
Abstract
Objective
This meta-analysis was aimed to verify the influences of interleukin 23 receptor (IL-23R) rs11209026 and rs2201841 polymorphisms on the susceptibility of rheumatoid arthritis (RA).
Methods
We searched potentially relevant studies on the relationships of IL-23R gene rs11209026 and rs2201841 polymorphisms with RA susceptibility from PubMed (Medline), CNKI and EMBASE web databases. Crude odds ratios (ORs) along with 95% confidence intervals (95% CIs) were calculated to assess the strength of association through the fixed- or random-effects model.
Results
Eight published articles containing 5544 RA patients and 5532 health individuals were included in our meta-analysis. In total analysis, we found IL-23R gene rs11209026 polymorphism was not related to RA susceptibility in all genetic models, but there was a significant association between rs2201841 polymorphism and RA susceptibility under G vs. A model. In stratified analysis by ethnicity, an increased RA susceptibility was detected for rs2201841 polymorphism in Caucasian group.
Conclusion
The results of meta-analysis indicated that IL-23R gene rs2201841 polymorphism might be a susceptible factor for RA under G vs. A model, especially in Caucasian population.
Keywords:
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease (AID) impacting human health severely [Citation1]. It is characterized by synoviocyte hyperplasia, neovascularization and partial infiltration of numerous T cells [Citation2], inducing synovial inflammation, articular cartilage damages, bone and joint capsules at different levels, and finally leads to joint deformity and functional incapacitation [Citation3]. As one of the primary disabling diseases, the pathogenesis of RA involves in genetic factors and environmental factors [Citation4,Citation5]. Moreover, the genetic factors account for 50–60% of all RA cases [Citation6,Citation7]. However, the precise aetiology of this disease is still beyond totally understood. So far, many RA-related susceptibility genes have been identified, including HLA, PADI4 and PTPN22 [Citation8–10]. Furthermore, other genes are still emerging to be implicated in the incidence of RA.
Interleukin 23 receptor (IL-23R) is produced by antigen-presenting cells (like macrophages and dendritic cells) with the actions of certain infections [Citation11]. It plays a key role not only in inflammatory diseases but also in innate immunity and adaptive immunity [Citation12,Citation13]. In addition, IL-23R also dramatically affects the process of cell transformation from CD4+T to Th17, which increases the number of Th17 cells and maintains their activity, thus inducing the generation of proinflammatory cytokine IL-17 [Citation14]. In accordance with relevant experimental models, Th17 lymphocyte subsets which secrete IL-17 may cause the damages in various positions, involving bones, cartilages, joints, brains, lungs, hearts and intestinal tracts [Citation15]. In addition, researches also demonstrate that the variants in IL-23R gene increase the susceptibilities of AIDs in patients with inflammatory bowel disease, psoriasis or multiple sclerosis [Citation16,Citation17]. Sato et al. suggested that IL-23R/IL-17 axis played a vital role not only in the growth stage of autoimmune arthritis but also in osteoclasia stage, indicating that IL-23R may correlate with the susceptibility of RA [Citation18].
Some researchers have reported the relationship between IL-23R gene polymorphisms and RA risk but got no consistent result. Therefore, we searched all eligible articles on the role of IL-23R gene rs11209026 and rs2201841 polymorphisms in individual susceptibility to RA so as to statistically discuss such relationship for a more reliable conclusion.
Materials and methods
Search strategy and selection criteria
Relevant publications were identified through searching PubMed (Medline), China National Knowledge Infrastructure (CNKI) and EMBASE web databases using the following search terms: “interleukin 23 receptor or IL-23R” and “polymorphism or mutation or variant” and “rheumatoid arthritis or RA”. What is more, we also checked the references of relevant articles to find any other potentially relevant papers. Studies for this meta-analysis were selected based on the following criteria: (1) with a case-control design; (2) involving the associations of IL-23R gene rs11209026 and rs2201841 polymorphisms with the susceptibility of RA; (3) providing adequate genotype data to calculate odds ratios (ORs) with 95% confidence intervals (95% CIs). The articles which did not meet the above-mentioned criteria were excluded.
Data extraction
The information extracted by two independent investigators from each study included first author’s name, year of publication, original country, ethnicity, source of control, genotyping method and genotype and/or allele distributions in cases and controls. Another investigator would be consulted whenever no consensus could not be reached over conflicting results of abstracted data after discussing between the two investigators.
Statistical analysis
Summary ORs and 95% CIs were calculated to evaluate the relationships of IL-23R gene rs11209026 and rs2201841 polymorphisms with the susceptibility of RA under five genetic contrasts: homozygote, dominant, recessive, allele and heterozygote models. Stratified analysis was performed based on ethnicity. Heterogeneity was measured using Q-statistic and I2 test, and if p < .05 or I2 > 50%, indicating significant heterogeneity, the random-effects model was applied to calculate pooled ORs; otherwise, the fixed-effects model was used. χ2 test was employed to measure the deviation of genotype distribution from Hardy–Weinberg equilibrium (HWE) in controls. Publication bias was inspected by funnel plots and Egger’s test. We also performed sensitivity analysis to detect the stability of our results by sequentially omitting each single study. The STATA version 12.0 (STATA Corp, College Station, TX, USA) software was used for all data syntheses in this meta-analysis. Significant threshold was fixed at p < .05 for all tests.
Results
Study characteristics
As shown in , 204 articles were initially searched from the databases, and 132 irrelevant publications were excluded through scanning abstracts. Then, additional 57 papers were removed in further screening without controls (17), meta-analysis (6) and not concerning IL-23R gene rs11209026 and rs2201841 polymorphisms (35). Additionally, six articles were deleted due to the lack of genotype data. Therefore, this meta-analysis included eight case-control studies [Citation19–26], containing 5544 RA patients and 5532 controls. demonstrates the main characteristics of included studies. The genotype distributions of the controls did not conform to HWE (p < .05) in 4 studies [Citation20,Citation22,Citation23,Citation26].
Figure 1. Flow diagram of article selection process.
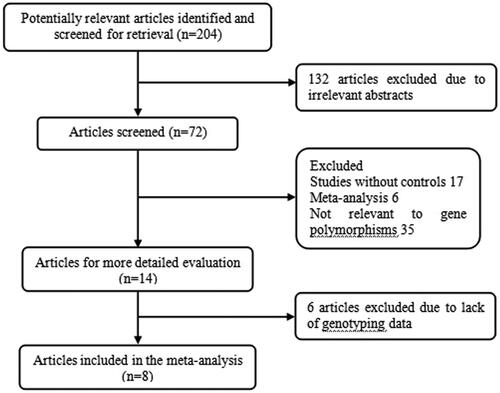
Table 1. Principal characteristics of the studies included in the meta-analysis.
Meta-analysis results
The main results of the meta-analysis are displayed in . From pooled results, we found no significant association between IL-23R gene rs11209026 and RA susceptibility under all comparison models in total analysis. However, a significant association was observed for IL-23R gene rs2201841 polymorphism in the model G vs. A (OR = 1.18, 95% CI = 1.05–1.32) ().
Figure 2. Forest plot of RA susceptibility associated with IL-23R gene rs2201841 polymorphism under the G vs. A model. The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
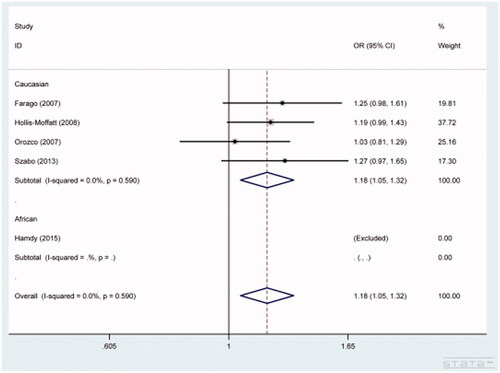
Table 2. IL-23R Gene polymorphisms and RA susceptibility.
In subgroup analysis based on ethnicity, only one article involved African populations, the combined analysis result was not accurate, thus the results were not presented in this study. Increased susceptibility of RA was found for the rs2201841 polymorphism in Caucasian group (allele G vs. allele A: OR = 1.18, 95% CI = 1.05–1.32) ().
Heterogeneity test
We observed significant heterogeneity for IL-23R gene rs11209026 (allele A vs. allele G: p = .000) and rs2201841 (GG vs. AA: p = .006) polymorphisms, so the random-effects model was utilized to calculate combined results. The fixed-effects model was used for the rest genetic models in current meta-analysis.
Sensitivity analysis and publication bias
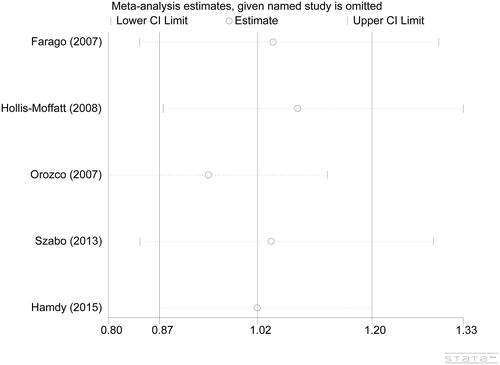
The results of sensitivity analysis showed that no single study impacted the overall ORs qualitatively, confirming the statistical stability of our findings ().
Figure 3. Sensitivity analysis for IL-23R gene rs2201841 polymorphism under the allele A vs. allele G model.
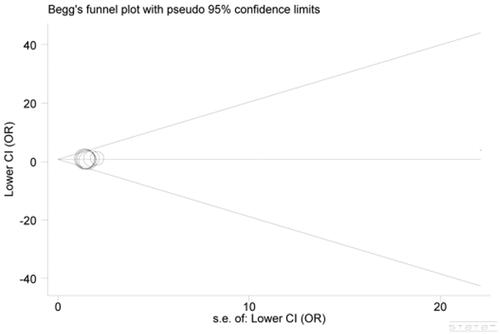
None of the funnel plots showed distinct asymmetry (), implying the absence of significant publication bias. Besides, all these results were also certified by statistical evidence from Egger’s test (p = .298).
Figure 4. Begg’s funnel plot for publication bias. Each point represents a separate study for the indicated association. Log(OR): natural logarithm of OR; Horizontal line: mean effect size.
Discussion
The pathogenesis of RA is still not completely understood, with an average prevalence rate of approximately 1% worldwide, and there are around 4 million RA patients in China. No specific medicine has been developed for the therapy of RA so far. Since conventional therapeutic approaches can only relieve patients’ pains and inflammations, retard or terminate the damages of joints, improve the health degree and action competence, they cannot radically cure such disease fundamentally. In recent years, the unceasing development of molecular biology has revealed that the mediation of cytokines may have pivotal influences on the generation and growth of joint diseases. The functions of cytokines such as interleukin and tumour necrosis factors are the critical mechanism of inflammatory responses.
IL-23, a new-found heterodimer cell-molecule, is mainly created by activated mononuclear macrophages and dendritic cells [Citation27] and also secreted by microglias in brain [Citation28]. It is composed of specific subunit IL-23p19 and IL-12p40 by disulfide bone, with extremely similar molecular structures as IL-12 [Citation27,Citation29]. IL-23, the cytokine connecting innate and adaptive immunity, can only exert its biological effects through binding to specific IL-23 receptor which has high affinity on the surface of target cells, so the latter is the key to regulate the biological activity of the former. IL-23 receptor consists of two subunits IL-23R and IL-12RB1 and is expressed on the surface of memory T cell principally [Citation30]. IL-23R gene, encoding for IL-23R, is polymorphic and is located on human chromosome 1p31.3. Focusing on the polymorphisms in this gene, scholars have reported their roles in individual susceptibility to RA.
Varade et al. found that the A allele of IL-23R rs11209026 polymorphism was associated with increased predisposition to RA in their studied Spanish [Citation19], and Hamdy et al. suggested a similar effect of the AA genotype of the polymorphism based on Egyptians, though they found no significant relationship for the other polymorphism rs2201841 [Citation25]. Besides, Farago et al. detected a risk-increasing influence of the CC genotype of IL-23R rs2201841 polymorphism on RA in their study [Citation22]. However, Hollis–Moffatt et al. insisted there was no significant relationship of RA risk either with the rs11209026 polymorphism or with the rs2201841 polymorphism [Citation20]. Moreover, Orozco et al. reported that there was no significant difference of allele or genotype frequencies of these two polymorphisms between RA patients and controls, and concluded that they seemed not to be related to RA predisposition in a Spanish population [Citation23].
Considering these controversial findings on the correlation between IL-23R polymorphisms and RA risk, we performed this study to combine them for a clearer perspective on this issue. Consequently, our results demonstrated that there was no significant association between IL-23R gene rs11209026 and RA susceptibility in total analysis, but the rs2201841 polymorphism increased the risk of RA under G vs. A contrast. Additionally, we also observed a similar influence of the two polymorphisms rs11209026 and rs2201841 on RA susceptibility after subgroup analysis according to ethnicity in African and Caucasian groups, respectively.
This meta-analysis had certain comprehensiveness, but there still were some limitations which should be taken into consideration. First, the number of included studies was relatively small, affecting the accuracy of results. Secondly, only published articles were included in our meta-analysis, so other relevant studies might be omitted. Third, gene–gene and loci–loci interactions were not discussed in the present study because of insufficient data. Fourth, only one article involved African populations, thus the subgroup analysis result based on ethnicity was not accurate. Finally, the majority of included studies were based on Caucasians, thus possibly introducing some selective bias.
In summary, our meta-analysis suggested that IL-23R gene rs2201841 polymorphism was related to the increased susceptibility of RA, especially in Caucasians. In future, the correlations of IL-23R gene polymorphisms with RA susceptibility require to be validated in larger studies.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Iwaszko M, Swierkot J, Kolossa K, et al. Influence of CD94 and NKG2A variants on susceptibility to rheumatoid arthritis and efficacy of anti-TNF treatment. Joint Bone Spine. 2016;83:75–79.
- Iwaszko M, Świerkot J, Kolossa K, et al. Polymorphisms within the human leucocyte antigen-E gene and their associations with susceptibility to rheumatoid arthritis as well as clinical outcome of anti-tumour necrosis factor therapy. Clin Exp Immunol. 2015;182:270–277.
- Emery P, Kavanaugh A, Bao Y, et al. Comprehensive disease control (CDC): what does achieving CDC mean for patients with rheumatoid arthritis? Ann Rheum Dis. 2015;74:2165–2174.
- Kharlamova N, Jiang X, Sherina N, et al. Antibodies to Porphyromonas gingivalis indicate interaction between oral infection, smoking and risk genes in rheumatoid arthritis etiology. Arthritis Rheumatol. 2016;68:604–613.
- Castro-Santos P, Diaz-Pena R. Genetics of rheumatoid arthritis: a new boost is needed in Latin American populations. Rev Bras Reumatol. 2016;56:171–177.
- Ruyssen-Witrand A, Lukas C, Nigon D, et al. Association of IL-2RA and IL-2RB genes with erosive status in early rheumatoid arthritis patients (ESPOIR and RMP cohorts). Joint Bone Spine. 2014;81:228–234.
- Combe B, Rincheval N. Early lessons from the recent-onset rheumatoid arthritis cohort ESPOIR. Joint Bone Spine. 2015;82:13–17.
- Spurlock CF, 3rd, Tossberg JT, Olsen NJ, et al. Cutting edge: chronic NF-kappaB activation in CD4+ T cells in rheumatoid arthritis is genetically determined by HLA risk alleles. JI. 2015;195:791–795.
- Lee YH, Bae SC. Association between susceptibility to rheumatoid arthritis and PADI4 polymorphisms: a meta-analysis. Clin Rheumatol. 2016;35:961–971.
- Ates A, Karaaslan Y, Karatayli E, et al. Association of the PTPN22 gene polymorphism with autoantibody positivity in Turkish rheumatoid arthritis patients. Tissue Antigens. 2011;78:56–59.
- Moens E, Brouwer M, Dimova T, et al. IL-23R and TCR signaling drives the generation of neonatal Vgamma9Vdelta2 T cells expressing high levels of cytotoxic mediators and producing IFN-gamma and IL-17. J Leukoc Biol. 2011;89:743–752.
- Kave M, Shadman M, Alizadeh A, et al. Analysis of the association between IL-23R rs11209026 polymorphism and incidence of atherosclerosis. Int J Immunogenet. 2015;42:341–345.
- Eken A, Singh AK, Treuting PM, et al. IL-23R + innate lymphoid cells induce colitis via interleukin-22-dependent mechanism. Mucosal Immunol. 2014;7:143–154.
- Wendling D, Cedoz JP, Racadot E. Serum and synovial fluid levels of p40 IL12/23 in spondyloarthropathy patients. Clin Rheumatol. 2009;28:187–190.
- Steinman L. A brief history of T(H)17, the first major revision in the T(H)1/T(H)2 hypothesis of T cell-mediated tissue damage. Nat Med. 2007;13:139–145.
- Cargill M, Schrodi SJ, Chang M, et al. A large-scale genetic association study confirms IL12B and leads to the identification of IL23R as psoriasis-risk genes. Am J Hum Genet. 2007;80:273–290.
- Nunez C, Dema B, Cenit MC, et al. IL23R: a susceptibility locus for celiac disease and multiple sclerosis?. Genes Immun. 2008; 9:289–293.
- Sato K, Suematsu A, Okamoto K, et al. Th17 functions as an osteoclastogenic helper T cell subset that links T cell activation and bone destruction. J Exp Med. 2006;203:2673–2682.
- Varade J, Ramon Lamas J, Rodriguez L, et al. IL23R and IL12B genes: susceptibility analysis in rheumatoid arthritis. Ann Rheum Dis. 2009;68:1230–1232.
- Hollis-Moffatt JE, Merriman ME, Rodger RA, et al. Evidence for association of an interleukin 23 receptor variant independent of the R381Q variant with rheumatoid arthritis. Ann Rheum Dis. 2009;68:1340–1344.
- Chang M, Saiki RK, Cantanese JJ, et al. The inflammatory disease-associated variants in IL12B and IL23R are not associated with rheumatoid arthritis. Arthritis Rheum. 2008;58:1877–1881.
- Farago B, Magyari L, Safrany E, et al. Functional variants of interleukin-23 receptor gene confer risk for rheumatoid arthritis but not for systemic sclerosis. Ann Rheum Dis. 2008;67:248–250.
- Orozco G, Rueda B, Robledo G, et al. Investigation of the IL23R gene in a Spanish rheumatoid arthritis cohort. Hum Immunol. 2007;68:681–684.
- Bogunia-Kubik K, Swierkot J, Malak A, et al. IL-17A, IL-17F and IL-23R gene polymorphisms in Polish patients with rheumatoid arthritis. Arch Immunol Ther Exp (Warsz). 2015;63:215–221.
- Hamdy G, Darweesh H, Khattab EA, et al. Evidence of association of interleukin-23 receptor gene polymorphisms with Egyptian rheumatoid arthritis patients. Hum Immunol. 2015;76:417–420.
- Szabo M, Safrany E, Pazar B, et al. Marked diversity of IL23R gene haplotype variants in rheumatoid arthritis comparing with Crohn's disease and ankylosing spondylitis. Mol Biol Rep. 2013;40:359–363.
- Oppmann B, Lesley R, Blom B, et al. Novel p19 protein engages IL-12p40 to form a cytokine, IL-23, with biological activities similar as well as distinct from IL-12. Immunity. 2000;13:715–725.
- McInnes IB, Leung BP, Sturrock RD, et al. Interleukin-15 mediates T cell-dependent regulation of tumor necrosis factor-alpha production in rheumatoid arthritis. Nat Med. 1997;3:189–195.
- Brombacher F, Kastelein RA, Alber G. Novel IL-12 family members shed light on the orchestration of Th1 responses. Trends Immunol. 2003;24:207–212.
- Kullberg MC, Jankovic D, Feng CG, et al. IL-23 plays a key role in Helicobacter hepaticus-induced T cell-dependent colitis. J Exp Med. 2006;203:2485–2494.