
Abstract
The objective of this research was to describe the use and utility of a dual diagnosis assessment scale and intervention strategies package for clinical and community mental health staff to better engage service users and explore reasons for use regarding dual diagnosis issues. A case study was developed, with the service user’s consent, to be used to train others in use of the Reasons for Use Package (RFUP). Findings were that the RFUP can enable staff to better tune in to service users in terms of how they are managing symptoms, side effects, social situations, peer pressure, affect and ambivalence. The RFUP helped enable the service user to feel a sense of being listened to and respected with regard to their dual diagnosis experiences. Conclusions drawn were that service users can engage with dual diagnosis assessment more readily when workers use dual diagnosis tools and mentoring purpose-designed to enhance an understanding of motivations and reasons for use of substances.
PUBLIC INTEREST STATEMENT
People with dual diagnosis die on average 20 years earlier than the general population from treatable and preventable issues. For service users, family members and staff, there is a need to address gaps in service delivery and provide a pathway to beneficial integrated treatment. This user-friendly purpose-built tool and associated workforce development approach could have a positive impact in reducing the economic and health burden of dual diagnosis. This paper will be of interest to a wide spectrum of stakeholders including service users, family members, service providers and governmental bodies.
1. Introduction
Research indicates it is very important across both mental health and substance use services to adopt dual diagnosis competencies as core business. (Minkoff & Cline, Citation2004). In the United States, the Epidemiological Catchment Area study in the early 1980s found that highest levels of co-morbidity were present in people with a lifetime history of any drug use, other than alcohol; with 53% having co-morbid mental disorders and 47% having co-morbid alcohol disorders (Teeson & Proudfoot, Citation2003, p. 1–2). To assist workers to open up dual diagnosis conversations with service users, screening tools can be useful; one such tool is the Reasons for Use scale (Spencer, Castle, & Michie, Citation2002). The first and second author of the current study extended the utility of the Reasons for Use scale to create a package of strategies that can be utilised with service users.
1.1. Reasons for Use Package (RFUP)
The Reasons for Use Package (RFUP), a dual diagnosis resource, was developed by a Melbourne metropolitan dual diagnosis service (Nexus), in consultation with service users, family members and staff. The RFUP consists of the Reasons for Use Scale (Spencer et al., Citation2002), and a number of potential follow up strategies to explore with the service user (Figure ). The package includes a specific “spirit” guiding the desired approach. This entails a collaborative and supportive process between staff and the service user using the RFUP as a doorway to conversation about dual diagnosis. Staff receive training and, importantly, mentoring in how to use the RFUP which reinforces this “spirit.” The service user is supported to actively explore their dual diagnosis issues. This deliberately shifts the power balance to the service user rather than the more passive approach whereby the staff member “assesses” the service user and decides on treatment options. The service user and the staff member gain a shared understanding and, importantly, the service user is actively involved in negotiating their treatment plan.
Figure 1. Components of the reasons for use package.

1.2. Mentoring as a part of the RFUP
Mentoring: One Definition
“Mentoring is a developmental relationship and, like education and training, the primary objective is learning.”
(McDonald J, Citation2002, p. 11)
The RFUP mentoring process has a number of purposes. Firstly, to facilitate reflection on initial use of the RFUP. Secondly, the purpose is to generate a potential source of new mentors. These mentors then sustain the use of the RFUP practice, as individual staff articulate and discuss their thoughts around their use of the RFUP. The staff who are involved are then better able to facilitate mentoring of colleagues in their own engagement with and use of the package.
The mentoring model is outlined in an organisational guide, a mentor’s guide, and a mentee’s guide. These have been developed and refined in response to feedback from various inputs and serve as a useful starting point when implementing RFUP mentoring. The model was designed to mirror the spirit of the RFUP so that mentoring sessions reflected the desired collaborative explorative style of the service user and staff interaction. Individual staff feel supported in exploring their practice and are thus able to move into mentoring colleagues by following a structure based on facilitation rather than the perceived need for expert knowledge. Mentoring helps externalise practice so it can be explored and change can occur (Scott & Spouse, Citation2013). The two-part mentoring process (described elsewhere Myers, K., Kroes, S., O’Connor, S., & Petrakis, M., Citation2018a). reflects the two-part service user process.
Staff need to feel that they can explore the use of the RFUP at different levels according to their experience. A staff member’s initial use should not be judged based on the service user outcome alone, as this will vary according to the service user’s circumstances. In practice, staff confidence in their use of the RFUP often reflects the service user’s experience. Thus, an organisational approach which aggregates various experiences is more likely to build practice wisdom. Implementation appears to work best when the RFUP process is completed within teams and organisations rather than to a group of disparate attendees from various services coming together.
At the first meeting with the creators of the package, implementing the mentoring model is discussed with the organisation. The model is explained so that the organisation gains a clear understanding of the model and its benefits and issues to consider. Importantly, at this stage, the organisation agrees to fully support the process, which includes freeing up staff to attend mentoring sessions. The creators of the RFUP suggest the allocation of a coordinator type role to assist with this process. Management identifies staff who they think would be effective mentors; usually, these are experienced staff who are seen as practice leaders. This organisational endorsement contributes to capacity building and culture change through further legitimising the importance of engaging in the full RFUP rather than just training alone. Practice wisdom on both the use and impact of the RFUP for service users is given support and conveyed through mentoring. Positive experiences can multiply over time rather than being lost as one-off events.
Using the RFUP has been very rewarding in practice, because it combines the RFU screening tool, follow up strategies, training and mentoring. This develops knowledge and confidence to explore and implement the strategies for staff and service users to work together.
1.3. Objective
To describe the use and utility of a dual diagnosis assessment scale and intervention strategies package for clinical and community mental health staff to better engage service users and explore reasons for use regarding dual diagnosis issues.
2. Methods
This paper is part of a wider national evaluation that employed mixed methods of data collection. A successful pilot was initially developed by Nexus in consultation with Monash in 2012. Nexus Dual Diagnosis Service, Neami National and Monash Social Work Department set up a research partnership in 2013. The first pilot in 2012 included six Neami National Staff in October 2012 who enthusiastically called on Neami National management to support a wider rollout within their organisation.
The RFUP research partnership aimed to further develop an evidence base, increase the number of Neami National staff able to use the RFUP and develop an implementation strategy which could be replicated for similar agencies. In 2014 due to the Victorian State Government reform of the PDRSS sector, research design including ethics applications was the main focus of activity. In April 2015, 10 senior practice leaders from Neami National were trained and mentored in the RFUP by Nexus. This group then went on to provide mentoring to their Victorian colleagues.
The dual diagnosis context, theory and approach of the RFUP national evaluation have been discussed elsewhere (Myers, Kroes, O’Connor & Petrakis, Citation2017; Myers, Kroes, & Petrakis, Citation2018) and the need for congruence between mentoring and the approach staff when using the RFUP with service users (Myers et al., Citation2018a; Petrakis, Robinson, Myers, Kroes & O'Connor, Citation2018).
2.1. Case study research methodology
Case study research approaches are characterised by choice of a methodology “that facilitates exploration of a phenomenon within its context using a variety of data sources” (Baxter & Jack, Citation2008, p. 544). The use of case studies is distinct from other forms of social inquiry—for example, experimental designs and studies utilising survey methodologies—since they are particularly explorative nature, they use a variety of methods, and they utilise bottom-up procedures (Gomm, Hammersley & Foster, Citation2000, p. 2; Meyer, Citation2015).
3. Results
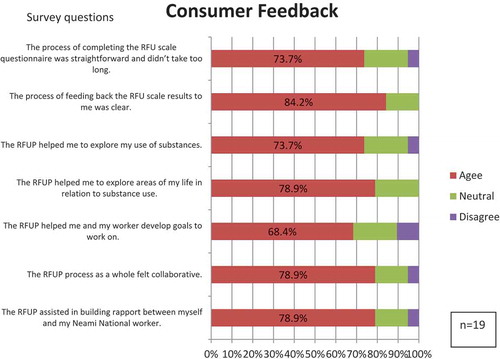
Data from a service user self-report questionnaire with a 5-point Likert scale ranging from strongly agree to strongly disagree (aggregated for display purposes in Figure ) strongly suggest that service users found the RFUP a beneficial tool.
Figure 2. Aggregated service user feedback.
3.1. Case study
This case study paper illustrates key elements of the RFUP approach and how creating a safe-structured space for exploration can assist treatment planning-benefiting service user and staff member.
3.2. Molly
Molly is a 62-year-old, Anglo-Australian woman living in an inner city suburb with her two children and her husband. Molly identifies as having a lived experience of Schizophrenia, anxiety and obsessive-compulsive disorder. Molly says she first started hearing voices around age 8. She has spent a great deal of her life in and out of psychiatric hospitals and this is where she said she started smoking cigarettes. Molly said that she had smoked over a pack a day for most of her life and had switched to using Nicotine patches and gum in her middle 50s.
3.3. Nicotine gum
Nicotine gum is a type of chewing gum that delivers nicotine to the body. It is used as an aid in nicotine replacement therapy (NRT), a process for smoking cessation. The nicotine is delivered to the bloodstream via absorption by the tissues of the mouth. The pieces are usually available in individual foil packages and come in various flavours. Users are directed to chew the gum until it softens and the gum is then “parked,” or tucked, in between the cheek and gums. It is chewed again until taste returns, and is then re-parked in a new location. These steps are repeated until the gum is depleted of nicotine (about 30 minutes) or the craving dissipates. Using Nicotine replacement therapy supported Molly to cease smoking, however, she said that to this day she still feels anxious about chewing the gum and had often expressed the desire to cease altogether.
3.4. RFUP: a structured therapeutic conversation
In one of the regular support visits the Reasons for Use Package and the questionnaire was introduced, and the purpose of the tool was explained. Molly was asked whether she would be interested in completing the RFUP around her Nicotine Gum use. It wasn’t until the conversation about using the Reasons for Use Package began that she disclosed she was chewing up to 40 pieces of 4 mg Nicotine gum per day the average is around 4 − 6 pieces.
The conversation before using the package was extremely valuable as Molly disclosed that she was chewing a significantly high amount of gum and was often going to bed chewing it and had at numerous times woken up choking on the gum in the night. Molly also explained that she believed she had grown a brain tumour from chewing the gum over the past few years and she was expecting to be diagnosed with cancer. Molly became very anxious when speaking about this. She explained that she thought nicotine gum and cigarettes would give her cancer. It was suggested to Molly that the Reasons for Use package could be used to start a conversation about her substance use in relation to her mental health, to get a better understanding why she chews the gum. If she wanted to discuss making some changes in her life this could be worked on together or through seeking additional professional support. A time to meet to complete the RFU scale questionnaire was made. The potential risks of chewing the gum before she slept were discussed, and she decided to try not to sleep with it anymore after the conversation.
3.5. Service user experience
Molly advised that she found the experience of using the questionnaire very easy and non-threatening even though she identified feeling a little confused that day. She was very engaged while doing the questionnaire. Each question was worked through and contributed to a very natural and fluid conversation. Molly reflected on the questions around symptoms of mental health. She said that she often chews gum when she’s feeling nervous, agitated, groggy or tired. Molly said the gum relaxes her in these moments. Molly also reflected on the questions that were around socialising. She said she felt she often chewed more pieces of gum in anticipation of friends or acquaintances coming to the house. Molly often identifies that talking with people is one of her biggest challenges and she realised she was chewing the gum to lower her anxiety. Molly also reflected on the questionnaire saying that she felt she used nicotine gum for many reasons and that she had never thought about this in depth before. She felt she used gum to minimise her anxiety in a lot of areas of her life, especially for motivation and/or in preparation for social situations and when she was feeling unwell. This information was useful in considering treatments. Overall using the questionnaire with Molly was a positive experience and thought-provoking for both service user and staff member.
3.6. Mentoring—a key component
As part of the RFUP, two mentoring sessions were undertaken. For the first session, there was discussion of the staff member’s experience of applying the initial part of the package (completing the RFU questionnaire). This was followed by brainstorming issues relating to the RFUPs five domains (see Figure ). Questions arose such as what could be brought back to the next support? What strategies could be used to present Molly with some reflections in a personal and meaningful way? In mentoring talk was about Molly and how she may best like to be presented with new information. Knowing she liked to read, taking her some information on nicotine replacement therapy seemed beneficial.
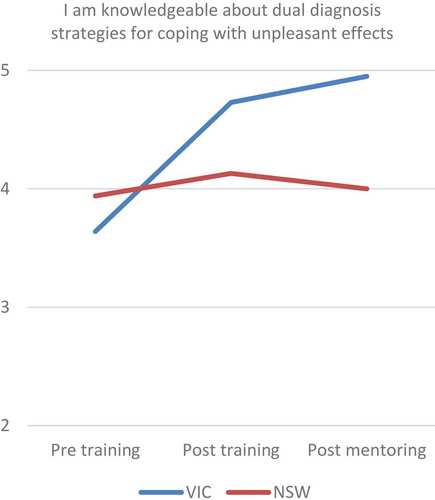
It was concerning that Molly reported having daily, anxiety-provoking thoughts of the gum causing her some form of cancer. More information on nicotine replacement therapy would assist her so that she would have a better understanding of what she was consuming. Her ambivalent relationship with her primary care physician prevented discussing her large consumption with her. The staff member decided to present Molly with some literature and then talk about having a discussion with a specialist health professional, possibly calling Quitline, and speaking to someone with greater knowledge of nicotine replacement therapy. Figure illustrates improvements in knowledge gained by using the RFUP.
Figure 3. Staff knowledge about dual diagnosis strategies for managing drug use related to coping with unpleasant affect.
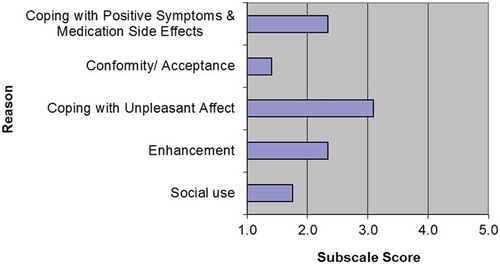
A mentor also provided a list of questions to give to Molly to assist her to explore medications with her primary care physician when ready. Molly had raised an issue during conversation about her psychiatric medication and whether the nicotine gum would be influencing this. After a mentoring session, the staff member and Molly read journal articles on nicotine replacement therapy that the mentor obtained. Fact sheets and information on NRT and other articles were printed and provided to Molly. She found these helpful. As well as gathering information on NRT some of the resources available in the Reasons for Use Package, especially around grounding techniques and mindfulness, were helpful to Molly. The second part of the intervention was to meet with Molly to discuss her results (Figure ) and develop treatment options.
Figure 4. Graph of reasons for using nicotine gum for Molly.
3.7. Goal and outcome-oriented approach
Molly completed the scale in which groups score into five domains. Molly agreed that the results generated from the RFU scale questionnaire were accurate with the domains she had scored in. She mostly identified with chewing gum to reduce her anxiety, which is in the coping with unpleasant affect domain. It was discussed that it might be possible that the nicotine gum may also be contributing to her anxiety. She said she had reflected on her NRT use over the past week and had stopped chewing most nights, just taking it out and putting it beside her bed before she went to sleep. Molly was presented with the information that had been gathered. Molly said she had great relief in knowing that using nicotine gum was much less harmful than smoking but also acknowledged she was probably consuming far beyond the recommended dosage. The session was spent reading the fact sheets and discussing the process that takes place when using Nicotine gum. Molly said she had never had the ins and outs of nicotine gum explained to her and that she had no idea that she could be chewing a lower dose.
Molly was still reluctant to speak to her primary care physician and said she was not ready to speak to a specialist. Molly wasn’t prepared to seek extra support just yet but would think about it in the future. She did decide that she wanted to reduce her gum intake and she had already become mindful of how much she was chewing after our first conversation. Using some mindful strategies as alternatives to anxiety-provoking situations were discussed. A small grounding exercise from one of the mindfulness print outs was practised. Molly said she would take home the information printed off for her to read. Molly reflected on the experience saying she found it extremely valuable.
4. Discussion
The Reasons for Use Package can be a practical way to start conversation with service users about their substance use in relation to their mental health in a gentle, non-threatening and non-judgmental way. Evidence suggests it gives service users a chance to discover why they might be using, how it may interact with their mental health, and that those reasons are genuine and understandable. The package has been a great tool to use with dual diagnosis service users. Many other assessments to open conversation about dual diagnosis issues focus more on what the person uses and the frequency rather than potential reasons for doing so.
The Reasons for Use Package can support service users to understand important reasons why they use particular substances. On discovering those reasons service users can look at alternative ways to cope or to just have a greater understanding of their situation that may lead to better-informed lifestyle choices. Using this tool means the service user's own understanding of their issues can be used to develop collaborative treatment. In this way, it is a more client and recovery centred approach. The third named author used the RFUP with four service users and mentored three workers to use the tool with service users they were supporting as part of the mentoring period. This experience has been in line with other literature (McDonald, Citation2002; Carter & Moreton, Citation2012; Sacks et al., Citation2012), that training alone is not sufficient for practice change. The RFUP Mentoring Model has been utilised in a national case-comparison trial during 2015, with a significant positive impact on the knowledge and confidence of those mentored. (Myers et al., Citation2018b). On reflection, each service user had a unique experience and positive outcome, including: a conversation that had not been had before and prompting a service user to themselves consider their treatment options.
5. Conclusions
A key aspect of the RFUP appears to be its potential to assist staff to facilitate, a non-judgmental way, straightforward conversation about dual diagnosis issues. The package resonates with the style of support aspired to under recovery-oriented practice, by assisting service users to reflect on the role of substances in their lives and the relationship to their recovery.
Additional information
Funding
Notes on contributors
Simon Kroes
The first two authors are senior clinicians with Nexus Dual Diagnosis Service, Melbourne, Australia; part of the Victorian Dual Diagnosis Initiative, established in 2001 supporting dual diagnosis capacity building in clinical mental health, mental health community support services and alcohol and other drug services. The third and fourth authors are from Neami National, a community mental health service supporting people living with mental illness to improve their health, live independently and pursue a life based on their own strengths, values and goals. Neami National provides services from 60+ sites in Western Australia, Queensland, South Australia, Victoria and New South Wales. The final author is a senior lecturer academic from Monash University. Monash is ranked in the top one per cent of world universities according to the Times Higher Education World University Rankings (2013-2014). The 2012-2013 rankings noted Monash as one of only six Australian universities in the world’s top 100.
Kevan Myers
The first two authors are senior clinicians with Nexus Dual Diagnosis Service, Melbourne, Australia; part of the Victorian Dual Diagnosis Initiative, established in 2001 supporting dual diagnosis capacity building in clinical mental health, mental health community support services and alcohol and other drug services. The third and fourth authors are from Neami National, a community mental health service supporting people living with mental illness to improve their health, live independently and pursue a life based on their own strengths, values and goals. Neami National provides services from 60+ sites in Western Australia, Queensland, South Australia, Victoria and New South Wales. The final author is a senior lecturer academic from Monash University. Monash is ranked in the top one per cent of world universities according to the Times Higher Education World University Rankings (2013-2014). The 2012-2013 rankings noted Monash as one of only six Australian universities in the world’s top 100.
Sarah Officer
The first two authors are senior clinicians with Nexus Dual Diagnosis Service, Melbourne, Australia; part of the Victorian Dual Diagnosis Initiative, established in 2001 supporting dual diagnosis capacity building in clinical mental health, mental health community support services and alcohol and other drug services. The third and fourth authors are from Neami National, a community mental health service supporting people living with mental illness to improve their health, live independently and pursue a life based on their own strengths, values and goals. Neami National provides services from 60+ sites in Western Australia, Queensland, South Australia, Victoria and New South Wales. The final author is a senior lecturer academic from Monash University. Monash is ranked in the top one per cent of world universities according to the Times Higher Education World University Rankings (2013-2014). The 2012-2013 rankings noted Monash as one of only six Australian universities in the world’s top 100.
Sarah O’Connor
The first two authors are senior clinicians with Nexus Dual Diagnosis Service, Melbourne, Australia; part of the Victorian Dual Diagnosis Initiative, established in 2001 supporting dual diagnosis capacity building in clinical mental health, mental health community support services and alcohol and other drug services. The third and fourth authors are from Neami National, a community mental health service supporting people living with mental illness to improve their health, live independently and pursue a life based on their own strengths, values and goals. Neami National provides services from 60+ sites in Western Australia, Queensland, South Australia, Victoria and New South Wales. The final author is a senior lecturer academic from Monash University. Monash is ranked in the top one per cent of world universities according to the Times Higher Education World University Rankings (2013-2014). The 2012-2013 rankings noted Monash as one of only six Australian universities in the world’s top 100.
Melissa Petrakis
The first two authors are senior clinicians with Nexus Dual Diagnosis Service, Melbourne, Australia; part of the Victorian Dual Diagnosis Initiative, established in 2001 supporting dual diagnosis capacity building in clinical mental health, mental health community support services and alcohol and other drug services. The third and fourth authors are from Neami National, a community mental health service supporting people living with mental illness to improve their health, live independently and pursue a life based on their own strengths, values and goals. Neami National provides services from 60+ sites in Western Australia, Queensland, South Australia, Victoria and New South Wales. The final author is a senior lecturer academic from Monash University. Monash is ranked in the top one per cent of world universities according to the Times Higher Education World University Rankings (2013-2014). The 2012-2013 rankings noted Monash as one of only six Australian universities in the world’s top 100.
References
- Baxter, P., & Jack, S. (2008). Qualitative case study methodology: Study design and implementation for novice researchers. The Qualitative Report, 13(4), 544–9.
- Carter, M., & Moreton, J. (2012). Capacity building & change management: A guide for community services. Melbourne: VAADA © Victorian Alcohol and Drug Association 2016.
- Gomm, R., Hammersley, M., & Foster, P. (Eds.). (2000). Case study method: Key issues, key texts. Sage.
- McDonald, J. (2002). Mentoring: An age old strategy for a rapidly expanding field A what, why and how primer for the alcohol and other drugs field. Adelaide: National Centre for Education and Training on Addiction (NCETA) Flinders University.
- Meyer, B. (2015). Case studies. In C. V. Angelelli & B. J. Baer (Eds.), Researching translation and interpreting (Chapter 14, pp. 195–202). London: Routledge.
- Minkoff, K., & Cline, C. A. (2004). Changing the world: The design and implementation of comprehensive continuous integrated systems of care for individuals with co-occurring disorders. Psychiatric Clinics, 27(4), 727–743. doi:10.1016/j.psc.2004.07.003
- Myers, K., Kroes, S., & Petrakis, M. (2018). A foundation for dual diagnosis practice: Wisdom, tools and resources. chapter 9 In M. Petrakis (Ed.), Social work practice in health: An introduction to contexts, theories and skills (pp. 135–152). Sydney: Allen & Unwin.
- Myers, K., Kroes, S., O’Connor, S., & Petrakis, M. (2018a). Community managed mental health and the NDIS–Learning from the past and working towards a good life. New Paradigm, 25.
- Myers, K., Kroes, S., O'Connor, S., & Petrakis, M. (2018b). The reasons for use package: How mentoring aids implementation of dual diagnosis practice. New Paradigm, 25–29.
- Myers, K., O’Connor, S., Petrakis, M., & Kroes, S. (2017). The reasons for use package: Development research and implementation lessons for the field. 26th Contemporary TheMHS in Mental Health Services, ‘People: Authenticity starts in the heart’ 23-26 August 2016, Auckland New Zealand. 2016 TheMHS Conference Proceedings. Australia.
- Petrakis, M., Robinson, R., Myers, K., Kroes, S., & O’Connor, S. (2018). Dual diagnosis competencies: A systematic review of staff training literature. Addictive Behaviors Reports, 7, 53–57. doi:10.1016/j.abrep.2018.01.003
- Sacks, S., Chaple, M., Sirkantraporn, J., Sacks, J., Knickman, J., & Martinez, J. (2012). Improving the capability to provide integrated mental health and substance abuse services in a state system of outpatient care. Journal of Substance Abuse Treatment, 44(5), 488–493. doi:10.1016/j.jsat.2012.11.001
- Scott, I., & Spouse, J. (2013). Practice based learning in nursing, health and social care: Mentorship, facilitation and supervision. John Wiley & Sons.
- Spencer, C., Castle, D., & Michie, P. T. (2002). Motivations that maintain substance use among individuals with psychotic disorders. Schizophrenia Bulletin, 28(2), 233–247. doi:10.1093/oxfordjournals.schbul.a006934
- Teeson, M., & Proudfoot, H. (2003). Comorbid mental disorders and substance use disorders: Epidemiology, prevention and treatment. Australia: National Drug and Alcohol Research Centre (NDARC), University of New South Wales.