

Abstract
Background
COPD is the fourth leading cause of death worldwide, with particularly high rates in the People’s Republic of China, even among never smokers. Large population-based cohort studies should allow for reliable assessment of the determinants of diseases, which is dependent on the quality of disease diagnoses. We assessed the validity of COPD diagnoses collected through electronic health records in the People’s Republic of China.
Methods
The CKB study recruited 0.5 million adults aged 30–79 years from ten diverse regions in the People’s Republic of China during the period 2004–2008. During 7 years of follow-up, 11,800 COPD cases were identified by linkage with mortality registries and the national health insurance system. We randomly selected ~10% of the reported COPD cases and then undertook an independent adjudication of retrieved hospital medical records in 1,069 cases.
Results
Overall, these 1,069 cases were accrued over a 9-year period (2004–2013) involving 153 hospitals across ten regions. A diagnosis of COPD was confirmed in 911 (85%) cases, corresponding to a positive predictive value of 85% (95% confidence interval [CI]: 83%–87%), even though spirometry testing was not widely used (14%) in routine hospital care. The positive predictive value for COPD did not vary significantly by hospital ranking or calendar period, but was higher in men than women (89% vs 79%), at age ≥70 years than in younger people (88%, 95% CI: 85%–91%), and when the cases were reported from both death registry and health insurance systems (97%, 95% CI: 94%–100%). Among the remaining cases, 87 (8.1%) had other respiratory diseases (chiefly pneumonia and asthma; n=85) and 71 (6.6%) cases showed no evidence of any respiratory disease on their clinical records.
Conclusion
In the People’s Republic of China, COPD diagnoses obtained from electronic health records are of good quality and suitable for large population-based studies and do not warrant systematic adjudication of all the reported cases.
Supplementary materials
Figure S1 The location of ten survey sites in China Kadoorie Biobank (CKB).
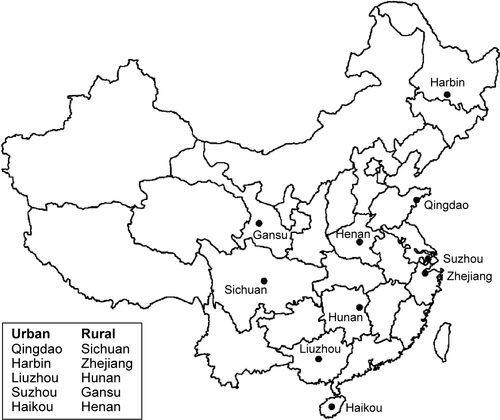
Figure S2 Venn diagram showing the breakdown of sources for total COPD outcomes in China Kadoorie Biobank (CKB).
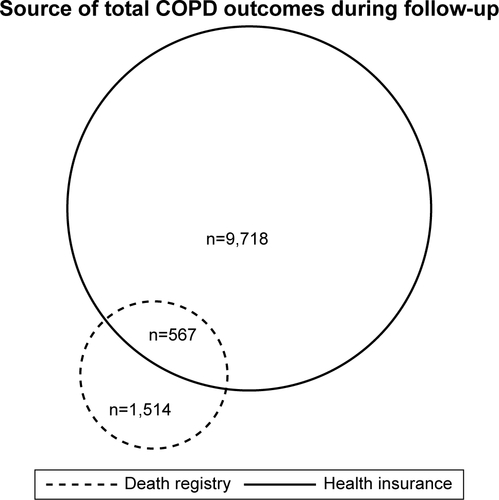
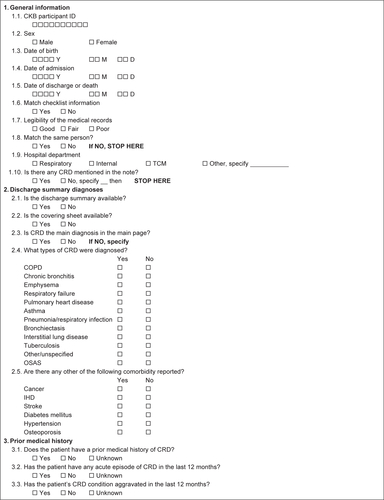
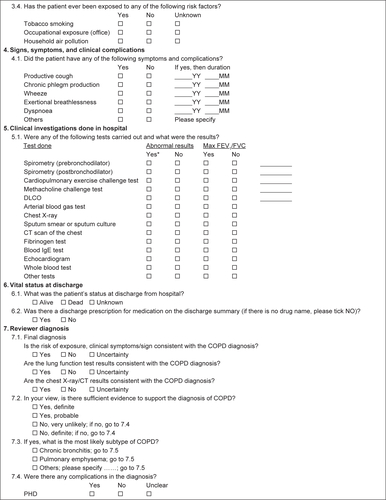
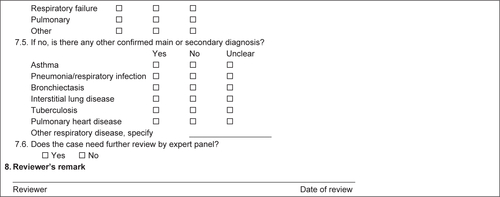
Figure S3 China Kadoorie Biobank (CKB) disease validation form for chronic respiratory diseases (CRD).
Abbreviations: OSAS, obstructive sleep apnea syndrome; IHD, ischemic heart diseases; FEV1/FVC, forced expiratory volume in 1 second/forced vital capacity; DLCO, diffusing capacity of the lungs for carbon monoxide; CT, computed tomography; IgE, immunoglobulin E; PHD, Pulmonary Heart Disease; ID, identification.
Acknowledgments
Our most important acknowledgment is to the participants in the study and the members of the survey teams in each of the ten regional centers, as well as to the project development and management teams based at Beijing, Oxford, and the ten regional centers. We gratefully acknowledge the support of the following organizations for our research: Baseline survey: Kadoorie Charitable Foundation, Hong Kong; long-term continuation: UK Wellcome Trust (088158/Z/09/Z, 104085/Z/14/Z); Chinese National Natural Science Foundation (81390541, 81390544); The British Heart Foundation; UK Medical Research Council and Cancer Research UK provided core funding to the Oxford CTSU; support for the present respiratory study was partly provided by GlaxoSmithKline (WEUKBRE5848). JV was personally supported by the Swiss National Science Foundation (P2LAP3_155086), Lausanne University Hospital, and Société Industrielle et Commerciale de Produits Alimentaires Foundation.
Disclosure
KJD is an employee of GlaxoSmithKline. The authors report no other conflicts of interest in this work.