, 31 studies were identified as being strong in their data collection methods (for example, where studies had used valid and reliable scales to measure stress).
Figure 2. Number of studies scoring across 5 quality assessment sections from weak to strong (left to right).
Moderating variables
The selection of moderating variables was determined through the availability of data reported in studies included in the review and informed by previous research reviews (as outlined earlier). Of the moderators initially noted in the pre-registration of the review, only study design (longitudinal vs cross-sectional) was not included due to too few studies adopting a longitudinal design (N = 1). Eating styles were considered as additional moderating variables after the completion of the pre-registration based on the potential availability of data on these variables. Whilst there were sufficient studies to conduct analyses on dietary restraint (i.e., 12 studies reported mean restraint scores), other eating styles (e.g., external and emotional eating) were not analysed due to a lack of available data.
Main findings
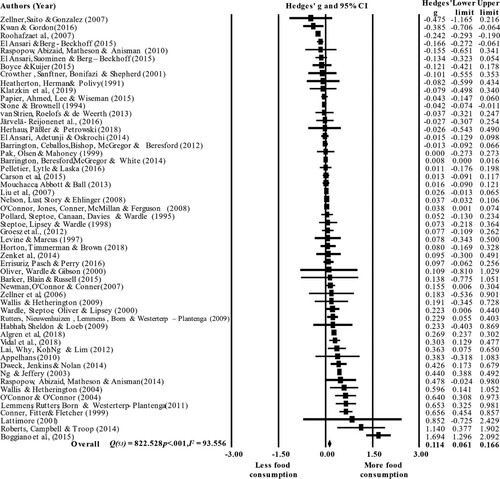
The relationship between stress and overall food intake was initially investigated. A significant positive association was found between stress and food intake, Hedges’ g = 0.114, 95% CIs [0.061, 0.166], Z = 4.255, p < .001. A proportional forest plot of stress and food consumption overall is presented in . There was considerable heterogeneity across subgroup analyses (see ) and considerable heterogeneity across the 54 studies overall, Q(53) =822.528, p < .001, I2 = 93.556. Therefore, further analyses were conducted to investigate whether type of food intake contributed to the high level of heterogeneity (Higgins & Green, Citation2011).
Figure 3. Proportional distribution plot of stress and eating behaviours overall across all studies (k = 54).
Publication bias
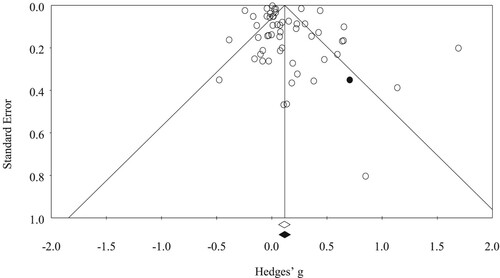
The presence of publication bias was investigated across the 54 studies included in the review. Egger’s regression analyses (Egger et al., Citation1997) indicated that there was not significant publication bias within the review (intercept = 1.086, df = 52, p = .069). A funnel plot of observed and imputed standard error values (see ) indicated that there may be one missing study to the right of the mean. Duval and Tweedie’s Trim and Fill analysis (Duval & Tweedie, Citation2000) indicated that inclusion of the missing study would result in a small increase to the overall effect size (observed Hedges’ g = 0.114, 95% CIs [0.061, 0.166]; computed Hedges’ g = 0.117, 95% CIs [0.065, 0.169]).
Figure 4. Funnel plot of publication bias with observed (white) and imputed (shaded) studies.
Sensitivity analysis was conducted to investigate the relative influence of each study on the main findings. Through the systematic removal of each study in turn, the analysis indicated that changes to the overall study findings of stress and food consumption were minimal, with the largest effect size change of −0.019 to +0.014 in the calculated Hedges’ g (with a change of effect size range from 0.095 to 0.128).
Independence of moderating variables
Pearson’s correlations were used to assess the independence between categorical moderating variables (study quality, stress measure and eating behaviour). No significant associations were found between these categorical moderating variables, therefore each of the moderating variables were investigated independently.
Moderating variables on stress and eating behaviours overall
The moderating effects of gender, study quality and stress measurement were examined via subgroup analyses. For gender, studies were included where the effect of stress on eating behaviour had been reported for males and females separately. The moderating effect of proportion of females, mean age, mean BMI, proportion of healthy / overweight individuals, restraint and sample size on stress and eating overall was investigated using meta-regressions (see and for a sum mary of results).
Table 1. Summary of heterogeneity within and between variable analyses in the meta-analysis (k = 54).
Table 2. Summary of findings from meta-regressions on stress and type of food intake.
Thirty studies included data on females only, with 9 studies including data on males only. No moderating effect of gender on the stress-eating overall relationship was found, Q(1) = 1.107, p = .293. Similarly, no moderating effect was found for the proportion of females on the stress-eating overall relationship, coefficient = 0.001, standard error = 0.002, Z = 0.79, p = .430.
Thirty studies were included in moderation analyses to investigate the effect of mean BMI on stress and eating overall. Mean BMI was not found to moderate the relationship between stress and eating behaviours, coefficient = −0.003, standard error = 0.019, Z = −0.16, p = .872. Further analyses investigated the proportion of healthy and overweight individuals on stress and eating overall. No moderating effect was found for the proportion of healthy weight individuals, coefficient <.001, standard error = 0.003, Z = 0.21, p = .838, nor for the proportion of overweight individuals on the association between stress and eating overall, coefficient = 0.002, standard error = 0.003, Z = 0.76, p = .448.
Twelve studies were included in moderation analyses to investigate the effect of restraint on stress and eating overall. Standardised mean restraint scores were not found to moderate stress and eating overall, coefficient = 0.035, standard error = 0.088, Z = 0.40, p = .687.
Forty-nine studies were included in moderation analyses to investigate the effect of mean age on stress and eating overall. The meta-regression indicated that mean age did not moderate the association between stress and food consumption, coefficient = −0.003, standard error = 0.005, Z = −0.63, p = .531.
The moderating effect of study quality was assessed across all studies included in the review. Analyses indicated that study quality (strong, moderate, weak) did not moderate the association between stress and food intake overall, Q(2) = 5.990, p = .050; however as the Q value was trending towards significant, subgroup analyses were conducted on study quality pairings. Effect sizes were largest and significant in the moderate quality studies (Hedges’ g = 0.147, 95% CIs [0.037, 0.257], Z = 2.629, p = .009), smaller in the weak quality studies (Hedges’ g = 0.115, 95% CIs [0.038, 0.193], Z = 2.193, p = .004) and smallest in the high quality studies (Hedges’ g = 0.039, 95% CIs [0.007, 0.071], Z = 2.371, p = .018). However, there were no significant differences in effect sizes based on study quality categories (strong versus weak, Q(1) = 3.183, p = .074; strong versus moderate, Q(1) = 3.449, p = .063; moderate versus weak, Q(1) = 0.217, p = .642).
The moderating effect of type of stress measurement was investigated using subgroup analyses. Overall, the type of stress measurement used (i.e., perceived vs induced) did not moderate the association between stress and eating behaviours, Q(1) = 0.621, p = .431.
Finally, the moderating effect of total sample size was assessed for all studies included in the review. The meta-regression indicated that total sample size did not moderate the association between stress and food intake overall, coefficient < −0.001, standard error <.001, Z = −0.42, p = .673.
Stress and type of food intake
The relationship between stress and food consumption was further investigated using unhealthy and healthy eating categories. Overall, there was a significant difference in effect sizes based on type of food intake, Q(2) = 41.239, p < .001. Analyses indicated a significant difference between unhealthy and healthy eating, Q(1) = 24.370, p < .001, where the effect sizes were significant and positive for the stress-unhealthy food consumption relationship, but significant and negative for the stress-healthy food intake relationship (). Analyses also indicated a significant difference between healthy and other food consumption, Q(1) = 34.757, p < .001, where the effect size was significant and positive for the stress-other food consumption relationship but significant and negative for the stress-healthy food intake relationship. No differences were found between unhealthy and other food intake, Q(1) = 1.165, p = .280 (). Next we explored the effects of stress in unhealthy eating and then in healthy eating. However, as noted earlier, the other food intake outcome was not used in moderation analyses due to the ambiguity of foods included in this categorisation.
Stress and unhealthy eating outcomes
Analyses indicated a significant, positive association between stress and consumption of unhealthy foods, Hedges’ g = 0.116, 95% CIs [0.055, 0.177], Z = 3.708, p < .001 (see for proportional forest plot of stress and unhealthy food consumption). There was significant heterogeneity between studies with measures of unhealthy food intake, Q(35) = 415.910, p < .001, I2 = 91.825.
Figure 5. Proportional forest plot of stress and consumption of unhealthy foods (k = 35).
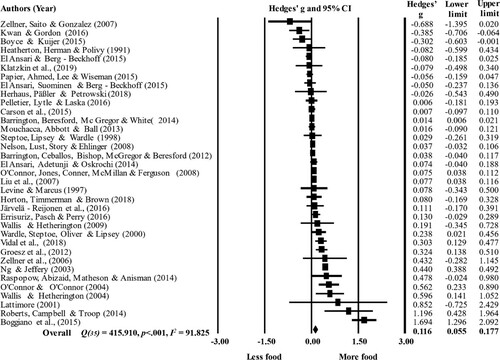
Next, analyses were conducted to determine the potential effect of moderators (see for a summary of heterogeneity for categorical subgroups) on the stress-unhealthy eating relationship. Analyses indicated no moderating effects of gender, Q(1) = 0.683, p = .408, or the proportion of females, coefficient = 0.003, standard error = 0.003, Z = 1.27, p = .202 on the relationship between stress and unhealthy eating.
Table 3. Summary of heterogeneity within and between studies on stress and unhealthy (k = 35) and healthy eating behaviours (k = 17).
Furthermore, no moderating effects were found for BMI, coefficient = −0.011, standard error = 0.028, Z = −0.39, p = .709, proportion of healthy weight, coefficient = −0.001, standard error = 0.001, Z = −1.16, p = .248, or proportion of overweight, coefficient < −0.001, standard error = 0.001, Z = −0.25, p = .806, on the stress-unhealthy eating relationship.
Six studies were included in moderation analyses to investigate the effect of restraint on the stress-unhealthy eating relationship. Mean restraint was found to significantly moderate stress and unhealthy eating, coefficient = −0.181, standard error = 0.080, Z = −2.28, p = .023. More restraint was associated with a weakening of the stress-unhealthy eating relationship.
Mean age did not moderate the association between stress and unhealthy food consumption, coefficient = 0.003, standard error = 0.007, Z = 0.41, p = .682.
Only three studies used a measure of unhealthy eating and was strong in study quality. Therefore, subgroup analyses were conducted to investigate differences in moderate and weak study quality only. Analyses indicated no moderating effect of study quality, Q(2) = 3.388, p = .184, or type of stress measure, Q(1) = 0.232, p = .630 on the stress-unhealthy eating relationship.
Similarly, sample size did not moderate the association between stress and unhealthy eating, coefficient < −0.001, standard error <.001, Z = −0.35, p = .726.
Stress and healthy eating outcomes
A significant, negative association was found between stress and healthy food consumption, Hedges’ g = −0.111, 95% CIs [−0.165, −0.056], Z = −3.981, p < .001 (see for a proportional forest plot). Further analyses indicated that there was significant heterogeneity between studies with measures of healthy food intake, Q(16) = 136.199, p < .001, I2 = 88.252.
Figure 6. Proportional forest plot of stress and consumption of healthy foods (k = 17).
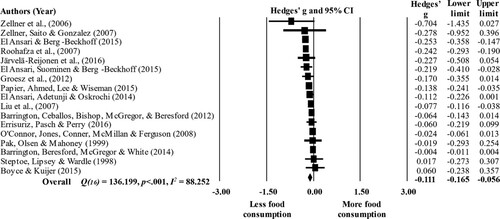
Moderating analyses were conducted to further investigate the effect of stress on healthy food consumption (see for a summary of heterogeneity across categorical subgroups). Similar to the effects for unhealthy eating outcomes, neither gender, Q(1) = 2.318, p = .128, nor proportion of females, coefficient = −0.002, standard error = 0.002, Z = −0.87, p = .387 was found to moderate the stress-healthy eating relationship.
Furthermore, no moderating effects were found for BMI, coefficient = −0.009, standard error = 0.010, Z = −0.88, p = .378, proportion of healthy weight, coefficient = −0.004, standard error = 0.002, Z = −1.96, p = .050, or proportion of overweight, coefficient = 0.009, standard error = 0.005, Z = 1.61, p = .107, on the stress-healthy eating relationship.
Moderation analysis for the effect of mean restraint on stress and healthy food was not conducted as only one study had reported mean restraint and measured an intake of healthy food.
Mean age did not moderate the association between stress and healthy food consumption, coefficient = 0.001, standard error = 0.003, Z = 0.33, p = .740.
Only one study used a measure of healthy eating and was strong in study quality. Therefore, subgroup analyses were conducted to investigate differences in moderate and weak study quality only. No differences between studies rated as moderate and weak in study quality, Q(1) = 0.035, p = .851 was found in relation to the stress-healthy eating relationship.
Moderation analysis for the type of stress measurement was not conducted as only two studies had used a stress induction methodology along with an intake of healthy food. Similarly, sample size did not moderate the association between stress and healthy eating, coefficient <0.001, standard error <.001, Z = 1.51, p = .130.
Discussion
The findings of this meta-analysis revealed for the first time that across the existing body of research that met our criteria the strength of the relationship between stress and overall food consumption was small in magnitude. These results are in line with previous narrative literature reviews which have indicated that food consumption changes as a function of stress in different individuals (Araiza & Lobel, Citation2018; Greeno & Wing, Citation1994; Lyzwinski et al., Citation2018). Moreover, the small overall effect size is also consistent with estimations that 35–40% of people increase their food intake when experiencing stress while others decrease or do not change their food intake (O’Connor & Conner, Citation2011; Oliver & Wardle, Citation1999; Pool et al., Citation2015; Sproesser et al., Citation2014). In addition, although the effect sizes are small, they are still noteworthy as they show that stress impacts on healthy and unhealthy food consumption differently. A large number of previous studies have focused on only one aspect of eating behaviour (e.g., between-meal snacking) or have been restricted to laboratory investigations of food intake in artificial environments (e.g., chocolate consumption in ad-libitum laboratory experiments). Therefore, the current findings emphasise the need to consider different aspects of eating behaviour and may indicate that disparate findings observed in past research may be, in part, accounted for by the variations in the type of eating behaviour and the environment in which it occurs (e.g., between-meal snacking, ad-libitum food intake). Nevertheless, the small effect sizes also suggest that stress-induced eating may not be such a major health concern in psychologically healthy non-disordered eaters as once thought. That said, as outlined below, drawing such a conclusion may be premature given the paucity of research that has carefully examined putative moderators of the stress-eating relationship (e.g., eating style, dispositional stress-related eating).
A secondary aim of this meta-analysis was to investigate the influence of two groups of moderating variables: individual differences (i.e., gender, weight, dietary restraint and age) and study specific characteristics (i.e., study quality, type of stress measure and sample size). Surprisingly, dietary restraint was found to be the only significant moderator, such that greater levels of restraint were associated with a weakening of the stress-unhealthy eating relationship. This is contrary to reported effects of restraint on the stress-eating relationship, where stress generally increases eating in people who are higher in dietary restraint compared to unrestrained eaters (Adriaanse et al., Citation2011; O'Connor et al., Citation2008; Torres & Nowson, Citation2007; Wallis & Hetherington, Citation2004). Whilst this finding is interesting, only 6 studies were included in the meta-regression for mean restraint (for the sample) on stress and unhealthy food consumption. This moderating effect may also be confounded by the quality of the data used in the present meta-analysis. Mean restraint scores were used for whole samples and standardised to account for differences in measurement methods for dietary restraint. As such, conclusions drawn from our analyses are difficult to compare to previous literature without the use of raw (individual level) data. Therefore, undue emphasis should not be placed on the findings of this moderating variable in this meta-analysis and, as such, should be interpreted with caution.
Taken together, the limited number of significant moderators identified here was unexpected given the findings of other narrative reviews and key studies in this area (e.g., Araiza & Lobel, Citation2018; Greeno & Wing, Citation1994; Lyzwinski et al., Citation2018; O’Connor & Conner, Citation2011). We recognise that some of the null effects may be explained by having relatively small numbers of studies in some of the subgroup analyses (e.g., for males k = 9). However, this was the exception not the rule. An alternative explanation is that the considerable unexplained heterogeneity in the stress-eating relationship is accounted for by important variables that we were unable to include in the review due to lack of studies and/or the details were not included in studies (e.g., emotional eating style, dispositional stress-related eating, cortisol reactivity, type of stressor).
It is clear that the effects of stress on eating behaviour are hugely complex. As indicated above, there is evidence emerging highlighting the role of dispositional factors or individual differences in stress-related eating that were not accounted for in the current review and which likely obscured the true magnitude of the stress-eating relationship (e.g., emotional eating scores, self-reported stress eater status). However, we found only a small number of studies that included sufficient data and as a result, we were unable to conduct any meaningful analyses on dispositional factors or individual differences in stress-related eating despite these being important factors in the stress-eating relationship. For example, Torres and Nowson (Citation2007) make the important distinction between under- and over-eating in response to stress and highlight the differing effects of stress-eating depending on factors such as the severity of the stressor. As such, the potential insights into stress-eating are limited in the present review due to the aggregation across these different types of stress-eating responders. In addition, it remains unknown the extent to which stress can induce increases in unhealthy and healthy eating within the same individual (i.e., is there a global increase in stress-related eating?) or whether stress triggers a switching from healthy to unhealthy eating within individuals or whether any dispositional or learned effects are limited to specific foods (e.g., unhealthy foods, snacks etc.). Consequently, we feel future research should explore the effects of dispositional factors in the stress-eating relationship and establish the approximate percentage of individuals who exhibit an increase, a decrease or no change in eating response to stress. In addition, individual differences in cortisol reactivity to stress have also been found to influence eating behaviours in adults and children and should be investigated further (Epel et al., Citation2001; Moss et al., Citation2020; Newman et al., Citation2007).
The considerable heterogeneity found across analyses may also be explained through individual differences in the evaluation and type of stressor experienced, which has previously been found to influence stress-related eating behaviours (Miller et al., Citation2007). For example, research has found that the severity of a stressor is more predictive of eating behaviours than merely whether one is experienced (Adam & Epel, Citation2007), although this is not consistently reported in previous research (Conner et al., Citation1999). Similarly, differences in food consumption exist between acute and chronic stress, where acutely experienced stress has been associated with inhibited appetite (Sominsky & Spencer, Citation2014) while chronically occurring stress has been linked with both increased (Tryon et al., Citation2013) and decreased food consumption, as well as weight changes (Dallman et al., Citation2003; Klatzkin et al., Citation2018). The type of stressor can also have a differential influence on stress-related eating behaviours. Ego-threatening stressors (O'Connor et al., Citation2008) and those with social evaluation (such as stress-induction paradigms) elicit much stronger stress responses and may be more likely to result in changes to normal eating behaviours (Dickerson & Kemeny, Citation2004). In contrast, O'Connor et al. (Citation2008) found that stressors that were physical in nature (e.g., anxious/frightened, feeling ill, threat of attack by a dog) were associated with a reduction in between-meal snacking. Moreover, it is worth noting that few studies in this meta-analysis considered situational factors around the experience of stress (e.g., type of stressor, perceived intensity), which may have provided greater insights into stress-related eating than merely the occurrence of stress.
Limitations
While the meta-analysis provides insights into the stress-eating relationship, there are limitations with the methodology which ought to be acknowledged. The conceptualisation of stress in the present review aimed to improve the specificity of the findings and ultimately the synthesis of data from studies where stress was clearly linked with an eating behaviour. To achieve this, a distinction was made between stress (defined as any noxious event or episode in one’s environment that could be appraised as threatening, risky or harmful) and psychological states (such as emotional distress and negative affect) which were considered to be responses to a stressor. This approach helped refine the scope of the review; however, we recognise that such refinement may have limited the generalisability of the current findings to inform the broader literature that has investigated the effects of emotions and emotional distress on eating. Moreover, it is important that researchers do not underestimate the influence of positive, as well as negative emotions, on eating behaviour (e.g., Evers et al., Citation2018; Moss et al., Citation2021).
Consequently, this differentiation between stress and other psychological states may limit the potential scope of the current review, specifically the omission of studies which consider emotional distress/anxiety/negative affect to be synonymous with stress. The definition of stress varies greatly within the literature and remains a subject of contention (Kagan, Citation2016; O’Connor et al., Citation2021). Future research should take care to clearly define stress in an effort to disentangle conceptualisations of stress, responses to stress and explore the extent to which food consumption is triggered by positive and negative emotional arousal. In addition, whilst attempts were made to include a wide variety of moderating variables of the stress and eating relationship, the range of moderators included in the present review was limited. This was mostly dictated by the availability of data reported in the studies, nevertheless, we are aware that as a result, the review does not report or test an exhaustive list of potential moderators of eating behaviours under conditions of stress.
Similar to a recent meta-analysis on emotions and eating (Evers et al., Citation2018), the present meta-analysis aimed to determine the impact of stress on overall food consumption. To understand this relationship further, food types were categorised into unhealthy, healthy, and other foods based on energy density and nutrient profiles. Although this method has provided useful insights into the differential effect between the types of foods consumed under stress, it does not consider the influence of food palatability on the stress-eating relationship. Under conditions of stress, highly palatable foods may be perceived as more rewarding which in turn increases the salience of these foods (Nieuwenhuizen & Rutters, Citation2008; Sominsky & Spencer, Citation2014). As such, consumption of palatable foods (regardless of their nutritional content) may attenuate the physiological effects of acute stress (Morris et al., Citation2015).
Based on the findings from this meta-analysis, there are several recommendations which should be considered in future stress and eating research generally, and specifically to address the unexplained heterogeneity identified in this review. First, studies should include more detailed measures of the nature of the stressors under consideration (e.g., acute, chronic, physical, ego-threatening etc.) and more accurate assessments of food consumption (calorie count, energy density, palatability). Inclusion of more detailed measures of food consumption, such as total energy intake will facilitate greater insights into outcomes of the stress-eating relationship such as body weight. Second, more studies are required that test key moderating variables on stress and eating habits. Although efforts were made in the current review to investigate potential moderators, instances of these being included in studies and the data reported were limited, making it difficult to obtain meaningful data on some of the potential moderators of interest. Third, researchers should routinely include measures of eating styles such as emotional eating, dietary restraint, disinhibition and external eating. Fourth, all studies should endeavour to capture accurate assessments of weight and height and diet status. Finally, studies should improve reporting practices and make study data freely available so that findings can be synthesised more accurately in meta-analyses such as this one (cf., Norris & O’Connor, Citation2019).
Conclusion
Stress is associated with decreased intake of healthy foods, and increased intake of unhealthy foods; however, the magnitude of these effects is small. With the exception of dietary restraint, effect sizes were not influenced by the moderating variables included in the current meta-analysis, although the limited range of such moderators examined is worth noting. This review has highlighted the need for future research to consider factors which may account for the large proportion of unexplained heterogeneity observed in this meta-analysis.
Author contributions
DH, DOC, MC and MB identified the gap in the literature and developed a search strategy for this review. DH carried out literature searching, collation of identified papers and screening. RM/SW independently screened articles and double coded study quality for inter-rater agreement. DH extracted data and FC double coded all data prior to analyses. DH conducted analyses with advice from DOC and MC. DH, DOC, MC and MB wrote this manuscript. All authors checked the final version of this review and are happy to be accountable for this piece.
Supplemental Material
Download MS Word (65.1 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adam, T. C., & Epel, E. S. (2007). Stress, eating and the reward system. Physiology and Behavior, 91(4), 449–458. https://doi.org/https://doi.org/10.1016/j.physbeh.2007.04.011
- Adriaanse, M. A., de Ridder, D. T., & Evers, C. (2011). Emotional eating: Eating when emotional or emotional about eating? Psychology and Health, 26(1), 23–39. https://doi.org/https://doi.org/10.1080/08870440903207627
- Algren, M. H., Ekholm, O., Nielsen, L., Ersbøll, A. K., Bak, C. K., & Andersen, P. T. (2018). Associations between perceived stress, socioeconomic status, and health-risk behaviour in deprived neighbourhoods in Denmark: A cross-sectional study. BMC Public Health, 18(1), 250. https://doi.org/https://doi.org/10.1186/s12889-018-5170-x
- Appelhans, B. M. (2010). Circulating leptin moderates the effect of stress on snack intake independent of body mass. Eating Behaviors, 11(3), 152–155. https://doi.org/https://doi.org/10.1016/j.eatbeh.2010.01.004
- Araiza, A. M., & Lobel, M. (2018). Stress and eating: Definitions, findings, explanations, and implications. Social and Personality Psychology Compass, 12(4), e12378. https://doi.org/https://doi.org/10.1111/spc3.12378
- Barker, M. E., Blain, R. J., & Russell, J. M. (2015). The influence of academic examinations on energy and nutrient intake in male university students. Nutrition Journal, 14(1), 98. https://doi.org/https://doi.org/10.1186/s12937-015-0088-y
- Barrington, W. E., Beresford, S. A., McGregor, B. A., & White, E. (2014). Perceived stress and eating behaviors by sex, obesity status, and stress vulnerability: Findings from the vitamins and lifestyle (VITAL) study. Journal of the Academy of Nutrition and Dietetics, 114(11), 1791–1799. https://doi.org/https://doi.org/10.1016/j.jand.2014.03.015
- Barrington, W. E., Ceballos, R. M., Bishop, S. K., McGregor, B. A., & Beresford, S. A. (2012). Perceived stress, behavior, and body mass index among adults participating in a worksite obesity prevention program, Seattle, 2005–2007. Preventing Chronic Disease, 9, E152. https://doi.org/https://doi.org/10.5888/pcd9.120001
- Boggiano, M. M., Wenger, L. E., Turan, B., Tatum, M. M., Sylvester, M. D., Morgan, P. R., Morse, K. E., & Burgess, E. E. (2015). Real-time sampling of reasons for hedonic food consumption: Further validation of the palatable eating motives scale. Frontiers in Psychology, 6, 1–8. https://doi.org/https://doi.org/10.3389/fpsyg.2015.00744
- Borenstein, M., Hedges, L., Higgins, J., & Rothstein, H. (2005). Comprehensive meta-analysis version 2. Biostat. 104.
- Boyce, J. A., & Kuijer, R. G. (2015). Perceived stress and freshman weight change: The moderating role of baseline body mass index. Physiology and Behavior, 139, 491–496. https://doi.org/https://doi.org/10.1016/j.physbeh.2014.12.011
- Carson, T. L., Desmond, R., Hardy, S., Townsend, S. N., Ard, J. D., Meneses, K., Partridge, E. E., & Baskin, M. L. (2015). A study of the relationship between food group recommendations and perceived stress: Findings from black women in the deep south. Journal of Obesity, 2015, 1–7. https://doi.org/https://doi.org/10.1155/2015/203164
- Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 20(1), 37–46. https://doi.org/https://doi.org/10.1177/001316446002000104
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Lawrence Erlbaum Associates.
- Cohen, S., Janicki-Deverts, D., Doyle, W. J., Miller, G. E., Frank, E., Rabin, B. S., & Turner, R. B. (2012). Chronic stress, glucocorticoid receptor resistance, inflammation, and disease risk. Proceedings of the National Academy of Sciences, 109(16), 5995–5999. https://doi.org/https://doi.org/10.1073/pnas.1118355109
- Cohen, S., Janicki-Deverts, D., & Miller, G. E. (2007). Psychological stress and disease. JAMA, 298(14), 1685–1687. https://doi.org/https://doi.org/10.1001/jama.298.14.1685
- Conner, M., Fitter, M., & Fletcher, W. (1999). Stress and snacking: A diary study of daily hassles and between-meal snacking. Psychology and Health, 14(1), 51–63. https://doi.org/https://doi.org/10.1080/08870449908407313
- Cotter, E. W., & Kelly, N. R. (2018). Stress-related eating, mindfulness, and obesity. Health Psychology, 37(6), 516–525. https://doi.org/https://doi.org/10.1037/hea0000614
- Cottone, P., Sabino, V., Roberto, M., Bajo, M., Pockros, L., Frihauf, J. B., Fekete, E. M., Steardo, L., Rice, K. C., Grigoriadis, D. E., Conti, B., Koob, G. F., & Zorrilla, E. P. (2009). CRF system recruitment mediates dark side of compulsive eating. Proceedings of the National Academy of Sciences, 106(47), 20016–20020. https://doi.org/https://doi.org/10.1073/pnas.0908789106
- Crawford, J. R., & Henry, J. D. (2004). The positive and negative affect schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 43(3), 245–265. https://doi.org/https://doi.org/10.1348/0144665031752934
- Crowther, J. H., Sanftner, J., Bonifazi, D. Z., & Shepherd, K. L. (2001). The role of daily hassles in binge eating. International Journal of Eating Disorders, 29(4), 449–454. https://doi.org/https://doi.org/10.1002/eat.1041
- Dallman, M. F., Pecoraro, N., Akana, S. F., La Fleur, S. E., Gomez, F., Houshyar, H., Bell, M. E., Bhatnagar, S., Laugero, K. D., & Manalo, S. (2003). Chronic stress and obesity: A new view of “comfort food”. Proceedings of the National Academy of Sciences, 100(20), 11696–11701. https://doi.org/https://doi.org/10.1073/pnas.1934666100
- Dickerson, S. S., & Kemeny, M. E. (2004). Acute stressors and cortisol responses: A theoretical integration and synthesis of laboratory research. Psychological Bulletin, 130(3), 355–391. https://doi.org/https://doi.org/10.1037/0033-2909.130.3.355
- Duval, S., & Tweedie, R. (2000). Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56(2), 455–463. https://doi.org/https://doi.org/10.1111/j.0006-341X.2000.00455.x
- Dweck, J. S., Jenkins, S. M., & Nolan, L. J. (2014). The role of emotional eating and stress in the influence of short sleep on food consumption. Appetite, 72, 106–113. https://doi.org/https://doi.org/10.1016/j.appet.2013.10.001
- Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. British Medical Journal, 315(7109), 629–634. https://doi.org/https://doi.org/10.1136/bmj.315.7109.629
- El Ansari, W., Adetunji, H., & Oskrochi, R. (2014). Food and mental health: Relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Central European Journal of Public Health, 22(2), 90–97. https://doi.org/https://doi.org/10.21101/cejph.a3941
- El Ansari, W., & Berg-Beckhoff, G. (2015). Nutritional correlates of perceived stress among university students in Egypt. International Journal of Environmental Research and Public Health, 12(11), 14164–14176. https://doi.org/https://doi.org/10.3390/ijerph121114164
- El Ansari, W., Suominen, S., & Berg-Beckhoff, G. (2015). Mood and food at the university of Turku in Finland: Nutritional correlates of perceived stress are most pronounced among overweight students. International Journal of Public Health, 60(6), 707–716. https://doi.org/https://doi.org/10.1007/s00038-015-0717-4
- Epel, E., Lapidus, R., McEwen, B., & Brownell, K. (2001). Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology, 26(1), 37–49. https://doi.org/https://doi.org/10.1016/S0306-4530(00)00035-4
- Errisuriz, V. L., Pasch, K. E., & Perry, C. L. (2016). Perceived stress and dietary choices: The moderating role of stress management. Eating Behaviors, 22, 211–216. https://doi.org/https://doi.org/10.1016/j.eatbeh.2016.06.008
- Evers, C., Dingemans, A., Junghans, A. F., & Boevé, A. (2018). Feeling bad or feeling good, does emotion affect your consumption of food? A meta-analysis of the experimental evidence. Neuroscience and Biobehavioral Reviews, 92, 195–208. https://doi.org/https://doi.org/10.1016/j.neubiorev.2018.05.028
- Finch, L. E., Tiongco-Hofschneider, L., & Tomiyama, A. J. (2019). Stress-induced eating dampens physiological and behavioral stress responses. In R. R. Watson (Ed.), Nutrition in the prevention and treatment of abdominal obesity (pp. 175–187). Elsevier. https://doi.org/https://doi.org/10.1016/B978-0-12-816093-0.00015-X
- Gibson, E. L. (2012). The psychobiology of comfort eating: Implications for neuropharmacological interventions. Behavioural Pharmacology, 23(5 6), 442–460. https://doi.org/https://doi.org/10.1097/FBP.0b013e328357bd4e
- Greeno, C. G., & Wing, R. R. (1994). Stress-induced eating. Psychological Bulletin, 115(3), 444–464. https://doi.org/https://doi.org/10.1037/0033-2909.115.3.444
- Groesz, L. M., McCoy, S., Carl, J., Saslow, L., Stewart, J., Adler, N., Laraia, B., & Epel, E. (2012). What is eating you? Stress and the drive to eat. Appetite, 58(2), 717–721. https://doi.org/https://doi.org/10.1016/j.appet.2011.11.028
- Habhab, S., Sheldon, J. P., & Loeb, R. C. (2009). The relationship between stress, dietary restraint, and food preferences in women. Appetite, 52(2), 437–444. https://doi.org/https://doi.org/10.1016/j.appet.2008.12.006
- Heatherton, T. F., Herman, C. P., & Polivy, J. (1991). Effects of physical threat and ego threat on eating behavior. Journal of Personality and Social Psychology, 60(1), 138–143. https://doi.org/https://doi.org/10.1037/0022-3514.60.1.138
- Herhaus, B., Päßler, S., & Petrowski, K. (2018). Stress-related laboratory eating behavior in adults with obesity and healthy weight. Physiology and Behavior, 196, 150–157. https://doi.org/https://doi.org/10.1016/j.physbeh.2018.08.018
- Higgins, J. P., & Green, S. (2011). Cochrane handbook for systematic reviews of interventions (H. JPT & G. S Eds. 5.1.0 ed.). The Cochrane Collaboration.
- Higgins, J. P., & Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21(11), 1539–1558. https://doi.org/https://doi.org/10.1002/sim.1186
- Higgins, J. P., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ, 327(7414), 557–560. https://doi.org/https://doi.org/10.1136/bmj.327.7414.557
- Hill, D. C., Moss, R. H., Sykes-Muskett, B., Conner, M., & O'Connor, D. B. (2018). Stress and eating behaviors in children and adolescents: Systematic review and meta-analysis. Appetite, 123, 14–22. https://doi.org/https://doi.org/10.1016/j.appet.2017.11.109
- Horton, S. E., Timmerman, G. M., & Brown, A. (2018). Factors influencing dietary fat intake among black emerging adults. Journal of American College Health, 66(3), 155–164. https://doi.org/https://doi.org/10.1080/07448481.2017.1390669
- Hoyt, W. T., & Del Re, A. C. (2015). Comparison of methods for aggregating dependent effect sizes in meta-analysis. Manuscript under review.
- Järvelä-Reijonen, E., Karhunen, L., Sairanen, E., Rantala, S., Laitinen, J., Puttonen, S., Peuhkuri, K., Hallikainen, M., Juvonen, K., Myllymäki, T., Föhr, T., Pihlajamäki, J., Korpela, R., Ermes, M., Lappalainen, R., & Kolehmainen, M. (2016). High perceived stress is associated with unfavorable eating behavior in overweight and obese Finns of working age. Appetite, 103, 249–258. https://doi.org/https://doi.org/10.1016/j.appet.2016.04.023
- Kagan, J. (2016). An overly permissive extension. Perspectives on Psychological Science, 11(4), 442–450. https://doi.org/https://doi.org/10.1177/1745691616635593
- Kasl, S. V., & Cooper, C. L. (1987). Stress and health: Issues in research methodology. John Wiley and Sons.
- Kirschbaum, C., Pirke, K.-M., & Hellhammer, D. H. (1993). The ‘Trier social stress test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1-2), 76–81. https://doi.org/https://doi.org/10.1159/000119004
- Klatzkin, R. R., Baldassaro, A., & Hayden, E. (2018). The impact of chronic stress on the predictors of acute stress-induced eating in women. Appetite, 123, 343–351. https://doi.org/https://doi.org/10.1016/j.appet.2018.01.007
- Klatzkin, R. R., Dasani, R., Warren, M., Cattaneo, C., Nadel, T., Nikodem, C., & Kissileff, H. R. (2019). Negative affect is associated with increased stress-eating for women with high perceived life stress. Physiology and Behavior, 210, 112639. https://doi.org/https://doi.org/10.1016/j.physbeh.2019.112639
- Kwan, M. Y., & Gordon, K. H. (2016). The effects of social support and stress perception on bulimic behaviors and unhealthy food consumption. Eating Behaviors, 22, 34–39. https://doi.org/https://doi.org/10.1016/j.eatbeh.2016.03.024
- Lai, Z., Why, Y. P., Koh, D. S. Q., Ng, V. A. C., & Lim, C. L. (2012). Body fat fluctuations among female adolescents with restrained eating behaviours. Appetite, 59(1), 17–20. https://doi.org/https://doi.org/10.1016/j.appet.2012.03.017
- Lattimore, P. (2001). Stress-induced eating: An alternative method for inducing ego-threatening stress. Appetite, 36(2), 187–188. https://doi.org/https://doi.org/10.1006/appe.2000.0387
- Lazarus, R. S. (1999). Stress and emotion: A new synthesis. Springer.
- Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. Springer.
- Lemmens, S. G., Rutters, F., Born, J. M., & Westerterp-Plantenga, M. S. (2011). Stress augments food ‘wanting’and energy intake in visceral overweight subjects in the absence of hunger. Physiology and Behavior, 103(2), 157–163. https://doi.org/https://doi.org/10.1016/j.physbeh.2011.01.009
- Levine, M. D., & Marcus, M. D. (1997). Eating behavior following stress in women with and without bulimic symptoms. Annals of Behavioral Medicine, 19(2), 132–138. https://doi.org/https://doi.org/10.1007/BF02883330
- Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis (Vol. 49). Sage Publications, Inc.
- Liu, C., Xie, B., Chou, C.-P., Koprowski, C., Zhou, D., Palmer, P., Sun, P., Guo, Q., Duan, L., Sun, X., & Anderson, J. C. (2007). Perceived stress, depression and food consumption frequency in the college students of China seven cities. Physiology and Behavior, 92(4), 748–754. https://doi.org/https://doi.org/10.1016/j.physbeh.2007.05.068
- Lyzwinski, L. N., Caffery, L., Bambling, M., & Edirippulige, S. (2018). The relationship between stress and maladaptive weight-related behaviors in college students: A review of the literature. American Journal of Health Education, 49(3), 166–178. https://doi.org/https://doi.org/10.1080/19325037.2018.1449683
- Mikolajczyk, R. T., El Ansari, W., & Maxwell, A. E. (2009). Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutrition Journal, 8(1), 1–8. https://doi.org/https://doi.org/10.1186/1475-2891-8-31
- Miller, G. E., Chen, E., & Zhou, E. S. (2007). If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychological Bulletin, 133(1), 25–45. https://doi.org/https://doi.org/10.1037/0033-2909.133.1.25
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269. https://doi.org/https://doi.org/10.7326/0003-4819-151-4-200908180-00135
- Morera, L. P. P., Marchiori, G. N., Medrano, L. A., & Defagó, M. D. (2019). Stress, dietary patterns and cardiovascular disease: A mini-review. Frontiers in Neuroscience, 13, 1226. https://doi.org/https://doi.org/10.3389/fnins.2019.01226
- Morris, M. J., Beilharz, J. E., Maniam, J., Reichelt, A. C., & Westbrook, R. F. (2015). Why is obesity such a problem in the 21st century? The intersection of palatable food, cues and reward pathways, stress, and cognition. Neuroscience and Biobehavioral Reviews, 58, 36–45. https://doi.org/https://doi.org/10.1016/j.neubiorev.2014.12.002
- Moss, R. H., Conner, M., & O’Connor, D. B. (2020). Exploring the effects of daily hassles on eating behaviour in children: The role of cortisol reactivity. Psychoneuroendocrinology, 117, 104692. https://doi.org/https://doi.org/10.1016/j.psyneuen.2020.104692
- Moss, R. H., Conner, M., & O’Connor, D. B. (2021). Exploring the effects of positive and negative emotions on eating behaviours in children and young adults. Psychology, Health & Medicine, 26, 457–466. https://doi.org/https://doi.org/10.1080/13548506.2020.1761553
- Mouchacca, J., Abbott, G. R., & Ball, K. (2013). Associations between psychological stress, eating, physical activity, sedentary behaviours and body weight among women: A longitudinal study. BMC Public Health, 13(1), 828. https://doi.org/https://doi.org/10.1186/1471-2458-13-828
- Nelson, M. C., Lust, K., Story, M., & Ehlinger, E. (2008). Credit card debt, stress and key health risk behaviors among college students. American Journal of Health Promotion, 22(6), 400–406. https://doi.org/https://doi.org/10.4278/ajhp.22.6.400
- Neuendorf, K. A. (2016). The content analysis guidebook. Sage.
- Newman, E., O’Connor, D. B., & Conner, M. (2007). Daily hassles and eating behaviour: The role of cortisol reactivity status. Psychoneuroendocrinology, 32(2), 125–132. https://doi.org/https://doi.org/10.1016/j.psyneuen.2006.11.006
- Ng, D. M., & Jeffery, R. W. (2003). Relationships between perceived stress and health behaviors in a sample of working adults. Health Psychology, 22(6), 638–642. https://doi.org/https://doi.org/10.1037/0278-6133.22.6.638
- Nieuwenhuizen, A. G., & Rutters, F. (2008). The hypothalamic-pituitary-adrenal-axis in the regulation of energy balance. Physiology and Behavior, 94(2), 169–177. https://doi.org/https://doi.org/10.1016/j.physbeh.2007.12.011
- Norris, E., & O’Connor, D. B. (2019). Science as behaviour: Using a behaviour change approach to increase uptake of Open Science. Psychology and Health, 34(12), 1397–1406. https://doi.org/https://doi.org/10.1080/08870446.2019.1679373
- O’Connor, D. B. (2018). Effects of stress and cortisol on eating behaviour in children and adolescents. In P. Murphy (Ed.), The Routledge international handbook of psychobiology (pp. 179–193). Routledge.
- O’Connor, D. B., & Conner, M. (2011). Effects of stress on eating behavior. In R. J. Contrada & A. Baum (Eds.), The handbook of stress science: Biology, psychology, and health (pp. 275–286). Springer Publishing Company.
- O'Connor, D. B., Conner, M., Jones, F., McMillan, B., & Ferguson, E. (2009). Exploring the benefits of conscientiousness: An investigation of the role of daily stressors and health behaviors. Annals of Behavioral Medicine, 37(2), 184–196. https://doi.org/https://doi.org/10.1007/s12160-009-9087-6
- O’Connor, D. B., & Ferguson, E. (2016). Stress and stressors. In Y. Benyamini, M. Johnston, & E. C. Karademas (Eds.), Assessment in health psychology (pp. 104–118). Hogrefe. 978-0889374522.
- O'Connor, D. B., Jones, F., Conner, M., McMillan, B., & Ferguson, E. (2008). Effects of daily hassles and eating style on eating behavior. Health Psychology, 27(1, Suppl), S20–S31. https://doi.org/https://doi.org/10.1037/0278-6133.27.1.S20
- O'Connor, D. B., & O'Connor, R. C. (2004). Perceived changes in food intake in response to stress: The role of conscientiousness. Stress and Health, 20(5), 279–291. https://doi.org/https://doi.org/10.1002/smi.1028
- O’Connor, D. B., Thayer, J. T., & Vedhara, K. (2021). Stress and health: A review of psychobiological processes. Annual Review of Psychology, 72(1), 663–688. https://doi.org/https://doi.org/10.1146/annurev-psych-062520-122331
- Oliver, G., & Wardle, J. (1999). Perceived effects of stress on food choice. Physiology and Behavior, 66(3), 511–515. https://doi.org/https://doi.org/10.1016/S0031-9384(98)00322-9
- Oliver, G., Wardle, J., & Gibson, E. L. (2000). Stress and food choice: A laboratory study. Psychosomatic Medicine, 62(6), 853–865. https://doi.org/https://doi.org/10.1097/00006842-200011000-00016
- Orwin, R. G. (1983). A fail-safe N for effect size in meta-analysis. Journal of Educational Statistics, 8, 157–159. https://doi.org/https://doi.org/10.3102/10769986008002157
- Pak, S.-H. K., Olsen, L. K., & Mahoney, B. S. (1999). The relationships of health behaviors to perceived stress, job satisfaction, and role modeling among health professionals in South Korea. International Quarterly of Community Health Education, 19(1), 65–76. https://doi.org/https://doi.org/10.2190/ux7n-h2mr-7bhk-513a
- Papier, K., Ahmed, F., Lee, P., & Wiseman, J. (2015). Stress and dietary behaviour among first-year university students in Australia: Sex differences. Nutrition, 31(2), 324–330. https://doi.org/https://doi.org/10.1016/j.nut.2014.08.004
- Pelletier, J. E., Lytle, L. A., & Laska, M. N. (2016). Stress, health risk behaviors, and weight status among community college students. Health Education and Behavior, 43(2), 139–144. https://doi.org/https://doi.org/10.1177/1090198115598983
- Pollard, T. M., Steptoe, A., Canaan, L., Davies, G. J., & Wardle, J. (1995). Effects of academic examination stress on eating behavior and blood lipid levels. International Journal of Behavioral Medicine, 2(4), 299–320. https://doi.org/https://doi.org/10.1207/s15327558ijbm0204_2
- Pool, E., Delplanque, S., Coppin, G., & Sander, D. (2015). Is comfort food really comforting? Mechanisms underlying stress-induced eating. Food Research International, 76, 207–215. https://doi.org/https://doi.org/10.1016/j.foodres.2014.12.034
- Poon, T., Labonté, MÈ, Mulligan, C., Ahmed, M., Dickinson, K. M., & L’Abbé, M. R. (2018). Comparison of nutrient profiling models for assessing the nutritional quality of foods: A validation study. British Journal of Nutrition, 120(5), 567–582. https://doi.org/https://doi.org/10.1017/S0007114518001575
- Raspopow, K., Abizaid, A., Matheson, K., & Anisman, H. (2010). Psychosocial stressor effects on cortisol and ghrelin in emotional and non-emotional eaters: Influence of anger and shame. Hormones and Behavior, 58(4), 677–684. https://doi.org/https://doi.org/10.1016/j.yhbeh.2010.06.003
- Raspopow, K., Abizaid, A., Matheson, K., & Anisman, H. (2014). Anticipation of a psychosocial stressor differentially influences ghrelin, cortisol and food intake among emotional and non-emotional eaters. Appetite, 74, 35–43. https://doi.org/https://doi.org/10.1016/j.appet.2013.11.018
- Reichenberger, J., Kuppens, P., Liedlgruber, M., Wilhelm, F. H., Tiefengrabner, M., Ginzinger, S., & Blechert, J. (2018). No haste, more taste: An EMA study of the effects of stress, negative and positive emotions on eating behavior. Biological Psychology, 131, 54–62. https://doi.org/https://doi.org/10.1016/j.biopsycho.2016.09.002
- Riley, R. D., Higgins, J. P., & Deeks, J. J. (2011). Interpretation of random effects meta-analyses. BMJ, 342(feb10 2), d549. https://doi.org/https://doi.org/10.1136/bmj.d549
- Roberts, C. J., Campbell, I. C., & Troop, N. (2014). Increases in weight during chronic stress are partially associated with a switch in food choice towards increased carbohydrate and saturated fat intake. European Eating Disorders Review, 22(1), 77–82. https://doi.org/https://doi.org/10.1002/erv.2264
- Roohafza, H., Sadeghi, M., Sarraf-Zadegan, N., Baghaei, A., Kelishadi, R., Mahvash, M., Sajjadi, F., Toghianifar, N., & Talaei, M. (2007). Relation between stress and other life style factors. Stress and Health, 23(1), 23–29. https://doi.org/https://doi.org/10.1002/smi.1113
- Rutters, F., Nieuwenhuizen, A. G., Lemmens, S. G., Born, J. M., & Westerterp-Plantenga, M. S. (2009). Acute stress-related changes in eating in the absence of hunger. Obesity, 17(1), 72–77. https://doi.org/https://doi.org/10.1038/oby.2008.493
- Scott, K. M., Lim, C., Al-Hamzawi, A., Alonso, J., Bruffaerts, R., Caldas-de-Almeida, J. M., Florescu, S., de Girolamo, G., Hu, C., De Jonge, P., Kawakami, N., Medina-Mora, M. E., Moskalewicz, J., Navarro-Mateu, F., O’Neill, S., Piazza, M., Posada-Villa, J., Torres, Y., & Kessler, R. C. (2016). Association of mental disorders with subsequent chronic physical conditions: World mental health surveys from 17 countries. JAMA Psychiatry, 73(2), 150–158. https://doi.org/https://doi.org/10.1001/jamapsychiatry.2015.2688
- Segerstrom, S. C., & O’Connor, D. B. (2012). Stress, health and illness: Four challenges for the future. Psychology and Health, 27(2), 128–140. https://doi.org/https://doi.org/10.1080/08870446.2012.659516
- Sims, R., Gordon, S., Garcia, W., Clark, E., Monye, D., Callender, C., & Campbell, A. (2008). Perceived stress and eating behaviors in a community-based sample of African Americans. Eating Behaviors, 9(2), 137–142. https://doi.org/https://doi.org/10.1016/j.eatbeh.2007.06.006
- Sinha, R. (2018). Role of addiction and stress neurobiology on food intake and obesity. Biological Psychology, 131, 5–13. https://doi.org/https://doi.org/10.1016/j.biopsycho.2017.05.001
- Sinha, R., & Jastreboff, A. M. (2013). Stress as a common risk factor for obesity and addiction. Biological Psychiatry, 73(9), 827–835. https://doi.org/https://doi.org/10.1016/j.biopsych.2013.01.032
- Sominsky, L., & Spencer, S. J. (2014). Eating behavior and stress: A pathway to obesity. Frontiers in Psychology, 5, https://doi.org/https://doi.org/10.3389/fpsyg.2014.00434
- Spielberger, C. D., Gorusch, R. L., & Lushene, R. E. (1970). State-trait anxiety inventory manual. CA7 Consulting Psychologists Press, Inc.
- Spitzer, R. L., Kroenke, K., & Williams, J. B., & Patient Health Questionnaire primary care study group. (1999). Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Journal of the American Medical Association, 282(18), 1737–1744. https://doi.org/https://doi.org/10.1001/jama.282.18.1737
- Sproesser, G., Schupp, H. T., & Renner, B. (2014). The bright side of stress-induced eating: Eating more when stressed but less when pleased. Psychological Science, 25(1), 58–65. https://doi.org/https://doi.org/10.1177/0956797613494849
- Steptoe, A., & Kivimäki, M. (2012). Stress and cardiovascular disease. Nature Reviews Cardiology, 9(6), 360–370. https://doi.org/https://doi.org/10.1016/j.jacc.2007.12.024
- Steptoe, A., Lipsey, Z., & Wardle, J. (1998). Stress, hassles and variations in alcohol consumption, food choice and physical exercise: A diary study. British Journal of Health Psychology, 3(1), 51–63. https://doi.org/https://doi.org/10.1111/j.2044-8287.1998.tb00555.x
- Stone, A. A., & Brownell, K. D. (1994). The stress-eating paradox: Multiple daily measurements in adult males and females. Psychology and Health, 9(6), 425–436. https://doi.org/https://doi.org/10.1080/08870449408407469
- Thomas, B., Ciliska, D., Dobbins, M., & Micucci, S. (2004). A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews on Evidence-Based Nursing, 1(3), 176–184. https://doi.org/https://doi.org/10.1111/j.1524-475X.2004.04006.x
- Tomiyama, A. J. (2019). Stress and obesity. Annual Review of Psychology, 70(1), 703–718. https://doi.org/https://doi.org/10.1146/annurev-psych-010418-102936
- Torres, S. J., & Nowson, C. A. (2007). Relationship between stress, eating behavior, and obesity. Nutrition, 23(11-12), 887–894. https://doi.org/https://doi.org/10.1016/j.nut.2007.08.008
- Tryon, M. S., Carter, C. S., DeCant, R., & Laugero, K. D. (2013). Chronic stress exposure may affect the brain's response to high calorie food cues and predispose to obesogenic eating habits. Physiology and Behavior, 120, 233–242. https://doi.org/https://doi.org/10.1016/j.physbeh.2013.08.010
- Ulrich-Lai, Y. M., Christiansen, A. M., Ostrander, M. M., Jones, A. A., Jones, K. R., Choi, D. C., Krause, E. G., Evanson, N. K., Furay, A. R., Davis, J. F., Solomon, M. B., de Kloet, A. D., Tamashiro, K. L., Sakai, R. R., Seeley, R. J., Woods, S. C., & Herman, J. P. (2010). Pleasurable behaviors reduce stress via brain reward pathways. Proceedings of the National Academy of Sciences, 107(47), 20529–20534. https://doi.org/https://doi.org/10.1073/pnas.1007740107
- van Strien, T., Herman, C. P., Anschutz, D. J., Engels, R. C., & de Weerth, C. (2012). Moderation of distress-induced eating by emotional eating scores. Appetite, 58(1), 277–284. https://doi.org/https://doi.org/10.1016/j.appet.2011.10.005
- Vidal, E. J., Alvarez, D., Martinez-Velarde, D., Vidal-Damas, L., Yuncar-Rojas, K. A., Julca-Malca, A., & Bernabe-Ortiz, A. (2018). Perceived stress and high fat intake: A study in a sample of undergraduate students. PloS One, 13, e0192827. https://doi.org/https://doi.org/10.1371/journal.pone.0192827
- Wallis, D. J., & Hetherington, M. M. (2004). Stress and eating: The effects of ego-threat and cognitive demand on food intake in restrained and emotional eaters. Appetite, 43(1), 39–46. https://doi.org/https://doi.org/10.1016/j.appet.2004.02.001
- Wallis, D. J., & Hetherington, M. M. (2009). Emotions and eating. Self-reported and experimentally induced changes in food intake under stress. Appetite, 52(2), 355–362. https://doi.org/https://doi.org/10.1016/j.appet.2008.11.007
- Wardle, J., Chida, Y., Gibson, E. L., Whitaker, K. L., & Steptoe, A. (2011). Stress and adiposity: A meta-analysis of longitudinal studies. Obesity, 19(4), 771–778. https://doi.org/https://doi.org/10.1038/oby.2010.241
- Wardle, J., Steptoe, A., Oliver, G., & Lipsey, Z. (2000). Stress, dietary restraint and food intake. Journal of Psychosomatic Research, 48(2), 195–202. https://doi.org/https://doi.org/10.1016/S0022-3999(00)00076-3
- Weinstein, S. E., Shide, D. J., & Rolls, B. J. (1997). Changes in food intake in response to stress in men and women: Psychological factors. Appetite, 28(1), 7–18. https://doi.org/https://doi.org/10.1006/appe.1996.0056
- Yau, Y. H., & Potenza, M. N. (2013). Stress and eating behaviors. Minerva Endocrinologica, 38(3), 255.
- Zellner, D. A., Loaiza, S., Gonzalez, Z., Pita, J., Morales, J., Pecora, D., & Wolf, A. (2006). Food selection changes under stress. Physiology and Behavior, 87(4), 789–793. https://doi.org/https://doi.org/10.1016/j.physbeh.2006.01.014
- Zellner, D. A., Saito, S., & Gonzalez, J. (2007). The effect of stress on men's food selection. Appetite, 49(3), 696–699. https://doi.org/https://doi.org/10.1016/j.appet.2007.06.013
- Zenk, S. N., Horoi, I., McDonald, A., Corte, C., Riley, B., & Odoms-Young, A. M. (2014). Ecological momentary assessment of environmental and personal factors and snack food intake in African American women. Appetite, 83, 333–341. https://doi.org/https://doi.org/10.1016/j.appet.2014.09.008