
ABSTRACT
Vaccination has played a key role in reducing the health burden of COVID-19, however, concern has been raised worldwide regarding risk compensation, a process whereby feelings of security arising from being vaccinated may lead people to reduce their engagement in other protective behaviours.
We investigated whether vaccination led to risk compensation and whether this changed over time by conducting a repeated cross-sectional study at seven intervals over the initial months (February to September 2021) of the vaccine rollout in France. Participants (N = 14,003) completed an online survey measuring vaccination status, vaccination intention and engagement in four preventive behaviours: mask wearing, avoidance of physical contact, hand hygiene, and avoiding social gatherings. Risk compensation was measured indirectly by comparing levels of engagement in protective behaviours according to vaccination status, with those unvaccinated but intending to vaccinate serving as a baseline.
Risk compensation did not occur systematically and was mostly observed towards the end of the vaccine rollout for two of the four protective behaviours: avoiding social gatherings (in July and September for fully-vaccinated participants (Adjusted Odds Ratio (AOR) = .72, p = .045; AOR = .54, p = .022, respectively) and wearing a mask (those vaccinated with one dose, in September: AOR = .48, p = .029)). Our findings suggest that whilst unlikely to impede the overall effectiveness of public health campaigns, risk compensation nonetheless merits attention when designing informed, targeted public health messages and policy.
Introduction
Vaccination has been heralded as a major breakthrough in combatting the spread and health consequences of COVID-19 (World Health Organisation (WHO), Citation2021, Citation2022). However, concerns have been raised that the vaccination campaign may instil in people a sense of security, leading them to reduce or abandon other preventive measures crucial in fighting the disease (Trogen & Caplan, Citation2021; WHO, Citation2020; European Centre for Disease Control (ECDC), Citation2021b). This is referred to as risk compensation, whereby engagement in one protective behaviour generates a perception of reduced risk and results in compensatory risky behaviour (Brewer et al., Citation2007). The current research therefore sought to investigate whether COVID-19 vaccination resulted in risk compensation, and whether this changed over time, during the initial stages of the vaccine rollout in France. Understanding whether vaccination elicits risk compensation is important not only to the management of future waves of the current pandemic, but also to that of those to come.
Background
First proposed by Peltzman (Citation1975) in response to increased numbers of road accidents following the introduction of mandatory seat belt use in the US, risk compensation has since attracted research attention, with varied findings (Mantzari et al., Citation2020; Pless, Citation2016), in various health domains, such as bike (Esmaeilikia et al., Citation2019; Messiah et al., Citation2012) and snow sport helmet wearing (Haider et al., Citation2012), HIV prevention (Cassell et al., Citation2006; Eaton & Kalichman, Citation2007; Underhill, Citation2013), vaccination against HPV (Kasting et al., Citation2016; Mayhew et al., Citation2014) and Lyme disease (Brewer et al., Citation2007). Previous studies of more chronic health issues suggest that although unlikely to negate the overall benefit of a public health campaign, risk compensation may nonetheless lead people to lessen their commitment to other protective behaviours (eg. Cassell et al., Citation2006; Kacelnik & Kacelnik, Citation2022), critical in reducing disease spread (Bottemanne & Friston, Citation2021; Kassa & Ouhinou, Citation2015). This is of particular relevance when combatting the spread of COVID-19, which involves adherence to multiple protective measures.
Over the last decades, empirical investigations of risk compensation have presented contradictory evidence (Mantzari et al., Citation2020), attributable perhaps in part to varying definitions. Risk compensation, the Peltzman effect (Peltzman, Citation1975), risk homeostasis (Wilde, Citation1998), ‘risk thermostat’ (Kacelnik & Kacelnik, Citation2022, p. 2), moral licensing, rebound (Mantzari et al., Citation2020) and negative spillover effect (Nilsson et al., Citation2017; Thøgersen & Crompton, Citation2009) are often used interchangeably in the literature, but yet have different significations. For instance, drawing from the economic and environmental literature, Jia et al. (Citation2022), refer to the Peltzman Effect as being a negative or compensatory ‘behavioural spillover effect’ (Jia et al., Citation2022, p. 11). Brewer et al. (Citation2007) and Wilde (Citation1998), on the other hand, view risk compensation as resulting from a need to restore a certain ‘optimal’ level of perceived risk. They propose that ‘[. . .] people have stable preferences for a certain amount of risk and that the feeling of safety created by the initial preventive activity creates a surplus of risk that will be expended elsewhere by reducing protective actions’ (Brewer et al., Citation2007, p. 95), whereas other researchers, including ourselves, understand risk compensation as occurring when engagement in one protective behaviour leads to a reduction in others targeting the same goal (eg. Hedlund, Citation2000; Jørgensen et al., Citation2021).
According to Hedlund (Citation2000), risk compensation occurs when four elements are present: visibility, efficacy, motivation and control. Firstly, the intervention must be noticeable- this was true of COVID-19 vaccination at this time, as health passes attesting to an up-to-date COVID-19 vaccination schedule were constantly required to be shown, either in paper format or using a ‘phone app, to gain entry to public venues. Secondly, people must believe in the efficacy of the intervention. With vaccines in France at this time reported to be between 80-95% effective (Thompson et al., Citation2021), this criterion is also met. Thirdly, vaccination motivation was present, particularly due not only to the perceived health threat, but also to the social benefit induced by the introduction of a mandatory health pass to gain access to public venues. Finally, with increased vaccine availability as the rollout progressed, improved access to vaccination afforded people a high level of control over when and where they could be vaccinated, thereby satisfying the final criterion. It is therefore clear that the COVID-19 pandemic provides a setting in which risk compensation might thrive.
Whilst research into risk compensation and COVID-19 to date has focused largely on the effect of mask wearing on other preventive measures (eg. Aranguren, Citation2022; Jørgensen et al., Citation2021; Luckman et al., Citation2021), there is a relative lack of studies in Europe investigating whether vaccination elicits risk compensation. From outside Europe, neither a three-wave, longitudinal investigation in the US (Thorpe et al., Citation2022) nor a two-wave repeated cross-sectional Canadian study (Hall et al., Citation2022) found evidence of risk compensation following vaccination. Instead, vaccinated participants maintained other protective behaviours. The current research therefore addresses a gap in the literature by exploring whether, during the initial vaccine rollout in France, vaccination against COVID-19 led people to reduce their engagement in four protective behaviours: mask wearing, hand hygiene, avoidance of social gatherings and avoiding physical contact in social settings. Conducted monthly over the first seven months of the French vaccine campaign, the current research investigated how risk compensation evolved over time, providing important insights that may impact future public health messages and policy during an unfolding epidemic.
Mask wearing and risk compensation
Given the relative dearth of research into COVID-19 vaccination and risk compensation at the time of writing, investigations of the impact of mask wearing on subsequent protective measures provide important contextual insights for our research. Despite misgivings that mask wearing may lead to a reduction in other protective measures (ECDC, Citation2020; Martin et al., Citation2020; WHO, Citation2020), this is not consistently supported in the research literature. For instance, whereas neither Blanken et al. (Citation2021) nor Liebst et al.’s (Citation2022) observational study in the Netherlands found evidence risk compensation towards physical distancing as a result of mask wearing, Seres et al. (Citation2020) and Marchiori (Citation2020) found it led to increased social distancing in Germany and Italy respectively.
Contrastingly, using a quasi-experimental, online self-report survey, Jørgensen et al. (Citation2021) observed limited risk compensation towards physical distancing, but not towards hand hygiene or number of physical contacts, following the introduction of mandated mask wearing in Denmark. Similar findings were reported by Luckman et al. (Citation2021) in their online simulation in the UK, when either participant or stranger, or both, wore a mask. A further online simulation in France also found reduced physical distancing among virtual mask wearers, particularly those in low-risk areas and alarmingly, those testing positive to COVID-19 (Cartaud et al., Citation2020). Comparable results were obtained among German participants in a virtual supermarket simulation in which physical distancing was not respected among mask-wearers, particularly when effortful (Kroczek et al., Citation2022). In an observational field experiment in France, Aranguren (Citation2022) also found support for risk compensation towards physical distancing among mask-wearers, particularly men. Finally, risk compensation was observed towards stay-at-home orders, as measured by mobile location data, following mask mandates in the US (Yan et al., Citation2021).
Risk compensation & vaccination
Such evidence in support of risk compensation highlights the need to understand whether it is also elicited by vaccination, and how this may change over time, however research in this area at the time of writing remains scant. Buckell et al. (Citation2021), using a repeated, cross-sectional design in the UK, found that overall, physical distancing, public transport usage, avoidance of social gatherings, working at home and avoiding physical contact were unaffected by vaccination. However, when adjusted for mandated policies, protective behaviours changed according to general population vaccination rates, providing support for limited risk compensation at the population, rather than individual level, across all four countries: England, Scotland, Wales and Northern Ireland, despite different mandate timing in each country. In a national, three-stage study of the US vaccine rollout, Jia et al. (Citation2022) also found evidence of risk compensation over time towards all forms of preventive behaviours, particularly social distancing, following the first vaccine dose. Contrastingly, Sun et al. (Citation2022) found no evidence of risk compensation in an online study of healthcare workers in China, except for the type of gloves used. Rather, the frequency and duration of hand washing and wearing gloves and masks increased among vaccinated healthcare workers, especially those vaccinated early in the campaign. Similarly, in two separate, longitudinal studies in the UK, Desrichard et al. (Citation2022) and Wright et al. (Citation2022) observed no risk compensatory behaviour following vaccination, finding instead that participants were more inclined to increase preventive measures, with the exception of social distancing (although not systematically, Wright et al., Citation2022) and avoidance of crowded spaces (Desrichard et al., Citation2022). Desrichard and his colleagues observed this after both first and second vaccine doses.
Whilst not specifically measuring risk compensation, researchers concluded that reduced vaccine efficacy alone could not account for the resurgence of COVID-19 cases in Qatar (Tang et al., Citation2021) and India (eg. Iyengar et al., Citation2021; Jain et al., Citation2021; Juyal et al., Citation2021; Kamath & Nivea, Citation2021; Parikh et al., Citation2021; Thankappan & Nedumpillil, Citation2021), and that despite a successful vaccination campaign, human behaviour, through risk compensation, must have been partly to blame.
Implications for management
Given that several studies suggest that mask wearing may lead to a reduction in other COVID-19 preventive behaviours, also instrumental in reducing disease spread and overall health burden, it is somewhat surprising that few empirical studies to date have sought to investigate whether COVID-19 vaccination also elicits risk compensation, and whether this changes over time. The hitherto contrasting findings suggest that more is to be gleaned in the area of risk compensation, and it is hoped that the current study will not only shed light on this topic, but also that the insights gained will help target health messages and inform public policy during the unfolding epidemic, as well as prepare for those to come.
Methods
Data
Cross-sectional data were collected via seven online surveys conducted monthly, from February through to September 2021, during the initial vaccine rollout in France. Participants (N = 14,003) were French residents aged between 18 and 99 years of age. A stratified sampling method was used so that the sample was representative of the French population on age, sex, education, socio-economic status, occupation and region of residence, according to the 2016 National Institute of Statistics and Economic Studies census (INSEE, Citation2017). The sample size for each survey wave was approximately 2,000. This sample size was chosen in order to obtain a maximum margin of error plus or minus two percentage points, with a 95% confidence interval for the behavioural measures. The study was conducted in compliance with the French national guidelines for ethical research in the social and human sciences. The research was declared to the EHESP School of Public Health Office for Personal Data Protection (Rennes, France) [Reference: MR 2510110520], and approved by the ethics committee of the University Hospital Institute, Méditerranée Infection (Marseille France) [Decision No. 2020-022]. Informed consent was obtained from participants.
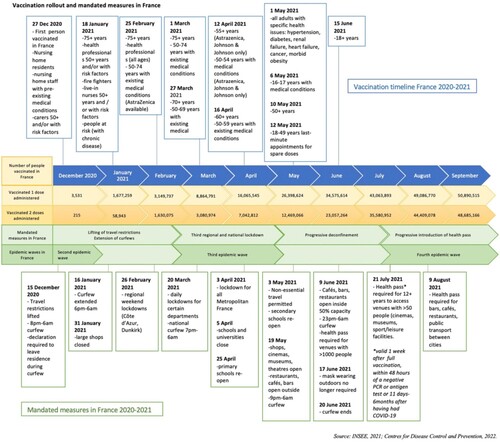
The first data collection wave took place following the introduction of a national curfew, regional weekend lockdowns, and first dose vaccination for people who were immunocompromised or over 75 years of age. During the second wave of data collection in March 2021, nineteen departments went into their third lockdown and by 3 April, this extended to all metropolitan France. Phases 1 and 2 of deconfinement began in early May, as Wave 4 of the surveys was conducted, and as vaccination opened up for people 50 + years and those aged 18–50 with comorbidities. The final stage (Phase 3) of deconfinement occurred in June, as participants responded to Wave 5 surveys, and first dose vaccination was extended to everyone over 18 years. Following the introduction in July of a mandatory health pass to gain access to cultural and leisure facilities, and its extension in August to public venues such as restaurants, cinemas, bars, gyms and swimming pools, as well as to their employees, the final wave of surveys (Wave 7) was undertaken. This September survey coincided with 80% of the population aged 12 and above’s having received their first dose of the vaccine (INSEE, Citation2021; Statsista, Citation2022). For an outline of vaccination rollout and mandatory measures, see .
Figure 1. Vaccine rollout and mandated measures in France.
Measures
Self-report measures were used to ascertain engagement in protective behaviour, vaccination status and intention, as well as health, sociocultural and demographic characteristics. The latter included questions regarding sex (male/female), age, secondary school completion (yes/no), socioeconomic status (high/low), financial situation (good/bad), housing overcrowding (yes/no), as well as whether they suffered from chronic illness (yes/no) or had experienced COVID-like symptoms (yes/no). Participants also reported whether they had been vaccinated, how many doses they had received and, for the unvaccinated, whether they intended to be vaccinated. In addition, they were asked whether they engaged in four protective behaviours: wearing a mask, observing hand hygiene, avoiding physical contact and avoiding social gatherings. For a complete list of questions regarding behaviour and possible responses, see . Behavioural frequency responses were dichotomised, with ‘Yes, systematically’ coded as 1 and ‘Yes, often’, ‘Yes, sometimes’ and ‘No, never’ as 0. This coding was adopted, grouping together the last three conditions, due there being a ceiling effect (Raude et al., Citation2020), as illustrated in . Risk compensation was measured indirectly by comparing levels of engagement in protective behaviours according to vaccination status. The behaviour of unvaccinated participants who intended to be vaccinated served as the baseline. Risk compensation was considered to be present when there was a reduction in behaviours in those vaccinated, as compared with those unvaccinated but intending to vaccinate.
Figure 2. Distribution of protective behaviours according to initial coding.
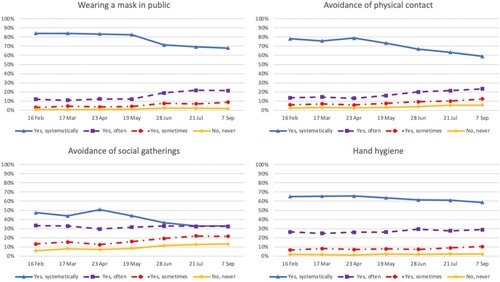
Table 1. Behaviour survey questions and responses.
Data analysis
A series of binary logistic analyses was performed to analyse the data, with preventive behaviour as the dependent variable. Odds ratios by vaccination status were calculated and then adjusted, controlling for age, sex and chronic health conditions, variables previously and consistently found to affect behavioural response (eg. Alleaume et al., Citation2021; Papageorge et al., Citation2021; Tang et al., Citation2021), to produce adjusted scores. Significant weighted odds ratio scores less than one were considered to be evidence of risk compensation in those who had received one or two vaccine doses.
Results
As illustrated in , the curve representing people having received one or two doses of the vaccine progresses in inverse proportion to those intending to be vaccinated. Information regarding vaccination status, age group, risk factors (chronic illness) and socio-demographic characteristics of participants at each of the seven survey waves is presented in . As explained earlier, risk compensation was measured indirectly by comparing protective behavioural engagement among vaccinated participants (1 or 2 doses) with those unvaccinated but intending to do so. It was hypothesised that there was evidence of risk compensation when vaccinated participants demonstrated a significant reduction in behavioural engagement, as compared with the unvaccinated-but-intending-to-vaccinate group (Hedlund, Citation2000; Jørgensen et al., Citation2021). Levels of engagement in the four different protective behaviours over time according to vaccination status were therefore measured and are presented in . As can be seen in the graphs of behavioural engagement in each of the four protective behaviours according to vaccination status at different stages over the seven-month period, following an initial rise in behavioural protection, frequencies thereof decreased towards the end of the measurement period. Although vaccinated participants appear to reduce their engagement in preventive behaviours, we are unable to tell whether this reduction is due to vaccination status. Logistic odds ratios and adjusted odds ratios (AOR) were therefore calculated and are presented in .
Figure 3. Vaccination status during the vaccine rollout in France, February – September, 2021.
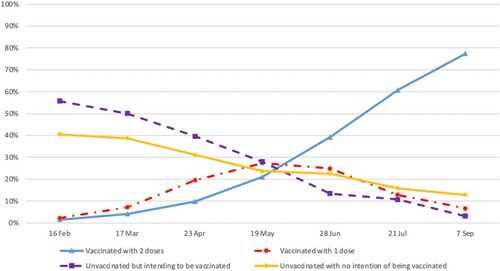
Figure 4. Engagement in protective behaviours according to vaccination status.
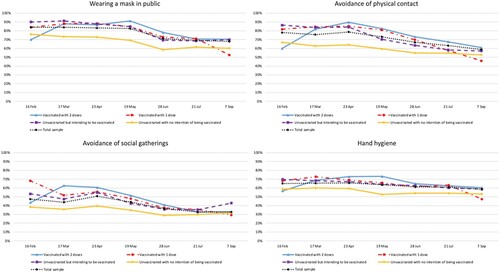
Table 2. Participant vaccination status according to age, risk factors (chronic illness), socio-demographic characteristics and survey wave (February – September, 2021).
Table 3. Odds ratios of protective behaviour according to vaccination status.
Overall, reduced engagement in protective behaviours among those fully vaccinated, as compared with those intending to do so, occurred neither systematically nor consistently but was nonetheless observed occasionally, particularly towards the end of the survey period, in Wave Six and Wave Seven (See ). Interestingly, comparatively reduced behavioural engagement was observed in February, among those who had received two vaccine doses (and were considered fully vaccinated at this time (ECDC, Citation2021a)), for two behaviours: wearing a mask in public (AOR = .22 (95% CI[.10,.50], p < .001)) and avoiding physical contact (shaking hands, hugging etc.) (AOR = .23 (95% CI[.10,.50], p. < 001)). It should be noted that participants having received a single Janssen dose were considered fully vaccinated (Centres for Disease Control and Prevention (CDC), Citation2022) and were therefore included in the fully-vaccinated (2-dose) group. To the extent that the Johnson & Johnson Janssen vaccine represented less than 1% of the national vaccination figures to the end of June, 2021 (Santé Publique, Citation2022), this concerned very few of the survey respondents. Curiously, an increase in protective behaviours among fully-vaccinated participants occurred in March towards avoiding social gatherings (AOR = 1.70 (95% CI[1.06,2.73], p = .029)) and in May towards hand hygiene (AOR = 1.47 (95% CI[1.07,2.00], p = .016)). As compared with the unvaccinated-but-intending-to vaccinate group, a decrease in frequency of adoption of protective measures was found towards the end of the vaccine rollout for two of the four protective behaviours: avoiding social gatherings in July (AOR = .72 (95% CI[.53,.99], p = .045)) and September (AOR = .54 (95% CI[.32,.91], p = .022)) among fully-vaccinated participants, and wearing a mask in September (AOR = .48 (95% CI[.25,.93], p = .029)) for those vaccinated with one dose.
From these results, it appears that fully-vaccinated participants reported being less likely to avoid social gatherings in July than the intending-to-vaccinate group. This trend was observed again in September. Similarly, in September, participants vaccinated with one dose reported wearing masks less frequently than the intending-to-vaccinate group. No such significant differential engagement in protective behaviour between the vaccinated and intending-to-vaccinate groups was observed towards hand hygiene or avoidance of physical contact at this stage.
Discussion
Overview
Consistent with an indirect measurement of risk compensation, through a comparison of behavioural engagement according to vaccination status, our results were suggestive of risk compensation when vaccinated participants demonstrated a reduction in protective measures, as compared with the baseline behaviour of those who were unvaccinated but intended to do so (Hedlund, Citation2000; Jørgensen et al., Citation2021). Overall, it would appear from our findings that from time to time, vaccinated participants adhered less frequently to protective behaviours than the baseline group, towards specific behaviours and with greater frequency towards the end of the survey period, which coincided with the final stages of the vaccination campaign in France.
According to the afore-mentioned definition, it would therefore seem that there was somewhat limited evidence of risk compensation during the 2021 COVID-19 vaccination campaign in France, particularly towards the end of the vaccine rollout towards two protective behaviours: avoiding social gatherings (in July and September for fully-vaccinated participants) and wearing a face mask (in September for people vaccinated with one dose). Indeed, of relevance from a public health perspective, it appears that fully-vaccinated participants avoided social gatherings less often in July than those intending to vaccinate, and this trend in lack of social gathering avoidance was repeated again in September. A similar trend was observed in September among participants vaccinated with one dose who reported wearing a mask less often than their intending-to-vaccinate counterparts. Whilst perhaps not representing a threat to the expected efficacy of the vaccination campaign (Buckell et al., Citation2021), such evidence of risk compensation, and indeed, decreasing levels of adherence to a particular protective behaviour among a specific group, during the late stages of the vaccine rollout nevertheless merits attention, as any reduction in behavioural preventive vigilance may result in subsequent propagation of the virus (Youssef et al., Citation2022).
Observed episodic behaviours
Although reduced levels of protective engagement indicative of risk compensation were observed in fully-vaccinated participants towards mask wearing and avoiding physical contact at the outset of the vaccine rollout, this concerned very few participants (n = 21/30), due in part to limited vaccine availability and at the time, vaccination’s being restricted to people who were immunocompromised or over the age of 85. The increased engagement in avoiding social gatherings in March among fully-vaccinated participants, as compared with those intending to be vaccinated, coincided with the introduction of regional lockdowns and curfews. At this stage, in March, vaccination was open to people over 75 and those 50–74 with a pre-existing medical condition. It is possible that this vulnerable population, in the context of regional lockdowns and curfews, may have preferred to avoid social gatherings so as not to come into contact with the rather large unvaccinated population. This increased avoidance of social gatherings may perhaps also be explained by differential risk reappraisal by these two groups. According to the theory of risk reappraisal, when faced with a health risk, an individual may adopt protective measures and, as a result of these protective actions, perceptions of risk are reduced which may, in turn, lead to a subsequent reduction in behavioural engagement (Brewer et al., Citation2004). Applied to the situation under investigation, the epidemic context and government-mandated measures may have led to different re-appraisals among the people who were fully vaccinated, as compared with those intending to do so. For instance, whereas in March, nineteen French departments were in lockdown and by early April, this had extended to the entire metropolitan population, May marked the beginning of Phase 1 deconfinement, during which only limited social gatherings were possible. Fully-vaccinated participants’ increased frequency of engagement in hand hygiene, as compared with the unvaccinated-but-intending-to-vaccinate group in May might perhaps reflect a more delayed time frame regarding risk re-appraisal and subsequent behaviour. Having being fully vaccinated earlier, it is possible that this group of people may have been initially more risk-averse and therefore maintained comparatively greater hand hygiene precautions, as they perhaps took longer than the intending-to-vaccinate group to re-appraise their risk and behaviour in response to deconfinement and an increasingly vaccinated general public. Interestingly, in June, the number of unvaccinated individuals who intended to be vaccinated may also be explained by a slowing down in vaccine distribution that occurred at around this time in France, which was the subject of media attention (Boisselier, Citation2021).
Risk compensation and vaccine rollout
Of relevance to risk management, through public health messages and campaigns targeting the mitigation of disease spread, is the reduction in levels of behavioural engagement, suggestive of risk compensation, observed towards the end of the vaccine rollout among the fully-vaccinated. Risk compensation at this stage, particularly with the appearance of new COVID-19 variants and possible reduced vaccine efficacy, may indeed pose a threat to combatting the disease, the battle against which is heavily reliant upon continued and prolonged maintenance of barrier measures. Although increasing vaccine uptake among the unvaccinated-but-not-intending-to-vaccinate group would also represent a means of disease mitigation, this was not the focus of our study. Moreover, people not intending to vaccinate have been observed to be less likely to respond to public health messages promoting behavioural protective measures, and in some cases, such messages have even been found to be counterproductive among those not intending to vaccinate (Nyhan et al., Citation2014). As this extends beyond the remit of the current study, our discussion therefore concentrates upon those unvaccinated-but-intending-to-vaccinate.
It should be noted that risk compensation, or comparatively reduced behavioural engagement, observed towards the end of the rollout coincided with 73.2% and 87.7% of the French adult population’s having received their first dose of the vaccine and 56.7% and 75.5% their full primary course in July and September respectively (ECDC, Citation2021a). In addition to being the French summer vacation period, July and August also marked the introduction of a mandatory health pass attesting to full primary course vaccination, or a negative polymerase chain reaction (PCR) test, to gain access firstly, to cultural and leisure facilities, and then to public venues such as restaurants, cinemas, swimming pools, amusement parks and gyms. Avoiding or foregoing such activities may have proven effortful and extremely costly socially, particularly following the extended period of lockdowns and reduced social interaction. This may account for the observed reduced behavioural adherence thought to represent risk compensation in July towards avoiding social gatherings. The sense of security afforded by being fully vaccinated, and frequenting venues along with others who also held a mandatory health pass, perhaps allowed people to participate in long-awaited social activities once again. This was perhaps not the case for those unvaccinated or partially vaccinated, who faced more barriers to access venues where social gatherings took place, and could also explain the differential avoidance of social gatherings among the fully and partially- or unvaccinated participants at this stage.
Whereas the July data collection period coincided with summer holidays, the September phase of data collection marked the return to work and beginning of the school year. It is curious that risk compensation, or relaxing of protective behavioural adherence, towards avoidance of social gatherings continued at these contextually different stages. Social gatherings were perhaps unavoidable in the context of returning to work and school. It is also possible that the extension of the mandated health pass in August to employees working in the aforementioned public venues and services, heightened the sense of security afforded by vaccination, not only due to one’s own vaccination, but also to that of others, as suggested by Buckell et al. (Citation2021). It is conceivable that participants who had not been vaccinated until this late stage were laggards and had perhaps been reticent to do so up until this point and therefore also less likely to engage in or maintain other protective behaviours (Sutton, Citation1994), particularly a costly one (Kroczek et al., Citation2022), such as avoiding social gatherings. As working-age French residents were eligible for vaccination from May 2021 onwards, possible motivating factors for being vaccinated may have emanated from a desire to protect oneself and others, or may have been unrelated to health reasons. If the underlying incentive to be vaccinated were driven by non-health-related reasons, such as the freedom and benefits accorded to those holding a health pass, then individuals in this category at this late stage of the vaccination campaign, for whom health grounds were not the main concern, may also have been less likely to engage in other means of protection. Another possibility is that this group believed that they had contributed adequately to herd immunity and therefore could relax other, non-pharmaceutical protective behaviours.
Interestingly, the quasi absence of lessened behavioural adherence, possibly indicative of risk compensation, during the first five months of the vaccination campaign, and towards the other protective behaviours throughout, would suggest that whether a particular behaviour is maintained may depend largely on the nature of the behaviour, whether it is easily achieved, as well as the social and professional context. For instance, it is easier to engage in all forms of preventive behaviour during phases of confinement than during deconfinement. Moreover, during deconfinement, it was perhaps easier to use hand sanitiser, wear a mask or avoid physical contact during social interactions than it was to avoid social gatherings altogether, particularly as confinement restrictions had just been lifted in July, allowing friends and family to reunite during the summer holidays, and September marked a physical return to the workplace and post-holiday work gatherings.
That risk compensation was also observed towards mask wearing in September among people vaccinated with one dose is interesting. By this stage in France, Pfizer and Moderna vaccines were administered predominantly, with an efficacy at the time estimated at 80% following a single dose (eg. Thompson et al., Citation2021). This was perhaps sufficient to elicit a sense of security and resultant risk compensation towards mask wearing among this group, and towards social gatherings among the fully-vaccinated participants. In addition, wearing a mask during the return to the workplace, and in hot weather, may have proven uncomfortable both physically and socially and therefore also been a costly behaviour in which to engage, however this does not explain why those who were fully vaccinated were nonetheless prepared to put up with this inconvenience.
A further possibility is that other contextual factors, combined with vaccination, may have contributed to a decrease in protective behaviours. For instance, decreased severity associated with the Delta variant (Miyashita et al., Citation2023), and for those vaccinated, a decrease in the number of COVID-19-related fatalities (Santé Publique, Citation2021), as well as the progressive relaxation of mandated restrictive measures and increased numbers of vaccinated people, may have contributed to a reduced perception of risk and subsequent adherence to protective measures.
Denoting a comparative reduction in protective behavioural engagement, it could be argued that risk compensation does not take into consideration people’s motivation to reduce protection and as such, does not distinguish between people who might justifiably reduce their level of protection and those who do so recklessly. Whilst vaccination did indeed protect against severe forms of the disease, breakthrough cases were nonetheless commonly reported and health authorities continued to advise maintenance of non-pharmaceutical protective measures (Covid et al., Citation2021). The fact that cases were less severe among those vaccinated may have led them to perceive a reduced threat to both themselves and others, allowing them to reduce other non-pharmaceutical measures that, themselves, were not without harms. For instance, social isolation, due to avoidance of social gatherings, was associated with mental health issues (Pancani et al., Citation2021; Pietrabissa & Simpson, Citation2020; Santé Publique, Citation2021) and mask wearing was associated with both physiological and psychological problems (Park et al., Citation2021; Rosner, Citation2020; Scheid et al., Citation2020). Such a reduction in non-pharmaceutical measures should in no way be interpreted as risky behaviour associated with wilful endangerment or compromising the health of oneself or others, that is certainly not the intention of this paper. What we seek to explore are differences in frequencies of engagement in protective behaviour between vaccinated and intending-to-vaccinate groups at different times throughout the pandemic, because a comparative reduction in protection by vaccinated people may be indicative of risk compensation, which certain researchers warn could ultimately lead to disease spread (Trogen & Caplan, Citation2021). Through our investigation, we hope to glean insight into the temporal variations in protective engagement, which may serve to inform targeted, strategic epidemic management.
A further result of note, from a public health perspective, is that with the exception of July, when all groups appeared to reduce their engagement in protective behaviours, a group of people who had no intention of being vaccinated was present at each study wave. Indeed, despite the introduction of the mandatory health pass, this group represented more than 10% of the sample (ie. over 200 participants) in the final survey wave in September. Previous research has found that for individuals in this category, for whom vaccination may have been less of a choice than an un-health-related, utilitarian necessity, engagement in other health protective behaviours would be an unlikely outcome of conscious decision-making on their behalf (Ouellette & Wood, Citation1998; Sutton, Citation1994). This is of concern as the behavioural reticence of this group, not only towards vaccination, but also towards non-pharmaceutical interventions, could ultimately have an impact on the spread of the epidemic.
Our findings and prior research
In light of the existing research into risk compensation following COVID-19 vaccination in Europe, our findings provide interesting insights. Indeed, they contrast those of Sun et al. (Citation2022) who, focusing on health care workers in China, targeted a population that was perhaps acutely aware of and educated about the importance of protective measures. In addition, due to their often constant and prolonged exposure to patients suffering from the virus, health care workers’ personal health risk was higher than that of the general population. This may explain their increased engagement in protective measures following vaccination. In contrast, our findings, based upon a large representative sample of the general population, provide ecologically relevant insights into the behaviour of the public at large, and may help inform policy makers’ decisions to target public health messages at particular epidemic stages and among particular populations in order to combat risk compensation and ultimately, disease spread.
The results of the current investigation partially diverge from those of two studies in the US and Canada that found protective behaviours of vaccinated participants were maintained over time, despite vaccination (Hall et al., Citation2022; Thorpe et al., Citation2022). Thorpe et al.’s (Citation2022) three-wave, longitudinal US investigation took place over the initial three and a half months of the vaccination campaign and may not reflect changes that occur as the vaccination campaign and the epidemic wore on. In their two-wave, longitudinal study in Canada, Hall et al. (Citation2022) compared behavioural engagement between fully-vaccinated and vaccine-hesitant participants at two different epidemic peaks. Whilst decreasing among all groups, levels of protection were significantly reduced among the unvaccinated, leading the authors to conclude that vaccinated participants were more likely to adhere to preventive behaviours than those who were unvaccinated. Targeting participants aged 18 - 55 years, who are perhaps less at risk of sever forms of the disease (INSEE, Citation2021), the protective behaviour of the over 55 age group, more susceptible to severe forms of the disease and a poorer health outcome (Miyashita et al., Citation2023), remains unknown. Additionally, comparing behaviour of fully-vaccinated with that of vaccine-hesitant groups, may provide more starkly contrasted results, in terms of beliefs, motivation and behaviour, than would the comparison between the vaccinated and intending-to-vaccinate groups in our study. Moreover, measuring behavioural response at the peak of two epidemic waves does not capture levels of protective engagement between waves which, from a public health perspective, could provide valuable insights, allowing researchers and public health authorities to develop targeted and timely management strategies which could contribute to reducing the spread and health impact of successive epidemic waves.
Our findings also differ from those of Desrichard et al. (Citation2022) and Wright et al. (Citation2022), who observed no evidence of risk compensatory behaviour, and even a slight increase in most protective behaviours following vaccination among their UK participants. This difference may be explained in part by national variations in health advice and the epidemic context, as well as by the stage and duration of the time frame investigated. In the case of Wright et al. (Citation2022), in addition to their non-representative sample’s being voluntary and older, and therefore more aware of and likely to adopt protective measures, their investigation coincided with lockdown, during which compliance with protective measures was easier, as well as the initial phase of limited vaccine rollout. Although administered later, Desrichard et al.’s (Citation2022) final survey wave was also conducted during the early stages of the UK vaccination campaign, whereas those in our investigation spanned all seven months of the vaccine rollout and therefore were perhaps able to capture changes in behaviour that appeared over a longer period of time – weeks and in some cases, months, following vaccination. An interesting parallel exists between the authors’ documentation of a decrease in avoidance of crowded areas (Desrichard et al., Citation2022) and in some groups, social distancing (Wright et al., Citation2022) and our finding of decreased avoidance of social gatherings. It is perhaps a need for social contact, particularly following repeated lockdowns and restrictions, that prevails over time, manifesting itself in reduced avoidance of social gatherings and settings.
There is a small degree of concordance between our findings and those of Jia et al. (Citation2022) who observed risk compensation towards avoiding social gatherings. However, whereas risk compensation occurred towards the end of the vaccine rollout and as people returned to work in our investigation, it was present in the US study immediately following partial vaccination. Unlike our American counterparts, who found that engagement in protective behaviours decreased over time, we found no such disengagement towards the other protective behaviours measured. Such differences may perhaps be attributed to national variations in health advice and government mandates in the two countries.
Like Buckell et al. (Citation2021), we also found limited evidence of risk compensation towards the avoidance of social gatherings. However, whilst risk compensation in our study was observed towards the end of the vaccine rollout for two behaviours among vaccinated participants, our British counterparts found no such association between personal vaccination and non-pharmaceutical protective behaviours. Rather, participants in England, Scotland, Wales and Northern Ireland demonstrated risk compensation as national vaccination uptake rates increased in the general population. These contrasting findings would, at first glance, suggest that different factors must be operating. However, whereas we investigated a range of behavioural measures (mask wearing, hand hygiene, avoiding physical contact, avoiding social gatherings), the UK study predominantly investigated variations of physical distancing measures. The level of choice, and therefore locus of control, involved these behaviours varies considerably. For instance, whilst an individual may be able to choose whether to avoid physical contact with different populations, this degree of choice may have been reduced for physical distancing due to the nature of people’s work, and negligible for those unable to work from home and for whom it was necessary to take public transport, or for those caring for others. In contrast, a greater degree of personal control and choice was associated with the behavioural measures investigated in our study. Individuals could choose whether they adhered to the mask mandate, avoided physical contact and / or observed hand hygiene and even to a certain extent, avoided social gatherings over the summer vacation period. The greater control afforded by personal choice to adhere to protective behaviours, reinforced by public health messages, may have focused vaccinated participants’ attention on their individual contribution to fighting the disease. This continued individual focus, the same one that initially motivated their engagement in protective measures and vaccination, may have elicited feelings of relative security, which subsequently resulted in risk compensation towards the end of the rollout.
Interestingly, it would appear that our findings echo those of our predecessors, who also found limited evidence of risk compensation towards COVID-19 protective measures as a result of mask wearing, (Aranguren, Citation2022; Cartaud et al., Citation2020; Jørgensen et al., Citation2021; Kroczek et al., Citation2022; Luckman et al., Citation2021; Yan et al., Citation2021). We therefore concur in concluding that whilst risk compensation may reduce the efficacy of the COVID-19 vaccination campaign, it would in no way negate the overall benefits.
Implications for management
Our findings, although suggesting that risk compensation would not detract from the overall efficacy of a public health campaign combining behavioural and pharmaceutical interventions, nonetheless have direct implications for the management of public health policies during an evolving pandemic or epidemic. Strategic timing of public health messages at particular stages of the pandemic, in response to government mandates or the relaxing thereof, whilst taking into account seasonality and the calendar of festivities and public events, would appear to be fundamental in combatting the disease. In addition, strategically targeting certain populations, notably those who are vaccinated or intend to be vaccinated, may also be advantageous. Given their acceptance of this protective measure, they are perhaps a motivated, receptive audience and with strategically-timed public health reminders and encouragement, may be more likely to maintain all protective behaviours. Educating and informing these populations, as well as health care professionals and policy makers, about risk compensation could also be effective in combatting the disease. Moreover, in order to orientate public health and government decision-making during an epidemic in real-time, it would be both advantageous and beneficial to prepare and establish in advance a partnership between health authorities and competent research teams so as to ensure that human and financial resources are available to be mobilised when, and as required.
Limitations
Targeting risk compensation arising from COVID-19 vaccination, our study provides an insight into changes in behaviour over time as the vaccine rollout and pandemic unfolded. Despite its advantages, our study nonetheless has some limitations. Being repeated and cross-sectional, it provides information over time at the population level. Future longitudinal research would provide interesting, complementary information as to patterns of individual behaviour change. Though our data were highly consistent with the actual vaccine coverage recorded by the French health authorities, as our surveys relied upon self-reports of protective behaviour, we have no way of knowing whether participants actually engaged in the reported behaviours, or if answers were subject to a social desirability bias (Crane et al., Citation2021; Sapsford, Citation2006). However, as it was not possible to measure participant behaviour directly, this online means of measurement served as a proxy that has been validated empirically, used widely in the research literature, and has been found to be less subject to social desirability biases than face-to-face surveys (Weinstein et al., Citation2005).
A methodological limitation of our exploratory study lies in the fact that whilst a reduction in behavioural protection was observed and satisfied the definition of risk compensation (Hedlund, Citation2000; Jørgensen et al., Citation2021), the underlying social psychological factors responsible remain unknown. It is possible that the reduced adherence to protective measures may have resulted from a number of other factors, such as those involved in the risk reappraisal process. From an ecological perspective, changes in the epidemiological trajectory, mandated measures, health authority guidelines, death incidence rates, perceived security due others’ being vaccinated or an economic need to return work and workplace gatherings, may also explain a general reduction in socially costly distancing behaviours over time (Crane et al., Citation2021; Petherick et al., Citation2021). However, the analysis of individual behavioural data in a series of seven cross-sectional studies enables us to at least partly control the influence of the epidemiological and regulatory context, as an absence of risk compensation effects was repeatedly found during the vaccination campaign at different points of time. Further research incorporating social cognitive variables, such as perceived risk, may provide valuable insights into factors contributing to and detracting from behavioural engagement, thereby shedding further light on risk compensation and allowing public health advisers to develop a targeted, strategic response.
Future research
As mentioned in the previous section, investigating changes in risk perception and behavioural response over time would enable researchers to develop a better understanding of the underlying factors and mechanisms involved in risk compensation. In addition to longitudinal research, further investigation of risk compensation, as well as the evolution of participant behaviour at an individual level, and in the period following the vaccine campaign, would allow us to ascertain as to whether risk compensation were increasingly present as time wore on, or whether it fluctuated, important elements to consider in pandemic management. Another interesting area of research would be to investigate motivation and behavioural response among the unvaccinated-but-not-intending-to-vaccinate group.
Conclusion
As one of the first investigations of risk compensation over time following COVID-19 vaccination among a large representative sample of the general French population, our findings of limited evidence of risk compensation, observed at the end of the vaccine rollout towards two protective behaviours, provide insights into the evolutive nature of people’s preventive behaviours in response to pandemic and epidemiological changes. Future longitudinal research in this area at an individual level may complement and refine our understanding of risk compensation and its behavioural implications. Congruent with the literature on risk compensation and mask wearing, we also conclude that whilst not negating the overall efficacy of the vaccination campaign, risk compensation can nonetheless detract from the achievement of optimal health benefits associated with vaccination (Iyengar et al., Citation2021). This has implications for the effective management of public health messages, campaigns and policy. Understanding when, among whom and towards which category of protective measures risk compensation may occur provides public health authorities with valuable tools with which to manage future campaigns. Strategically planned, well-timed public health interventions, delivered at contextually advantageous phases and stages, focusing on specific behaviours and targeting relevant groups most likely to respond with the desired behaviour, in addition to educating people about risk compensation, may prove to be an effective way forward in managing and combatting not only the spread of new variants of COVID-19, but also that of epidemics and pandemics to come.
Ethics statement
This study was conducted in compliance with the French national guidelines for ethical research in the social and human sciences. The research was declared to the EHESP School of Public Health Office for Personal Data Protection (Rennes, France) [Reference: MR 2510110520], and approved by the ethics committee of the University Hospital Institute, Méditerranée Infection (Marseille France) [Decision No. 2020-022]. Informed consent was obtained from participants.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by an Institutional Review Board/Ethics committee. See details above and under Methods.
Acknowledgements
The authors are grateful to Dr Pierre Arwidson and the COVIPREV group (Enguerrand du Roscoät, Jean-Michel Lecrique, Linda Lasbeur, Christophe Léon, Pierre Arwidson, Isabelle Bonmarin, and Oriane Nassany) from the Department of Health Promotion and Prevention (Santé Publique France) for their valuable support.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Alleaume, C., Verger, P., Dib, F., Ward, J. K., Launay, O., & Peretti-Watel, P. (2021). Intention to get vaccinated against COVID-19 among the general population in France: Associated factors and gender disparities. Human Vaccines & Immunotherapeutics, 17(10), 3421–3432. https://doi.org/10.1080/21645515.2021.1893069
- Aranguren, M. (2022). Face mask use conditionally decreases compliance with physical distancing rules against COVID-19: Gender differences in risk compensation pattern. Annals of Behavioral Medicine, 56(4), 332–346. https://doi.org/10.1093/abm/kaab072
- Blanken, T. F., Tanis, C. C., Nauta, F. H., Dablander, F., Zijlstra, B. J., Bouten, R. R., Oostvogel, Q. H., Boersma, M. J., van der Steenhoven, M. V., van Harreveld, F., & de Wit, S. (2021). Promoting physical distancing during COVID-19: A systematic approach to compare behavioral interventions. Scientific Reports, 11(1), 1–8. https://doi.org/10.1038/s41598-021-98964-z
- Boisselier, A. (2021, March 9). COVID-19. ‘Les livraisons de vaccins revues à la baisse en France. Ouest France. https://www.ouest-france.fr/sante/vaccin/covid-19-les-livraisons-de-vaccins-revues-a-la-baisse-en-france-7180683 [accessed 20 March 2023]
- Bottemanne, H., & Friston, K. J. (2021). An active inference account of protective behaviours during the COVID-19 pandemic. Cognitive, Affective, & Behavioral Neuroscience, 21(6), 1117–1129. https://doi.org/10.3758/s13415-021-00947-0
- Brewer, N. T., Cuite, C. L., Herrington, J. E., & Weinstein, N. D. (2007). Risk compensation and vaccination: Can getting vaccinated cause people to engage in risky behaviors? Annals of Behavioral Medicine, 34(1), 95–99. https://doi.org/10.1007/BF02879925
- Brewer, N. T., Weinstein, N. D., Cuite, C. L., & Herrington, J. E. (2004). Risk perceptions and their relation to risk behavior. Annals of Behavioral Medicine, 27, 125–130. https://doi.org/10.1207/s15324796abm2702_7
- Buckell, J., Jones, J., Matthews, P. C., Diamond, I., Rourke, E., Studley, R., Cook, D., Walker, A. S., & Pouwels, K. B. (2021). COVID-19 vaccination, risk-compensatory behaviours, and social contacts in four countries in the UK. medRxiv, https://doi.org/10.1101/2021.11.15.21266255
- Cartaud, A., Quesque, F., & Coello, Y. (2020). Wearing a face mask against COVID-19 results in a reduction of social distancing. PLoS One, 15(12), e0243023. https://doi.org/10.1371/journal.pone.0243023
- Cassell, M. M., Halperin, D. T., Shelton, J. D., & Stanton, D. (2006). Risk compensation: The Achilles’ heel of innovations in HIV prevention? Bmj, 332(7541), 605–607. https://doi.org/10.1136/bmj.332.7541.605
- Centers for Disease Control and Prevention. (2022). Vaccines and immunizations: Janssen (Johnson & Johnson) COVID-19 Vaccine [online], Centers for Disease Control and Prevention. https://www.cdc.gov/vaccines/covid-19/info-by-product/janssen/index.html [Accessed 27 March 2023]
- Covid, C. D. C., Team, V. B. C. I., Birhane, M., Bressler, S., Chang, G., Clark, T., Dorough, L., Fischer, M., Watkins, L. F., Goldstein, J. M., & Kugeler, K. (2021). COVID-19 vaccine breakthrough infections reported to CDC – United States, January 1–April 30, 2021. Morbidity and Mortality Weekly Report, 70(21), 792. https://doi.org/10.15585/mmwr.mm7021e3
- Crane, M. A., Shermock, K. M., Omer, S. B., & Romley, J. A. (2021). Change in reported adherence to nonpharmaceutical interventions during the COVID-19 pandemic, April-November 2020. Jama, 325(9), 883–885. https://doi.org/10.1001/jama.2021.0286
- Desrichard, O., Moussaoui, L., & Ofosu, N. (2022). Reduction of precautionary behaviour following vaccination against COVID-19: A test on a British cohort. Vaccines, 10(6), 936. https://doi.org/10.3390/vaccines10060936
- Eaton, L. A., & Kalichman, S. C. (2007). Risk compensation in HIV prevention: Implications for vaccines, microbicides, and other biomedical HIV prevention technologies. Current HIV/Aids Reports, 4(4), 165–172. https://doi.org/10.1007/s11904-007-0024-7
- Esmaeilikia, M., Radun, I., Grzebieta, R., & Olivier, J. (2019). Bicycle helmets and risky behaviour: A systematic review. Transportation Research Part F: Traffic Psychology and Behaviour, 60, 299–310. https://doi.org/10.1016/j.trf.2018.10.026
- European Centre for Disease Prevention and Control. (2020). Using face masks in the community – reducing Covid-19 transmission from potentially asymptomatic or pre-symptomatic people through the use of face masks [online ], European Centre for Disease Prevention and Control. https://www.ecdc.europa.eu/en/publications-data/using-face-masks-community-reducing-covid-19-transmission [Accessed 18 March 2021]
- European Centre for Disease Prevention and Control. (2021a). COVID-19 vaccine tracker [online ], European Centre for Disease Prevention and Control. https://vaccinetracker.ecdc.europa.eu/public/extensions/covid-19/vaccine-tracker.html [Accessed 3 May 2022]
- European Centre for Disease Prevention and Control. (2021b). Non-pharmaceutical interventions against COVID-19 [online], European Centre for Disease Prevention and Control. https://www.ecdc.europa.eu/en/covid-19/prevention-and-control/non-pharmaceutical-interventions [Accessed 17 June 2022]
- Haider, A. H., Saleem, T., Bilaniuk, J. W., & Barraco, R. D. (2012). An evidence based review: Efficacy of safety helmets in reduction of head injuries in recreational skiers and snowboarders. The Journal of Trauma and Acute Care Surgery, 73(5), 1340. https://doi.org/10.1097/TA.0b013e318270bbca
- Hall, P. A., Meng, G., Sakib, M. N., Quah, A. C., Agar, T., & Fong, G. T. (2022). Do the vaccinated perform less distancing, mask wearing and hand hygiene? A test of the risk compensation hypothesis in a representative sample during the COVID-19 pandemic. Vaccine, https://doi.org/10.1016/j.vaccine.2022.10.028
- Hedlund, J. (2000). Risky business: Safety regulations, risk compensation, and individual behavior. Injury Prevention, 6(2), 82–89. https://doi.org/10.1136/ip.6.2.82
- Institut National de la Statistique et des Études Économiques. (2017). Statistiques et Études: Bilan démographique 2016 [online], Institut National de la Statistique et des Études Économiques (INSEE). https://www.insee.fr/fr/statistiques/2554860#:~:text = Au%201er%20janvier%202017,hausse%20de%200%2C4%20%25. [accessed 3 May 2022]
- Institut National de la Statistique et des Études Économiques. (2021). Statistics and studies: France, social portrait 2021 edition. The Covid-19 pandemic: 4 waves, 116 deaths and severe consequences for the healthcare system. https://www.insee.fr/en/statistiques/6438589?sommaire = 6438617. [accessed 20 March 2022]
- Iyengar, K. P., Ish, P., Botchu, R., Jain, V. K., & Vaishya, R. (2021). Influence of the Peltzman effect on the recurrent COVID-19 waves in Europe. Postgraduate Medical Journal, 98(e2), e110–e111. https://doi.org/10.1136/postgradmedj-2021-140234
- Jain, V. K., Iyengar, K., Garg, R., & Vaishya, R. (2021). Elucidating reasons of COVID-19 re-infection and its management strategies. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 15(3), 1001–1006. https://doi.org/10.1016/j.dsx.2021.05.008
- Jia, J. S., Yuan, Y., Jia, J., & Christakis, N. A. (2022). Risk perception and behaviour change after personal vaccination for COVID-19 in the USA.
- Jørgensen, F., Lindholt, M. F., Bor, A., & Petersen, M. B. (2021). Does face mask use elicit risk-compensation? Quasi-experimental evidence from Denmark during the SARS-CoV-2 pandemic. European Journal of Public Health, 31(6), 1259–1265. https://doi.org/10.1093/eurpub/ckab136
- Juyal, D., Pal, S., Thaledi, S., & Pandey, H. C. (2021). COVID-19: The vaccination drive in India and the Peltzman effect. Journal of Family Medicine and Primary Care, 10(11), 3945–3947. https://doi.org/10.4103/jfmpc.jfmpc_739_21
- Kacelnik, O., & Kacelnik, A. (2022). Behavioral risk compensation and the efficacy of nonpharmacological interventions. Behavioural Public Policy, 6(1), 1–12. https://doi.org/10.1017/bpp.2021.1
- Kamath, V., & Nivea, B. (2021). COVID-19 Vaccines: A weapon for global security. APIK Journal of Internal Medicine, 9(4), 200. https://doi.org/10.1093/eurpub/ckab136
- Kassa, S. M., & Ouhinou, A. (2015). The impact of self-protective measures in the optimal interventions for controlling infectious diseases of human population. Journal of Mathematical Biology, 70(1), 213–236. https://doi.org/10.1007/s00285-014-0761-3
- Kasting, M. L., Shapiro, G. K., Rosberger, Z., Kahn, J. A., & Zimet, G. D. (2016). Tempest in a teapot: A systematic review of HPV vaccination and risk compensation research. Human Vaccines & Immunotherapeutics, 12(6), 1435–1450. https://doi.org/10.1080/21645515.2016.1141158
- Kroczek, L. O., Böhme, S., & Mühlberger, A. (2022). Face masks reduce interpersonal distance in virtual reality. Scientific Reports, 12(1), 1–10. https://www.nature.com/articles/s41598-022-06086-x.pdf
- Liebst, L. S., Ejbye-Ernst, P., de Bruin, M., Thomas, J., & Lindegaard, M. R. (2022). No evidence that mask-wearing in public places elicits risk compensation behavior during the COVID-19 pandemic. Scientific Reports, 12(1), 1–7. https://www.nature.com/articles/s41598-022-05270-3.pdf
- Luckman, A., Zeitoun, H., Isoni, A., Loomes, G., Vlaev, I., Powdthavee, N., & Read, D. (2021). Risk compensation during COVID-19: The impact of face mask usage on social distancing. Journal of Experimental Psychology: Applied, 27(4), 722. https://doi.org/10.1037/xap0000382
- Mantzari, E., Rubin, G. J., & Marteau, T. M. (2020). Is risk compensation threatening public health in the COVID-19 pandemic? Bmj, 370), https://doi.org/10.1136/bmj.m2913
- Marchiori, M. (2020). COVID-19 and the social distancing paradox: Dangers and solutions. arXiv preprint arXiv:2005.12446, https://doi.org/10.48550/arXiv.2005.12446
- Martin, G. P., Hanna, E., & Dingwall, R. (2020). Urgency and uncertainty: COVID-19, face masks, and evidence informed policy. BMJ: British Medical Journal (Online), 369, https://doi.org/10.1136/bmj.m2017
- Mayhew, A., Mullins, T. L. K., Ding, L., Rosenthal, S. L., Zimet, G. D., Morrow, C., & Kahn, J. A. (2014). Risk perceptions and subsequent sexual behaviors after HPV vaccination in adolescents. Pediatrics, 133(3), 404–411. https://doi.org/10.1542/peds.2013-2822
- Messiah, A., Constant, A., Contrand, B., Felonneau, M. L., & Lagarde, E. (2012). Risk compensation: A male phenomenon? Results from a controlled intervention trial promoting helmet use among cyclists. American Journal of Public Health, 102(S2), S204–S206. https://doi.org/10.2105/AJPH.2012.300711
- Miyashita, K., Hozumi, H., Furuhashi, K., Nakatani, E., Inoue, Y., Yasui, H., Karayama, M., Suzuki, Y., Fujisawa, T., Enomoto, N., & Inui, N. (2023). Changes in the characteristics and outcomes of COVID-19 patients from the early pandemic to the delta variant epidemic: A nationwide population-based study. Emerging Microbes & Infections, 12(1), 2155250. https://doi.org/10.1080/22221751.2022.2155250
- Nilsson, A., Bergquist, M., & Schultz, W. P. (2017). Spillover effects in environmental behaviors, across time and context: A review and research agenda. Environmental Education Research, 23(4), 573–589. https://doi.org/10.1080/13504622.2016.1250148
- Nyhan, B., Reifler, J., Richey, S. and Freed, G. L. (2014). Effective messages in vaccine promotion: a randomized trial. Pediatrics, 133(4), e835–e842.
- Ouellette, J. A., & Wood, W. (1998). Habit and intention in everyday life: The multiple processes by which past behavior predicts future behavior. Psychological Bulletin, 124(1), 54. https://doi.org/10.1037/0033-2909.124.1.54
- Pancani, L., Marinucci, M., Aureli, N., & Riva, P. (2021). Forced social isolation and mental health: A study on 1,006 Italians under COVID-19 lockdown. Frontiers in Psychology, 12, 663799. https://doi.org/10.3389/fpsyg.2021.663799
- Papageorge, N. W., Zahn, M. V., Belot, M., Van den Broek-Altenburg, E., Choi, S., Jamison, J. C., & Tripodi, E. (2021). Socio-demographic factors associated with self-protecting behavior during the Covid-19 pandemic. Journal of Population Economics, 34(2), 691–738. https://doi.org/10.1007/s00148-020-00818-x
- Parikh, P., Joshi, S., & Gulia, A. (2021). Resurgence of COVID-19 in India-challenges and solution. Indian Journal of Medical Sciences, 73(1), 70. https://doi.org/10.25259/IJMS_149_2021
- Park, S. R., Han, J., Yeon, Y. M., Kang, N. Y., & Kim, E. (2021). Effect of face mask on skin characteristics changes during the COVID-19 pandemic. Skin Research and Technology, 27(4), 554–559. https://doi.org/10.1111/srt.12983
- Peltzman, S. (1975). The effects of automobile safety regulation. Journal of Political Economy, 83(4), 677–725. https://doi.org/10.1086/260352
- Petherick, A., Goldszmidt, R., Andrade, E. B., Furst, R., Hale, T., Pott, A., & Wood, A. (2021). A worldwide assessment of changes in adherence to COVID-19 protective behaviours and hypothesized pandemic fatigue. Nature Human Behaviour, 5(9), 1145–1160. https://doi.org/10.1038/s41562-021-01181-x
- Pietrabissa, G., & Simpson, S. G. (2020). Psychological consequences of social isolation during COVID-19 outbreak. Frontiers in Psychology, 11, 2201. https://doi.org/10.3389/fpsyg.2020.02201
- Pless, B. (2016). Risk compensation: Revisited and rebutted. Safety, 2(3), 16. https://doi.org/10.3390/safety2030016
- Raude, J., Lecrique, J. M., Lasbeur, L., Leon, C., Guignard, R., Du Roscoät, E., & Arwidson, P. (2020). Determinants of preventive behaviors in response to the COVID-19 pandemic in France: Comparing the sociocultural, psychosocial, and social cognitive explanations. Frontiers in Psychology, 11, 3345. https://doi.org/10.3389/fpsyg.2020.584500
- Rosner, E. (2020). Adverse effects of prolonged mask use among healthcare professionals during COVID-19. J Infect Dis Epidemiol, 6(3), 130. https://doi.org/10.23937/2474-3658/1510130
- Santé Publique, F. (2021). Coronavirus (COVID-19): Enjeux de santé dans le contexte de la COVID-19 [online], Santé Publique France. https://www.santepubliquefrance.fr/dossiers/coronavirus-covid-19/enjeux-de-sante-dans-le-contexte-de-la-covid-19 [Accessed 31 March 2023]
- Santé Publique, F. (2022). Info Covid France: chiffres clés et évolution de la Covid-19 en France et dans le monde [online], Santé Publique France. https://www.santepubliquefrance.fr/dossiers/coronavirus-covid-19/coronavirus-chiffres-cles-et-evolution-de-la-covid-19-en-france-et-dans-le-monde [Accessed 27 March 2023]
- Sapsford, R. (2006). Survey research. Survey Research, 1–296.
- Scheid, J. L., Lupien, S. P., Ford, G. S., & West, S. L. (2020). Commentary: Physiological and psychological impact of face mask usage during the COVID-19 pandemic. International Journal of Environmental Research and Public Health, 17(18), 6655. https://doi.org/10.3390/ijerph17186655
- Seres, G., Balleyer, A. H., Cerutti, N., Danilov, A., Friedrichsen, J., Liu, Y., & Süer, M. (2020). Face masks increase compliance with physical distancing recommendations during the COVID-19 pandemic (No. 253). Discussion Paper. http://hdl.handle.net/10419/224069 [Accessed 20 May 2022]
- Statista. (2022). Cumulative number of people who received one, two, or three doses of vaccines against the coronavirus (COVID-19) in France from December 27, 2020, to March 15, 2022 [online], Statista. https://www.statista.com/statistics/1195620/vaccines-again-covid19-france/ [Accessed 11 March 2022]
- Sun, L. X., Chen, L. L., Chen, W. Y., Zhang, M. X., Yang, M. G., Mo, L. C., Zhu, J. J., Tung, T. H., & Li, F. P. (2022). Association between health behaviours and the COVID-19 vaccination: Risk compensation among healthcare workers in Taizhou, China. Human Vaccines & Immunotherapeutics, 18(1), 2029257. https://doi.org/10.1080/21645515.2022.2029257
- Sutton, S. (1994). The past predicts the future: Interpreting behaviour–behaviour relationships in social psychological models of health behaviour. In D. R. Rutter, & L. Quine (Eds.), Social psychology and health: European perspectives (pp. 71–88). Avebury/Ashgate Publishing Co.
- Tang, C. C., Chen, H., & Wu, W. W. (2021). Factors influencing the protective behavior of individuals during COVID-19: A transnational survey. Scientific Reports, 11(1), 1–6. https://doi.org/10.1038/s41598-021-01239-w
- Tang, P., Hasan, M. R., Chemaitelly, H., Yassine, H. M., Benslimane, F. M., Al Khatib, H. A., AlMukdad, S., Coyle, P., Ayoub, H. H., Al Kanaani, Z., & Al Kuwari, E. (2021). BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the SARS-CoV-2 Delta variant in Qatar. Nature Medicine, 27(12), 2136–2143. https://doi.org/10.1038/s41591-021-01583-4
- Thankappan, S., & Nedumpillil, S. (2021). Peltzman effect and resurgence of COVID-19 in India. Asian Pacific Journal of Tropical Medicine, 14(5), 193. https://doi.org/10.4103/1995-7645.315896
- Thøgersen, J., & Crompton, T. (2009). Simple and painless? The limitations of spillover in environmental campaigning. Journal of Consumer Policy, 32(2), 141–163. https://doi.org/10.1007/s10603-009-9101-1
- Thompson, M. G., Burgess, J. L., Naleway, A. L., Tyner, H. L., Yoon, S. K., Meece, J., Olsho, L. E., Caban-Martinez, A. J., Fowlkes, A., Lutrick, K., & Kuntz, J. L. (2021). Interim estimates of vaccine effectiveness of BNT162b2 and mRNA-1273 COVID-19 vaccines in preventing SARS-CoV-2 infection among health care personnel, first responders, and other essential and frontline workers—eight US locations, December 2020–March 2021. Morbidity and Mortality Weekly Report, 70(13), 495. https://doi.org/10.15585/mmwr.mm7013e3
- Thorpe, A., Fagerlin, A., Drews, F. A., Shoemaker, H., & Scherer, L. D. (2022). Self-reported health behaviors and risk perceptions following the COVID-19 vaccination rollout in the USA: An online survey study. Public Health, 208, 68–71. https://doi.org/10.1016/j.puhe.2022.05.007
- Trogen, B., & Caplan, A. (2021). Risk compensation and COVID-19 vaccines. Annals of Internal Medicine, 174(6), 858–859. https://doi.org/10.7326/M20-8251
- Underhill, K. (2013). Study designs for identifying risk compensation behavior among users of biomedical HIV prevention technologies: Balancing methodological rigor and research ethics. Social Science & Medicine, 94, 115–123. https://doi.org/10.1016/j.socscimed.2013.03.020
- Weinstein, N. D., Marcus, S. E., & Moser, R. P. (2005). Smokers’ unrealistic optimism about their risk. Tobacco Control, 14(1), 55–59. https://doi.org/10.1136/tc.2004.008375
- Wilde, G. J. (1998). Risk homeostasis theory: An overview. Injury Prevention, 4(2), 89–91. https://doi.org/10.1136/ip.4.2.89
- World Health Organization. (2020). Advice on the use of masks in the context of covid-19: Interim guidance [online ], World Health Organisation. https://www.who.int/publications-detail/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019- ncov)-outbreak [Accessed 5 June 2020]
- World Health Organization. (2021). Looking back at a year that changed the world: WHO’s response to COVID-19, 22 January 2021 (No. WHO/WHE/2021.01). World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/340321/WHO-WHE-2021.01-eng.pdf?sequence = 1&isAllowed = y [Accessed 12 May 2022]
- World Health Organization. (2022). COVID-19 vaccines [online ], World Health Organisation. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines [Accessed 31 March 2022]
- Wright, L., Steptoe, A., Mak, H. W., & Fancourt, D. (2022). Do people reduce compliance with COVID-19 guidelines following vaccination? A longitudinal analysis of matched UK adults. Journal of Epidemiology & Community Health, 76(2), 109–115. https://doi.org/10.1136/jech-2021-217179
- Yan, Y., Bayham, J., Richter, A., & Fenichel, E. P. (2021). Risk compensation and face mask mandates during the COVID-19 pandemic. Scientific Reports, 11(1), 1–11. https://doi.org/10.1038/s41598-021-82574-w
- Youssef, D., Issa, O., Kanso, M., Youssef, J., Abou-Abbas, L., & Abboud, E. (2022). Practice of non-pharmaceutical interventions against COVID-19 and reduction of the risk of influenza-like illness: A cross-sectional population-based study. Journal of Pharmaceutical Policy and Practice, 15(1), 1–12. https://doi.org/10.1186/s40545-022-00450-y