

ABSTRACT
Introduction
Approximately 40% of people with type 2 diabetes (T2D) also have chronic kidney disease (CKD), which substantially increases their risk of cardiovascular (CV)-related complications and mortality. Until recently, no approved therapies have directly targeted inflammatory and fibrotic pathways that drive disease progression and organ damage in patients with CKD associated with T2D.
Areas covered
Finerenone is a potent, selective, nonsteroidal mineralocorticoid receptor antagonist (MRA) that targets fibrosis and inflammation by blocking overactivation of the MR in the kidneys and heart. Finerenone has been associated with significant reductions in kidney- and CV-related endpoints compared with placebo and minimal effects on serum potassium and kidney function in phase III trials involving >13,000 patients with diabetic kidney disease (DKD). In addition to reviewing the clinical data, this review compares the properties of finerenone with those of the older steroidal MRAs spironolactone and eplerenone.
Expert opinion
Unlike spironolactone and eplerenone, finerenone has demonstrated a favorable benefit-risk profile offering an effective new treatment for patients with CKD associated with T2D. Increases in serum potassium are predictable and manageable and should not discourage the use of finerenone in clinical practice. It is important to discuss where finerenone ‘fits best’ within the current DKD management landscape.
Plain Language Summary
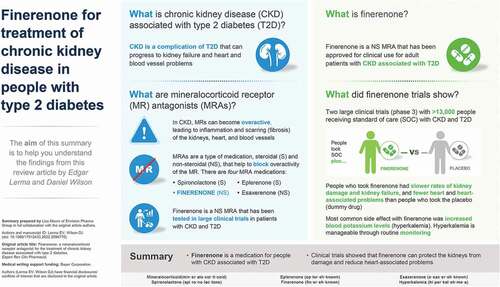
Around 4 in 10 people with type 2 diabetes (T2D) also have a condition called chronic kidney disease (also frequently referred to as diabetic kidney disease). People with T2D and chronic kidney disease have an overactive protein called the mineralocorticoid receptor (MR for short) in their kidney and heart cells. Overactive MRs causes inflammation and cell injury and can eventually cause damage to people’s kidneys and heart. Mineralocorticoid receptor antagonists (MRAs for short) are a type of drug that can be used to block the activity of the MR to reduce inflammation and damage to the kidneys and heart. There are two types of MRA – steroidal MRAs and non-steroidal MRAs. Steroidal MRAs (spironolactone and eplerenone) are an older type of MRA. Finerenone is a non-steroidal MRA and is a newer type of MRA. Researchers studied the effects of finerenone in two clinical trials involving more than 13,000 people withchronic kidney disease and T2D. In these trials people who took finerenone had slower rates of kidney damage and less heart and heart-associated problems than people who took a dummy drug (called a placebo). Some people taking finerenone may have increased blood potassium levels (called hyperkalemia), but this side effect can be managed and so people can continue to take finerenone. Researchers are continuing to research and consider where finerenone “fits best” among the available treatment options for people with T2D and chronic kidney disease.
Graphical abstract
Article highlights
Finerenone is a nonsteroidal mineralocorticoid receptor (MR) antagonist that is indicated to reduce the risk of sustained estimated glomerular filtration rate (eGFR) decline, end-stage renal disease, cardiovascular (CV) death, nonfatal myocardial infarction, and hospitalization for heart failure in adult patients with chronic kidney disease (CKD) associated with type 2 diabetes (T2D)
Upregulation of the renin-angiotensin-aldosterone system in CKD associated with T2D triggers overactivation of the MR to result in fibrosis and inflammation in the heart and kidneys
Finerenone has high potency and selectively for the MR, where it blocks sodium resorption and overactivation; tissue distribution of finerenone is balanced between the kidneys and heart
Finerenone is administered at a starting dose of 10 or 20 mg orally once daily (QD) based on eGFR and serum potassium thresholds. The target daily dose is 20 mg QD
In the largest phase III CKD outcomes program to date (>13,000 patients with diabetic kidney disease), finerenone has demonstrated efficacy benefits, including significant reductions in kidney- and CV-related endpoints, when compared with placebo
Finerenone has minimal effects on serum potassium and kidney function
Information resources
For further information regarding the published phase II and phase III randomized, controlled trials of finerenone, please refer to the cited references (see reference list). These articles can also be accessed via the following links:
Phase II (ARTS): https://pubmed.ncbi.nlm.nih.gov/23713082/
Phase II (ARTS-DN): https://pubmed.ncbi.nlm.nih.gov/26325557/
Phase II (ARTS-HF): https://pubmed.ncbi.nlm.nih.gov/27130705/
Phase III (FIDELIO-DKD): https://www.nejm.org/doi/full/10.1056/NEJMoa2025845
Phase III (FIGARO-DKD): https://www.nejm.org/doi/full/10.1056/NEJMoa2110956
Phase III (pooled analysis [FIDELITY]): https://pubmed.ncbi.nlm.nih.gov/35023547/
Data availability
Data sharing/availability is not applicable to this article as no new data were created or analyzed in this study.
Disclosure statement
EV Lerma has disclosed employment with Associates in Nephrology; consultancy agreements with Bayer and Vifor; ownership interest in Fresenius Joint Venture; receiving honoraria from Elsevier Publishing, McGraw-Hill Publishing, National Kidney Foundation, UpToDate, and Wolters Kluwer Publishing; serving as a scientific advisor or member of Journal of Clinical Lipidology, International Urology and Nephrology Journal, Journal of Vascular Access, Prescribers Letter, Renal and Urology News, ASN Kidney News, Reviews in Endocrinology and Metabolic Disorders, American Journal of Kidney Diseases Blog, American Heart Association Kidney and Cardiovascular Disease Leadership Group, and SCILL Committee; and speakers bureau for AstraZeneca, Bayer, Otsuka, and Vifor. DJ Wilson is a nephrologist and an employee of Bayer US LLC, Pharmaceuticals, Whippany, NJ, USA, who previously held academic and clinical positions at the Cleveland Clinic, Wake Forest University School of medicine, and Mayo Clinic Rochester.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.