
ALSUntangled Update 27
ALSUntangled reviews alternative and off label treatments on behalf of people with ALS (PALS). Here we review inosine, for which we have received more than 1500 requests (Citation1).
Overview
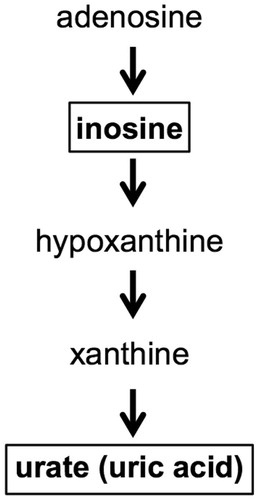
Inosine is available as an over-the-counter oral supplement (Citation2). When taken by mouth, it is rapidly metabolized, resulting in increased blood levels of urate (). Inosine can cross the blood-brain barrier (Citation3) and increase CSF levels of urate as well (Citation4).
Figure 1. How inosine increases urate.
Mechanism
Urate (sometimes referred to as uric acid) is a naturally occurring antioxidant (Citation5,Citation6). Interest in urate as a possible neuroprotective agent began when researchers noted that high urate levels are associated with lower risk of developing Parkinson’s disease (Citation7–9) and Alzheimer’s disease (Citation10). Naturally occurring high levels of urate are also associated with slower disease progression in Parkinson’s disease (Citation11–13).
The biological mechanisms that cause ALS are not completely understood, but they are likely to include damage to the motor neurons from oxidative stress, as supported by both autopsy and laboratory studies (Citation14). It follows that antioxidants such as urate (or agents that increase levels of these such as inosine) might theoretically be neuroprotective in ALS. Some (Citation15–18) but not all (Citation19–22) studies find that high urate is associated with prolonged survival in PALS. Further database analyses and clinical trials are underway to try and clarify this.
Beyond just neuroprotection via urate elevation, recent work suggests that inosine can stimulate the growth of axons in culture, promote collateral sprouting in the corticospinal tract, and even enhance motor recovery after traumatic brain injury (Citation23). These observations suggest that inosine might be able to enhance reinnervation in ALS.
ALSUntangled assigns a TOE ‘Mechanism’ grade of C based on this information ().
Table I. TOE grades for inosine as an ALS treatment.
Pre-clinical data
Several well-controlled studies have demonstrated that urate is neuroprotective in cell culture and animal models of neurologic diseases. Across a range of Parkinson’s disease models, urate elevation has prevented in vitro cell death induced by oxidative and mitochondrial toxins (Citation24–26) and has improved function in vivo (Citation24). Urate was also neuroprotective in various models of neurotoxicity beyond Parkinson’s disease, including cultured spinal cord neurons (Citation27) and models of spinal cord injury and stroke (Citation28,Citation29). Studies of urate modulation in pre-clinical models of ALS are ongoing but results are not yet available.
ALSUntangled assigns a TOE ‘Pre-Clinical’ grade of U based on this information ().
Data in PALS
Cases
Within the online community PatientsLikeMe, 14 people reported taking inosine for ALS and seven have evaluations (Citation30). These PALS used doses ranged from 500 mg daily to 3000 mg daily. One reported ‘slight’ effectiveness, “it makes me feel better, like a tonic”. The others reported either no effectiveness (n = 2) or unknown effectiveness (n = 4). Google search identified no additional PALS reporting on inosine’s effectiveness.
ALSUntangled assigns a TOE ‘Cases’ grade of D based on this information ().
Trials
Trials of inosine in PALS are currently in progress. These studies leverage the rapidly accumulating experience with inosine use in Parkinson’s disease. SURE-PD, a recent study of safety of urate elevation in Parkinson’s disease (Citation4), demonstrated that inosine administration was safe and well tolerated when performed under medical monitoring of urate levels and urine studies (see below). Based on SURE-PD, as well as compelling epidemiologic and pre-clinical evidence, a phase III study of inosine (SURE-PD3) was recently launched for this population (details for the design of this trial are available on clinicaltrials.gov; NCT02642393). With relevance to ALS, a small pilot, open-label study of inosine in PALS was recently completed (details for the design of this trial are available on clinicaltrials.gov; NCT02288091) and results are being analyzed. A follow-up, phase II study of inosine in PALS is in the planning stages. These studies will help clarify the therapeutic potential of inosine for ALS.
ALSUntangled assigns a TOE ‘Trials’ grade of U based on this information ().
Risks and costs
The physiologic range of urate in blood is 3.6–8.5 mg/dl, with levels typically higher in males than females (Citation31). Target urate levels in the above-described clinical trials were 7–8 mg/dl; when people take inosine by mouth, blood levels of urate rise. If levels rise too far above physiologic range, people may develop gout and kidney stones. In one trial of inosine for multiple sclerosis, 25% of treated patients developed kidney stones (Citation32). There is also the potential risk for adverse cardiovascular events (such as high blood pressure, heart attack, or stroke), although this is still debated (Citation33). When taking inosine it is therefore very important to monitor urate levels in the blood on a regular basis (approximately every 3–6 weeks) under the direction of a physician.
Another important safety concept is that urine acidity and concentration are major determinants of the risk of developing kidney stones (Citation34). There are several types of kidney stones. Urate stones tend to develop when urine is very concentrated and acidic (Citation34). Maintaining good hydration helps reduce this risk. When urine is acidic, the risk of forming stones made of urate increases significantly (Citation34). Some people have urine that is more acidic than others’. In addition, some foods such as high doses of vitamin C or cranberry juice can potentially lower urine pH (Citation35). Therefore, urine pH (a measure of acidity) needs to be monitored regularly.
Based on all this, ALSUntangled assigns a Risks grade of C ().
A month’s supply of inosine costs approximately between $10 and $60 depending on the brand and how much inosine one needs to take to achieve the desired blood levels of urate (usual dose is one to six 500-mg capsules a day depending on one’s metabolism).
Conclusions
Inosine is a low-cost supplement that increases the levels of urate, a naturally occurring antioxidant. With appropriate blood and urine monitoring, it appears reasonably safe. Epidemiologic data suggest that high urate levels may be associated with improved survival in ALS, which prompted pre-clinical studies and clinical trials of inosine. These are still ongoing and will help determine whether inosine could be a useful treatment for ALS.
Declaration of interest
ALSUntangled is sponsored by the ALS Association and the Motor Neurone Disease Association.
References
- URL:http://www.alsuntangled.com/completed.html. Accessed: 2016-07-30. (Archived by WebCite® at http://www.webcitation.org/6jOZoknma)
- URL:http://www.swansonvitamins.com/source-naturals-inosine-500-mg-120-tabs?otherSize=SN094&SourceCode=INTL405C&CAWELAID=249784076&catargetid=530002460000100149&cadevice=c&mkwid=VLkUpZ12&pcrid=80480685367&gclid=CNCdoq6-jc4CFRJahgodw9YLzA. Accessed: 2016-07-30. (Archived by WebCite® at http://www.webcitation.org/6jOa32ySH)
- Marangos P, Trams E, Clark-Rosenberg R, Pal S, Skolick P. Anticonvulsant doses of inosine result in brain levels sufficient to inhibit [3H] diazepam binding. Psychopharmacology (Berl). 1981;75:175–8.
- Parkinson Study Group S-PDI, Schwarzschild MA, Ascherio A, Beal MF, Cudkowicz ME, Curhan G, et al. Inosine to increase serum and cerebrospinal fluid urate in Parkinson's disease: a randomized clinical trial. JAMA Neurol. 2014;71:141–50.
- Ames BN, Cathcart R, Schwiers E, Hochstein P. Uric acid provides an antioxidant defencee in humans against oxidant- and radical-caused aging and cancer: a hypothesis. Proc Natl Acad Sci U S A. 1981;78:6858–62.
- Bowman GL, Shannon J, Frei B, Kaye JA, Quinn JF. Uric acid as a CNS antioxidant. J Alzheimers Dis. 2010;19:1331–6.
- Alonso A, Rodriguez LA, Logroscino G, Hernan MA. Gout and risk of Parkinson's disease: a prospective study. Neurology. 2007;69:1696–700.
- Gonzalez-Aramburu I, Sanchez-Juan P, Jesus S, Gorostidi A, Fernandez-Juan E, Carillo F, et al. Genetic variability related to serum uric acid concentration and risk of Parkinson's disease. Mov Disord. 2013;28:1737–40.
- Weisskopf MG, O'Reilly E, Chen H, Schwarzschild MA, Ascherio A. Plasma urate and risk of Parkinson's disease. Am J Epidemiol. 2007;166:561–7.
- Lu N, Dubreuil M, Zhang Y, Neogi T, Rai SK, Ascherio A, et al. Gout and the risk of Alzheimer's disease: a population based, BMI-matched cohort study. Ann Rheum Dis. 2016;75:547–551.
- Ascherio A, LeWitt PA, Xu K, Eberly S, Watts A, Mattson W, et al. Urate as a predictor of the rate of clinical decline in Parkinson's disease. Arch Neurol. 2009;66:1460–8.
- Schwarzschild MA, Schwid SR, Marek K, Watts A, Lang AE, Oakes D, et al. Serum urate as a predictor of clinical and radiographic progression in Parkinson's disease. Arch Neurol. 2008;65:716–23.
- Simon KC, Eberly S, Gao X, Oakes D, Tanner CM, Shoulson I, et al. Mendelian randomization of serum urate and Parkinson's disease progression. Ann Neurol. 2014;76:862–8.
- D'Amico E, Factor-Litvak P, Santella RM, Mitsumoto H. Clinical perspective on oxidative stress in sporadic amyotrophic lateral sclerosis. Free Radic Biol Med. 2013;65:509–27.
- Abraham A, Drory VE. Influence of serum uric acid levels on prognosis and survival in amyotrophic lateral sclerosis: a meta-analysis. Journal of Neurology. 2014;261:1133–8.
- Paganoni S, Zhang M, Quiroz Zarate A, Jaffa M, Yu H, Cudkowicz M, et. al. Uric acid levels predict survival in men with amyotrophic lateral sclerosis. Journal of Neurology. 2012;259:1923–8.
- Kuffner R, Zach N, Norel R, Hawe J, Schoenfeld D, Wang L, et al. Crowd-sourced analysis of clinical trial data to predict amyotrophic lateral sclerosis progression. Nat Biotechnol. 2015;33:51–7.
- Atassi N, Berry J, Shui A, Zach N, Sherman A, Sinani E, et al. The PRO-ACT database: design, initial analyses, and predictive features. Neurology. 2014;83: 1719–25.
- Keizman D, Ish-Shalom M, Berliner S, Maimon N, Vered Y, Artamonov I, et al. Low uric acid levels in serum of patients with ALS: further evidence for oxidative stress? J Neurol Sci. 2009;285:95–9.
- Zheng Z, Guo X, Wei Q, Song W, Cao B, Huang R, et al. Serum uric acid level is associated with the prevalence but not with survival of amyotrophic lateral sclerosis in a Chinese population. Metab Brain Dis. 2144.29:771–5.
- Chio A, Calvo A, Bovio G, Canosa A, Bertuzzo D, Galmozzi F, et al. Amyotrophic lateral sclerosis outcome measures and the role of albumin and creatinine: a population-based study. JAMA Neurology. 2014;71: 1134–42.
- Duan Y, Fan D. Association of serum uric acid level with amyotrophic lateral sclerosis. Zhonghua Yi Xue Za Zhi. 2016;96:207–9.
- Moore T, Pessina M, Finkelstein S, Killiany R, Bethany B, Benowitz L, et al. Inosine enhances recovery of grasp following cortical injury to the primary motor cortex of the rhesus monkey. Restor Neurol Neurosci. 2016. [Epub ahead of print].
- Chen X, Burdett TC, Desjardins CA, Logan R, Cipriani S, Xu Y, et al. Disrupted and transgenic urate oxidase alter urate and dopaminergic neurodegeneration. Proc Natl Acad Sci U S A. 2013;110:300–5.
- Cipriani S, Desjardins CA, Burdett TC, Xu Y, Xu K, Schwarzschild MA. Urate and its transgenic depletion modulate neuronal vulnerability in a cellular model of Parkinson's disease. PLoS One. 2012;7:e37331.
- Cipriani S, Desjardins CA, Burdett TC, Xu Y, Xu K, Schwarzschild MA. Protection of dopaminergic cells by urate requires its accumulation in astrocytes. J Neurochem. 2012;123:172–81.
- Du Y, Chen CP, Tseng CY, Eisenberg Y, Firestein BL. Astroglia-mediated effects of uric acid to protect spinal cord neurons from glutamate toxicity. Glia. 2007;55:463–72.
- Yu ZF, Bruce-Keller AJ, Goodman Y, Mattson MP. Uric acid protects neurons against excitotoxic and metabolic insults in cell culture, and against focal ischemic brain injury in vivo. J Neurosci Res. 1998;53:613–25.
- Scott GS, Cuzzocrea S, Genovese T, Koprowski H, Hooper DC. Uric acid protects against secondary damage after spinal cord injury. Proc Natl Acad Sci U S A. 2005;102:3483–8.
- URL:https://www.patientslikeme.com/treatments/show/533-inosine-side-effects-and-efficacy#overview. Accessed: 2016-07-27. (Archived by WebCite® at http://www.webcitation.org/6jK2vIwxo).
- Cipriani S, Chen X, Schwarzschild MA. Urate: a novel biomarker of Parkinson's disease risk, diagnosis and prognosis. Biomark Med. 2010;4:701–12.
- Markowitz C, Spitsin S, Zimmerman V, Jacobs D, Udupa J, Hooper D, et al. The treatment of multiple sclerosis with inosine. J Altern Compliment Med. 2009;15:619–25.
- Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med. 2008;359:1811–21.
- Cameron MA, Sakhaee K. Uric acid nephrolithiasis. Urol Clin North Am. 2007;34:335–46.
- Gettman MT, Ogan K, Brinkley LJ, Adams-Huet B, Pak CY, Pearle MS. Effect of cranberry juice consumption on urinary stone risk factors. J Urol. 2005; 174:590–4.