
ABSTRACT
We describe the development of an evidence-based motor intervention and an implementation pilot study in ten primary schools, involving 515 children (4–11 years). ‘Helping Handwriting SHINE’ (HHS) is a novel, school-led, group-based handwriting intervention. Teaching staff delivered HHS and provided feedback through a questionnaire, reporting that: (i) the children found the tasks enjoyable; (ii) the background and booklet instructions were easy to understand, (iii) there was a need for more comprehensive staff training. The teaching staff made recommendations about session duration, group size, resource availability, and age differentiation of tasks. These suggestions are applicable to the development of any school-based group-led motor intervention, and we used this feedback to refine the HHS intervention. This study shows that implementing school-led motor interventions at scale is possible. Moreover, the work provides insights into the factors to consider when developing school-based motor interventions prior to conducting randomized controlled trials (RCT). The process outlined in this manuscript has led to an RCT to test the effectiveness of HHS within primary schools.
Introduction
Handwriting continues to be the main way of authoring text in the classroom and is the standard method of communication used in most examinations (McMaster & Roberts, Citation2016; Santangelo & Graham, Citation2016). This remains the situation despite the growing use of technology (such as tablets and laptops) within educational settings. This means that children who struggle in acquiring age-appropriate handwriting skills are at a considerable disadvantage in a number of different ways. For example, children who struggle with the mechanics of handwriting (so that the skill is not automated) may have reduced cognitive capacity for other mentally-demanding tasks such as generating creative ideas (Medwell, Strand, & Wray, Citation2009). Furthermore, a ‘presentation effect’ has been noted, whereby pieces of writing with the same content are scored more harshly when the writing is less legible (Graham, Harris, & Herbert, Citation2011; Santangelo & Graham, Citation2016). More generally, the process of handwriting has been shown to play an important role in the development of children’s cognitive and literacy skills (Frolek Clark & Luze, Citation2014; Graham, Struck, Santoro, & Berninger, Citation2006; Longcamp et al., Citation2008; Longcamp, Zerbato-Poudou, & Velay, Citation2005; Mangen & Velay, Citation2010; McCarney, Peters, Jackson, Thomas, & Kirby, Citation2013; Waterman, Havelka, Culmer, Hill, & Mon-Williams, Citation2014). It is therefore unsurprising that handwriting ability has been found to predict academic attainment (Dinehart, Citation2015; McCarney et al., Citation2013).
In recent UK national curriculum assessments, 31% of children aged 5–6 years and 22% of children aged 10–11 years did not achieve the expected standard of writing (Department for Education, Citation2019a, Citation2019b). It has been suggested that improved handwriting instruction and support should be available for all children given the scale of these difficulties (Feder, Majnemer, & Synnes, Citation2000; Hoy, Egan, & Feder, Citation2011; McCarney et al., Citation2013; Thomas & Radimsky, Citation2013; Wood, Eddy, & Hill, Citation2019). In the UK, one common pathway for children with handwriting difficulties is via referral to occupational therapy services (Feder et al., Citation2000). There is evidence that occupational therapy can improve outcomes (Hoy et al., Citation2011) but access to these services can be very limited (Kolehmainen, MacLennan, Francis, & Duncan, Citation2010). Thus, it would be beneficial to have an evidence-based handwriting intervention delivered autonomously by teaching staff within schools. The current work presents a description of a novel school-led method and an exploration of the barriers to the implementation of such an intervention.
Research Aims
This project specifically set out to:
1. Develop a novel intervention (Helping Handwriting SHINE) based on evidence from occupational therapy, education, and motor learning approaches that educational professionals could deliver autonomously in school.
2. Provide a comprehensive description of the intervention, to encourage transparency and allow the possibility for replication.
3. Pilot the intervention program in 10 primary schools, in order to identify any potential barriers to school-led implementation, prior to evaluation in a randomized controlled trial.
Methods (I): Developing the Intervention
In order to develop the intervention, the first author (KAS) considered evidence from a meta-analysis (Santangelo & Graham, Citation2016) and systematic review (Hoy et al., Citation2011) on handwriting therapy, in order to identify ‘what works’ in handwriting interventions (school-led or otherwise). KAS also reviewed the broader motor skills literature to ensure clinical recommendations for best practice were considered, with a focus on Developmental Coordination Disorder (Blank, Smits-Engelsman, Polatajko, & Wilson, Citation2011; Smits-Engelsman, Blank, & van der Kaay, Citation2013a). This aligned with recommendations that effective interventions need to be based on evidence from the handwriting and motor learning literature (Wallen, Duff, Goyen, & Froude, Citation2013). In parallel to this work, several of the coauthors (SM, LJBH & MMW) conducted a systematic review of motor skill interventions (Preston et al., Citation2017). We then drafted initial intervention plans with input from coauthors (KAS, SM, LJBH, AHW, DAS & MMW) who have expertise in the fields of developmental and cognitive psychology, education, occupational therapy, and motor learning. Independently, DAS consulted with fellow experts on the advisory board of the National Handwriting Association (UK-based charity), feeding back their recommendations into the development process.
The following sections explain the design choices made following these reviews and discussions, and a summary of the intervention. A completed Template for Intervention Description and Replication (TIDieR) checklist (Hoffmann et al., Citation2014) is available in Supplementary Material B.
Rationale for In-school Group-based Intervention
Graded approaches and/or integrated pathways have been suggested as a means of widening access to services for children with motor disorders (Stephenson & Chesson, Citation2008). The first step in such approaches is to increase the provision of support in the home or school environment through, for example, enhanced skills training programs that can be provided by teachers or parents (Camden, Wilson, Kirby, Sugden, & Missiuna, Citation2015). These approaches should be beneficial to children with or without a formal diagnosis. Children who continue to have difficulties following this stage can then be referred for more specialist help, in accordance with guidelines such as the ‘Partnering for Change’ Model (Missiuna et al., Citation2012) or ‘Response to Intervention Frameworks’ (National Center on Response to Intervention, Citation2010). One example of using such an approach ended a two-year waiting list for physiotherapy and reduced occupational therapy referrals, giving children earlier access to intervention which was often provided in their schools (Angilley & Locking, Citation2011).
One challenge in such graded approaches is identifying viable ‘frontline’ interventions that are suitable for school use in the initial phases. One potentially viable intervention is small group delivery which can be an effective method for children who have co-ordination difficulties (Smits-Engelsman et al., Citation2018). Small groups offer the potential for children to enjoy activities and games with their peers, gain feedback, obtain support, and allow strategy sharing (Anderson, Wilson, & Williams, Citation2017; Williams & Shellenberger, Citation1996). It may also be more socially acceptable for a child to work within a group rather than being ‘singled out’ in the classroom for individual attention (Milsom, Citation2006). Working in the everyday context of school (as opposed to a clinical setting) has also been identified as beneficial as it ensures therapy is adapted to recognize the child’s usual environment (Rens & Joosten, Citation2014).
Group interventions for handwriting have been successfully employed previously. For example, the ‘Write Start’ program (Case-Smith, Holland, & Bishop, Citation2011) involved teachers and occupational therapists co-teaching a twelve-week intervention with two 45-minute group sessions per week. The intervention involved handwriting instruction, self-evaluation, and feedback, and was found to be effective in subsequent studies (Case-Smith, Holland, Lane, & White, Citation2012; Case-Smith, Weaver, & Holland, Citation2014). However, the cost of employing an occupational therapist, for multiple classes, is a prohibitive factor in the implementation of this type of intervention for many schools. One potential solution is to create a group-based intervention that can be teacher-led. We, therefore, developed a group setting intervention, though we did not prescribe the number of children per group (to allow for teacher autonomy). Since we developed the intervention, a systematic review confirmed that small group interventions are at least as effective, and potentially more practical and resource-efficient, than one-to-one sessions (Smits-Engelsman et al., Citation2018).
Rationale for Specific Intervention Approach
The systematic review used to develop HHS focused on interventions for improving handwriting, specifically for elementary school-age children with handwriting difficulties (Hoy et al., Citation2011). Eleven studies were included, with a diverse range of intervention approaches, e.g., relaxation, electromyography (EMG), or sensory-based training, with and without handwriting practice. The intervention settings and delivery methods also varied, with some co-taught by teachers and occupational therapists in the classroom, some taught solely by occupational therapists in a handwriting group setting, and some taught purely by the teacher in the classroom. The majority of studies involved Grade 1–4 children (age 6–10 years). Only the interventions that included handwriting-based practice with a minimum threshold of 20 sessions and at least two sessions per week improved the legibility of handwriting (Hoy et al., Citation2011). We discuss other key findings below.
Ergonomic Factors
There is evidence that in-hand manipulation is affected by the quality of a child’s seated position (Smith-Zuzovsky & Exner, Citation2004) and that proficient and non-proficient writers significantly differ on ergonomic factors – such as body positioning, pen-grip, pen positioning, and consistency of pen grip (Rosenblum, Goldstand, & Parush, Citation2006). Therefore, a ‘preparing for handwriting’ section started each session, where session leaders would encourage the children to adopt a stable and comfortable position before starting writing. The advice included seating position, making sure the page was steady, and adopting an appropriate pen-grip.
Writing Practice and Component Skills Tasks
The reduction of a task into its various components has been found to help with training (particularly with younger children), provided these tasks are subsequently integrated in a functional context (Darrah, Law, & Pollock, Citation2001). Thus, five ‘drawing’ tasks were included in the intervention (drawing shapes, drawing crosses, completing mazes, coloring, and circling dots). These provide children with practise at more elementary stylus skills (pen or pencil) that are essential for composing written letters. For example, the ‘crosses’ activity emphasized accurately drawing lines, which is necessary for forming letters correctly.
These skills were then utilized in one of the handwriting tasks (writing individual letters, writing groups of two or three letters, writing letters that joined similarly, writing whole sentences, and planning and writing longer pieces of work). These writing tasks were particularly important because teaching handwriting (rather than other aspects of ‘writing’ such as phonological awareness or spelling) is necessary for improving legibility and speed of handwriting (Santangelo & Graham, Citation2016), and effective interventions all include handwriting practice (Hoy et al., Citation2011).
Variability of Practice
Theoretical frameworks within the sensorimotor literature suggest that ‘variability of practice’ accelerates motor learning (Schmidt & Lee, Citation1988). This principle implies that the same skill (i.e. using a pen) should be practised in as many ways as possible so that the skill can be transferred to other situations (Levac, Wishart, Missiuna, & Wright, Citation2009). Therefore, the HHS intervention included several manual dexterity tasks in each session together with tasks that specifically involved practising writing skills. For pen skills, sessions included a choice of five drawing activities and a selection of five handwriting activities. We also included other manual skills (making shapes with playdough, necklaces, folding paper, using scissors and stickers), which provided more choice for teachers with regard to ‘fun activities’ and was aimed at enhancing group process, engagement, and motivation.
Cognitive Orientation
The most effective type of approach for handwriting interventions has been argued to involve cognitive-based activities (Weintraub, Yinon, Hirsch, & Parush, Citation2009). Intervention for children with motor difficulties, such as the Cognitive Orientation to Daily Occupational Performance approach (Missiuna, Mandich, Polatajko, & Malloy-Miller, Citation2001; Polatajko & Mandich, Citation2004; Polatajko, Mandich, Miller, & Macnab, Citation2001) and Neuromotor Task Training (Schoemaker, Niemeijer, Reynders, & Smits-Engelsman, Citation2003) are built around the development of task awareness through verbal instructions and self-evaluation (although neither of these approaches focus specifically on handwriting). In sum, cognitive methods are recommended for effective handwriting instruction (Santangelo & Graham, Citation2016; Troia & Graham, Citation2003). We, therefore, built a ‘model-plan-evaluate’ structure into each task in HHS, in alignment with the principles of the Cognitive Orientation to Daily Occupational Performance (CO-OP) method (Polatajko & Mandich, Citation2004).
Task Difficulty
In order to maximize the potential for learning, Guadagnoli and Lee (Citation2004) suggest that there is an optimal task difficulty (Schmidt & Lee, Citation1988). The task must be achievable to provide useful feedback, but if the task is too easy then completing the task does not yield information. This ‘just-right’ level of challenge, described as the ‘zone of proximal development’ (Vygotsky, Citation1980), is a key part of occupational therapy practice (Rebeiro & Polgar, Citation1999) and the cognitive approach used in this intervention. Thus, three ‘stages’ of difficulty were developed for each task, and the session leader was instructed to pick a level of difficulty for each child that they felt would be suitably challenging for them, whilst still being achievable. The booklet’s guidance states: “You should use your judgement as to which stage is most suitable for the children in your group on each task; you should progress to the next stage if they are finding a task too simple”. One stage is associated with each task in a given session using the model-plan-evaluate approach, with the option to increase, decrease, or maintain this stage the next time this task was completed.
Summary of the Intervention Sessions
In line with the evidence-based principles identified in the previous section, we designed the HHS intervention session to be 20 minutes in duration. The first five minutes involve ‘preparing for handwriting.’ The next ten minutes cover ‘pen skills,’ where session leaders select one drawing task as a warm-up activity (from a choice of five), and one handwriting activity (from a choice of five). Finally, the last five minutes comprise practise of one of the ‘other manual skills’ (from the choice of five). See for a representation of the session, and the booklet in Supplementary Material A for further details of these activities.
Figure 1. Outline of a session
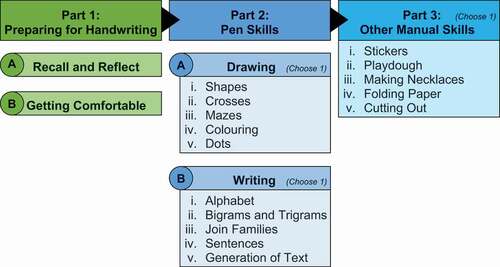
We asked that different tasks be used within a given week to ensure maximum variability. Each task was divided into three ‘stages,’ differentiating the anticipated difficulty level for children with different levels of ability, with Stage 1 as the easiest and Stage 3 as the hardest. There was also a model-plan-evaluate table for each task, which encapsulated the cognitive aspect of the intervention.
Methods (II): Implementation
Research Context
The City of Bradford, UK, is a low socioeconomic status (SES) area according to the Index of Multiple Deprivation (Office for National Statistics, Citation2011). Low SES has been identified as a factor associated with poorer academic outcomes (Sirin, Citation2005), and with higher rates of handwriting and motor co-ordination problems (Lingam, Hunt, Golding, Jongmans, & Emond, Citation2009; Potter, Mashburn, & Grissmer, Citation2013). Established to address the high levels of childhood morbidity and mortality, the Born in Bradford longitudinal cohort began in 2007 (Wright et al., Citation2013). Through links with this project, a group of 10 Primary schools in Bradford had approached our research team with concerns about the high number of children with motor co-ordination difficulties in their classrooms (with handwriting identified as a particular problem).
Participants
Ten primary schools in Bradford, UK, signed up to pilot the intervention at the beginning of 2015. Teachers from Reception (aged 4–5 years) through to Year 6 (aged 10–11 years) selected children they believed had handwriting difficulties that would benefit from intervention in a small group. No more specific inclusion/exclusion criteria were set, since the aim was that the selection and running of the intervention would be as autonomous as possible within the schools. Five hundred and fifteen children were initially selected by their teachers to participate, which represented 10.4% of the entire school roll of all the schools (n = 4961). The mean age of participants was 7.8 years (ranging between 4.5 and 11.5 years), 393 (76.3%) were male (one child’s gender was not recorded), and 450 (87.4%) were right-handed.
We obtained informed written consent from Head Teachers of the participating schools. As the school staff were delivering the intervention, the schools also obtained informed consent directly from the parents/guardians of the children, giving them written information in advance about the intervention and their right to opt out, should they wish to do so. The University of Leeds Research Ethics committee (ref: 15–0089) provided Ethical approval for the study.
Materials
The background, instructions, tasks, and templates for the HHS intervention were contained within a single booklet (see Supplementary Material A for examples). Each school received one pack containing one booklet per class and 20 color photocopies of each ‘additional materials’ page (e.g. session plans, templates) per class. The packs also contained a sample of materials for the ‘other manual skills’ section of the intervention session, including playdough, stickers, beads, and thread. The research team designed these tasks with the expectation in mind that the materials they required would be readily available in schools.
Task Delivery
We piloted the intervention as three 20-minute sessions a week for five weeks in order to assess any barriers for autonomous school-led implementation. Approximately 60 ‘session leaders,’ who were either class teachers, teaching assistants (TAs), or special educational needs coordinators (SENCOs), delivered the intervention. We designed the 20-minute duration so that children were not removed from entire lessons. We considered this duration a sufficient length of time to expose any issues with the structure and the intervention.
Session leaders were briefed in person in one of the two briefing meetings (two-hour duration) conducted by the first author (KAS), with approximately 30 leaders attending each meeting. The attendees could cascade the training to colleagues as appropriate. In the briefings, the session leaders looked through the packs and booklets and had the opportunity to ask questions. We provided session leaders with contact details for the first author. We provided this minimal, economical level of support and instruction in order to identify any barriers to the future autonomous implementation of the intervention. Schools had indicated that the amount of time provided for the briefing was commensurate with the amount of time they had available to set aside for this type of training. They also indicated they were happy to experiment with establishing if this was sufficient within the pilot.
We implemented the intervention in five schools at a time, in two waves. The schools had the choice of wave subject to their availability. The schools in the first wave took part in the intervention during the Spring term of 2015 (between March and April), with the second wave of five schools taking part in the intervention in the Summer term of 2015 (between May and June).
We did not assess adherence and fidelity but we captured feedback from the session leaders regarding their experiences when implementing the intervention via an online questionnaire. We emailed a link to this questionnaire to the main contact at each school after the second wave of schools had completed the intervention, asking them to forward the questionnaire to the members of staff who had acted as session leaders. We sent a follow-up e-mail to the same contact five days later, asking them to remind session leaders to complete this.
Results
Two of the ten schools dropped out during the course of the study, one from each wave (68 and 60 participating children, respectively). For one of these schools, the new intervention lead did not know when to start the study because there was a changeover of staff. The other school dropped out because they needed to prioritize participating in an Office for Standards in Education, Children’s Services and Skills (Ofsted) inspection of their school (unannounced). We noted that both of the schools reported they would be keen to be part of future research on the intervention.
Issues and Improvements
Possible barriers to autonomous implementation by teaching staff were identified via informal discussions held as part of the two pre-intervention briefing meetings (attended by approximately 30 teaching staff each) and through an online post-intervention feedback questionnaire, which received 19 responses (See S3 File for the questions asked and sample responses). Of these 19 questionnaire responses, eight responders were from one school who took part in the first intervention wave, with one responder from a second school in this wave; seven responders came from a single school in the second intervention wave, two from a second school in this wave, and one from a third school. This amounts to five of the ten schools engaging with the post-intervention questionnaire. In terms of roles, the respondents were 15 teaching assistants, one teacher, and three ‘others’ describing themselves, respectively, as an Inclusion Support Leader, a SEN Inclusion Leader, and a Cover Supervisor.
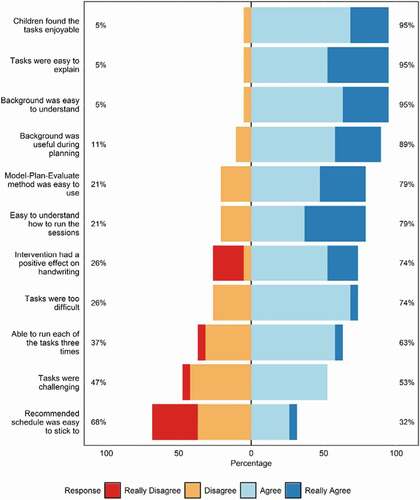
shows responses to the Likert-style questions. There was a pattern of high agreement (79–95%) to statements such as the tasks being enjoyable and easy to explain, the background being useful and easy to understand, and the Model-Plan-Evaluate method being easy to use. Notably, 74% of teaching staff believed that the intervention has a positive effect on the children’s handwriting. However, while 53% agreed that the tasks were challenging, 74% felt that the tasks were too difficult. Finally, 68% disagreed that the schedule was easy to stick to, and 37% were not able to deliver each task three times during the intervention. Teaching staff also provided qualitative responses, where five main issues were raised. We discuss these in turn, feeding in key quantitative responses where appropriate.
Figure 2. Responses to the feedback questionnaire
Issue 1. Age-appropriateness of Tasks
In the briefing meeting with the first wave of schools, session leaders suggested that a number of the writing tasks would be too demanding for younger children. This parallels the responses to the Likert questions, where 74% responded that the tasks were too difficult. For the purposes of this study, we told the schools to replace a more difficult writing task with one of the simpler ones if the children could not complete them, and we communicated this decision to schools at the briefing meeting with the second wave of schools. Although we originally intended one booklet to cover all ages, the study showed that producing separate booklets tailored to different ages would be beneficial. For example, we could create two difficulty levels with each containing five age-appropriate writing tasks. This would ensure the most appropriate level of challenge whilst maintaining the variability of tasks for the younger children.
Issue 2. Availability of Resources
Some session leaders stated they did not have suitable resources for the ‘other manual skills’ section (e.g. the playdough and beads). While the packs provided to schools included a set of these materials, it appeared that even within these schools, it was difficult for all of the classes to gain access to them. When asked, “Was there any additional support (for example, extra materials/training sessions etc.) you would have found useful when running the intervention?” in the feedback questionnaire, one of the respondents commented:
“It took time finding resources and it was costly buying some of the resources that were required. (My own money!)”
It was possible to alter the three tasks requiring materials (stickers, playdough, and threading beads) so that no extra equipment was needed. We, therefore, revised HHS to remove the ‘other manual skills’ activities, allowing more time to practice the ‘pen skills’ sections. Whilst some non-writing activities were included to help encourage and engage students, this is not consistent with a task-oriented approach so removing these activities is potentially a good amendment. Removing the ‘other manual skills’ activities is consistent with the pen-skill components having a stronger evidence base for directly influencing handwriting. Specific pen skill tasks (writing, drawing) are more directly relevant to the ‘activity’ the intervention seeks to support, in the context of the International Classification of Functioning, Disability and Health (World Health Organisation, Citation2001). This change is also supported by findings that handwriting improves through handwriting practice itself rather than via more generic training subcomponent-focused activities (such as hand strengthening exercises), which do not directly involve pen/pencil work (Hoy et al., Citation2011; Smits-Engelsman et al., Citation2018).
Issue 3. Session Duration
A number of the session leaders felt that it was not easy to adhere to the recommended schedule. The main reason identified for this was that it was difficult to fit the intervention session into 20 minutes, for example
“Some of the children in the groups were children who took longer than 10-15 minutes to settle down. This affected how long the activity took and the success of the session.”
“It was very difficult to run the intervention within the allocated 20 minutes. This was because the handwriting tasks were quite long.”
This mirrored quantitative responses, where 68% responded that the schedule was not easy to maintain. We, therefore, extended HHS intervention sessions to 30 minutes to help ensure fidelity to the intervention. The new session structure was then: 5 minutes preparing for handwriting (as before), 5–10 minutes warm-up on the drawing tasks, and 15–20 minutes on the handwriting tasks.
Issue 4. Example Sessions
Three of the schools in the second wave asked the first author to go through an example session with members of staff (or for one school, with a group of children) so that they felt more comfortable running the intervention. We provided such sessions. Teaching staff also raised this issue through the questionnaire. When asked “Was there any additional support (for example, extra materials/training sessions etc.) you would have found useful when running the intervention?”, and “Do you have any final suggestions or comments as to how we could improve the intervention, or make it easier to run?”, respondents raised this issue. For example,
“Training should of contained some demonstration of how to carry out the activities. The booklet was easy to follow but this would of helped.”
“Although the handbook was self explanatory I felt some activities would have been understood better if discussed and shown in person.”
We, therefore, expanded the HHS intervention training to include an initial 6 hours (rather than 2 hours) full-day training session led by a team including an occupational therapist. Moreover, we designed the training in collaboration with specialist leaders in teacher education. We also developed website hosting demonstration videos for the activities. The longer training session allowed time to explain why handwriting is important, and facilitated a discussion on what helps or hinders teaching initiatives of this type. Teachers’ suggestions from this discussion could then be related to the set of ‘key principles’ underpinning the intervention and teaching staff could be introduced to the structure and activities. The trainers then simulated a 30-minute intervention session, while the teachers noted down any potential challenges they foresaw. Following lunch, the trainers troubleshot any challenges, with input from other teachers, before providing all staff with the opportunity to role-play, act as the session leads and deliver the three parts of the session.
Issue 5. Size of Groups
The final issue raised regarded the intervention group size. The schools were responsible for deciding the number of children in their groups. Some session leaders chose to work with groups of 3–4, but other session leaders worked with groups of 5–7 children, reporting that they found this group size to be too large. We, therefore, amended the HHS intervention so that it was delivered in groups of around four students.
Discussion
This study aimed to justify, describe, and identify possible improvements in the early stages of developing a school-led, evidence-based handwriting intervention. This is a necessary precursor before evaluated of any such intervention in a randomized controlled trial. We designed the intervention so that it could be carried out entirely by teaching staff in their schools, and teaching staff identified barriers to autonomous implementation with such an approach.
Overall, the session leaders reported that they found the intervention easy to understand and explain, and felt the Model-Plan-Evaluate method was easy to use. Handwriting was a recognized issue within this group of schools; on average, more than 10% of students in the ten participating schools were included in the intervention. This concurs with reports of 10–30% of children being identified with handwriting difficulties in other studies (Karlsdottir & Stefansson, Citation2002). Whilst we were primarily interested in feasibility, three quarters of feedback respondents believed that the intervention positively affected children’s handwriting. Although extreme caution must be exercised when interpreting such anecdotal reports, it is encouraging to learn teacher’s perceptions were this positive.
We successfully implemented the intervention in eight of the ten schools, and the two schools that dropped out were keen to implement the intervention at another time. Thus, from the perspectives of teachers and teaching assistants, this approach shows excellent potential as a novel method of implementing a school-based intervention for children with handwriting difficulties. Such interventions are needed as steps are made within health and education to move toward more integrated service delivery for assessment and intervention (Missiuna et al., Citation2012).
Limitations and Directions for Future Research
Further to the improvements identified by teachers in the previous section, there are recommendations for how the current work could be refined. First, whilst the teachers reported that their students enjoyed the handwriting activities, we did not evaluate this directly with the children. Future research will focus on the children’s experience of the intervention through both observation and interview, together with teachers’ and parent/guardians’ opinions. Second, there is an interplay between the content of the intervention, the person delivering the intervention, the child, and the environment, which we were not able to capture fully in this pilot study. The HHS intervention meets the Medical Research Council’s definition of ‘complex’ (Craig et al., 2008), meaning that the way the session leaders work with their groups to foster learning attributes and build self-esteem could be a key factor in the effectiveness of an intervention. Future studies could incorporate process evaluation into the study (Moore et al., 2015) to help improve understanding of the active components of the intervention; for example, how the session leader’s skills and the environmental context can support children’s learning.
Third, because this was a feasibility study, this study did not record factors such as the children’s first language, knowledge of the alphabet, or special educational needs status. Future work could explore how such individual learner’s needs interact with (and affect) the individual’s experiences of the intervention. This would help to inform a pathway for referral to the next tier of intervention such as specialist, individual therapy (Missiuna et al., Citation2012). Fourth, the same author completed the intervention training, data gathering, and evaluation in this pilot study. In future work, separate teams should complete the training of the teaching staff, and evaluation of the intervention. Finally, we did not assess adherence and fidelity as part of the pilot but this will be an important component of the forthcoming randomized controlled trial (ISRCTN.com/ISRCTN13315075; doi: 10.1186/ISRCTN13315075).
Practice Implications
HHS could be one of the range of interventions that teachers can use autonomously, or in collaboration with occupational therapists. While we designed the intervention as an alternative to direct input from occupational therapists, occupational therapists could complement this approach. This approach could reduce the number of children referred to occupational therapy at a later stage and have a positive impact on waiting list times, as per the Partnering for Change Model (Missiuna et al., Citation2012) and Response to Intervention Frameworks (National Center on Response to Intervention, Citation2010).
Conclusions
There is a need for evidence-based motor interventions to be more widely available to schools, and for newly developed interventions to be more transparent in reporting their design and development. We designed HHS to provide a step in a graded approach to supporting children with handwriting difficulties, facilitating earlier and wider access to intervention. Following this study, we have revised HHS before evaluation via a randomized controlled trial. The important conclusion from the present study is that delivering clinically informed, structured support for motor skills within the classroom is both promising and viable.
Declaration Of Interest Statement
No potential conflict of interest was reported by the authors.
Acknowledgments
We dedicate this paper to the memory of Professor David Sugden. David was a passionate advocate for supporting children’s educational needs, and he played a fundamental role in highlighting the necessity of considering a child’s motor abilities when providing educational support. Moreover, David was an inspiration and a wonderful man who touched many lives – including all of his fellow authors on this paper, who will sorely miss his wisdom and kindness. We are extremely grateful to all the teachers, teaching assistants, children, and parents who made this research possible.
Additional information
Funding
References
- Anderson, L., Wilson, J., & Williams, G. (2017). Cognitive orientation to daily occupational performance (CO‐OP) as group therapy for children living with motor coordination difficulties: An integrated literature review. Australian Occupational Therapy Journal, 64, 170–184. doi:https://doi.org/10.1111/1440-1630.12333
- Angilley, H., & Locking, T. (2011). An integrated pathway for children with coordination difficulties in Wakefield. Association of Paediatric Chartered Physiotherapists Journal, 2(3), 31–33.
- Berninger, V. W., Vaughan, K., Abbott, R. D., Begay, K., Coleman, K. B., Curtin, G., … Graham, S. (2002). Teaching spelling and composition alone and together: Implications for the simple view of writing. Journal of Educational Psychology, 94(2), 291–304. doi:https://doi.org/10.1037/0022-0663.94.2.291
- Blank, R., Barnett, A. L., Cairney, J., Green, D., Kirby, A., Polatajko, H., … Vinçon, S. (2019). International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Developmental Medicine and Child Neurology, 61(3), 242–285. doi:https://doi.org/10.1111/dmcn.14132
- Blank, R., Smits-Engelsman, B., Polatajko, H., & Wilson, P. (2011). European academy for childhood disability (EACD): Recommendations on the definition, diagnosis and intervention of developmental coordination disorder (long version). Developmental Medicine and Child Neurology, 54(1), 54–93. doi:https://doi.org/10.1111/j.1469-8749.2011.04171.x
- Camden, C., Wilson, B. N., Kirby, A., Sugden, D. A., & Missiuna, C. (2015). Best practice principles for management of children with developmental coordination disorder (DCD): Results of a scoping review. Child: Care, Health and Development, 41(1), 147–159. doi:https://doi.org/10.1111/cch.12128
- Case-Smith, J., Holland, T., & Bishop, B. (2011). Effectiveness of an integrated handwriting program for first-grade students: A pilot study. American Journal of Occupational Therapy, 65(6), 670–678. doi:https://doi.org/10.5014/ajot.2011.000984
- Case-Smith, J., Holland, T., Lane, A., & White, S. (2012). Effect of a coteaching handwriting program for first graders: One-group pretest-posttest design. American Journal of Occupational Therapy, 66(4), 396–405. doi:https://doi.org/10.5014/ajot.2012.004333
- Case-Smith, J., Weaver, L., & Holland, T. (2014). Effects of a classroom-embedded occupational therapist-teacher handwriting program for first-grade students. American Journal of Occupational Therapy, 68(6), 690–698. doi:https://doi.org/10.5014/ajot.2014.011585
- Darrah, J., Law, M., & Pollock, N. (2001). Innovations in practice. Family-centered functional therapy — A choice for children with motor dysfunction. Infants and Young Children, 13(4), 79–87. doi:https://doi.org/10.1097/00001163-200113040-00014
- Department for Education. (2019a). Phonics screening check and key stage 1 assessments in England, Retrieved March 26, 2020, from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/851296/Phonics_screening_check_and_key_stage_1_assessments_in_England_2019.pdf
- Department for Education. (2019b). National curriculum assessments at key stage 2 in England, Retrieved March 26, 2020, from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/851798/KS2_Revised_publication_text_2019_v3.pdf
- Dinehart, L. H. (2015). Handwriting in early childhood education: Current research and future implications. Journal of Early Childhood Literacy, 15(1), 97–118. doi:https://doi.org/10.1177/1468798414522825
- Engel, C., Lillie, K., Zurawski, S., & Travers, B. G. (2018). Curriculum-based handwriting programs: A systematic review with effect sizes. American Journal of Occupational Therapy, 72(3), 7203205010p1–8. doi:https://doi.org/10.5014/ajot.2018.027110
- Feder, K. P., Majnemer, A., & Synnes, A. (2000). Handwriting: Current Trends in Occupational Therapy Practice. Canadian Journal of Occupational Therapy, 67(3), 197–204. doi:https://doi.org/10.1177/000841740006700313
- Frolek Clark, G., & Luze, G. (2014). Predicting handwriting performance in kindergarteners using reading, fine-motor, and visual-motor measures. Journal of Occupational Therapy, Schools, & Early Intervention, 7(1), 29–44. doi:https://doi.org/10.1080/19411243.2014.898470
- Glasziou, P., Meats, E., Heneghan, C., & Shepperd, S. (2008). What is missing from descriptions of treatment in trials and reviews? BMJ (Clinical Research Ed.), 336(7659), 1472–1474. doi:https://doi.org/10.1136/bmj.39590.732037.47
- Graham, S., Harris, K. R., & Herbert, M. (2011). It is more than just the message: Presentation effects in scoring writing. Focus on Exceptional Children, 44(4), 1–12.
- Graham, S., Struck, M., Santoro, J., & Berninger, V. W. (2006). Developmental neuropsychology dimensions of good and poor handwriting legibility in first and second graders: Motor programs, visual – spatial arrangement, and letter formation parameter setting. Developmental Neuropsychology, 29(1), 43–60. doi:https://doi.org/10.1207/s15326942dn2901
- Guadagnoli, M. A., & Lee, T. D. (2004). Challenge point: A framework for conceptualizing the effects of various practice conditions in motor learning. Journal of Motor Behavior, 36(2), 212–224. doi:https://doi.org/10.3200/JMBR.36.2.212-224
- Hall, T., Meyer, A., & Rose, D. (2012). Universal design for learning in the classroom. New York: Guilford Press.
- Hoffmann, T. C., Erueti, C., & Glasziou, P. P. (2013). Poor description of non-pharmacological interventions: Analysis of consecutive sample of randomised trials. BMJ, 347(7924), f3755. doi:https://doi.org/10.1136/bmj.f3755
- Hoffmann, T. C., Glasziou, P. P., Boutron, I., Milne, R., Perera, R., Moher, D., … Voigt-Radloff, S. (2014). Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ, 7(348), g1687. doi:https://doi.org/10.1136/bmj.g1687
- Hoy, M. M. P., Egan, M. Y., & Feder, K. P. (2011). A systematic review of interventions to improve handwriting. Canadian Journal of Occupational Therapy, 78(1), 13–25. doi:https://doi.org/10.2182/cjot.2011.78.1.3
- Karlsdottir, R., & Stefansson, T. (2002). Problems in developing functional handwriting. Perceptual and Motor Skills, 94(2), 623–662. doi:https://doi.org/10.2466/pms.2002.94.2.623
- Kolehmainen, N., MacLennan, G., Francis, J. J., & Duncan, E. A. (2010). Clinicians’ caseload management behaviours as explanatory factors in patients’ length of time on caseloads: A predictive multilevel study in paediatric community occupational therapy. BMC Health Services Research, 10(1). doi:https://doi.org/10.1186/1472-6963-10-249
- Levac, D., Wishart, L., Missiuna, C., & Wright, V. (2009). The application of motor learning strategies within functionally based interventions for children with neuromotor conditions. Pediatric Physical Therapy, 21(4), 345–355. doi:https://doi.org/10.1097/PEP.0b013e3181beb09d
- Lingam, R., Hunt, L. P., Golding, J., Jongmans, M. J., & Emond, A. (2009). Prevalence of developmental coordination disorder using the DSM-IV at 7 years of age: A UK population-based study. Pediatrics, 123(4), e693–e700. doi:https://doi.org/10.1542/peds.2008-1770
- Longcamp, M., Boucard, C., Gilhodes, J.-C., Anton, J.-L., Roth, M., Nazarian, B., & Velay, J.-L. (2008). Learning through hand- or typewriting influences visual recognition of new graphic shapes: Behavioral and functional imaging evidence. Journal of Cognitive Neuroscience, 20(5), 802–815. doi:https://doi.org/10.1162/jocn.2008.20504
- Longcamp, M., Zerbato-Poudou, M.-T., & Velay, J.-L. (2005). The influence of writing practice on letter recognition in preschool children: A comparison between handwriting and typing. Acta psychologica, 119(1), 67–79. doi:https://doi.org/10.1016/j.actpsy.2004.10.019
- Mangen, A., & Velay, J.-L. (2010). Digitizing literacy: Reflections on the haptics of writing. In M. H. Zadeh (Ed.), Advances in haptics (pp. 385–403). INTECH.
- McCarney, D., Peters, L., Jackson, S., Thomas, M., & Kirby, A. (2013). Does poor handwriting conceal literacy potential in primary school children? International Journal of Disability, Development and Education, 60(2), 105–118. doi:https://doi.org/10.1080/1034912X.2013.786561
- McMaster, E., & Roberts, T. (2016). Handwriting in 2015: A main occupation for primary school-aged children in the classroom? Journal of Occupational Therapy, Schools, and Early Intervention, 9(1), 38–50. doi:https://doi.org/10.1080/19411243.2016.1141084
- Medwell, J., Strand, S., & Wray, D. (2009). The links between handwriting and composing for Y6 children. Cambridge Journal of Education, 39(3), 329–344. doi:https://doi.org/10.1080/03057640903103728
- Milsom, A. (2006). Creating positive school experiences for students with disabilities. Professional School Counseling Journal, 10(1), 66–72. doi:https://doi.org/10.5330/prsc.10.1.ek6317552h2kh4m6
- Missiuna, C., Mandich, A., Polatajko, H., & Malloy-Miller, T. (2001). Cognitive orientation to daily occupational performance (CO-OP): Part I - Theoretical foundations. Physical & Occupational Therapy in Pediatrics, 20(2–3), 69–81. doi:https://doi.org/10.1007/s13398-014-0173-7.2
- Missiuna, C. A., Pollock, N., Levac, D., Campbell, W., Whalen, S., Bennett, S., … Russell, D. (2012). Partnering for Change: An innovative school-based occupational therapy service delivery model for children with developmental coordination disorder. Canadian Journal of Occupational Therapy, 79(1), 41–50. doi:https://doi.org/10.2182/cjot.2012.79.1.6
- National Center on Response to Intervention. (2010). Essential Components of RTI – A Closer Look at Response to Intervention. U.S. Office of Special Education Programs.
- Office for National Statistics. (2011). Index of Multiple Deprivation 2010. Newport.
- Olsen, J. (1980). Handwriting Without Tears (3rd ed.). Brookfield, IL: Fred Sammons.
- Polatajko, H. J., & Mandich, A. D. (2004). Enabling occupation in children: The cognitive orientation to daily occupational performance (CO-OP) approach. Ottawa: Canadian Association of Occupational Therapists.
- Polatajko, H. J., Mandich, A. D., Miller, L. T., & Macnab, J. J. (2001). Cognitive orientation to daily occupational performance (CO-OP): Part II - The evidence. Physical & Occupational Therapy In Pediatrics, 20(2–3), 83–106. doi:https://doi.org/10.1080/J006v20n02_06
- Potter, D., Mashburn, A., & Grissmer, D. (2013). The family, neuroscience, and academic skills: An interdisciplinary account of social class gaps in children’s test scores. Social Science Research, 42(2), 446–464. doi:https://doi.org/10.1016/j.ssresearch.2012.09.009
- Preston, N., Magallon, S., Hill, L. J., Andrews, E., Ahern, S. M., & Mon-Williams, M. (2017). A systematic review of high quality randomized controlled trials investigating motor skill programmes for children with developmental coordination disorder. Clinical Rehabilitation, 31(7), 857–870. doi:https://doi.org/10.1177/0269215516661014
- Rebeiro, K., & Polgar, J. (1999). Enabling occupational performance: optimal experiences in therapy. Canadian Journal of Occupational Therapy, 66(1), 14–22.
- Rens, L., & Joosten, A. (2014). Investigating the experiences in a school-based occupational therapy program to inform community-based paediatric occupational therapy practice. Australian Occupational Therapy Journal. doi:https://doi.org/10.1111/1440-1630.12093
- Riddell, S., Tisdall, K., & Mulderrig, J. (2007). Literature review of educational provision for pupils with additional support needs. Practical Research for Education, 37(June), 65–74.
- Rosenblum, S., Goldstand, S., & Parush, S. (2006). Relationships among biomechanical ergonomic factors, handwriting product quality, handwriting efficiency, and computerized handwriting process measures in children with and without handwriting difficulties. American Journal of Occupational Therapy, 60(1), 28–39. doi:https://doi.org/10.5014/ajot.60.1.28
- Santangelo, T., & Graham, S. (2016). A comprehensive meta-analysis of handwriting instruction. Educational Psychology Review, 28(2), 225–265. doi:https://doi.org/10.1007/s10648-015-9335-1
- Schmidt, R. A., & Lee, T. D. (1988). Motor control and learning. Human Kinetics.
- Schoemaker, M. M., Niemeijer, A. S., Reynders, K., & Smits-Engelsman, B. C. M. (2003). Effectiveness of neuromotor task training for children with developmental coordination disorder: A pilot study. Neural Plasticity, 10(1–2), 155–163. doi:https://doi.org/10.1155/NP.2003.155
- Sirin, S. R. (2005). Socioeconomic status and academic achievement: A meta-analytic review of research. Review of Educational Research, 75(3), 417–453. doi:https://doi.org/10.3102/00346543075003417
- Smith-Zuzovsky, N., & Exner, C. E. (2004). The effect of seated positioning quality on typical 6- and 7-year-old children’s object manipulation skills. American Journal of Occupational Therapy, 58(4), 380–388. doi:https://doi.org/10.5014/ajot.58.4.380
- Smits-Engelsman, B., Vinçon, S., Blank, R., Quadrado, V. H., Polatajko, H., & Wilson, P. H. (2018). Evaluating the evidence for motor-based interventions in developmental coordination disorder: A systematic review and meta-analysis. Research in Developmental Disabilities, 74, 72–102. doi:https://doi.org/10.1016/j.ridd.2018.01.002
- Smits-Engelsman, B. C. M., Blank, R., & van der Kaay, A. C. (2013a). Efficacy of interventions to improve motor performance in children with developmental coordination disorder: A combined systematic review and meta‐analysis. Developmental Medicine and Child Neurology, 55(3), 229–237. doi:https://doi.org/10.1111/dmcn.12008
- Smits-Engelsman, B. C. M., Blank, R., & van der Kaay, A.-C. (2013b). Efficacy of interventions to improve motor performance in children with developmental coordination disorder: A combined systematic review and meta-analysis. Developmental Medicine and Child Neurology, 55(3), 229–237. doi:https://doi.org/10.1111/dmcn.12008
- Stephenson, E. A., & Chesson, R. A. (2008). ‘Always the guiding hand’: Parents’ accounts of the long-term implications of developmental co-ordination disorder for their children and families. Child: Care, Health and Development, 34(3), 335–343. doi:https://doi.org/10.1111/j.1365-2214.2007.00805.x
- Thomas, L., & Radimsky, C. (2013). NHS Wales award handwriting motorway. Retrieved March 12, 2019, from http://www.nhswalesawards.wales.nhs.uk/document/216997
- Troia, G. A., & Graham, S. (2003). Effective writing instruction across the grades: What every educational consultant should know. Journal of Educational and Psychological Consultation, 14(1), 75–89. doi:https://doi.org/10.1207/S1532768XJEPC1401_04
- Venetsanou, F., Kambas, A., Ellinoudis, T., Fatouros, I., Giannakidou, D., & Kourtessis, T. (2010). Can the movement assessment battery for children-test be the “gold standard” for the motor assessment of children with Developmental Coordination Disorder? Research in Developmental Disabilities, 32(1), 1–10. doi:https://doi.org/10.1016/j.ridd.2010.09.006
- Vygotsky, L. (1980). Mind in society: The development of higher psychological processes. Cambridge, MA: Harvard University Press.
- Wallen, M., Duff, S., Goyen, T.-A., & Froude, E. (2013). Respecting the evidence: Responsible assessment and effective intervention for children with handwriting difficulties. Australian Occupational Therapy Journal, 60(5), 366–369. doi:https://doi.org/10.1111/1440-1630.12045
- Waterman, A. H., Havelka, J., Culmer, P. R., Hill, L. J. B., & Mon-Williams, M. (2014). The ontogeny of visual-motor memory and its importance in handwriting and reading: A developing construct. Proceedings of the Royal Society B: Biological Sciences, 282, 20140896. doi:https://doi.org/10.1098/rspb.2014.0896
- Weintraub, N., Yinon, M., Hirsch, I. B.-E., & Parush, S. (2009). Effectiveness of sensorimotor and task-oriented handwriting intervention in elementary school-aged students with handwriting difficulties. OTJR: Occupation, Participation, Health, 29(3), 125–134. doi:https://doi.org/10.3928/15394492-20090611-05
- Williams, M. S., & Shellenberger, S. (1996). How does your engine run? A leader’s guide to the alert program for self regulation. Albuquerque: TherapyWorks Inc.
- Eddy, L. H., Wood, M. L., Shire, K. A., Bingham, D. D., Bonnick, E., Creaser, A., … & Hill, L. J. (2019). A systematic review of randomized and case‐controlled trials investigating the effectiveness of school‐based motor skill interventions in 3‐to 12‐year‐old children. Child: care, health and development, 45(6), 773-790.
- World Health Organisation. (2001). International classification of functioning, disability and health: ICF. Geneva, Switzerland: Author. doi:https://doi.org/10.1055/s-0033-1338283
- Wright, J., Small, N., Raynor, P., Tuffnell, D., Bhopal, R., Cameron, N., … West, J. (2013). Cohort profile: The born in bradford multi-ethnic family cohort study. International Journal of Epidemiology, 42(4), 978–991. doi:https://doi.org/10.1093/ije/dys112
- Zwicker, J. G., & Hadwin, A. F. (2009). Cognitive versus multisensory approaches to handwriting intervention: A randomized controlled trial. OTJR: Occupation, Participation, Health, 29(1), 40–48. doi:https://doi.org/10.3928/15394492-20090101-06