
ABSTRACT
Cognitive models of post-traumatic stress disorder (PTSD) suggest maladaptive appraisals play a central role in the aetiology of this disorder. The current meta-analysis sought to provide a comprehensive, quantitative examination of the relationship between maladaptive appraisals and PTSD. One-hundred and 35 studies met study inclusion criteria and were subject to random effects meta-analysis. A large effect size was found for the relationship between appraisals and PTSD (r = 0.53, 95% CI = 0.51–0.56, k = 147), albeit with significant heterogeneity. In studies using only the Posttraumatic Cognitions Inventory or Child Post-traumatic Cognitions Inventory, the effect size remained large (r = 0.56; k = 104). In adults, appraisals about the self had a large effect size (r = 0.61), appraisals about the world had a medium effect size (r = 0.46) and self-blame appraisals had a small effect size (r = 0.28). In child/adolescent studies, large effect sizes were found for both ‘fragile person in a scary world’ and ‘permanent and disturbing change’ appraisals (r = 0.54 and r = 0.60, respectively). The effect size remained large in prospective longitudinal studies up to one year after trauma. There was no moderation effect for civilian vs military populations, questionnaire vs interview measures of PTSD, single vs multiple trauma exposure, or intentional vs unintentional trauma. The main effect size estimate was robust to sensitivity analyses concerning statistics used, study quality and outliers. These findings are consistent with the strong role for maladaptive appraisals in the aetiology of PTSD proposed by cognitive models. In particular, the role of self-appraisals in adults was highlighted. Avenues for future research include more studies in child, multiple trauma and military populations and longer-term follow up studies.
HIGHLIGHTS
• We examined the strength of the relationship between maladaptive appraisals and symptoms of PTSD in trauma-exposed adult and child populations.• One-hundred and 47 independent effect sizes from 135 studies (N=29,812 participants) were included.• A large effect size was found (r=0.53, 95% CI = 0.51-0.56).• In adults, appraisals about the self were more strongly related to PTSD than appraisals about the world, or self-blame.• Trauma-related appraisals are comparatively under-studied in military populations.• The effect size remained large up to 6 months following trauma and was medium at 12 months.
Los modelos cognitivos del trastorno de estrés postraumático (TEPT) sugieren que las valoraciones desadaptativas desempeñan un rol central en la etiología de este trastorno. El presente metanálisis buscó proporcionar un examen exhaustivo y cuantitativo de la relación entre las valoraciones desadaptativas y el TEPT. Ciento treinta y cinco estudios cumplieron con los criterios de inclusión y fueron sujeto de un metanálisis de efectos aleatorios. Se encontró un gran tamaño del efecto para la relación entre las valoraciones y el TEPT (r = 0,53, IC del 95% = 0,51-0,56, k = 147), aunque con una heterogeneidad significativa. En los estudios que utilizaron solo el Inventario de Cogniciones Postraumáticas o el Inventario Infantil de Cogniciones Postraumáticas, el tamaño del efecto se mantuvo grande (r = 0.56; k = 104). En adultos, las valoraciones sobre el sí mismo tuvieron un tamaño de efecto mayor (r = 0,61), las valoraciones sobre el mundo tuvo un tamaño de efecto medio (r = 0,46) y las valoraciones auto-culpables tuvieron un tamaño de efecto pequeño (r = 0,28). En estudios con niños/adolescentes, se encontraron mayores tamaños de efecto para las valoraciones de ‘persona frágil en un mundo aterrador’ y ‘cambio permanente y perturbador’ (r = 0.54 y r = 0.60, respectivamente). El tamaño del efecto se mantuvo grande en estudios longitudinales prospectivos hasta un año después del trauma. No hubo efecto de moderación para las poblaciones civiles frente a las militares, las medidas de cuestionario versus a la entrevista del trastorno de estrés postraumático, la exposición trauma individual versus la exposición múltiple o el trauma intencional versus al no intencional. La estimación del tamaño del efecto principal fue robusta para los análisis de sensibilidad relativos a las estadísticas utilizadas, la calidad del estudio y los valores atípicos. Estos hallazgos son consistentes con el fuerte papel de las valoraciones desadaptativas en la etiología del TEPT propuesto por los modelos cognitivos. En particular, se destacó el papel de las autovaloraciones en adultos. Las vías para futuras investigaciones incluyen más estudios en niños, traumas múltiples y poblaciones militares y estudios de seguimiento a más largo plazo.
创伤后应激障碍(PTSD)的认知模型表明,适应不良的评估在其病因学中起着重要作用。本元分析旨在对适应不良评估与创伤后应激障碍之间的关系进行全面定量的检查。有135项研究符合研究纳入标准,并进行了随机效应元分析。 评估和创伤后应激障碍之间的关系,有较大的效应量(r = 0.53,95%CI = 0.51-0.56,k = 147),尽管表现出了显著的异质性。在使用创伤后认知量表或儿童创伤后认知量表的研究中,效应量保持较大(r = 0.56; k= 104)。 在成人中,对自我的评价具有较大的效应量(r = 0.61),对世界的评价具有中等效应量(r = 0.46),自责评价具有小的效应量(r = 0.28)。在儿童/青少年中,发现‘恐怖世界中的脆弱个体’和‘永久性和令人不安的变化’评估(分别为r = 0.54和r = 0.60)的效应量大。在创伤后长达一年的前瞻性纵向研究中,效应量仍然保持很大。平民vs军队群体,PTSD问卷调查vs访谈测量,单次vs多次创伤暴露,或故意vs非故意创伤都么有调节作用。针对使用的统计方法,研究质量和异常值进行敏感性分析,发现主效应量估计稳健。这些发现呼应了认知模型提出的适应不良评估在创伤后应激障碍病因学中的强大作用。特别强调了自我评估在成人中的作用。未来研究的途径可进行更多关于儿童,多次创伤和军人群体的研究以及进行长期随访研究。
1. Introduction
Post-traumatic stress disorder (PTSD) is a debilitating psychological disorder arising after the direct or indirect experience of a traumatic event. Traumatic events are common, with 60–90% of individuals being exposed to at least one traumatic event during their lifetime (Kilpatrick et al., Citation2013). However, lifetime prevalence estimates of PTSD are 3.9% in adults (Koenen et al., Citation2017) and 5% in children (Merikangas et al., Citation2010). Most individuals recover from traumatic events without intervention within six months (Foa & Riggs, Citation1995; Hiller et al., Citation2016). Research has therefore concentrated on identifying risk factors for the development of PTSD, with much research attention over the past 15 years being given to the role of appraisals.
Appraisals have come to be central components of many theoretical models of emotion (Dalgleish, Citation2004b) and several cognitive models of PTSD give appraisals a central role in explaining individual differences in PTSD outcomes (e.g. Brewin, Dalgleish, & Joseph, Citation1996; Dalgleish, Citation2004a; Ehlers & Clark, Citation2000; Foa & Riggs; Citation1995). The cognitive model described by Ehlers and Clark (Citation2000) has had considerable influence. In this model, disturbance in autobiographical memory, maladaptive appraisals and poor coping strategies create a sense of current threat that is central to the development and maintenance of PTSD. The model proposes that highly threatening appraisals related to the trauma and its aftermath may be developed, such as the overgeneralisation of danger (‘bad things always happen to me’) or judgements of their own actions (‘I should have coped better’). Appraisals of trauma sequelae are also hypothesised to be central to the maintenance of persistent negative emotions. These may relate to specific symptoms (e.g. intrusions as a sign they are ‘going crazy’) or their future (‘I will never be the person I was again’). In addition to directly generating negative affect, negative appraisals are seen in this model as encouraging the use of maladaptive behavioural strategies and cognitive processing styles that further promote the maintenance of PTSD.
Most cognitive models of PTSD include some role for appraisals or personal meaning in the development and maintenance of this disorder. Commonalities amongst the theories seem to be beliefs that the world is a dangerous place and the self as incompetent or somehow to blame for the trauma. Several authors have made the case for applying such models to PTSD in children and adolescents (hereafter just children; Alisic, Zalta & Van Wesel, Citation2014).
Many studies have shown that maladaptive appraisals about the self, the world and self-blame are risk factors for PTSD. Cross-sectional studies have found measures of maladaptive appraisals, such as the Post-Traumatic Cognitions Inventory (PTCI; Foa, Ehlers, Clark, Tolin, & Orsillo, Citation1999) and Child Post-Traumatic Cognitions Inventory (CPTCI; Meiser-Stedman et al., Citation2009), to relate strongly with PTSD symptoms in children (e.g. Diehle, de Roos, Meiser-Stedman, Boer, & Lindauer, Citation2015; Mitchell, Brennan, Curran, Hanna, & Dyer, Citation2017) as well as adults (e.g. Duffy, Bolton, Gillespie, Ehlers, & Clark, Citation2013). Maladaptive appraisals have been shown to prospectively predict PTSD symptom severity and the maintenance of PTSD symptoms in adults (e.g. Halligan, Michael, Clark, & Ehlers, Citation2003) and children (e.g. Bryant, Salmon, Sinclair, & Davidson, Citation2007). Maladaptive appraisals have also been found to predict severity of acute stress reactions in the first four weeks after a traumatic event (e.g. Nixon & Bryant, Citation2005). This suggests that appraisals may be particularly important in the initial stages following trauma, and could play a role in the onset of post-traumatic stress reactions.
Some other studies have shown a much more limited role for maladaptive appraisals (e.g. Kangas, Henry, & Bryant, Citation2005). For example, negative appraisals about the self and the world were found to predict a significant amount of variance in PTSD symptoms in the initial period following a stroke but no additional variance in PTSD symptoms at 3 months follow up (Field, Norman, & Barton, Citation2008). It is possible that appraisals play a different role at different time points following trauma.
The PTSD field has seen the development of numerous self-report measures for the assessment of maladaptive or negative post-traumatic appraisals. Measures such as the PTCI and CPTCI were developed with specific cognitive or cognitive-behavioural accounts of PTSD in mind (i.e. Ehlers & Clark, Citation2000; Foa et al., Citation1999). Other measures have been developed in response to different models of PTSD, for example, the World Assumptions Scale (Janoff-Bulman, Citation1989).
Previous meta-analyses of risk factors for PTSD in trauma-exposed adults have found pre-traumatic risk factors to have smaller effect sizes (smaller than r = 0.20) than peri-traumatic (r = 0.23–0.35) or post-traumatic risk factors (r = 0.29–0.40; Brewin, Andrews, & Valentine, Citation2000; Ozer, Best, Lipsey, & Weiss, Citation2003). In these studies, the effect size varied depending on the population being studied (e.g. military versus civilian samples) and methodology (e.g. prospective versus retrospective study design). Meta-analyses conducted in child and adolescent studies also found the largest effect sizes for peri-traumatic and post-traumatic risk factors (Cox, Kenardy, & Hendrikz, Citation2008; Trickey, Siddaway, Meiser-Stedman, Serpell, & Field, Citation2012). These studies, however, did not explore the role of maladaptive appraisals. Mitchell et al. (Citation2017) did explore appraisals and PTSD in children and adolescents, and performed a meta-analysis of 11 studies, finding a large effect size (r = 0.63, 95% CI = 0.58–0.68) for this association. To date, however, no quantitative synthesis has been carried out to summarise the role of maladaptive appraisals in PTSD in both adults and children which includes a wide range of measures of maladaptive appraisals. Given the theoretical importance of maladaptive appraisals in psychological models of PTSD, it is important to summarise the literature in this area to obtain a more accurate estimate of the effect size of the relationship between appraisals and PTSD symptoms. The seemingly crucial role played by the modification of appraisals in the treatment of PTSD (Jensen, Holt, Ormhaug et al., Citation2018; Kleim et al., Citation2013) and the recent addition of negative cognitions to diagnostic criteria for PTSD (American Psychiatric Association, Citation2013) underlines the clinical significance of this research.
Here we additionally explore variables that moderate the relationship between maladaptive appraisals and PTSD. Such moderation analyses will allow for a thorough empirical evaluation of the generalisability and methodological robustness of the research supporting an association between appraisals and PTSD. A key moderator when exploring the impact of psychological mechanisms in developing populations is age. Children’s capacity to appraise a traumatic event will be influenced by their developmental stage and cognitive ability (Salmon & Bryant, Citation2002). In particular, a lack of knowledge and experience in young children will mean they have less detail in their schematic models about themselves and the world. This lack of detail about the causes and consequences of emotional events means young children may have fewer cognitive and emotional tools to appraise emotional events. The relationship between maladaptive appraisals and PTSD may also vary according to context, in particular, the type of traumatic event, the intentionality of the trauma, or whether or not the trauma was a single event or multiple event trauma. For example, individuals who have suffered sexual assaults have been shown to score more highly on the PTCI, than individuals involved in other traumatic events (Startup, Makgekgenene, & Webster, Citation2007). Previous meta-analyses have reported that study design, population (civilian vs military) and measures used moderately the effect sizes found (Brewin et al., Citation2000; Ozer et al., Citation2003; Trickey et al., Citation2012). A particular aim of the current study was to compare different subtypes of maladaptive appraisals and the relative strength of their relationship with PTSD, in particular the sub-scales of the PTCI (self, world and self-blame appraisals) and the CPTCI (‘permanent and disturbing change’ and ‘fragile person in a scary world’ appraisals). This may shed some light into which appraisals might be most significant risk factors for PTSD and therefore important to target clinically.
It is also important to explore the effect size of the relationship between maladaptive appraisals and PTSD symptoms at different time points following the trauma. This will help to establish whether appraisals have a role in the onset of post-traumatic stress symptoms, consider whether the association between appraisals and PTSD weakens over time, and also test the hypothesis that appraisals predict subsequent PTSD (i.e. lending support to an aetiological role for appraisals).
In summary, the primary aim of the current study was to systematically evaluate and summarise the existing PTSD literature to estimate the strength of the relationship between trauma-related maladaptive appraisals and symptoms of PTSD. The secondary aim of the study was to examine putative theoretical, population and methodological influences on the relationship between appraisals and PTSD, including the comparative strength of the relationship of different subtypes of maladaptive appraisal (self, world and self-blame) with PTSD symptoms, and the change in the strength of the relationship over time.
2. Methods
2.1. Registration
The current meta-analysis was prospectively registered with PROSPERO on 14 September 2015 (CRD42015026224).
2.2. Search strategy
Studies were selected following a systematic search for relevant publications dating from 1980 (when PTSD was first introduced in the DSM) in PsycINFO, MEDLINE, CINAHL and PILOTS (Published International Literature on Traumatic Stress; US Department of Veterans Affairs, 2015), completed by the 3 February 2017. Reference sections of relevant book chapters and review articles were screened, a citation search for the PTCI and CPTCI was carried out and the Journal of Traumatic Stress was searched to identify further relevant literature. Further unpublished or ‘grey’ literature was sought by searching the databases OpenGrey, Dissertation Abstracts International and the British Library e-theses Online Service. Researchers who were first authors on two or more studies included in the meta-analysis were contacted via email to request any unpublished data. Two researchers provided data which extended and overlapped with papers they had published.
Search terms were: PTSD OR Posttraumatic stress OR Posttraumatic stress OR Posttraumatic stress OR traumatic neurosis AND cognitive appraisal* OR appraisal* OR negative cognition* OR ‘negative belief’ OR “posttraumatic cognition* OR misappraisal*. To be included in the analysis, studies were required to meet all of the following inclusion criteria:
Included participants exposed to trauma, as defined by DSM-5 PTSD Criterion A (American Psychiatric Association, Citation2013);
Included a validated measure of PTSD/ASD or PTSD/ASD severity that considers intrusions, avoidance and hyperarousal, which demonstrates adequate reliability and validity via publication of their psychometric properties in a peer-reviewed journal; and
Included a measure of trauma-relevant maladaptive appraisals, operationally defined as how you see yourself, the world or your symptoms in the aftermath of trauma as well as self-blame or other trauma attributions.
The following exclusion criteria were applied:
Review article, case study, qualitative study or book chapter;
Treatment trial or sample involving only those who have a PTSD diagnosis. This is because the amount of variability in the sample for PTSD severity would be reduced in treatment trials as all individuals would have high levels of symptomatology due to having been diagnosed with PTSD. We did not exclude universal preventative treatment trials as these studies would comprise a wide spectrum of PTSD responses, allowing for a valid examination of whether PTSD severity was associated with appraisals.
Not published in English;
Dissertations where the full text was not available after contacting the authors and where the abstract did not provide sample size and effect size;
Measures only the appraisal of a threat to life during the traumatic event. This has been addressed in previous meta-analyses (Cox et al., Citation2008; Ozer et al., Citation2003; Trickey et al., Citation2012) and did not fit our operational definition of post-trauma appraisals as outlined above. Moreover, it may be argued that peri-traumatic threat reflects an adaptive response, i.e. they accurately reflected threat during a trauma, and may have served an important function in contributing to the body’s normal ‘flight or fight’ response.
Measures appraisals prior to trauma or at the time of trauma rather than in the aftermath of trauma (e.g. appraisal of treatment, appraisal of the traumatic experience as it was happening).
Measures coping self-efficacy or appraisal of ability to cope with the practical demands of life after trauma. These were excluded as they were judged to be insufficiently related to the trauma-related appraisals of interest here (i.e. relating to self, the world or PTSD symptoms).
Data set previously included in another study. Estimates were taken from the peer reviewed journal article or the largest sample where more than one study or dissertation used the same data set;
Study does not provide an effect size, nor sufficient data to calculate an effect size even after contacting authors;
Data from individuals with PTSD were combined with data of individuals with other diagnoses (e.g. depression) but not PTSD and it was not possible to look at the groups separately; or
Participants had a traumatic brain injury.
2.3. Screening method
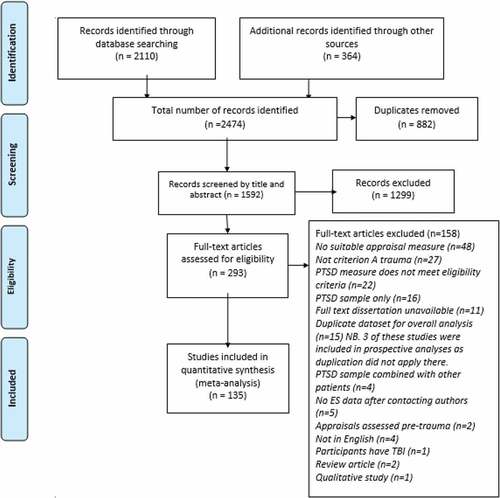
The screening is outlined in the PRISMA diagram in . Titles and abstracts were reviewed by GG. SS reviewed all excluded abstracts. Where disagreements occurred, studies were included and put through to the next stage. The full text of eligible studies were then independently reviewed by GG and SS or JD. Where disagreements occurred a final decision about inclusion was made by the last author (RMS).
Figure 1. PRISMA diagram outlining results from the study selection process.
2.4. Data extraction
Information was extracted and coded by GG. Twenty per cent of studies were double-coded by SS. Agreement between GG and SS on the items in the data extraction form was 91%. Where disagreements occurred, the data was double-checked by GG in discussion with RMS.
Pearson’s zero-order correlation coefficient (r) was the primary estimate of effect size. Where other measures of effect size data were given, these were converted into Pearson’s r. If insufficient data was given to calculate an effect size, study authors were contacted. If authors were unable to provide the relevant information or did not respond within two weeks of being contacted then the study was excluded. If studies reported separate effect sizes for appraisal subscale scores as well as the total scores, subscale scores were used in the subscale analyses, but only the effect size for the total score was used to estimate the overall effect size. When studies reported effect sizes for multiple subscales or multiple items without the total score, then these effect sizes were combined for use in the main analysis.
Multiple effect sizes were extracted for prospective studies to explore the change in the relationship over time. In the main meta-analysis, the effect size reported for the first concurrent time point was extracted. If no concurrent data were available, then the first prospective time point was used.
2.5. Quality assessment framework
A quality assessment tool was developed for the purposes of the current study (available from the first author) as no individual quality assessment scales were found to be recommended in the literature for use with cross-sectional or prospective studies of risk factors (Jarde, Losilla, & Vives, Citation2012). In developing the assessment tool, existing checklists were reviewed and the elements relevant to the current study were adapted for inclusion. These checklists included the Quality Appraisal Checklist for Studies Reporting Correlations and Associations (NICE, Citation2012), the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Von Elm et al., Citation2007), the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (National Heart Lung and Blood Institute, Citation2014) and other relevant critical appraisal tools published in the literature (e.g. Hoy et al., Citation2012; Munn, Moola, Riitano, & Lisy, Citation2014; Shamliyan et al., Citation2011).
Threats to internal and external validity relevant to the current meta-analysis included: the representativeness of the sample; appropriate recruitment and sampling; non-response bias and drop-out rates and the reliability of appraisal measures. Studies were rated low, medium or high quality depending on the number of questions answered as being at ‘low risk’ of bias. Studies were judged to be of high quality if they scored ‘low risk’ on 4 or 5 of the 5 items; medium quality if they scored ‘low risk’ on 2 or 3 items; and low quality if they scored ‘low risk’ on 0 or 1 of the items. Quality assessment was performed by GG, and 20% of studies were double-coded by SS or JD. Percentage agreement for the individual items in the quality assessment checklist was 80%. The weighted Kappa was 0.52 (‘moderate’) for overall quality rating.
2.6. Data synthesis
Random effects meta-analyses were performed using Comprehensive Meta-Analysis (Borenstein, Hedges, Higgins, & Rothstein, Citation2006). Hedges’ method (Hedges & Olkin, Citation1985) was used to calculate an estimate of population effect size. R values were transformed into a Fisher’s Z score for use in the analysis and then back-transformed to r for interpretation. Estimates of heterogeneity were calculated, using the Q statistic and the I2 statistic. The degree of heterogeneity was classified as ‘low’ (25%), ‘medium’ (50%) or ‘large’ (75%; Higgins, Thompson, Deeks, & Altman, Citation2003).
2.7. Subgroup and sensitivity analyses
When planning this review we decided that moderator analyses were only be undertaken if 10 or more studies included data relevant to a given analysis. We also identified variables at this stage that we wished to examine as moderators. Putative a priori methodological moderator variables were study design, publication status, measure of PTSD, administration of PTSD measure, administration of appraisal questionnaire, appraisal measure, and when PTSD symptoms were measured. Putative study population moderator variables were civilian versus military sample and age of the population (child/adolescent vs. adult). Putative trauma characteristics moderator variables were trauma type (accident, illness or injury; combat/war exposure; interpersonal violence/sexual abuse; natural/human disaster), single trauma (e.g. road traffic accident) vs multiple trauma (e.g. domestic abuse), and intentional (e.g. assault) vs. unintentional trauma (e.g. earthquake). Not all studies provided data on each moderator variable; numbers of studies included for each moderator variable are shown in . Subgroup analyses were performed if there were 2 studies or more in each subgroup (Cuijpers, Citation2016). In order to guard against making Type I errors (finding an effect when none exists; Higgins & Thompson, Citation2004) the Holm method was used to adjust the level of significance for moderator analyses (Holm, Citation1979). No power calculations were undertaken.
Table 1. Results from overall and subgroup meta-analyses.
Results of subgroup analyses showed a significant amount of heterogeneity was accounted for by the measure of maladaptive appraisals. In order to explore subgroup analyses without the confound of maladaptive appraisal measure blurring the results, the overall meta-analysis was repeated for studies using the PTCI or CPTCI only. These measures were selected as they are well validated and the most widely used appraisal measures. Moreover, separate meta-analyses were carried out on studies that reported effect sizes for the PTCI subscales of self, world and self-blame in adults, or the CPTCI subscales of ‘fragile person in a scary world’ and ‘permanent and disturbing change’ in children.
A separate meta-analysis was performed on prospective studies only. Studies were included in this analysis if they assessed maladaptive appraisals within one month of a trauma and reported PTSD two to four months, six months or 12 months post-trauma, where there was at least one month between appraisal assessment and assessment of PTSD. Some studies reported data at more than one follow-up time. Given that only one effect size can be extracted from each study (Borenstein, Hedges, Higgins, & Rothstein, Citation2009), three separate random-effects meta-analyses were performed for each of the time points to enable all studies to be included.
Sensitivity analyses were conducted to establish whether the findings were influenced by the decisions made in the process of obtaining them (Borenstein et al., Citation2009). These excluded studies in which the beta value was imputed in place of r, low-quality studies and outliers. Studies whose 95% confidence interval did not overlap with the 95% confidence interval of the pooled effect size were considered to be outliers (Cuijpers, Citation2016).
2.8. Publication bias
Funnel plots were used to graphically explore publication bias. Egger’s test of the intercept (Egger, Davey Smith, Schneider, & Minder, Citation1997) and Duval and Tweedie’s trim and fill method (Duval & Tweedie, Citation2000) were used as further estimates of publication bias.
3. Results
3.1. Search results
Overall, 2474 studies were identified and 135 met inclusion criteria (see ). Supplementary Table 1 provides references for all full-text studies reviewed and the reasons for inclusion or exclusion.
3.2. Study characteristics
Supplementary Table 3a and b describe the characteristics of all studies included in the meta-analysis. Of the 135 included studies, there were 147 independent effect sizes extracted. The total number of participants included in the main meta-analysis was 29,812. Supplementary Table 2 describes each appraisal measure included in the review.
3.3. Meta-analysis of all eligible data
A random-effects meta-analysis of 147 independent effect sizes from 135 studies indicated a large effect size for the relationship between maladaptive appraisals and PTSD symptoms, r= .53, 95%CI = .51-.56. There was significant heterogeneity in these relationships, Q= 1382.31, df= 146, p < 0.0001, I2= 89.4%. Effect sizes for each individual study are reported in Supplementary Table 4.
3.4. Subgroup and sensitivity analyses
Subgroup and sensitivity analysis results are shown in . Significant heterogeneity was accounted for by several variables. Child studies showed a significantly larger effect size than adult studies, but both effects were large (i.e. >.5). Unpublished studies yielded a larger effect size than published studies. However, both the age-related and publication status moderator analyses ceased to be significant when a Holm correction for multiple comparisons was applied. Interview measures of appraisal had a significantly smaller effect size than self-report measures, but only three studies utilised an interview format for assessing appraisals and these studies comprised relatively few participants. Individual appraisal measure also explained a significant amount of heterogeneity. No heterogeneity was explained by population (civilian vs military), study design (cross-sectional vs prospective); the validity of appraisal measure; PTSD measure administration (interview vs questionnaire), single vs multiple trauma; traumatic event type or time since trauma. Given the small number of participants in the military and multiple trauma populations and the unpublished studies, some caution should be exercised when considering these findings. The main effect size estimate was robust to the sensitivity analyses (see ).
3.5. Meta-analysis of PTCI/CPTCI studies only
Given the large amount of heterogeneity accounted for by measure of appraisals, the meta-analysis was repeated with just the studies that used the PTCI and CPTCI (k= 104). The overall analysis showed a large effect size, r= .56, 95%CI = .53-.59. Heterogeneity was high (I2= 86.2%). See Supplementary Table 5 for the contribution of each study to the overall effect size. Subgroup and sensitivity analysis results are given in . There was a significant difference between child and adult studies, with child studies having a significantly larger effect size than adult studies, though both effect sizes would still be considered large. Moreover, when a Holm correction for multiple comparisons was applied this relationship ceased to be significant. No heterogeneity was explained by population (civilian vs military), study design (cross-sectional vs longitudinal), PTSD measure type (continuous vs dichotomous), PTSD measure administration (interview vs self-report), single vs multiple trauma, traumatic event type or time since trauma. As noted above, it should be stressed that some moderator analyses comprised relatively small numbers of participants or studies. The overall effect size remained large in all sensitivity analyses.
Table 2. Table of subgroup analysis and sensitivity analysis results for ptci and cptci studies only.
3.6. Comparing subtypes of maladaptive appraisal
A series of meta-analyses were conducted looking at the sub-scales of the PTCI (in adults) and the CPTCI (in children). These analyses were planned, but given the large number (>5000) of children and adolescents who also completed the PTCI in three studies, further sub-scale analyses were undertaken for these studies. Results of these analyses are summarised in . Detailed subgroup and sensitivity results are given in Supplementary Tables 6–10; these do not include the child and adolescent PTCI studies as there was only three to consider, rendering sub-group analyses impossible. In adults the strongest relationship between maladaptive appraisals and PTSD symptoms was found for appraisals about the self (r= .61; 95%CI = .57-.64; I2= 84.9%), followed by world appraisals (r= .45; 95%CI = .41-.49; I2= 78.3%), and self-blame appraisals (r =.28; 95%CI = .24-.33; I2= 79.3%).
Figure 2. Forest plot showing effect sizes across different subtypes of maladaptive appraisal.
In children and adolescents, the relationships for PTCI self (r= 0.57; 95%CI = 0.42–0.68; I2= 97.7%), world (r= 0.43; 95%CI = 0.36–0.49; I2= 85.2%) and self-blame appraisals (r= 0.35; 95%CI = 0.26–0.44; I2= 66.8%) were broadly similar to the pattern for adults. The relationship between CPTCI-PC appraisals and PTSD symptoms (r= .59; 95%CI = .48-.67; I2= 86.7%) was slightly larger than CPTCI-SW appraisals (r= .53; 95%CI = .43-.62; I2= 84.3%). However, the confidence intervals of the effect sizes overlap, indicating that there is not a significant difference between these appraisal subtypes. Forest plots for each CPTCI sub-scale are presented in Supplementary Figures 1 and 2.
3.7. Meta-analysis of effect size between appraisals in the acute phase and PTSD at different time points
At 2–4 months following trauma, the effect size between maladaptive appraisals and PTSD symptoms was large (see ; r =.53, 95%CI = .44-.61; k= 9), with significant heterogeneity (Q = 45.45, df = 8, p < 0.0001; I2 = 82.4%). At 6 months the effect size remained large (r = .53, 95%CI = .48-.57, k = 13; Q = 21.60, df = 12, p < .04; I2= 44.43%). Only 3 studies reported prospective data about the correlation between maladaptive appraisals within 1 month of trauma and PTSD symptoms 12 months following trauma. Results showed a moderate effect size (r = .32, 95%CI = .13-.48, k = 3; Q = 22.51, df = 2, p < .001; I2 = 91.1%). The effect size was slightly lower at 12 months following trauma; however, given the low number of studies at 12 months and the overlapping confidence intervals for the effect sizes at the different time points, the difference may not be significant.
Figure 3. Forest plot showing effect size of relationship between acute appraisals and PTSD symptoms at 2–4 months, 6 months and 12 months since trauma.
3.8. Publication bias
shows the results of the tests of publication bias, which found little evidence of publication bias.
Table 3. Estimates of publication bias for all analyses.
Funnel plots indicated small studies may have been missing, suggesting a publication bias towards larger studies (see and ). Nevertheless, any publication bias that is in evidence does not affect the estimates of effect size seen; if anything, the use of Duval & Tweedie’s Trim and Fill method led to slightly larger effects (see ).
Figure 4. Funnel plot of standard error by Fisher’s Z for overall effect size (all studies included) showing the symmetry of the data in relation to publication bias.
Figure 5. Funnel plot of effect sizes exploring publication bias for meta-analysis of appraisals measured using only PTCI and CPTCI.
4. Discussion
The current meta-analysis aimed to summarise the literature on the relationship between measures of maladaptive appraisal used in the PTSD literature and PTSD symptoms. Results from pooling 147 independent effect sizes from 135 studies showed the effect size of the relationship between maladaptive appraisals and PTSD to be large (r= .53). When repeated including only the studies that used the PTCI or CPTCI, a similarly large effect was found (r= .56).
Analysis of putative moderators revealed few differences in this relationship. There were considerable differences in effect size between measures used to index trauma-related appraisals. We were therefore concerned that appraisal measure may have acted as a confound influencing other moderator analyses, particularly when sub-groups comprised small numbers of studies. Equally noteworthy was the lack of moderation effects for several variables, including study design (cross-sectional vs prospective), method for assessing PTSD, number of traumas, intentionality, trauma type and time when appraisals assessed. Since this pattern of results persisted even when restricting our studies to those which used the conceptually related PTCI or CPTCI, this suggests that appraisal measure did not have a major confounding effect. Moreover, effect sizes were robust to sensitivity analyses, i.e. when considering the impact of regression statistics, study quality or outliers. Minimal publication bias was apparent.
Comparison with previous meta-analyses of trauma-exposed populations is instructive. Within adults, the contrast between the effect of appraisals (r= .52, 95%CI = .49-.55) and other variables is stark. In their meta-analysis, Brewin et al. (Citation2000) synthesized data pertaining to a wide range of risk factors for PTSD. All risk factors were statistically significant, and the effect sizes ranged from r = .05 (race) to r = .40 (social support), a weaker relationship than that found in the current study for appraisals. In child studies, the effect size of r= .59 is comparable to the Mitchell et al., meta-analysis (r= 0.63, 95%CI = 0.58–0.68) and similar in size only to the relationship of thought suppression and PTSD in the Trickey et al. (Citation2012) meta-analysis. However, Mitchell et al. (Citation2017) omitted several studies included here (k= 11 vs k= 25).
4.1. Theoretical implications
The strength of the relationship between maladaptive appraisals and PTSD is consistent with claims made by cognitive theorists that such appraisals are strongly associated with PTSD (e.g. Dalgleish, Citation2004a; Ehlers & Clark, Citation2000; Foa & Riggs, Citation1995). This relationship was present in the earliest acute phase (albeit with relatively few studies) as well as later. Crucially, several prospective studies found that acute appraisals predicted PTSD months later, albeit slightly reduced at the one-year point.
The strong relationship between maladaptive appraisals and PTSD may raise the question of whether or not measures of maladaptive appraisals are simply proxy measures of PTSD symptoms. This is particularly pertinent given that negative cognitions are now part of the diagnostic criteria for the disorder in DSM-5. Indeed, some items on assessment tools of maladaptive appraisals relate to the interpretation of intrusions or reactions since the trauma, i.e. individuals can only score highly on such items if they are experiencing such symptoms. Nevertheless, other strands of research support a causative rather than epiphenomenal role for appraisals, e.g. pre-trauma maladaptive appraisals predicting PTSD following trauma (Bryant & Guthrie, Citation2007) and clinical trials evidence showing that change in appraisals mediates treatment responsiveness (e.g. Jensen et al., Citation2018; Kleim et al., Citation2013; Meiser-Stedman, Smith, McKinnon et al., Citation2017).
While not definitive proof of an aetiological role for appraisals in PTSD, this review has highlighted the different relationships between subtypes of appraisal and PTSD symptoms. In adults, negative appraisals about the self were significantly more strongly related to PTSD symptoms than negative appraisals about the world, followed by appraisals of self-blame. A similar picture was observed for adolescent samples that also used the PTCI. The moderate effect for world appraisals is perhaps surprising given the strong orientation towards external threat that the disorder is typically associated with, e.g. hypervigilance, exaggerated startle, behavioural avoidance. Cognitive models of PTSD place emphasis on the role of self-appraisals in maintaining the disorder. These findings strongly support this, and suggest that an internally focused sense of current threat (represented by maladaptive appraisals of the self) is more important than an externally focused sense of threat (represented by maladaptive appraisals of the world) in PTSD.
Although the relationship between self-blame and PTSD symptoms was significant, it was the subtype of appraisal with the weakest relationship with PTSD symptoms. Doubts have been raised about the importance of the self-blame subscale of the PTCI, with some studies showing no relationship between self-blame appraisals and PTSD (e.g. Beck et al., Citation2004) or even a negative correlation with PTSD (Startup et al., Citation2007). One contribution to this disparity could be the different conceptualisations of self-blame. For example, Janoff-Bulman (Citation1992) made a distinction between behavioural self-blame (attributing the cause of trauma to modifiable characteristics of oneself) and characterological self-blame (attributing the cause of events to one’s personality).
Attention should also be drawn to the strong relationship between maladaptive appraisals and PTSD symptoms in child and adolescent studies of PTSD. The age range of the participants in the included studies did not comprise very young children, and given the youngest mean age for the studies included in this meta-analysis was 9.9 years (the median age being 13.5 years), these studies would perhaps be better described as adolescent rather than child and adolescent. By this stage, youth will have developed at least some complex cognitive and emotional capacity enabling them to appraise traumatic situations and their responses (Salmon & Bryant, Citation2002), making the potentially distorting appraisals thought to contribute to the maintenance of PTSD possible. Another factor that might contribute to the large effect size found in the child studies could be the measures themselves used to assess appraisals. Both sub-scales of the CPTCI relate to self-appraisals. Moreover, the CPTCI does not contain a self-blame scale, which as seen in the adult studies has the weakest relationship with PTSD symptoms. While there was no difference between the CPTCI-SW and CPTCI-PC sub-scales, this may be attributable to the large proportion of items relating to the self in the CPTCI-SW subscale.
4.2. Clinical implications
The strong relationship found between maladaptive appraisals and PTSD symptoms across populations and types of trauma reinforces their role as an important target for psychological intervention. Maladaptive appraisals about the self could be a priority for treatment. Treatment such as trauma-focused CBT should focus on helping the person to recover a sense of themselves as a worthy person who is in control and not ‘damaged’.
It is noteworthy that trauma characteristics did not moderate the effect size in any of the analyses, i.e. appraisals play an important role regardless of whether the trauma was interpersonal or not, intended or not, or even involving single or multiple trauma. This pattern was consistent across subtypes of appraisal. Thus, while certain types of trauma exposure may seem particularly severe, it remains the case that the individuals’ appraisals remain a key aspect of their traumatic stress reaction. The finding in this study that appraisals within one month of trauma are related to PTSD symptoms up to one year after the traumatic event suggests that appraisals may be something to include in screening programmes for individuals recently exposed to trauma.
4.3. Suggestions for future research
Several populations have received little attention with respect to the role of appraisals. More studies in younger child populations are needed. Given the unique combination of high exposure rates and occupational demands placed on military personnel, this population would also warrant closer attention, especially given that a previous meta-analysis found that being in the military is a moderator of effect size for PTSD risk factors (Brewin et al., Citation2000). The current meta-analysis also highlighted a relative lack of studies exploring appraisals in multiple trauma populations. Additionally, only three studies looked at PTSD symptoms at a one-year follow-up. Research efforts should, therefore, be focused at longer-term follow up of trauma survivors, even beyond the 1-year mark, to explore the role of appraisals at extended time-points following trauma.
Future studies may wish to explore the role of self-blame in PTSD in more detail including characterological and behavioural self-blame. Future systematic reviews might also pay attention to the issue of specificity, i.e. are appraisals around trauma as strongly related to other psychopathology as to PTSD.
4.4. Limitations of the current study
This meta-analysis was limited by the large amount of heterogeneity in the included studies. Subgroup analyses revealed that a significant amount of variation could be explained by moderator variables identified a priori. However, several of our moderator analyses were limited by the small number of studies available, particularly for military and multiple trauma populations, and may have been influenced by other confounding variables, e.g. the measures used in certain types of study. It should be noted that the estimate of the effect size remained very similar when outliers were removed and heterogeneity reduced. Further subgroups such as gender may be useful to explore; however, it is important to note that some moderation effects (notably for the child vs adult comparison) were non-significant once adjustment was made for multiple comparisons. Future reviews may, therefore, need to choose moderator variables more selectively or seek to address a specific theoretical question concerning the relationship between appraisals and PTSD.
A further limitation was the lack of reporting of information in some of the studies. Several studies failed to report the time since the traumatic event occurred that assessments were taken. Many studies grouped individuals who had experienced different types of trauma together.
4.5. Conclusion
The current review found a large effect size for the relationship between maladaptive appraisal and PTSD. This relationship was robust to sensitivity analyses and publication bias. In adults, there was a clear difference between subtypes of maladaptive appraisal, with maladaptive appraisals about the self having the strongest relationship to PTSD symptoms, followed by appraisals about the world and finally self-blame. The relationship between maladaptive appraisals and PTSD was no weaker in child/adolescent studies than adult studies, with both age groups demonstrating a large effect (rs>.5). The relationship remained significant (if slightly weaker) up to 1 year following trauma. Maladaptive appraisals should be important targets for intervention in children, young people and adults. Further research is warranted in relation to several highly vulnerable groups (e.g. young children, military populations, those exposed to multiple traumas).
Supplemental Material
Download MS Word (340 KB)Disclosure statement
RMS was a co-author of one of the measures included in this review.
Supplementary materials
Supplementary data for this article can be accessed here
References
- Alisic, E., Zalta, A. K., van Wesel, F., Larsen, S. E., Hafstad, G. S., Hassanpour, K., & Smid, G. E. (2014). Rates of posttraumatic stress disorder in trauma-exposed children and adolescents: Meta-analysis. The British Journal of Psychiatry : The Journal of Mental Science, 204, 335–15.
- American Psychiatric Association. (2013). The diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: APA.
- Beck, J. G., Coffey, S. F., Palyo, S. A., Gudmundsdottir, B., Miller, L. M., & Colder, C. R. (2004). Psychometric properties of the Posttraumatic Cognitions Inventory (PTCI): A replication with motor vehicle accident survivors. Psychological Assessment, 16(3), 289–298.
- Borenstein, M., Hedges, L. V., Higgins, J. P., & Rothstein, H. R. (2006). comprehensive meta-analysis version 3. Engelwood, NJ: Biostat, Inc.
- Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to meta-analysis. Chichester, UK: John Wiley & Sons Ltd.
- Brewin, C., Andrews, B., & Valentine, J. (2000). Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consultulting and Clinical Psychology, 68(5), 748–766.
- Brewin, C., Dalgleish, T., & Joseph, S. (1996). A dual representation theory of posttraumatic stress disorder. Psychological Review, 103, 670–686.
- Bryant, R. A., & Guthrie, R. M. (2007). Maladaptive self-appraisals before trauma exposure predict posttraumatic stress disorder. Journal of Consulting and Clinical Psychology, 75(5), 812–815.
- Bryant, R. A., Salmon, K., Sinclair, E., & Davidson, P. (2007). A prospective study of appraisals in childhood posttraumatic stress disorder. Behaviour Research and Therapy, 45(10), 2502–2507.
- Cox, C. M., Kenardy, J. A., & Hendrikz, J. K. (2008). A meta-analysis of risk factors that predict psychopathology following accidental trauma. Journal for Specialists in Pediatric Nursing, 13(2), 98–110.
- Cuijpers, P. (2016). Meta-analyses in mental health research. Colofon: Vrije Universiteit Amsterdam.
- Dalgleish, T. (2004a). Cognitive approaches to posttraumatic stress disorder: The evolution of multirepresentational theorizing. Psychological Bulletin, 130(2), 228–260.
- Dalgleish, T. (2004b). The emotional brain. Nature Reviews. Neuroscience, 5(7), 583–589.
- Diehle, J., de Roos, C., Meiser-Stedman, R., Boer, F., & Lindauer, R. J. L. (2015). The Dutch version of the child posttraumatic cognitions inventory: Validation in a clinical sample and a school sample. European Journal of Psychotraumatology, 6, 26362.
- Duffy, M., Bolton, D., Gillespie, K., Ehlers, A., & Clark, D. M. (2013). A community study of the psychological effects of the omagh car bomb on adults. PLoS One, 8(9), e76618.
- Duval, S., & Tweedie, R. (2000). Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56(2), 455–463.
- Egger, M., Davey Smith, G., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ, 315(7109), 629–634.
- Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319–345.
- Field, E. L., Norman, P., & Barton, J. (2008). Cross-sectional and prospective associations between cognitive appraisals and posttraumatic stress disorder symptoms following stroke. Behaviour Research and Therapy, 46(1), 62–70.
- Foa, E., & Riggs, D. S. (1995). Posttraumatic stress disorder following assault: Theoretical considerations and empirical findings. Current Directions in Psychological Science, 4, 61–65.
- Foa, E. B., Ehlers, A., Clark, D. M., Tolin, D. F., & Orsillo, S. M. (1999). The Posttraumatic Cognitions Inventory (PTCI): Development and validation. Psychological Assessment, 11(3), 303–314.
- Halligan, S. L., Michael, T., Clark, D. M., & Ehlers, A. (2003). Posttraumatic stress disorder following assault: The role of cognitive processing, trauma memory, and appraisals. Journal of Consulting and Clinical Psychology, 71(3), 419–431.
- Hedges, L. V., & Olkin, I. (1985). Statistical methods for meta-analysis. London: Academic Press.
- Higgins, J. P. T., & Thompson, S. G. (2004). Controlling the risk of spurious findings from meta-regression. Statistics in Medicine, 23, 1663–1682.
- Higgins, J. P. T., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ: British Medical Journal, 327(7414), 557–560.
- Hiller, R. M., Meiser-Stedman, R., Fearon, P., Lobo, S., McKinnon, A., Fraser, A., & Halligan, S. L. (2016). Research review: Changes in the prevalence and symptom severity of child posttraumatic stress disorder in the year following trauma – A meta-analytic study. Journal of Child Psychology and Psychiatry, 57(8), 884–898.
- Holm, S. (1979). A simple sequentially rejective multiple test procedure. Scandinavian Journal of Statistics, 6, 65–70.
- Hoy, D., Brooks, P., Woolf, A., Blyth, F., March, L., Bain, C., … Buchbinder, R. (2012). Assessing risk of bias in prevalence studies: Modification of an existing tool and evidence of interrater agreement. Journal of Clinical Epidemiology, 65(9), 934–939.
- Janoff-Bulman, R. (1989). Assumptive worlds and the stress of traumatic events: Applications of the schema construct. Social Cognition, 7(2), 113–136.
- Janoff-Bulman, R. (1992). Shattered assumptions: Towards a new psychology of trauma. New York: Free Press.
- Jarde, A., Losilla, J., & Vives, J. (2012). Methodological quality assessment tools of non-experimental studies: A systematic review. Anales De psychologia/Annals of Psychology, 28(2), 617–628.
- Jensen, T. K., Holt, T., Mørup Ormhaug, S., Fjermestad, K. W., & Wentzel-Larsen, T. (2018). Change in posttraumatic cognitions mediates treatment effects for traumatized youth—A randomized controlled trial. Journal of Counseling Psychology, 65(2), 166–177.
- Kangas, M., Henry, J. L., & Bryant, R. A. (2005). Predictors of posttraurnatic stress disorder following cancer. Health Psychology, 24(6), 579–585.
- Kilpatrick, D. G., Resnick, H. S., Milanak, M. E., Miller, M. W., Keyes, K. M., & Friedman, M. J. (2013). National estimates of exposure to traumatic events and PTSD Prevalence using DSM-IV and DSM-5 criteria. Journal of Traumatic Stress, 26(5), 537–547.
- Kleim, B., Grey, N., Wild, J., Nussbeck, F. W., Stott, R., Hackmann, A., … Ehlers, A. (2013). Cognitive change predicts symptom reduction with cognitive therapy for posttraumatic stress disorder. Journal of Consulting and Clinical Psychology, 81(3), 383–393.
- Koenen, K., Ratanatharathorn, A., Ng, L., McLaughlin, K., Bromet, E., Stein, D., … Kessler, R. (2017). Posttraumatic stress disorder in the world mental health surveys. Psychological Medicine, 47(13), 2260–2274.
- Meiser-Stedman, R., Smith, P., Bryant, R., Salmon, K., Yule, W., Dalgleish, T., & Nixon, R. D. (2009). Development and validation of the Child posttraumatic Cognitions Inventory (CPTCI). Journal of Child Psychology and Psychiatry, 50(4), 432–440.
- Meiser‐Stedman, R., Smith, P., McKinnon, A., Dixon, C., Trickey, D., Ehlers, A., … Dalgleish, T. (2017). Cognitive therapy as an early treatment for posttraumatic stress disorder in children and adolescents: A randomized controlled trial addressing preliminary efficacy and mechanisms of action. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 58(5), 623–633.
- Merikangas, K. R., He, J., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., … Swendsen, J. (2010). Lifetime prevalence of mental disorders in u.s. adolescents: Results from the national comorbidity survey replication–Adolescent supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry, 49(10), 980–989.
- Mitchell, R., Brennan, K., Curran, D., Hanna, D., & Dyer, K. F. W. (2017). A meta-analysis of the association between appraisals of trauma and posttraumatic stress in children and adolescents. Journal of Traumatic Stress, 30(1), 88–93.
- Munn, Z., Moola, S., Riitano, D., & Lisy, K. (2014). The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. International Journal of Health Policy and Management, 3(3), 123–128.
- National Heart Lung and Blood Institute. (2014). Quality assessment tool for observational, cohort and cross-sectional studies. Retrieved from https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort
- NICE. (2012). Methods for the development of NICE public health guidance.
- Nixon, D. V., & Bryant, A. (2005). Are negative cognitions associated with severe acute trauma responses? Behaviour Change, 22(1), 22.
- Ozer, E. J., Best, S. R., Lipsey, T. L., & Weiss, D. S. (2003). Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin, 129(1), 52–73.
- Salmon, K., & Bryant, R. A. (2002). Posttraumatic stress disorder in children. The influence of developmental factors. Clinical Psychology Review, 22(2), 163–188.
- Shamliyan, T. A., Kane, R. L., Ansari, M. T., Raman, G., Berkman, N. D., Grant, M., … Tsouros, S. (2011). Development quality criteria to evaluate nontherapeutic studies of incidence, prevalence, or risk factors of chronic diseases: Pilot study of new checklists. Journal of Clinical Epidemiology, 64(6), 637–657.
- Startup, M., Makgekgenene, L., & Webster, R. (2007). The role of self-blame for trauma as assessed by the Posttraumatic Cognitions Inventory (PTCI): A self-protective cognition? Behaviour Research and Therapy, 45(2), 395–403.
- Trickey, D., Siddaway, A. P., Meiser-Stedman, R., Serpell, L., & Field, A. P. (2012). A meta-analysis of risk factors for posttraumatic stress disorder in children and adolescents. Clinical Psychology Review, 32(2), 122–138.
- Von Elm, E., Altman, D., Egger, M., Pocock, S. J., Gotzsche, P. C., & Vandenbroucke, J. P. (2007). The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. The Lancet, 370, 1453–1457.